
Abstract
Personal mobile phone has become an integral part of our lives. In the medical field, the growing popularity of medicine applications allows more rapid communication among healthcare professionals and quick access to helpful information, which facilitates and improves patient care practice. The use of smartphones during work activities by healthcare professionals can cause a lack of attention and errors while carrying out health procedures. The result might be an increased threat endangering the safety of patients. The purpose of the present study was to investigate the level of nomophobia (a psychological condition regarded as a fear of being detached from mobile phone connectivity) and its correlations with the use of smartphones in clinical practice, distraction due to personal use and policies regarding mobile phones use in a sample of resident doctors of a University of Southern Italy. A cross-sectional study was carried out on 204 hospital residents divided into three areas depending on their duties: clinical, surgical, and services. Two tools were used: nomophobia questionnaire (NMP-Q) and a composite questionnaire investigating smartphone use in the specific healthcare setting. Sixty percent of participants were affected by a moderate level of nomophobia and 10% by a severe degree, jeopardizing both the work and social relationships of young doctors. Smartphone use can certainly represent a helpful support tool for clinical practice; consequently, we believe it would be appropriate to find instruments to screen smartphone dependence or compulsive use to further prevent, early diagnose or treat this detrimental disorder for health professionals.
Introduction
Over the years portable technology has undergone considerable development resulting in the spread of “smart devices” such as tablets, laptops, notebooks, and smartphones. Smartphone has gradually gained an increasingly central role in ordinary daily activities: from a simple, valuable device for making telephone calls, it gradually evolved into a multifunctional device able to deal with heterogeneous support functions of daily life (e.g., internet access, use of social networks, e-mails, instant messaging services, applications, e-commerce). Often, doctors are “digital omnivores,” using multiple devices routinely in a professional setting, and the number of healthcare professionals who use even three digital platforms at the same time (smartphone, tablet, and laptop/desktop) has been projected to increase (Epocrates, 2013).
The percentage of health professionals using smartphones has risen from 66 to 90% in 2012 (Dubey et al., 2014). Recently, an online survey conducted by Accreditation Council for Graduate Medical Education (ACGME) in California, revealed that more than 85% of participants used a smartphone (Abolfotouh et al., 2019). The usage of smartphone technology influenced clinical practice in several ways, in particular regarding the ease of interpersonal communication and quick access to data (Stergiannis et al., 2017; Zarandona et al., 2019).
Healthcare professionals use the digital platform as proper support of their clinical practice, to perform calculations, to obtain information about the technical data sheet of drugs, to timely access guidelines, and to study and update. An increasing body of evidence suggests that these devices would improve decision-making procedures and upgrade the communication among hospital staff (Feroz et al., 2020; Firdouse et al., 2018; Payne et al., 2012) and between healthcare workers and patients (Say et al., 2015; Thompson, 2016). By sharing instant messaging, photos, diagnostic reports, and real-time therapy updates (Cho & Lee, 2016; Nerminathan et al., 2017; Salam et al., 2018), the clinical practice would be exponentially enhanced in terms of productivity, efficiency and precision. Further, patient access to primary care and medical care in the hospital setting would be optimized (Chauhan et al., 2018; De La Cruz Monroy & Mosahebi, 2019; Yaman et al., 2016).
However, a careful analysis of the relationship between technological innovation and productivity is essential for awareness of both learning opportunities and work efficiency and the possible associated problems. The extensive use of the mobile phone at work and for training purposes could create a potential source of distraction (Al-Ghamdi, 2018; Soto et al., 2017; Tran et al., 2014), representing a hazard to privacy and patient safety (Gill et al., 2012; Katz-Sidlow et al., 2012). Distractions, indeed, could cause a loss of productivity and also determine medical errors potentially characterized by severe repercussions for the patient’s health (McBride, 2015).
The issues arising from the incorrect use of mobile technology would add up to other distressing elements for both mental health and cognitive functions, in particular within the younger medical population, including night-shift workers (Briguglio et al., 2021; Costa et al., 2020). This category is particularly prone to suffer from nomophobia (“NO-MObile-PHOne-phoBIA”), defined as an uncontrollable fear of being without a personal mobile phone or being unable to use it when needed. Nomophobia is a newly defined psychological disorder since it can cause anxiety and awkwardness when the subject is deprived of his mobile phone (Rodríguez-García et al., 2020; Yildirim et al., 2016). Technology dependences were not recognized as a different diagnosis in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-4). Nevertheless, “Internet Gaming Disorder” has been included in the fifth edition (DSM-5), proving the need for the improvement of research in digital dependency. It is crucial to distinguish between the necessity of using healthcare technologies and their potential negative consequences for the health of the user (King et al., 2020).
Therefore, the possible adverse events, arising from smartphone technology use during clinical practice, suggest the need to establish restriction policies and to educate health professionals on the appropriate use of the smartphone in the working context. These precautions will prevent any possible form of technology misuse (Gill et al., 2012; Katz-Sidlow et al., 2012).
Many studies have focused on nursing students (Ayar & Gürkan, 2022; Çatıker et al., 2021; Çobanoğlu et al., 2021; Özdil et al., 2022; Ramjan et al., 2021; Yatmaz et al., 2022) and medical students (Chatterjee & Kar, 2021; Gupta et al., 2021; Sanusi et al., 2022; Wang et al., 2021); but only a few investigated the effects of mobile technology misuse on healthcare professionals (Alan et al., 2022; Hoşgör et al., 2021) and post-graduated residents (Al Mukhaini et al., 2021).
Under these premises, this study aimed to assess the level of nomophobia and its correlation with the use of smartphones in clinical practice, and the level of distraction due to personal use within a sample of resident doctors. As a secondary aim, we also investigated the occurrence of predictive independent variables of nomophobia, such as sociodemographic characteristics and life habits.
Subjects and Methods
This cross-sectional study was carried out on a sample consisting of resident physicians (doctors on training courses) operating at the University Hospital of Messina, in Southern Italy. As part of a compulsory health surveillance program for healthcare personnel, according to legislative Decree n.81/2008 on occupational health and safety (D.lgs. 9 aprile 2008, n. 81, 925, 2008), resident doctors had to undergo a medical examination to gain work eligibility. On that occasion, they were asked to participate in this study and to give their written informed consent. Their participation was voluntary and without any reward. This study was carried out in accordance with the Declaration of Helsinki’s ethical standards. Being part of the mandatory occupational health surveillance, the study needed no formal approval by the local Ethics Committee. Inclusion criteria were considered: to be resident doctors (in health specialties within the same University Hospital), to agree to the study involvement, and to possess a personal mobile phone. The only exclusion criterium was the occurrence of any psychological issue; thus, people were not included if they had psychological diagnoses which would presumably change levels of nomophobia (especially if someone had anxiety). Enrolled subjects belonged to three working areas: clinical, surgical, and services. The medical specialties of the clinical area included diversified daily activities, such as blood gas sampling, thoracentesis, coronary angiography, assisted ventilation, several diagnostic instruments and tools usage (e.g., ultrasound scan, ergometry, digestive endoscopy, respiratory function tests and allergy diagnostics). General surgery, neurosurgery, obstetrics and gynecology and orthopedics belong to the surgical area. The surgery activities were mainly represented by surgical operating room activities and the management of the pre- and post-operative hospitalization procedures. The area of services included the residents of forensic medicine, hygiene and preventive medicine, occupational medicine, anesthesiology, clinical microbiology and clinical pharmacology. The main activities of this area can be summarized in laboratory activity, mandatory health surveillance, and biological/environmental monitoring.
The interview consisted of the administration (during a medical examination) of a data collection form to assess both sociodemographic characteristics and lifestyle habits (gender, age, marital status, parenthood, coffee consumption, smoking habit, alcohol intake, diseases, medications and year in the training course). Additionally, personal information about mobile technology tools usage was also collected (i.e., the overall time of smartphone usage, usage of additional electronic devices, usage of smartphone for social network platforms consultation, for sending/receiving messages, for voice calls and leisure). To assess the prevalence of nomophobia and its correlation with the daily use of the mobile phone device by resident doctors, two tools were included in the survey: the Italian version of the validated nomophobia (NMP-Q) questionnaire (Adawi et al., 2018; Yildirim & Correia, 2015) and a composite questionnaire used by Zarandona et al. (2019). The average time for filling in the questionnaires ranged between 15 and 30 min. NMP-Q includes 20 items using a 7-point Likert scale, with different response options: ranging from 1 (totally disagreeing) to 7 (totally agreeing). NMP-Q questions are divided into four main themes: not accessing information, giving up convenience, not communicating, and losing connectedness. Nomophobia severity was calculated by summing item answers to produce a total score, ranging from 20 to 140. A score ≤20 indicates a complete absence of nomophobia; 21 to 59 identifies a mild form of nomophobia; a 60 to 99 score expresses moderate levels of nomophobia, with the risk of interferences with life, work, and social relationships. A score ≥100 classifies a severe degree of nomophobia; the subject experiences significant anxiety when he cannot access his phone, which might be frequently associated with cognitive disorders, social phobia, depression, substance abuse and other addictions (Adawi et al., 2018). NMP-Q showed a Cronbach’s alpha of .95.
The composite questionnaire, proposed by Zarandona et al. (2019) consisted of 24 items. The first nine items assessed the frequency of smartphone use during clinical practice for professional purposes (Q1–Q9 with a Cronbach’s alpha of .80). Item Q10 concerned the improvement of work efficiency, while Q11a and Q11b assessed the time of smartphone use per day during working hours. Items Q12 to Q20 (Cronbach’s alpha of .86) evaluated distraction related to the use of a mobile phone (due to both personal use and for other purposes). The last four items (Q21–Q24) focused on the policies regarding smartphone use (Cronbach’s alpha of .82). Q1 to Q9 and Q21 to Q24 items were scored on a 5-point Likert scale with the following response options: never = 1, rarely (1–4 times/month) = 2, sometimes (1–6 times/week) = 3, often (1–10 times/day) = 4, and always (>10 times/day) = 5; Q10 to 11 and Q21 to Q24 items were also scored on a 5-point Likert scale, but with different response options: strongly disagree = 1, disagree = 2, uncertain = 3, agree = 4, and strongly agree = 5. The final score was calculated by adding single items score.
Data Analysis
Numerical data are expressed as mean and standard deviation (SD) and categorical variables as numbers and percentages. The non-parametric approach was used since the numerical variables were not normally distributed, as demonstrated by the Kolmogorov-Smirnov test results. The Chi-Square test was applied, regarding categorical variables, to individuate possible differences among the three areas. The non-parametric analysis of variance (Kruskal Wallis test) was used for numerical parameters: total NMP-Q score, frequency of professional use of smartphones during clinical practice, improvement of working efficiency, duration of use of the smartphone during working hours per day, distractions related to the use of mobile phone and policies on smartphone use. The reliability of the NMP-Q questionnaire and the sections “frequency of smartphone use during clinical practice for professional purposes” (Q1–Q9), “distraction related to the use of a mobile phone” (Q12–Q20) and “questions surround the desire for policies” (Q21–Q24) for the questionnaire proposed by Zarandona et al., were evaluated by assessing their internal consistency through the computation of Cronbach’s alpha.
The Spearman correlation test was applied to assess significant interdependence between analyzed parameters, separately for each area. A generalized linear model was also applied to identify the occurrence of predictive independent variables of nomophobia. Statistical analyses were performed using IBM SPSS for Windows, Version 22 (Armonk, NY, IBM Corp.). A p-value ≤ .05 was considered statistically significant.
Results
The sociodemographic characteristics of the study sample are described in Table 1.
Participants’ Sociodemographic Characteristics, Life Habits, Health Status and Work-Related Factors.

Of a total of 260 invited subjects, 204 (93 women and 111 men) agreed to participate and they were all enrolled in the study (acceptance rate 78.5%). Residents were divided into three specialty areas: 44.6% belonged to the clinical area, 25.5% to the surgical area and 29.9% to the services area. The mean age was 30.6 ± 3.3; the majority of the sample was not married (92.2%) and without children (95.1%). The majority of participants usually drank coffee (83.3%), did not smoke (79.9%) or drank alcohol (59.8%). Grouping by year of training course resulted in 27.9% of participants attending the first year, 22.1% in the second year, 20.6% in the third year, 21.1% and 8.3% in the fourth and fifth year respectively.
The information collected regarding the personal use of mobile technology tools is described in Table 2.
Information About Personal Use of Mobile Technology Tools.
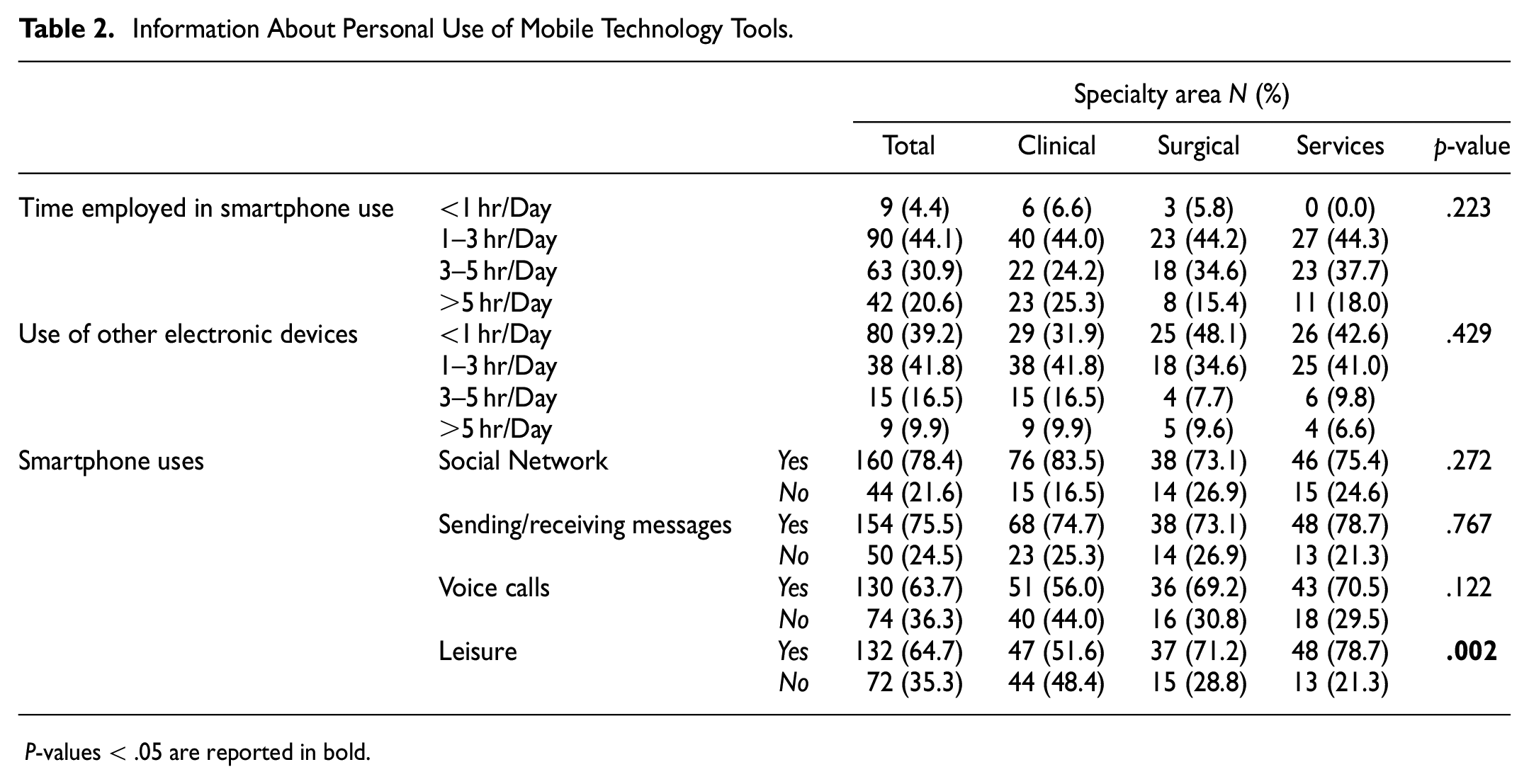
P-values < .05 are reported in bold.
For what concerns personal mobile technology tools use, most of the respondents (44.1%) used smartphones for 1 to 3 hr/day, as well as other electronic devices (41.8%), without any statistically significant differences between the three groups. Resident physicians declared to use smartphones for social networking (78.4%), sending/receiving messages (75.5%), voice calls (65.7%) and leisure (64.7%). From the analysis of the data obtained, it was measured a relevant difference in the use of smartphones for leisure among doctors belonging to the Service area (78.7%), who reported utilizing mobile phones for this use more frequently compared with other areas (71.2% in Surgical Area and 51.6% in Clinical Area).
Concerning the assessment of nomophobia, NMP-questionnaire suggested that the majority of participants (61.3%) had a moderate degree of nomophobia: 65.9% in the clinical area, 48.1% in surgery and 65.6% in services. Only 9.8% had a severe degree of nomophobia (6.6% clinical, 13.5% surgery and 11.7% services), as shown in Figure 1.

Nomophobia degree grouped by area, according to the NMP questionnaire.
Mean scores of NMP-Q and composite questionnaire by Zarandona et al. are reported in Table 3.
Mean Scores of NMP-Q and Composite Questionnaire by Zarandona et al.
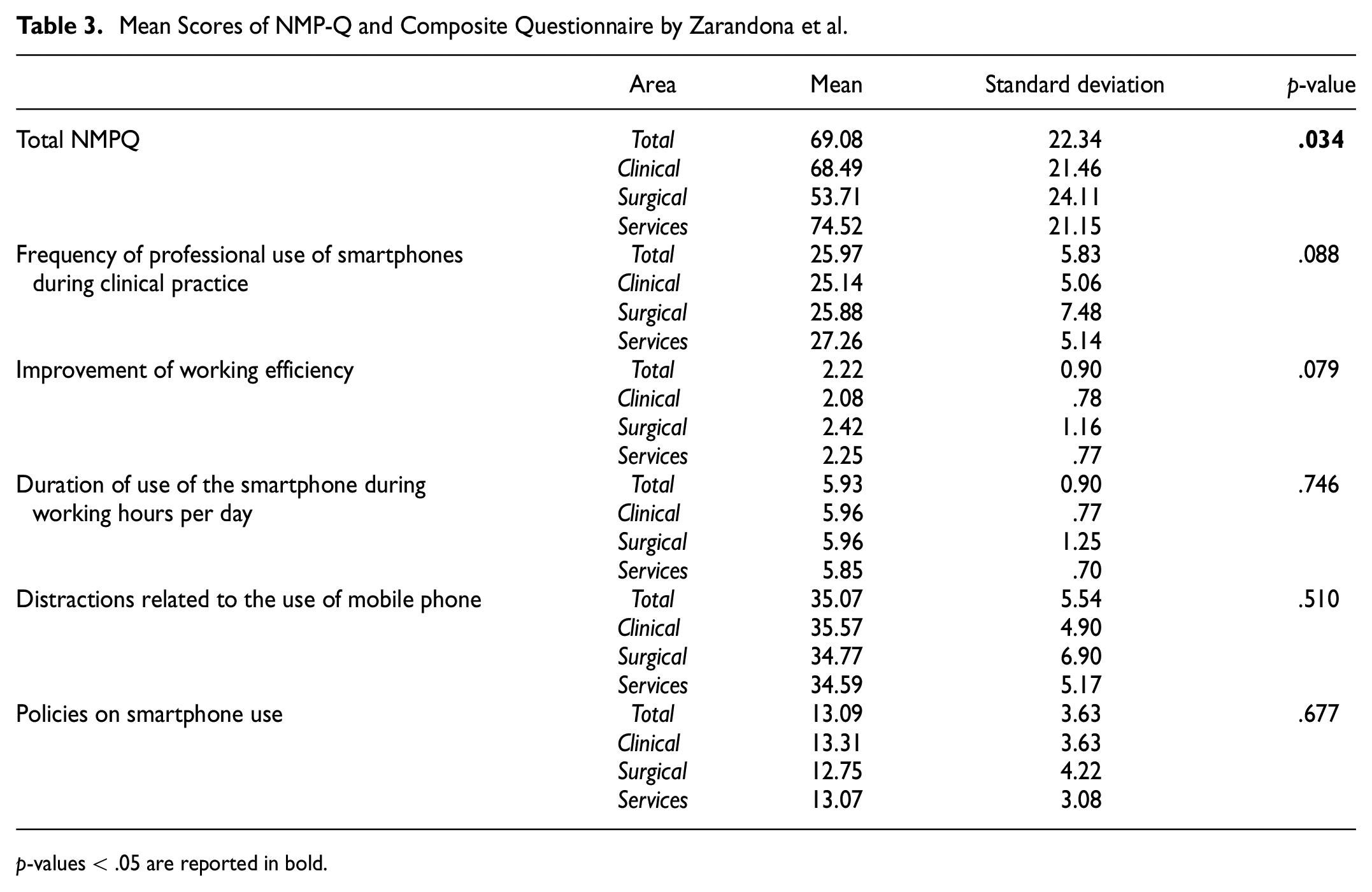
p-values < .05 are reported in bold.
Resident physicians of the service area reported the highest mean scoring in the nomophobia questionnaire, thereby highlighting a statistically relevant difference compared to the other two areas. Conversely, statistical analysis did not reveal any differences in the frequency of professional use of smartphones during clinical practice, improvement of working efficiency, duration of use of the smartphone during working hours per day, distractions related to the use of mobile phones and policies on smartphone use. The non-parametric correlation analysis between NMP-Q and composite questionnaire by Zarandona et al is reported in Table 4.
Non-parametric Correlations.

p-values < .05 are reported in bold.
Only one significant association was observed between the total NMP-Q score and the variable “distraction related to the use of mobile phone,” selectively for the surgical area (r = .29 and p = .035).
The final step of our investigation consisted of the identification of possible independent variables predicting nomophobia through the application of a generalized linear model. The analysis of the results obtained showed that the time employed in smartphone use was a positive predictor of nomophobia, as reported in Table 5.
Generalized Linear Model for NMP-Q.

p-values < .05 are reported in bold.
Discussion
This study investigated the level of nomophobia and the correlation of nomophobia with the frequency of usage of personal smartphones in clinical practice, the improvement of work efficiency, the duration of use of the smartphone during working hours, the amount of distraction due to personal use and, finally, the policies regarding mobile phones use. The study was performed on a defined sample of resident doctors. Furthermore, sociodemographic characteristics and life habits were investigated, as predictive independent variables of nomophobia.
The majority of the sample (44.1%) declared using smartphones from 1 to 3 hr per day, showing a moderate degree of nomophobia (61.3%), especially in residents belonging to the service area. Instead, the NMP-Q questionnaire was associated with distraction related to the use of the mobile phone in the surgical area. Moreover, the time spent using personal smartphones was a predictor of nomophobia.
The majority of the studies already published focused on the mutual relationship existing between perceived stress, the occurrence of sleep disorders and the use of smartphones in clinical practice. The arisen observations highlight that the usage of personal mobile phones has consequences on both mental health and job performance, further suggesting the need for implementing restriction policies (Ramjan et al., 2021).
Our results agree with recent studies about the prevalence of nomophobia in young adults (Gurbuz & Ozkan, 2020; Jilisha et al., 2019) and further identified the use per day of the personal smartphone as a predictor of nomophobia. Consequently, the identified group of doctors may be at risk of developing this condition (Bartwal & Nath, 2020; Schwaiger & Tahir, 2020). As it was previously supposed that the data on daily smartphone usage predisposed doctors to nomophobia, the current results agree with the scores of the NMP-Q questionnaire; 60% of the participants were found to be affected by a moderate degree of nomophobia, and about 1 in 10 residents of the surgical and services area achieved a severe degree of nomophobia. A moderate degree of nomophobia is correlated with the risk of interference with life, work, and social relationships since several studies associated nomophobia with internalizing symptoms such as anxiety, sadness or loneliness (Ozdemir et al., 2018; Samaha & Hawi, 2016; Thomée et al., 2011).
Smartphone distraction, especially from tasks characterized by high responsibility, among healthcare workers could compromise the safety of the patient (Aggarwal et al., 2012). Regarding the reason for smartphone use, the results showed that the most common activities among the residents were respectively social networking (78%), sending/receiving messages (76%) and voice calls (64%). If on the one hand, this wider use of smartphone technology can be a source of distraction, on the other hand, it can positively impact work performance, helping young doctors to restore their concentration and to reduce stress and fatigue (Costa et al., 2021; King et al., 2020; Lin et al., 2013; McBride, LeVasseur, & Li, 2015). But this positive effect applies only when doctors manage to retain control of the time dedicated to this activity.
However, the critical point seems to be the ratio between the frequency of professional use during clinical practice versus the distractions related to the use of a mobile phone. While the first aspect seemed to not be relevant, distractions were positively correlated to nomophobia issues in residents belonging to the surgical area. Participants reported higher values in “distractions related to the use of mobile phone” (nine questions) than in the “frequency of professional use of smartphones during clinical practice” (nine questions). The professional use of the smartphone could be explained by using medical applications for clinical activities or the usage of resources such as medical calculators, drug references, formularies, and guidelines. Thus, for a doctor, applications that increase clinical practice efficiency by saving time, reducing clinical risk and allowing “mobile” rapid decision-making can become popular. Oppositely, the use of a smartphone could increase the sources of distraction during clinical practice, increasing the risk of unfortunate events which can damage patient safety, as demonstrated in other studies (Osorio-Molina et al., 2021; van Harten et al., 2021). Therefore, during worktime, the use of personal communication devices should be dedicated almost exclusively to professional reasons and not to recreational or leisure purposes.
As the two sides of a coin, mobile device usage can be a distraction for young doctors, but at the same time, it could be used for beneficial purposes during clinical training. For example, tutors might choose to share a variety of medical applications, which can be accessed by personal mobile devices, to share data or useful information. As the workplace turns more mobile and global, smartphones bear the ability to instantly connect team members.
Conclusion
Personal smartphones and their functionalities became an integral part of human social and working life. In the medical field, this communication device is widely used by doctors during their daily routine, both for personal and professional purposes. However, this study showed that most of the physicians (61.3%) developed moderate levels of nomophobia, while no associations have been observed between nomophobia and distraction time during clinical practice.
The attention to the correct use of smartphones by healthcare workers is still an emerging topic of interest, given the current lack of scientific papers published on this issue. Besides, the absence of standardized instruments to screen smartphone dependence or the compulsive use of such devices demonstrated the strong need to create novel strategies for prevention, early diagnosis and treatment of this emerging issue for healthcare professionals. Our suggestions include the need to introduce acceptable and ethical guidelines to inform doctors about the appropriate behavior correlated to mobile devices’ usage within the clinical setting. It is needed an improvement of the restriction policies and enforcement of the actual regulations to make correct decisions, to balance the risks associated with distractions, including patient safety and benefits.
Limitations
One of the significant limitations of this study is that it was conducted on a population of doctors in training, therefore relatively young. Consequently, this analysis does not consider the generation gap and does not include doctors with greater working seniority, who have “met” the smartphone when aged compared to younger residents. Moreover, consultants were not enrolled in this study. Nonetheless, these categories, which were not considered for enrollment, might have a lower risk of developing nomophobia. Furthermore, it would have been interesting to investigate the emotional sphere of the participants using additional psycho-diagnostic tools, but this would have required the administration of additional questionnaires, going beyond our study purposes. Finally, self-reported questionnaires might bear the risk of being biased or inaccurate and this might be an additional limitation of this study design.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440231194463 – Supplemental material for Smartphone Use Among Resident Physicians: Prevalence and Risk Factors in Clinical Practice
Supplemental material, sj-docx-1-sgo-10.1177_21582440231194463 for Smartphone Use Among Resident Physicians: Prevalence and Risk Factors in Clinical Practice by Chiara Costa, Michele Teodoro, Manuela Coco, Francesca Verduci, Federica Giambò, Sebastiano Italia, Angela Alibrandi and Concettina Fenga in SAGE Open
Footnotes
Acknowledgements
None.
Authors’ Contributions
CF, CC conceived, designed and supervised the study. AA, and FV analyzed the data. FG and MC performed the studies. SI and MT wrote and supervised the study. All authors read, edited and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The study was carried out in accordance with the Declaration of Helsinki’s ethical standards. Being part of the mandatory occupational health surveillance, the study needed no formal approval by the local Ethics Committee. Written informed consent was obtained and the participation was voluntary and without any reward.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.