
Abstract
Given the high rates of completed suicide and poor help-seeking among young men, this research explored how young men, who had successfully sought help from a Child and Adolescent Mental Health Service (CAMHS), experienced help-seeking. The study focused on the factors that facilitated initial access and ongoing engagement in services. Eight young men between the ages of 16 to 18, who had entered CAMHS following self-harm or suicidal ideation, and who were engaged in ongoing therapy, were recruited. Each young man was interviewed to elicit his personal experiences of help-seeking and help-receiving. Interviews were transcribed and subjected to Interpretative Phenomenological Analysis. Four superordinate themes, which overarched participant’s individual experiences, emerged from the data: Role of external adult in recognizing, normalizing, and initiating help-seeking; challenging and renegotiating perception of need for help and meaning behind this need; maintaining an independent self; and mechanisms of engagement. Help-seeking was described as a journey of two stages: (a) initial access and (b) ongoing engagement, during which the presence and timing of external influences (parents, teachers) and internal influences (personal beliefs and attitudes) were crucial. A model of help-seeking in young men who self-harmed was developed, which considered both access and engagement to help, and combined a consideration of internal and external influences on their ability to access help.
Introduction
Males and Self-Harm
The scale of self-harm and suicidal ideation among young people has become a global health concern (Hawton, Saunders & O’Conor, 2012; World Health Organization, 2014). Raising most concern is the significant association between self-harm, suicidal ideation, and an increased risk of completed suicide (Andover & Gibb, 2010; Muehlenkamp, Claes, Havertape, & Plener, 2012). Young men are seen as a particularly “at risk group” with an alarming increase in suicide in men aged 15 to 44 over the past decade (National Suicide Prevention Strategy; Department of Health [DH], 2012). This trend has been accounted for by increased lethality of self-harm methods by men (Garland & Zigler, 1993) and poorer help-seeking intentions (Cusack, Deane, Wilson, & Ciarrochi, 2006).
Theoretical Models of Help-Seeking
In the context of mental health difficulties, help-seeking refers to “using informal and professional networks to gain support in coping with mental health problems” (Michaelmore & Hindley, 2012, p. 507). Informal sources refer to family, peers, and the Internet, and formal sources includes trained health care professionals, teachers, and youth workers.
A wide range of theoretical models have been proposed to understand the complex process of help-seeking including deterministic models (Andersen & Newman, 1973) and dynamic models (Pescosolido, 1992). A common criticism across the literature, however, is its adult-oriented focus, resulting in limited direct relevance for young people (Murray, 2005). Incorporating consideration of the differential impact of life stages within help-seeking models is important. This is particularly true for young people given that the unique tasks associated with adolescence (increased autonomy and independent decision making), which have been highlighted as potentially obstructive to the help-seeking process (Rickwood, Deane, & Wilson, 2007). Costello, Pescosolido, Angold, and Burns (1998) attempted to do this in their adaptation of the Network Episode Model (Pescosolido, 1992). The Network Episode Model–Revised (NEM-R; Costello et al., 1998) highlighted the difference in autonomy and agency that children and adults have over their health care and focused on the influence of external agencies (family, school) on facilitating help-seeking.
In contrast to the focus on external influences, Biddle, Donovan, Sharp, and Gunnell (2007) developed a model of help-seeking based on intra-personal influences (attitudes and beliefs) and obtained this data through interviewing young adults who had self-harmed. The Cycle of Avoidance (COA; Biddle et al., 2007) explored the way in which young adults interpret their internal distress and how this affects their decision not to seek help (barriers). The COA explained that help-seeking for self-harm was dependent on the following: (a) lay diagnosis (“normal” requiring no intervention, or “real” requiring action), (b) normalizing and coping, (c) a movable threshold of need, and (d) social meanings attached to distress and help-seeking.
Despite the numerous models proposed to predict and describe help-seeking, there remains a discrepancy between the need for accessing professional help and the actual seeking of professional help, particularly for self-harm and suicidal behaviors (Hawton, Rodham, Evans & Harriss, 2009; Meltzer, Harrington, Goodman, & Jenkins, 2001). This has resulted in increased research into factors that inhibit (barrier) and enable (facilitate) help-seeking.
Barriers to Help-Seeking for Self-Harm
Barriers to help-seeking have been extensively researched. In terms of stable, demographic barriers, gender has been highlighted as one of the most consistent predictors of non-help-seeking for self-harm by young people (Mariu, Merry, Robinson, & Watson, 2012; Michaelmore & Hindley, 2012). In terms of more dynamic barriers, a number of studies have explored how young people’s attitudes and beliefs about help-seeking for self-harm negatively influence their behavior. These studies have found that men, in particular, exhibit more anti-help-seeking attitudes.
Male-sensitive attitudes are characterized by the desire to uphold the dominant stereotyped characteristics of masculinity (Jordan et al., 2012; Pederson & Vogel, 2007) and include beliefs that they should handle problems themselves (Rickwood, Wilson, Deane, & Ciarrochi, 2005) and cope independently (Cigularov, Chen, Thurber, & Stallones, 2008; Curtis, 2010; Gould et al., 2004), and that seeking help might negatively affect their sense of self or social standing (Cigularov et al., 2008; Curtis, 2010; Fortune, Sinclair, & Hawton, 2008; Freedenthal & Stiffman, 2007; Gilchrist & Sullivan, 2006; Wadman, 2010). In addition, beliefs regarding “no perceived need for help” were also endorsed by young men, which might suggest difficulties with recognizing their own experiences of distress (Rickwood et al., 2007). One particularly gender-salient variable that is endorsed by males and replicated throughout studies is self-stigma (Vogel, Wade, & Hackler, 2007), whereby negative societal views on help-seeking by men are internalized and enacted (Jordan et al., 2012).
Rationale for Research
In comparison with the wealth of data pertaining to unmet need and barriers to help-seeking for self-harm by young people, very little is known about met need and the factors that facilitate help-seeking (Gulliver, Griffiths, & Christensen, 2010; Rothì & Leavey, 2006). A number of reports have acknowledged this imbalance and have recommended that research priorities should shift to explore where and how young people seek help (Barker, 2007), focusing on what enabled help-seeking rather than what obstructed it.
While help-seeking research has traditionally focused on understanding the process of access to services, there is now growing interest into researching the factors that enable (facilitate) ongoing engagement once help is sought, particularly since poor treatment engagement is a marker for adverse outcomes (Pillay & Wassenaar, 1995). Given the high rates of treatment drop-out by young people who self-harm (Ougrin & Latif, 2011), research into the factors that facilitate ongoing engagement is crucial in this area.
Young men are seen as a particularly “at risk group” for suicide, with an increase in suicide in men aged 15 to 44 over the past decade (National Suicide Prevention Strategy [DH], 2012). This trend has been accounted for by increased lethality of self-harm methods by men (Garland & Zigler, 1993) and poorer help-seeking intentions (Cusack et al., 2006). With young men being underrepresented in support services and overrepresented in mortality figures following completed suicide, it was felt that this research should focus on how young men, who self-harm, have made sense of their journey of help-seeking.
The aim of this research was to explore how young men, who have successfully accessed formal help for self-harm, understand their journey of help-seeking and how their experiences led them to continue to seek help after initial access. The research questions included the following:
Method
Research Design
A nonexperimental, descriptive design was selected for this study to enable exploration of the nature and defining features of young men’s experiences of seeking help. A qualitative methodology was chosen to expand on the existing quantitative “self-report” approaches, which have previously dominated the help-seeking literature. This study utilized in-depth semistructured interviews and sought to explore the lived experience of formal help-seeking for self-harm by young men.
Interpretative Phenomenological Analysis (IPA; Smith, 1996) was selected as the analytic paradigm for this study. IPA’s commitment to phenomenological enquiry allows the researcher to explore the meanings people make from the experiences they have lived through (Smith, Flowers, & Larkin, 2009). It attempts to gain insights into how a given person, in a given context, makes sense of a given phenomenon. In the present study, IPA allowed for an exploration of how young men make sense of their experiences of help-seeking. By utilizing an analytic approach that focused on subjective meaning making, this study offered a valuable contribution to the field of help-seeking research, which has previously attempted to measure if and why help is achieved, rather than considering the complex, individual processes of how help is sought.
Participants
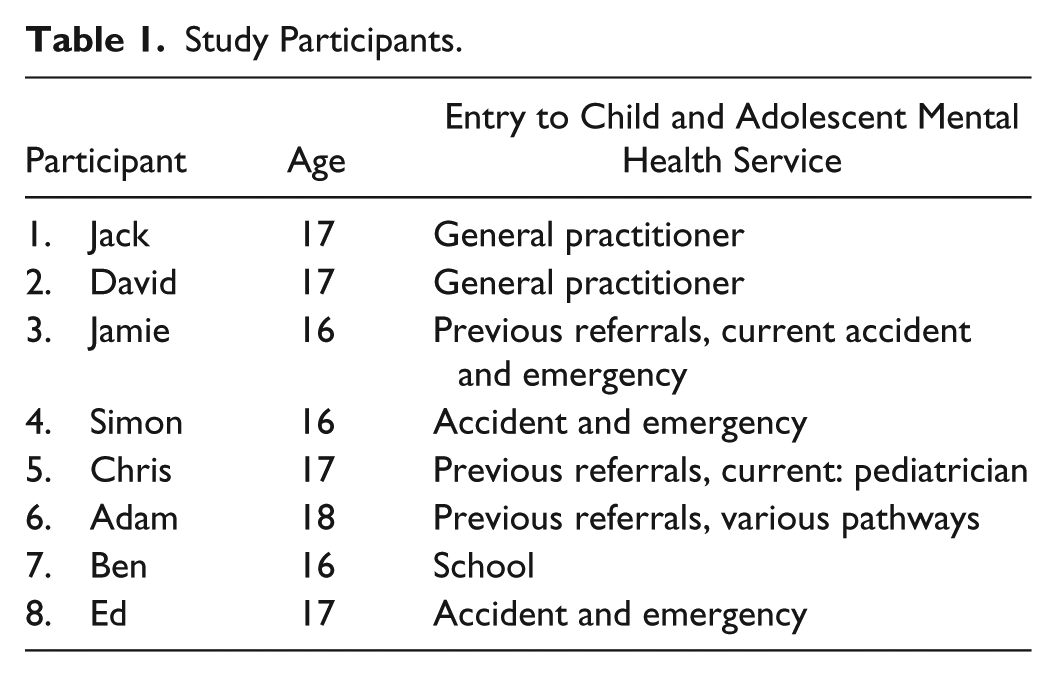
Criteria for inclusion to the project were as follows: male, 16 to 18 years, engaged with CAMHS for therapeutic intervention at time of recruitment and interview, self-harm (cutting, overdose, scratching, burning, strangulation, head banging, punching walls) is a key feature of referral to CAMHS, two or more episodes of self-harm in past 12 months. Exclusion criteria included severe anorexia, current acute episode of psychosis, and a learning disability that would impede capacity to comply with research requirements.
Participants were eight young men currently receiving care from CAMHS (see Table 1). The sample size selected for this project was within recommended guidelines for IPA studies, which utilize a concentrated focus on a small number of cases (Smith et al., 2009) to allow for carrying out depth interviews and analysis.
Study Participants.
Ethical Approval
A local NHS Research Ethics Committee granted full ethical approval for this study to take place. Research and development approval was also granted by the four NHS trusts that were involved in recruitment. The study was conducted in line with the code of ethics and conduct outlined by the British Psychological Society (2006; Health Professionals Council, 2009).
Recruitment
Participants were recruited from four National Health Service (NHS) CAMHS clinics across the south of England. Participants who met the inclusion criteria were identified by a named clinician at the recruitment site, and the participant information sheet was discussed with the young person at the end of their usual session. If the young person expressed an interest in the study and demonstrated that they clearly understood what their participation would involve, verbal consent to be contacted by the researcher was gained. Initial contact between researcher and young person took place via telephone where the purpose of the study and requirements for involvement were discussed once again. Once the young person demonstrated enough knowledge of the study to make an informed decision, a date for the interview was agreed at which point the consent form was filled out.
Interviews
Semistructured interviews were the chosen method of data collection for this project allowing for a discursive interaction between the participant and researcher. Interview schedules were developed to provide a loose framework for eliciting the rich accounts of how young men made sense of their journey of seeking help for self-harm. The preparation of a schedule was particularly helpful in this context given that the area of discussion (self-harm) was emotionally laden and thus needed to be sequenced and approached in a sensitive way. The questions were reviewed by two clinical psychologists experienced at working with young people who self-harm and a youth consultation group. This process was invaluable for considering ways to word questions. The interview schedule asked questions related to the young person’s help-seeking journey and included the following: when they first came to CAMHS, when you realized they needed help for their self-harm, things that helped them ask for help from informal sources (such as school, friends, parents, etc.) and from formal sources (such as CAMHS, Counseling service, A&E), what things got in the way of them asking for or receiving help, and about their overall experience of seeking help from CAMHS. The interviews lasted between 40 to 60 min and were digitally recorded, transcribed, and anonymized for analysis. Interviews took place over a period of 14 months.
Analysis
Once collected, data were subjected to Interpretative Phenomenological Analysis (Smith, 1996) following published guidelines in Smith et al. (2009). The authors suggest that, given the idiographic commitment, analysis should take place on a case by case basis and should progress through six stages:
Reading and re-reading: Repeated reading of the transcripts, while simultaneously listening to the audio-recording, took place to enable the researcher to become immersed in the data. Attention was paid to the most striking observations of the data, and these observations were noted down as a process of bracketing in an effort to suspend judgment and to enable focus on the participant’s idiographic account.
Initial noting: The researcher examined semantic content and language use, similarities, differences, echoes, amplifications, and contradictions in the participant’s narratives. Comments were made on a lefthand-side column of the transcript with different colors to represent different aspects of the analysis. For example, exploratory commenting took place in three parallel stages; descriptive comments (blue) had a clear phenomenological focus and focused on the participants’ explicit meaning, linguistic comments (green) focused on exploring the use of language by the participant, and finally, more interpretative noting, which involved engaging with the data at a more interrogative and conceptual level (red) took place.
Developing emergent themes: The hermeneutic cycle was particularly evident in this stage during which the data set of notes made during Stage 2 became the focus of analysis. The researcher attempted to identify emergent themes by mapping interrelationships, connections, and patterns. This involved focusing on discrete chunks of data, while remaining cognizant of what was learnt from the process of whole transcript coding. Emergent themes were noted in the lefthand column.
Searching for connections across themes: A list of all themes made on the transcript was printed out. Themes were then cut out and spread on a floor to move themes around. This provided a spatial representation of how themes relate to each other. The process of abstraction was used to aid identification of patterns and involved scanning each individual theme and identifying like with like. Similar themes were clustered together and were given a new theme title to represent a “super-ordinate theme.”
Moving to the next case: Given the idiographic commitment of IPA, to retain individuality, it was crucial to treat each case on an individual basis. Ideas from the previous interview were bracketed by noting assumptions and ideas developed from the analysis. Bracketing was used to inform the researchers of their own assumptions throughout the research process and to see how those interacted with the interpretive process rather than as a way of transcending them.
Looking for patterns: The final stage involved looking for patterns across cases. Each superordinate theme for each participant was cut out and spread on the floor to move around and consider links and similarities to establish “higher-order concepts.” Higher-order concepts were then listed, and example quotes were provided for each concept. Finally, recurrence of higher-order concepts was considered, and in line with recommendations from Smith et al. (2009), themes endorsed by half of the sample or more were retained as “over-arching themes” and included in the research write-up.
Quality Assurance
The process of data analysis was subjected to quality assurance practices recommended in Mays and Pope (2000). To assess analytic reliability, investigator triangulation took place. Two researchers (research supervisors) independently analyzed the same transcripts (for three cases) to assess the reliability of the data analysis. Their analyzed transcripts were then compared with the original transcript, analyzed by the main researcher, to check for selective attention and interpreter bias and to explore alternative explorations. On all six occasions (three transcripts each), themes and overarching themes were satisfactorily similar.
The role of prior assumptions and personal characteristics were reflected on and discussed with a research supervisor. In the present study, particular consideration was given to the gender difference between the researcher, who was female, and the participants, who were male, and the potential for this to influence the data. It was possible that experiences expressed within the interviews by the young men might be influenced by the gender of the researcher, and consideration was paid to whether this might have been enacted in the interviews. For example, the researcher was mindful that, in the context of talking to a female, the young men might have felt compelled toward promoting the more stereotypically dominant characteristics of masculinity (i.e., coping independently, not appearing weak).
The researcher approached this project with assumptions about, but not direct experience of, being a young man. These assumptions were, therefore, informed by personal and clinical experiences of interacting with young men and reading of literature within this area. Assumptions included that young men would have difficulty expressing their experience using spoken words and that they would be reluctant to share their intrapersonal world.
Refection on this process was undertaken by engaging in discussion with a male supervisor prior to and during data collection to identify any personal or intellectual biases on the part of the researcher. This supervisor also read and coded three of the original transcripts, which offered the opportunity for discussion about any likely biases within the young men’s narratives about their experience. A research diary was used during the process of data collection and analysis to note down any assumptions or observations that may have biased the data.
Results
While the journey of help-seeking was unique for each participant, four superordinate themes, that overarched participants’ individual experiences, emerged from the data: role of external adult in recognizing, normalizing, and initiating help-seeking; challenging and renegotiating perception of need for help and meaning behind this need; maintaining an independent self; and mechanisms of engagement. Table 2 provides examples of the superordinate themes and subthemes.
Superordinate Themes and Subthemes.
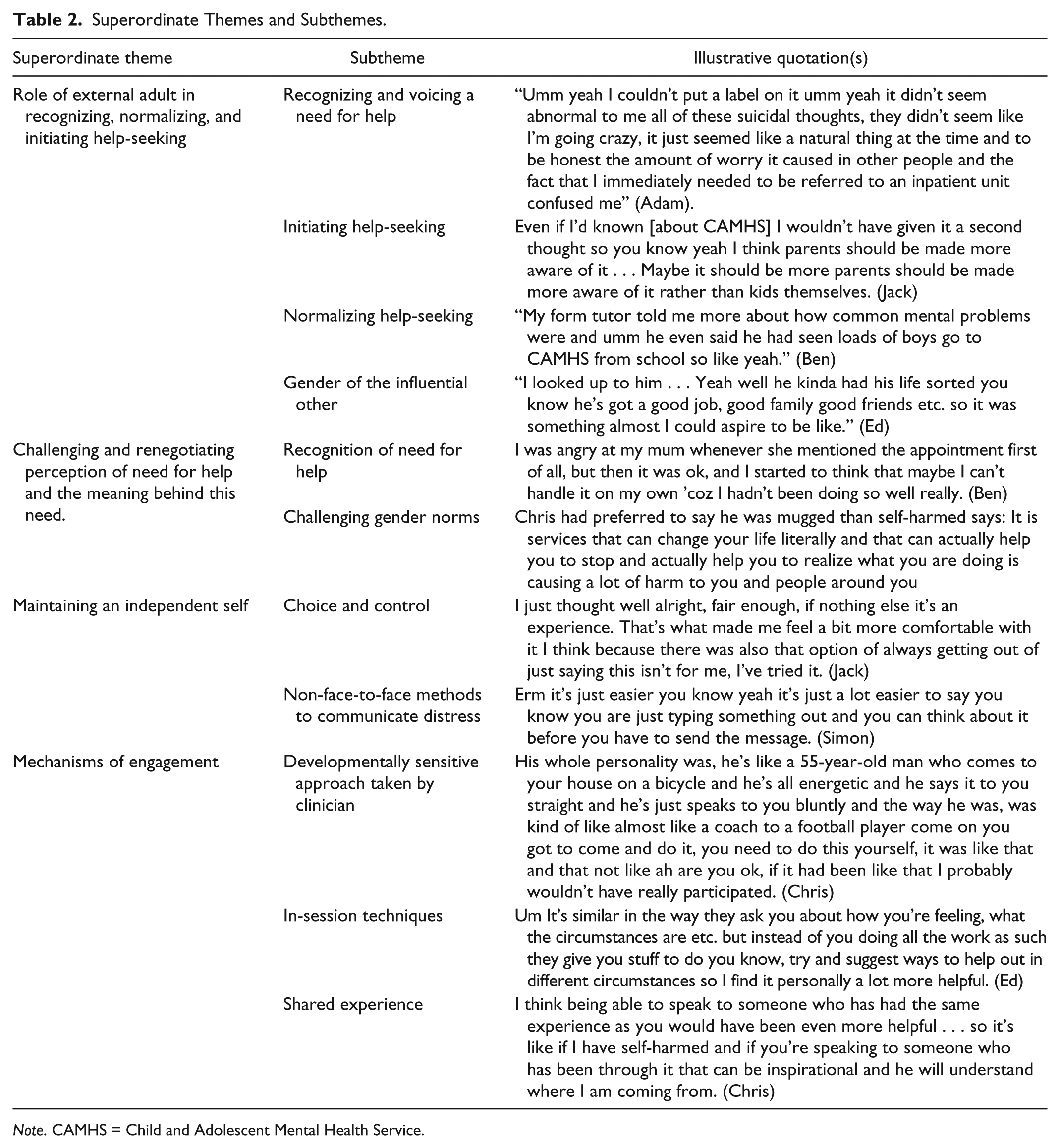
Note. CAMHS = Child and Adolescent Mental Health Service.
Theme 1: Role of External Adult in Recognizing, Normalizing, and Initiating Help-Seeking
The superordinate theme related to the role of external adults in enabling the young person to acknowledge the need for help and their role in initiating the process of help-seeking.
Recognizing and voicing a need for help
In all cases, initial recognition of need for help came from external sources such as parents, friends, or schoolteachers. It was evident that there was considerable confusion about whether their experiences of self-harm reflected “normal” behavior or “real” distress as Adam illustrates:
Umm yeah I couldn’t put a label on it umm yeah it didn’t seem abnormal to me all of these suicidal thoughts, they didn’t seem like I’m going crazy, it just seemed like a natural things at the time and to be honest the amount of worry it caused in other people and the fact that I immediately needed to be referred to an inpatient unit confused me.
In addition to failure to recognize need, comments made by three participants spoke to the difficulty in translating need into words and indicated that other people initiating conversations about their difficulties was a “relief.” For example, Jamie, who had taken multiple overdoses, offered an insight into his difficulty in vocalizing his troubles and the influence of others on making it possible:
Like at first I wasn’t going to tell my friends and I was always saying I was upset. . . I thought if they walk away they are not my true friends and if they stay they will not think they are any different. They helped by asking if something’s wrong.
Initiating help-seeking
Striving for independence and autonomy, a characteristic of the developmental stage of adolescence (Erikson, 1963), was strongly reflected in the interviews and was characterized by dominant themes of wanting to cope independently: “I like to sort things out for myself,” “I needed to do things myself and not rely so much on other people.” Nevertheless, these beliefs were contradicted in the young men’s actual help-seeking behaviors, which relied on external adult help to initiate help-seeking. The extract below draws our attention to this conflict and demonstrates Jack’s acknowledgment of the importance of his mother in helping him to access help, which starkly contrasts with his dominant narrative around wanting to solve [problems] myself and his suggestion that relying on others for help is considered to be weak.
Even if I’d known [about CAMHS] I wouldn’t have given it a second thought so you know yeah I think parents should be made more aware of it . . . Maybe it should be more parents should be made more aware of it rather than kids themselves.
While the majority of young men described an external influence for accessing help (parent or other influential adult), Ed’s narrative contrasted with the other young men in that his help-seeking was more internally motivated:
Well at the time I was in employment and it was effecting how I was working the way I was working and the way I was working died down quite a bit so I thought I want to continue working I got to sort myself out otherwise I will lose my job.
In addition to his different help-seeking practices, Ed was the only young person in the sample who was in full-time employment and not in education. It is possible that, while the education environment maintains a need for adult guidance and direction, the workplace environment fosters responsibility and autonomy. This observation might indicate that different lifestyle choices interact with developmental stages and changes the way that help may or may not be sought.
Normalizing help-seeking
The normalizing approach taken by external sources was particularly powerful. This subtheme spoke to concerns about stigma and illustrated the power of increasing awareness of the prevalence of suffering of young people, as Ben noted, “My form tutor told me more about how common mental problems were and umm he even said he had seen loads of boys go to CAMHS from school so like yeah.” Normalizing from a gender perspective was endorsed by many of the participants and reduced the sense of social isolation. For example, David, like the majority of participants, made inaccurate assumptions about the well-being of other young men in his school: “Yeah because everyone in my school was like that big kind of guy.” For David, when his GP provided an insight into the prevalence of help-seeking by young men, this offered an alternative perspective:
Ok so it sounds like you spoken to your mum and she spoke to the Doctor, what was it like going to see the Doctor?
It was fine really because you saw there was light like you can get through it.
Ok, so what helped about that process? Where did the light come from?
Just like knowing you were not the only one who went through it and that there were other people who had gone through it . . . they started talking about I’m not the only male.
Normalizing the experience of emotional difficulties from a gender perspective enabled David and the majority of participants to shift from holding a generalized and accepted image of young men as “tough” and able to “cope independently” toward the development of a multifaceted identity whereby masculinity can be coupled with emotional vulnerability and difficulty.
Adam, who had over 5 years of inpatient and outpatient CAMHS experiences and who did not share the group concerns of stigma about accessing services for mental illness offered a different insight into how his experiences had been normalized:
I mean I’ve never told anyone that I’m here but I wouldn’t have any problem I wouldn’t be embarrassed about it if it came up . . . there’s not much of a stigma anymore.
Why do you think that it, why do you think that’s changed?
Umm I mean the news is always telling us how sort of like depression is a really valid illness which you know is to be treated as seriously as a physical ailment umm yeah . . . my age group we have grown up learning how depression is such a serious thing and that all mental illness is a serious thing like mood disorders and schizophrenia and yeah so I don’t think if it did tell someone I don’t think there would be any sort of judgment or any sort of shame whatsoever.
Gender of the influential other
While only three participants had a male therapist, five young men indicated that their journey of help-seeking was positively influenced by having contact with a male in some way. Jack, who had been against accessing help when encouraged by his mother, changed his mind following an informal discussion with a male family friend: “I was probably, in hindsight, looking for some kind of male perspective.”
Despite its dominant reference, gender was not, on its own, as crucial as anticipated. Instead, participants’ narratives highlighted that gender was only considered influential when coupled with respect. Jack went on to say, “because he was a good friend of my dad’s I trusted him, his opinion.” Similarly, Ed’s description of his older friend highlights the respect he felt, “I looked up to him . . . Yeah well he kinda had his life sorted you know he’s got a good job, good family good friends etc. so it was something almost I could aspire to be like.”
David further endorsed this notion of being influenced by someone who he looked up to, although speaking hypothetically, “Like have a male model who has gone through it like at the other side, like a successful guy who has been through it.”
Theme 2: Challenging and Renegotiating Perception of Need for Help and the Meaning Behind This Need
In addition to the influence of external sources, there was evidence that the young men’s own internal influences played a crucial role. For example, each young man appeared to engage in an ongoing process of negotiating and renegotiating their need for help and the meaning behind this need.
Recognition of need for help
Illustrated in the three extracts below are participants’ dominant beliefs about being able to “handle” and “control” problems, which contrasted with eventual realization of the limits to their coping styles. This is highlighted by Ben:
I was angry at my mum whenever she mentioned the appointment first of all, but then it was ok and I started to think that maybe I can’t handle it on my own ’coz I hadn’t been doing so well really. Similarly, David reported, “I didn’t really think . . . I needed it, I thought I could control my emotions [but] my emotions are strong so it’s not always easy to control them.” Chris also demonstrated a shift in his perception of need: “I was a bit reluctant, then I thought that yeah, in this time I’ve tried to do it by myself I’ve not got any answers or got anywhere so clearly I do need some help.”
Challenging gender norms
Through the process of accessing and receiving help, participants’ displayed a shift away from the polarized position of “help-seeking is weak” to a more balanced position and in some cases a position of increased feelings of masculinity. For example, Chris, who explained that he would have preferred to tell his friends he had been mugged rather than own up to having self-harmed, for fear of this information compromising his “image” and “social acceptance,” changed his mind and noted,
It is services that can change your life literally and that can actually help you to stop and actually help you to realize what you are doing is causing a lot of harm to you and people around you.
This extract draws our attention to the way in which Chris, like a number of the participants, reframes help-seeking as a responsibility he has to others.
Theme 3: Maintaining an Independent Self
Inherent in participants’ narratives was a resistance to committing fully to the process of help-seeking. This was illustrated by participants employing strategies to establish some distance between them and the help-seeking process, possibly in an effort to avoid the associations with “patient” or “client” and to maintain their pre-therapy sense of developing self.
Choice and control
A number of participants exhibited internal processing strategies to maintain some level of choice and control, as Jack illustrated:
I just thought well alright, fair enough, if nothing else it’s an experience. That’s what made me feel a bit more comfortable with it I think because there was also that option of always getting out of just saying this isn’t for me, I’ve tried it.
Ed drew on his experience of others’ help-seeking to reassure himself that he could escape if he wanted to:
My friend was fed-up with the way the CAMHS worker was treating her and decided to leave, it is a voluntary service and if you don’t want to come here it’s completely up to you, they are not going to force you.
In addition to internal strategies for maintaining control, there was evidence that external sources also acknowledged the importance of handing back control to the young man to support his engagement. For example, Simon, who disclosed his overdose to a friend, was asked, “Is there anything you would not like me to mention?” by his friend’s mum prior to her disclosing his overdose to his parents. In this situation, in which Simon’s personal experiences faced exposure, he was given the opportunity to grasp some control over the process. This was possibly reflected in his later comment, “I know what will happen now, no one is going to try and lock you up because I told them that I am feeling like that.”
Non-face-to-face methods to communicate distress
For a number of participants, non-face-to-face methods of communication such as social networking or text messaging were used as a vehicle for maintaining some control over their communication of distress both in terms of accessing help and engaging in services. Simon, who was concerned that his disclosure would come as a shock as he believed that others perceived him to be “happy” and “fine,” highlighted the usefulness of a social network for enabling him to communicate his difficulties: “Erm it’s just easier you know yeah it’s just a lot easier to say you know you are just typing something out and you can think about it before you have to send the message.” This non-face-to-face approach, which enabled Simon to maintain some choice and control over his disclosure, was similarly recognized by Adam who noted,
The texting service that this place offers is useful . . . I recommend that I think it’s really helpful and it doesn’t have to be used it’s good to have that kind of safety net.
Theme 4: Mechanisms of Engagement
Given that none of the participants entered CAMHS entirely of their own volition and were, therefore, not the main stakeholders in the referral process, this might imply that their motivation to seek help and continue to engage with help was low. Having maintained their engagement in services, however, all participants offered an insight into what helped to keep them engaged.
Developmentally sensitive approach taken by clinician
All participants highlighted an appreciation for the relationship that developed between them and their clinician. In most instances, participants reported that the approach of their clinician was developmentally sensitive, scaffolding the development of a respectful and egalitarian partnership, possibly further breaking down the stigma associated with asking for help. For example, Chris likened his clinician to a “football coach” and noted,
His whole personality was, he’s like a 55-year-old man who comes to your house on a bicycle and he’s all energetic and he says it to you straight and he’s just speaks to you bluntly and the way he was kind of like almost like a coach to a football player come on you got to come and do it, you need to do this yourself, it was like that and that not like ah are you ok, if it had been like that I probably wouldn’t have really participated.
Similarly, Adam, who had experienced a number of different CAMHS teams due to having moved areas frequently, reflected on his diverse experiences of clinicians’ approaches,
Just where they treat you like an adult they don’t talk down to you, they talk to you as if they were talking to your parents—umm that’s been the most useful, I don’t know just no bullshit basically.
The appreciation of no bullshit was similarly reflected by Ed who summarized his clinician as, “He’s quite a sound guy, he’s very straight forward.”
In-session techniques
Young people in this study provided an insight into what they had found useful about their therapeutic experience. Two young men, who had previously accessed school and voluntary counseling services compared these experiences with their experience of CAMHS. Ed noted,
I did kind of have an idea in my head that it was just gonna be ah how does this make you feel . . . and upon going for my meeting it did turn out to be like that so I didn’t think that was particularly the best option for me so er a lot of the questions he was asking me I already knew the answers to myself and I didn’t see it progressing anywhere.
So is the approach of CAMHS, did it feel different to [counseling] or does it feel quite similar?
Um it’s similar in the way they ask you about how you’re feeling, what the circumstances are etc. but instead of you doing all the work as such they give you stuff to do you know, try and suggest ways to help out in different circumstances so I find it personally a lot more helpful.
There was a tendency for participants to privilege a practical, skill learning approach in therapy, opposed to reflection on their experiences. From a developmental perspective, this tendency may reflect their familiarity with goal-focused approaches inherent in the education system, a context within which they have all spent the majority of their formative years. Adam similarly endorsed an approach that had a practical focus in comparison with his experience of counseling, which he described as “flimsy” and “no direction,” “. . . I just wanted to work as it were and that’s why I like this service as well, because there are clear, firm objectives to work towards, set topics before each session and that.”
Shared experience
Experiencing emotional distress, in the context of beliefs about stigma and difficulty in vocalizing their experiences, can result in feelings of isolation. This was reflected by a number of young men who were unaware of how common it is to experience self-harm or how typical it is to need some external help. The extract below was typical of the beliefs of young men. Chris noted,
[it is] like really shocking to learn that that was something that was common but I don’t think there’s not many males that self-harm. It just doesn’t I don’t get it, they all seem, when you are in a group of boys, it’s almost like emotion doesn’t exist and then you can’t envision what they are doing in their private time, you think, well they must be like that all of the time so I think that is probably why.
Ed noted that talking to other people with similar experiences “slowly takes the bricks out of the wall [the] mental block you put up then eventually it wears away.” He indicated that shared experience was much more than simply helpful for normalizing experiences and made reference to the bigger picture. Chris similarly spoke to this theme and proposed that the usefulness of shared experience is learning not only about others experiences of self-harm but also about hearing their journey of recovery and gaining some hope and strength from this:
I think being able to speak to someone who has had the same experience as you would have been even more helpful . . . so it’s like if I have self-harmed and if you’re speaking to someone who has been through it that can be inspirational and he will understand where I am coming from.
Preliminary Model of Help-Seeking by Young Men Who Self-Harm
The experiences of help-seeking expressed by the young men in this study are synthesized into a graphical representation within Figure 1. This model depicts help-seeking as a complex process that takes place within two stages and is dependent on the presence and timing of specific influences. This model describes these two stages: as comprising initial access and ongoing engagement. Help-seeking was also described as determined by the presence and timing of specific external and internal influences.

Model of adolescent male help-seeking for self-harm.
The model proposes that there is a fine balance between external and internal factors that leads young men to seek help and then maintaining that engagement. The model emphasizes the role of external sources in “Recognising Need,” “Normalising Experience” and “Initiating Help-Seeking” within the process of facilitating help-seeking. The model also emphasizes the need to inform young people, and especially young men, from an early age about the incidence of mental health difficulties and for help-seeking to be talked about in keeping with gender norms.
In terms of external factors that maintain engagement, the quality and “fit” of the service, encompassing “Techniques” and “Clinician Approach” and the importance of it as a shared experience are seen as important facilitating factors. The internal factors influencing maintenance in engagement in this study were primarily connected to “Maintaining an Independent Self” and factors that enabled participants to have a sense of “Choice and Control.”
Discussion
This study explored how young men make meaning of their decision to seek help from CAMHS, including the factors that facilitated their decision, and how they experienced the help they received. Help-seeking was described as a journey of two stages: (a) initial access and (b) ongoing engagement. This, therefore, builds on traditional models that assume help-seeking is achieved once entry into services has occurred. Help-seeking was also described as determined by the presence and timing of specific external and internal influences, (Figure 1). Again, this builds on traditional models of help-seeking that privilege either external or internal influences.
Links to Previous Research and Theory
Previous models of help-seeking
The present study both supports and extends previous conceptualizations of help-seeking. Similarly, to the NEM-R (Costello et al., 1998), which emphasizes external influences in help-seeking, the present study highlights the influence of the young persons’ network (parents, peers, and school) in identifying need, deciding a plan of action, and supporting access to services. Furthermore, similarly to the COA (Biddle et al., 2007), in which the cognitive processes (attitudes and beliefs) of the individual help-seeker is central to determining help-seeking, the current model highlights the impact of “internal influences” in accessing and engaging in help.
The present study goes on to extend this work and demonstrates that, for a cohort of young men who self-harm, help-seeking was predicated on integrating both “external influences” and “individual influences” and finding a balance between the two. For example, while young men relied on gentle guidance from external sources, they simultaneously engaged in strategies to maintain a sense of independence (i.e., acknowledging that their participation in services is voluntary). This consequently resulted in them changing their perspective and renegotiating their need for help and the meaning of help-seeking (“I probably wanted for someone to help me a little bit in the end”). This process is typical of the developmental stage of adolescence, during which a young person oscillates between striving for independence and autonomy to explore new roles and identities, and a continued need for guidance and support from influential others (Erikson, 1963).
Promoting engagement
This study acknowledged the fundamental need to learn about factors that help to retain young people who self-harm in services given their high rates of drop-out (Ougrin & Latif, 2011). Participants identified influential factors including their clinician fostering a developmentally sensitive relationship with them; being treated as equal and being given control and choice. These findings support recommendations made in a recent study by Green, Wisdom, Wolfe, and Firemark (2012), which considered strategies for engaging youths in treatment and also support recommendations from a literature review into factors that motivate and engage suicidal youth in therapeutic interventions (Daniel & Goldston, 2009).
The CAMHS Review (Department for Children, Schools and Families (DCSF) & DH, 2008) also acknowledges the importance of paying consideration to the developmental stage of those entering services and, similarly to the present study, recommended that services enable the young person to feel in control. This review, however, highlighted a number of recommendations aimed at fostering a sense of control that were not recognized directly by participants in the present study, including involving young people in their own treatment and care planning. This is further reflected in the DH’s “You’re Welcome” quality criteria (DH, 2011) that set out principles to help health services become young people friendly.
Stigma
In the present study, participants indicated that help-seeking presented a challenge to the gender ideal of masculinity and demonstrated evidence of self-stigma (i.e., “relying on others for help is weak”). While this supports an abundance of literature in the area of adult male help-seeking and stigma (Shepherd & Rickard, 2012; Vogel, Heimerdinger-Edwards, Hammer, & Hubbard, 2011), the present study adds to the limited research considering late adolescent male’s accounts of stigma and help-seeking. This is important since there may be qualitative differences between the experience of stigma for adults and for adolescents given their different developmental stages. Kranke, Floersch, Kranke, and Munson (2011) suggest that, while adults are most concerned by the impact of stigma on social status, jobs, and significant relationships, adolescents, who are in the thralls of the complex task of identity development, wish to protect their developing sense of self and may feel increasingly threatened by the possibility that who they are could become defined by their current experiences of distress and need for external help.
Gender-typical beliefs surrounding masculinity (the need to be self-sufficient and cope independently) seemed to result in the young men developing a higher threshold for perceived need for help. It is possible, therefore, that for young men in the present study, the influence of having external sources model concern and initiate help-seeking eased the internal pressure of maintaining this stereotype.
The factors that helped challenge barriers for young men in the present study included having their experiences normalized by external sources and being offered practical, skills-building approaches with clear objectives. This might reflect recommendations by Hammer and Vogel (2010) who developed a male-sensitive brochure to promote therapy by highlighting approaches that are considered more compatible with traditional gender roles such as “strategy for attacking,” “solution-focused,” “cost-effective,” and “client-directed team effort” (p. 301).
Implications
To effectively translate this research into practice, approaches that aim to facilitate help-seeking and engagement should balance consideration of internal and external influences.
Facilitating help-seeking: External
The role of external sources in “Recognising Need,” “Normalising Experience,” and “Initiating Help-Seeking” was highlighted in this study. Educating universal services and parents in recognizing emotional distress and determining need for help is crucial. CAMHS teams are well placed to offer training and workshops to a wide range of professionals within universal services (school, nursing, GP, social work, looked after, youth justice, pediatrics). This approach should aim to educate about recognizing emotional distress and self-harm, normalizing experiences, and managing concerns around risk.
CAMHS services may also support professionals and parents to begin the help-seeking process by offering a telephone consultation/advice line. This could provide informal support in assessing risk and providing proactive recommendations for supporting young people, prior to specialist services involvement.
The media is a useful and accessible platform from which parents can be educated about best-practice procedures for supporting emotional well-being and managing self-harm. In addition to educational websites, an interactive online advice service may offer parents an informal consultation process from which they can gather information, support, and signposting. This could be offered as an add-on to existing counseling services on offer to young people.
Facilitating help-seeking: Internal
Paralleling the need for education, but particularly with the aim to reduce stigma, this study highlighted the need to inform young people and especially young men, from an early age about the incidence of mental health difficulties and for help-seeking to be talked about in keeping with gender norms. Young Minds (2014) identify that mental health education should be included alongside physical health education in the curriculum, and schools could consider employing a full-time dedicated mental health liaison advocate who takes a lead emotional well-being. This may enable young people to recognize the need for help sooner and encourage more informal help-seeking practices such as using self-help materials, peer support, and attending after school drop-in sessions.
The present study highlights young people’s reticence to share their internal world due to concern about how they might be perceived. This supports the already popular and growing area of “on-line counselling” (Street, 2013) and promotes the value of further developing online mental health resources including websites and apps to educate and support self-care (Children and Young People’s Mental Health Taskforce, 2015).
Maintaining engagement: External
The key external factors influencing maintenance of engagement, described by participants in this study, were the quality and “fit” of the service, encompassing “Techniques” and “Clinician Approach.” First, the quality of the therapeutic relationship is frequently highlighted as counting for the largest variance in subsequent treatment engagement (Oruche, Downs, Holloway, Draucker, & Aalsma, 2014). Supporting clinicians to develop their interpersonal approach should therefore be a priority. Findings from this study parallel feedback from a consultation with young people who indicate that mental health professionals should balance a professional approach with an appropriate level of informality (friendly, appropriate language, a degree of flexibility; Young Minds, 2014). In additional to training clinicians, monitoring tools could be used routinely to evaluate the effectiveness of the clinical approach. The Session Rating Scale (SRS; Miller, Duncan, & Johnson, 2002) uses real-time feedback and has been highlighted as an effective tool to empower clients, promote collaboration, and ultimately improving outcomes (Lambert, 2005).
In speaking about their favored therapeutic techniques, participants from the present study highlighted approaches that were goal orientated and skill focused, preferences that may somewhat reflect developmental and gender differences. It is important that all professionals working therapeutically within CAMHS services receive appropriate supervision and training, and that this should encompass developmental and gender considerations. In the context of “CAMHS Service Transformation,” one aspect of which is to improve the range and choice of therapeutic interventions on offer by providing training for the workforce (NHS England, 2015), it will be important for training to encompass consideration of gender and also developmental contexts.
Having a “Shared Experience” was identified by participants as influential in their help-seeking. This reflects a movement toward sharing personal stories of mental health difficulties, and journeys of recovery over regulated “blogging” sites (Time to Change, https://www.time-to-change.org.uk/). Signposting young people to these sites may help address feelings of isolation and negative beliefs around help-seeking.
Maintaining engagement: Internal
The internal factors influencing maintenance in engagement in this study were primarily connected to “Maintaining an Independent Self” and factors that enabled participants to have a sense of “Choice and Control.” As has been indicated elsewhere (DCSF & DH, 2008), this can be achieved by young people being at the core of their care planning. In addition to this, participants in the present study spoke of seeking and accessing help as a journey of “changing and renegotiating need for help.” Services could ensure that treatment reviews are planned at regular intervals to take account of the changing landscape for the developing client.
Limitations and Future Directions
Sampling
Consideration should be paid to the sampling procedure selected for this study. First, the small sample size in this study was necessary to enable an in-depth exploration of participants’ experiences of help-seeking for self-harm. Nevertheless, this limits the ability to generalize these findings to a wider population, and we cannot assume that the experiences of the young men in this study are representative of young men who self-harm and seek help in general. For example, this study only recruited participants who were attending CAMHS settings and, therefore, limited consideration of whether the help-seeking experiences expressed in this study reflect experiences of help-seeking from other sources including voluntary counseling services.
Future research in this area would be beneficial to ascertain whether the journey of help-seeking by young men who self-harm differs depending on where help is sought. In addition to this, recruiting young men aged 16 to 18 limited consideration of potential differences in help-seeking across the stages of adolescence. Future research may consider whether adolescence, although classified as one distinct developmental stage, affects help-seeking differentially depending on where young people fall, that is, “young adolescence” (13-15) or “old adolescence” (16-19).
Finally, while the model of help-seeking described in this study is developed based on the experiences of young men who self-harm, it is unclear whether this model is specific to self-harm or whether it describes a process of help-seeking by young men more generally. Future research might consider replicating this study with non-self-harming young men to determine its specificity to self-harm.
Data collection and analysis
While steps were taken in this study to ensure reliability of the Interpretive Phenomenological Analytic approach, a number of possible limitations of this methodology should be highlighted. First, data collection took place via semistructured interviews. This strategy may have reduced the opportunity to gather accurate and detailed accounts of participants’ experiences given the evidence that young men may have difficulty with verbalizing their experiences (Jordan et al., 2012). In addition, given that participants were considered to be in the adolescent stage of identity development, the experiences they chose to verbalize may have been biased toward accounts that they perceived to be more socially acceptable.
Finally, given that the researchers’ interpretation is central to the IPA process, steps were taken to acknowledge and control for the potential impact on data collection and analysis (see “Method” section). Despite this, however, there may have been a tendency for results to be biased toward reflecting the researchers’ beliefs and may have resulted in missing out key features of the participants’ narratives. To account for these limitations, this study may have benefited from returning to participants to check out their agreement with interpretations made.
Conclusion
This study attempted to consider, in depth, how young men aged 16 to 18 experience the journey of help-seeking following self-harm. It is also attempted to conceptualize help-seeking as a process of two stages involving access and engagement. Despite its limitations, this study suggests that young men’s help-seeking for self-harm is facilitated by a balance of external influences (parents, teachers, peers, and mental health clinicians) and internal influences (the young person’s own cognitive processes). This has important implications and points to the need for the provision of education in the area of self-harm and help-seeking. For parents, peers, and teachers, this may include provision of information about how to identify need for help (in young people) and ways to facilitate access to services. For commissioners, service developers, and clinicians, this may include provision of guidelines to help adapt services to meet the complex developmental needs of young men, necessary for facilitating continued engagement in services.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.