
Abstract
In literature, there are many instruments for measuring the work–family conflict (W-F-C). The Work–Family Conflict Scale (WFCS) is one of the most used tools. This study aimed to evaluate its psychometric properties on a sample of 684 Italian workers (42.1% males, 57.9% females, mean age = 45.51 ± 10.91). We also evaluated if there were some demographic differences in the W-F-C, with relation to gender, the presence of children, and the kind of job (i.e., medical doctors and other health professionals, teachers and researchers, employees, manual workers, self-employed workers). We found that the Italian WFCS has good psychometric properties. Moreover, contrary to our hypotheses, males experience higher W-F-C than females, and the lowest level of W-F-C characterize doctors and other health professionals. Manual workers and self-employed workers seem to be the two job categories that experience the highest level of W-F-C.
Introduction
In literature, there has been an increasing interest on the interface and the reciprocal impact between work and family. This might be due to some work-related changes, such as dual-earning partners, the greater participation of women to the workforce, and a blurring of gender roles (Alby, Fatigante, & Zucchermaglio, 2014).
From one perspective, scholars pointed out some positive effects of combining work and family roles (i.e., enrichment, enhancement, and facilitation), and they highlighted that the balance between the two domains entails a partners’ sharing and hence the opportunity to realize their own roles in both the work and family domains (Ferguson, Carlson, Zivnuska, & Whitten, 2012; Greenhaus & Powell, 2006). From the other perspective, an extensive research area focused on the work–family conflict (W-F-C), namely an inter-role conflict that may have many negative outcomes for the individuals, but also their families and their organizations (Greenhaus & Beutell, 1985).
The present study deals with the W-F-C. More specifically, we aim to contribute to the Italian validation of the Work–Family Conflict Scale (WFCS; Carlson, Kacmar, & William, 2000), because it is one of the most used instruments for evaluating the W-F-C.
Work–Family Conflict (W-F-C)
Work and family are the two most important life domains. While some scholars argued that the functionality of each area depends only by its internal situation (Amstad, Meier, Fasel, Elfering, & Semmer, 2011), others highlighted that these two life domains are interdependent. More specifically, they proposed the spillover effect: attitudes, emotions, and behaviors established in one domain flow into the other (Edwards & Rothbard, 2000). However, there is a positive, as well a negative, spillover. In the first case, the engagement in one of the two roles allows transferring positive experiences, mood, and competences to the other domain. Also, it compensates the negative experiences lived in the other domain. Then, it enhances its positive functioning (Greenhaus & Powell, 2006; Maeran, Pitarelli, & Cangiano, 2013). With regard to the negative spillover, the engagement in one of the two roles is harmful to the other, and it is associated with some negative outcomes, such as family dissatisfaction, difficulties at work, work dissatisfaction, and higher distress (Erdamar & Demirel, 2014; Fischer, Zvonkovic, Juergens, Engler, & Frederick, 2015). In this second case, scholars used the term W-F-C, which indicates a form of inter-role conflict: work and family role pressures are mutually incompatible in some respect (Greenhaus & Beutell, 1985).
Greenhaus and Beutell (1985) defined three types of W-F-C: (a) time-based conflict, or the time required by one of the two domains prevents the possibility to fulfill the other role’s expectations; (b) strain-based conflict, in which strain, fatigue, tension, anxiety, or dissatisfaction in one domain affects the performance in the other one; and (c) behavior-based conflict, where specific behaviors, expectations, or rules required by one role are incompatible with those needed for the other role. They also theorized the bidirectionality of the W-F-C, distinguishing between work-to-family conflict (WFC) and family-to-work conflict (FWC). In the WFC, the persons have some difficulties at work that affect their functioning at home; in contrast, in the FWC, their functionality at work is impaired due to some issues experienced at home. Then, Carlson et al. (2000), integrated the three kinds of W-F-C with its two directions (i.e., WFC and FWC), proposing the following six types of W-F-C: time-based work interference with family (time-based WIF), time-based family interference with work (time-based FIW), strain-based work interference with family (strain-based WIF), strain-based family interference with work (strain-based FIW), behavioral-based work interference with family (behavior-based WIF), and behavioral-based family interference with work (behavior-based FIW).
It is important to study the W-F-C because literature shows many negative outcomes associated with it on both the person and his or her family and organization. The W-F-C is harmful to the individual’s mental and physical health (Panatik, Badri, Rajab, Rahman, & Shah, 2011), for the quality of his or her marital and familial relationships, and for the satisfaction of his or her partner and family (Carroll, Hill, Yorgason, Larson, & Sandberg, 2013). It has a negative impact also on the organization, as it may lead to a decrease in productivity, commitment, and job satisfaction, and an increase in absenteeism and turnover (Ahmad, 2008; Ahmed, 2014).
Moreover, it is important analyzing moderating factors of W-F-C. Concerning sociodemographic characteristics, gender differences have been extensively investigated (Aycan & Eskin, 2005; van Veldhoven & Beijer, 2012). Men and women have to manage their time and energies to distribute them among the various activities required by both work and family roles (Dhanabhakyam & Malarvizhi, 2014). The more substantial familial responsibilities of women and the greater emphasis of men on their work roles (Alby et al., 2014) seem to be associated with the higher levels of W-F-C in females than in males (Cinamon, 2006; Leineweber, Baltzer, Magnusson Hanson, & Westerlund, 2012; Todesco, 2013). Kinnunen, Geurts, and Mauno (2004) found, through a longitudinal study, that W-F-C in women predicts job dissatisfaction, parental distress, and psychological stress symptoms; instead, for men, the W-F-C is predicted by marital dissatisfaction, parental distress, and psychological and physical stress symptoms. Moreover, Aycan and Eskin (2005) observed a gender difference for the effects of social support on W-F-C: for women, spousal support is critical; for men, both marital and organizational supports are important. However, some scholars outlined that gender differences are poor predictive factors of W-F-C (Byron, 2005); moreover, Colombo and Ghislieri (2008) found that work interference with family life is perceived similarly by women and men.
Another moderating factor is related to occupational types. Dierdorff and Ellington (2008) suggested that different levels of W-F-C between workers may be attributable to the specific characteristics of their jobs. Roche and Haar (2010), in managers, observed a negative association between autonomy competence and relatedness and both WFC and FWC conflict. Concerning the interrelation between occupational types and gender, female teachers and grocery and drug store workers experience higher W-F-C than males with the same job (Erdamar & Demirel, 2014; Maume & Sebastian, 2012); moreover, female academic scientists express more WFC and FWC then men (Fox, Fonseca, & Bao, 2011). However, Maeran et al. (2013) noticed that their teacher sample (almost all females) expressed only moderate W-F-C. Focusing on women nurses, Grzywacz, Frone, Brewer, and Kovner (2006) found more prevalence of WFC especially in those who work many hours in a week, and they pointed out that having young children is related to higher FWC. Moreover, Kunst et al. (2014) highlighted that WFC in nurses seems to be due to their shift patterns (day and evening, night).
Measurement of the W-F-C
Literature offers many instruments for measuring different aspects of the W-F-C. Often, these tools evaluate the respondents’ perception of their W-F-C, and there are both ad hoc (e.g., Moore, Grunberg, & Krause, 2014) and validated scales.
Between the validated scales, some assess the work–life balance (Work–Life Balance Scale; Hayman, 2005) or cognitive aspects, such as the employees’ expectations about either W-F-C and work–family enrichment (Work–Family Balance Scale; Zhang et al., 2012) or irrational and rational cognitions related to both WFC and FWC (Work–Family Conflict Cognitions Questionnaire by Buligaa & Turliuca, 2014; cited in Turliuca & Buligaa, 2014). There are also instruments that focus on the negative and positive work-to-family and family-to-work spillovers (Work–Family Interface Scale; Curbow, McDonnell, Spratt, Griffin, & Agnew, 2003) and tools that measure instead the positive and enriching effects of work–family roles, the time-based W-F-C, and the strain-based W-F-C (Work–Family Relations Questionnaire; Vieira, Àvila, & Matos, 2012). There are also specific tools related to enrichment/enhancement only (18-item Work–Family Enrichment Scale; Carlson, Kacmar, Wayne, & Grzywacz, 2006) or conflict only, such as the scale used by Wiese, Seiger, Schmid, and Freund (2010) that is derived from an instrument developed by Carlson and Frone (2003).
About comprehensive tools of W-F-C, there are daily measures, such as that used by Ilies et al. (2007), which requires reporting each evening the W-F-C experienced during the day by answering to four items. However, there are also validated scales that evaluate the two directions of the W-F-C (i.e., WFC and FWC), such as the 10-item scale of Netemeyer, Boles, and McMurrian (1996) and the 14-item Inventory of Work–Family Conflict (Greenhaus, Callanan, & Godshalk, 2000). Finally, there are also instruments assessing the three forms of the W-F-C (i.e., time-based conflict, strain-based conflict, and behavioral-based conflict), as the scale by Stephens and Sommer (1996).
As we can see from this short review of instruments, there are many tools to use for measuring W-F-C. However, the WFCS by Carlson et al. (2000) is the most comprehensive instrument, because it is a multidimensional measure that assesses both the directions of the W-F-C considering the three different forms of conflict (for a total of six types of W-F-C). More specifically, the WFCS is an 18-item instrument that evaluates each kind of W-F-C through three items.
Adkins and Premeaux (2012) used the WFCS adapting the time- and strain-based scales for the roles of spouse, parent, home care, and leisure. So, they considered the following: time-based work–spouse conflict, time-based spouse–work conflict, strain-based work–spouse conflict and strain-based spouse–work conflict. Three parallel scales measure the conflict between the role demands of work and parent, work and home care, and work and leisure.
The Present Study
As outlined above, there are many instruments for measuring the W-F-C, given its recognized importance for the workers’ well-being. The WFCS (Carlson et al., 2000) is one of the most used instruments, and its main merit is its multidimensional nature. There is not yet an Italian validation of the WFCS. Hence, we aimed to contribute to its Italian validation through the evaluation of the factor structure and the psychometric properties of the WFCS on a sample of Italian workers characterized by different jobs (most of them are teachers or researchers, clerks or employees, and doctor or other health professionals). We hypothesized that (a) the WFCS has the better fit for the six-factor model, in line with Carlson et al. (2000); (b) the WFCS six scales have good internal reliability, as well as the WFCS total score; (c) the WFCS has good divergent validity, as analyzed by means of the correlation between the WFCS and the Dyadic–Familial Relationship Satisfaction Scale (DFRS; Raffagnino & Matera, 2015). The DFRS is an instrument designed for evaluating the satisfaction with the partner and the family. Hence, it assesses a positive dimension concerning family life. Instead, the WFCS measures a negative aspect concerning family life. In line with this, Carroll et al. (2013) showed that the W-F-C negatively impacts the quality of the marital and familial relationships, as well as the satisfaction with the partner and family.
Finally, we also evaluated if there are some demographic differences in the W-F-C, as evaluated by means of the WFCS, in particular concerning gender, job, and the presence of sons or daughters in the family. More specifically, we hypothesized that (d) Italian women experience higher W-F-C than men, as in Italy females have higher commitment in family roles than males (Istat, 2010), and in line with international literature highlighting such a gender asymmetry (e.g., Alby et al., 2014; Leineweber et al., 2012); (e) people with children experience higher levels of W-F-C than people without children, given that parenthood is a challenging and stressful life phase (e.g., Ford, Heinen, & Langkamer, 2007; Loscalzo, Giannini, Contena, Gori, & Benvenuti, 2015); (f) health professionals report higher levels of work-to-family conflict (WFC) than other workers due to the higher level of stress that many studies observed in this job (e.g., Canadas-De la Fuente et al., 2015; Kheiraoui, Gualano, Mannocci, Boccia, & La Torre, 2012; Morse, Saylers, Rollins, Monroe-DeVita, & Pfahler, 2012).
We believe that the WFCS could be a useful screening instrument to use for both health prevention and clinical aims because it could contribute to measuring how the interventions are effective in improving the way in which people deal with the conflicting roles in their work and family domains.
Method
Participants
The participants were 684 adults (42.1% males, 57.9% females), aged between 20 and 75 years (M = 45.51 ± 10.91). Almost all of them were of Italian origin (98%) and of Catholic religion (78.1%; the 18.8% of the participants did not provide such information). Moreover, 56.7% lived in Central Italy, 42.6% in South Italy, and only a few in North Italy (0.8%). As regard to their level of education, most had attained a secondary school education (45.5%) or held a bachelor degree (37.6%). With regard to their socioeconomic status (SES), the majority of participants (62.6%) reported having a medium SES. Most of the participants worked as medical doctors or other health professionals (31.1%), teachers or researchers (22.6%), or employees (18.5%). Most of them were married (73.4%), cohabited with their partner even if they were not married (15.7%), or were engaged (2.9%). A lower percentage were either separated or divorced (2.8%) or single (5.1%). Finally, while there were participants without children (26.7%), there were participants with one child (27%), two children (36%), three or more children (9.3%), and a few who were going to become parents (1.1%).
Materials
WFCS
We administered our Italian translation of the WFCS (Carlson et al., 2000), which has been verified by means of a back-translation. It is a self-report instrument that comprehends 18 items on a Likert-type scale ranging from 1 (completely disagree) to 5 (completely agree). The items measure the six dimensions of the W-F-C, which arise from the integration of the three forms of W-F-C (time-based, strain-based, behavioral-based) and its two directions (Work Interference With Family, Family Interference With Work): time-based WIF, time-based FIW, strain-based WIF, strain-based FIW, behavior-based WIF, and behavior-based FIW.
DFRS
The participants filled out the Dyadic-Familial Relationship Satisfaction Scale (DFRS; Raffagnino & Matera, 2015). It is a 14-item self-report instrument, and it evaluates two dimensions: Dyadic Relationship Satisfaction (nine items) and Familial Relationship Satisfaction (five items). The items are on a 5-point Likert-type scale (0 = not satisfied at all; 4 = completely satisfied).
Regarding the Dyadic Relationship Satisfaction scale, it evaluates some domains such as partner support, agreement, and sharing. A sample item is “How much I am satisfied with the way in which my desires and needs are fulfilled within my current relationship.” For the Familial Relationship Satisfaction scale, there are two items regarding child management and education (which are filled only by couples with children) and three items regarding house management (which are filled only by couples that cohabit). An item is “How much I am satisfied with the management of children.”
The internal consistency of the two subscales is high (α = .93 and .88, for the Dyadic and the Familial Satisfaction subscales respectively).
Procedure
The participants constitute a convenience sample, as they took part in the study on a voluntary basis. We recruited them through a direct phone call or the collaboration of the directors of some organizations.
The participants signed a consent form which informed them of the purpose of the study and the confidential nature of the data. Then, they gave some demographic information (i.e., gender, age, education level, the city of residence, job, SES, and relationship status) and filled the WFCS and the DFRS.
Data Analysis
We conducted the analyses through the statistical softwares SPSS.20 and AMOS.20. First, we calculated the descriptive statistics of the WFCS. Hence, we tested the factorial structure of the WFCS by means of four confirmatory factor analyses (CFAs; maximum likelihood estimation) to compare the models tested by Carlson et al. (2000). To evaluate the goodness of fit of the models, we made reference to the following indexes and cut-off scores: the χ2/df ratio, which indicates a good fit if it is less than 3 (Byrne, 2001); the goodness-of-fit index (GFI), the comparative fit index (CFI), and Tucker–Lewis index (TLI), which have the same cut-off values: <.90, lack of fit; .90 to .95, good fit; and >.95, excellent fit (Hu & Bentler, 1999); and the root mean square error of approximation (RMSEA), whose cut-off values are: <.05, excellent fit, and .05 to .08, acceptable fit (Reeve et al., 2007).
Then, we evaluated the reliability of the subscales by calculating the Cronbach’s alpha, and we analyzed the discriminant validity of the test using the Pearson correlation coefficient between the WFCS subscales and total score and the two DFRS subscales.
Finally, aiming to assess differences on the WFCS total and subscales scores between (a) males and females, (b) people with or without children, and (c) different kind of jobs, we carried out three multivariate analyses of variance (MANOVAs; followed by a Bonferroni post hoc analysis for examining job-related differences).
Results
Descriptive Statistics
Table 1 shows the average score for each item of the WFCS (referring to the six subscales presented by Carlson et al., 2000), as well as skewness and kurtosis values, highlighting how the average values range between 1.70 and 2.71.
Descriptive Statistics (N = 648).

Note. WFCS = Work–Family Conflict Scale.
CFA
We compared the four models, which were tested by Carlson et al. (2000), to verify if the six-factor model shows the best fit to the Italian data too. More specifically, the six-factor model comprehends six factors, which correspond to the six categories of W-F-C that arises by crossing the three forms of W-F-C (i.e., time, strain, and behavior) with its two directions (i.e., WIF and FIW). The three-factor model, instead, represents the three form of W-F-C collapsed across direction. The two-factor model represents the two directions of W-F-C collapsed across the form. Finally, the one-factor model comprehends one factor only, and it represents a general W-F-C perspective.
In line with the original version, the six-factor model is the best one and the values of factor correlation range between .44 and .92 (see Table 2 for the values of the fit indexes of the four models, and Figure 1 for a graphical representation of the six-factor model).
Fit Indexes of the Four WFCS Models (N = 648).
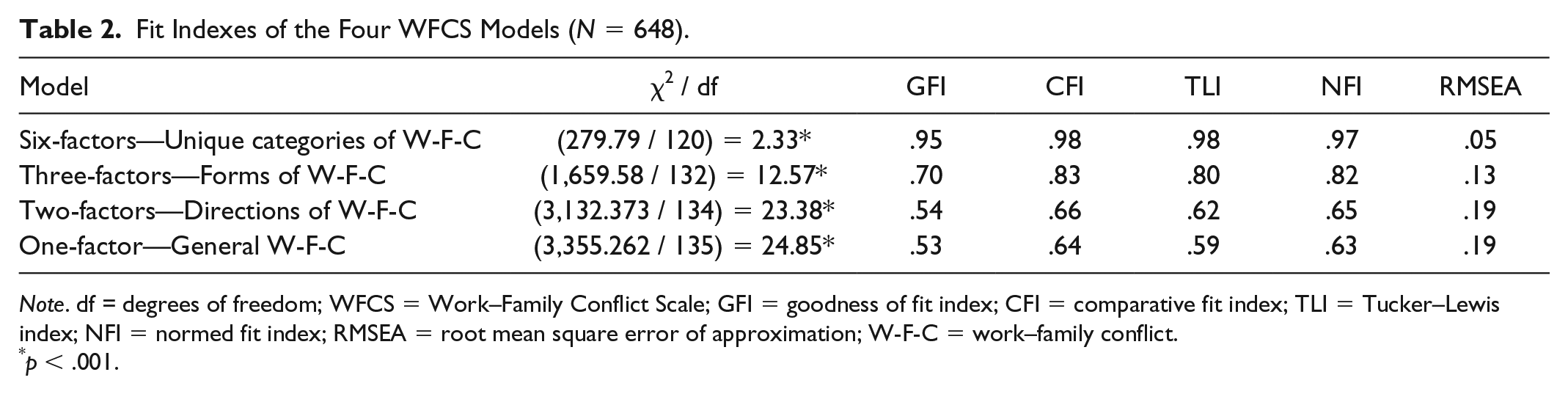
Note. df = degrees of freedom; WFCS = Work–Family Conflict Scale; GFI = goodness of fit index; CFI = comparative fit index; TLI = Tucker–Lewis index; NFI = normed fit index; RMSEA = root mean square error of approximation; W-F-C = work–family conflict.
p < .001.

Six-factor model of the Work–Family Conflict Scale (N = 684).
Reliability and Discriminant Validity
The values of the Cronbach’s alpha are good for all the six scales of the test and the total score. More specifically, the values are the following: time-based WIF (α = .89), time-based FIW (α = .86), strain-based WIF (α = .86), strain-based FIW (α = .88), behavioral-based WIF (α = .86), behavioral-based FIW (α = .94), and total score (α = .94).
To assess the discriminant validity of the WFCS, we calculated the correlations between the WFCS subscales and its total score and the two DFRS scales, namely Dyadic Relationship Satisfaction and Familial Relationship Satisfaction. The values of correlation are negative, as expected, though they are low: r values range between –.01 and –.15. Also, the negative correlation is statistically significant only for the correlation between the DFRS Dyadic Relationship Satisfaction scale and the WFCS total score (r = −.10, p = .02), the WFCS strain-based FIW (r = −.15, p < .001), behavior-based WIF (r = −.12, p = .01), and the behavior-based FIW (r = −.08, p = .04). Finally, the DFRS Familial Relationship Satisfaction scale has a statistically significant correlation with the WFCS behavior-based WIF scale only (r = −.10, p = .05).
Demographic Differences in W-F-C
We evaluated through three MANOVAs if there are demographic-related differences in the W-F-C, as evaluated using the total score and the six subscales of the WFCS as dependent variables.
As far as concern gender, the multivariate tests showed that it has a statistically significant effect, F(7, 640) = 2.73, p < .001,
MANOVA—Gender Differences in Work–Family Conflict (N = 648).
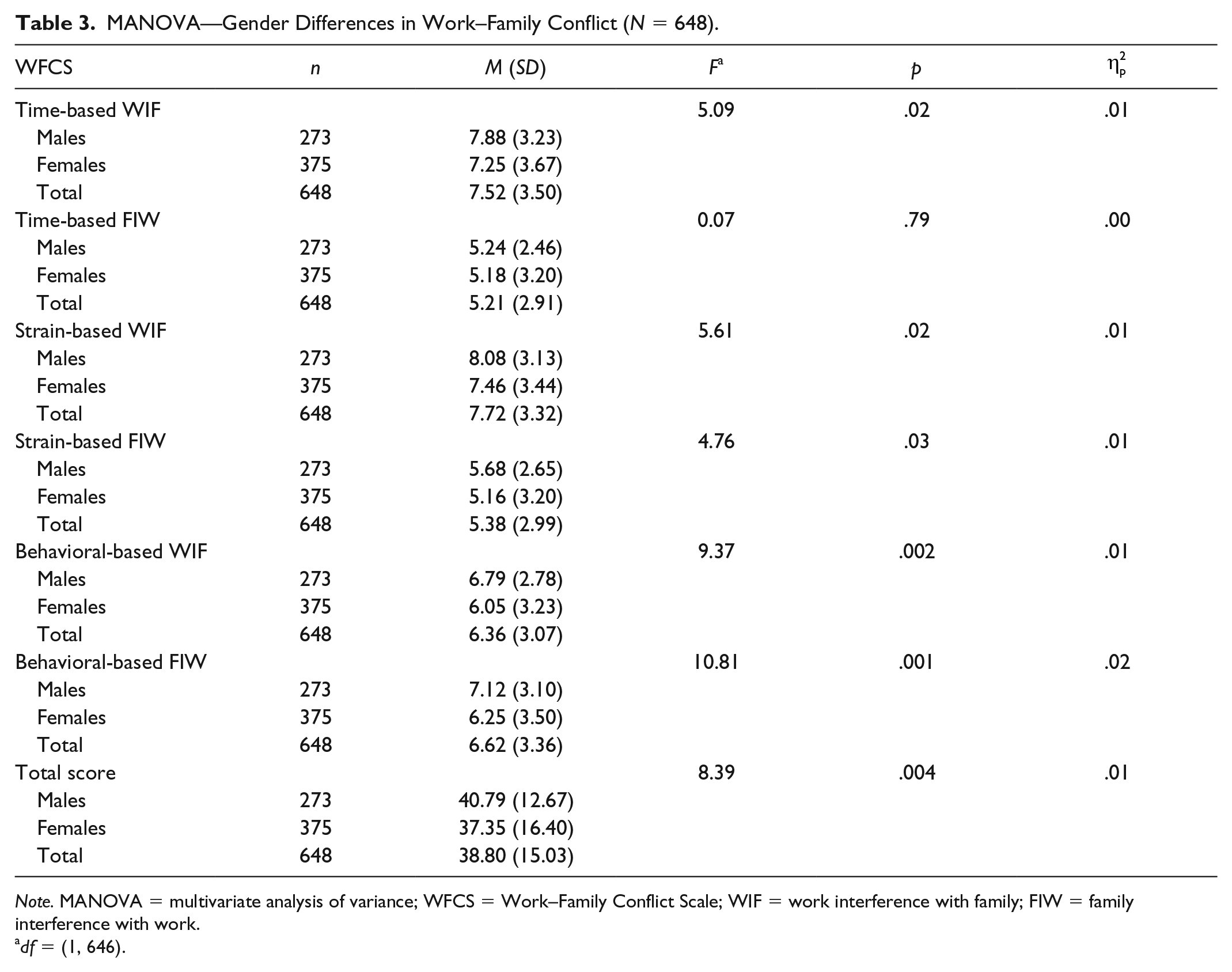
Note. MANOVA = multivariate analysis of variance; WFCS = Work–Family Conflict Scale; WIF = work interference with family; FIW = family interference with work.
df = (1, 646).
With regard to differences in the W-F-C between people with (n = 475) or without (n = 173) children, the multivariate tests showed that this variable has a statistically significant effect, F(7, 640) = 2.54, p = .014,
Finally, as far as job-related differences are concerned, we created the following job categories: (a) medical doctors and other health professionals (n = 201), (b) teachers and researchers (n = 146), (c) employees (n = 120), (d) manual workers (n = 61), and (e) self-employed workers (n = 61).
The multivariate tests showed that the job has a statistically significant effect, F(28, 2085) = 9.54, p < .001,
MANOVA—Job Differences in Work–Family Conflict (n = 589).
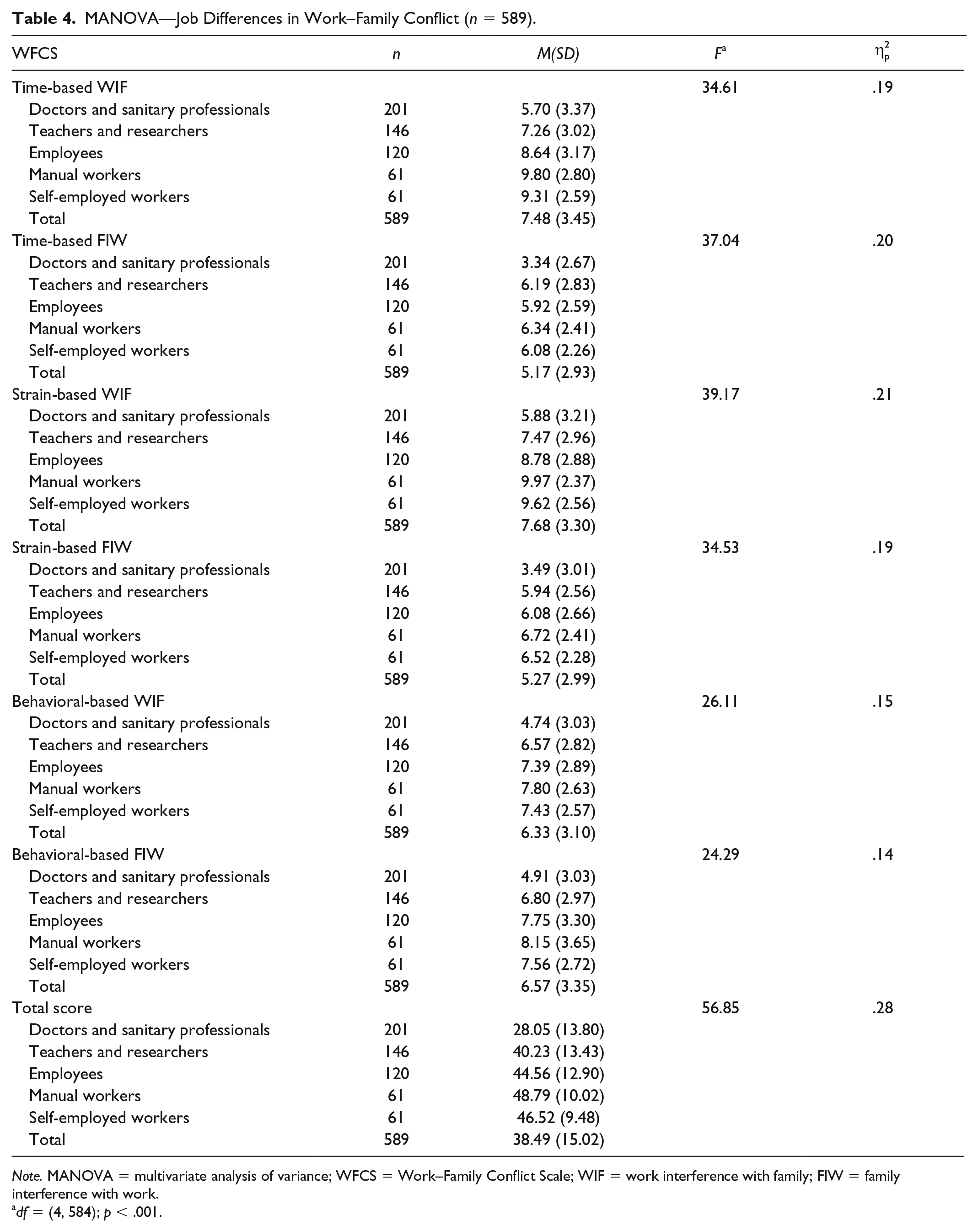
Note. MANOVA = multivariate analysis of variance; WFCS = Work–Family Conflict Scale; WIF = work interference with family; FIW = family interference with work.
df = (4, 584); p < .001.
The Bonferroni post hoc analysis revealed that medical doctors and other health professionals experience significantly (p < .001) the lowest level of time-based and strain-based work interference with family than all the other job categories. Teachers and researchers have instead significantly lower levels of time-based and strain-based work interference with family than employees (p = .003), manual workers and self-employed workers (p < .001). Finally, there are no statistically significant differences between employees, manual workers, and self-employed workers.
Moreover, medical doctors and other health professionals have a statistically significant (p < .001) lower level of both time-based and strain-based family interference with work than all the other job categories. We did not find any other significant difference between the other groups of workers.
Medical doctors and other health professionals also have the lowest level of both behavioral-based WIF (p < .001) and behavioral-based FIW (p < .001). There is also a statistically significant difference (p = .05) between teachers and researchers and manual workers. Hence, manual workers have higher levels of both behavioral-based WFC and FWC than teachers and researchers.
Finally, as regard to the W-F-C in general (as evaluated by the WFCS total score), medical doctors and other health professionals experience the lowest level of W-F-C, with a statistically significant difference (p < .001) with all the other job categories. Moreover, teachers and researchers have lower W-F-C than manual workers (p < .001) and self-employed workers (p = .01). Instead, there is not a statistically significant difference between employees, manual workers, and self-employed workers.
Discussion
The WFCS (Carlson et al., 2000) is one of the most used instruments for assessing the multidimensional construct of the W-F-C. Compared with other instruments (e.g., the 10-item scale of Netemeyer et al., 1996), the WFCS allows evaluating various aspects of the W-F-C. It distinguishes the three forms of the W-F-C (time-based conflict, strain-based conflict, and behavioral-based conflict), and its two directions (WFC, or work to family conflict, and FWC, or family to work conflict). Because in literature there was not an Italian validation of the WFCS, the present study aimed to analyze the factorial structure and the psychometric properties of the Italian translation of the WFCS. Moreover, we also investigated some demographical-related differences in the W-F-C.
The results of the psychometric analyses showed that the Italian version of the WFCS has good psychometric properties. The CFA supported the original six-factor model of the test. Moreover, the values of the Cronbach’s alpha of all the subscales and the total score indicate a good internal reliability, and further support the construct validity of the WFCS. These results are in line with other studies related to the validation of this scale (e.g., Vieira, Lopez, & Matos, 2014).
To further analyze the WFCS, we evaluated the discriminant validity of the instrument through the correlations between the WFCS subscales and total score and the two subscales of the DFRS (Raffagnino & Matera, 2015), namely Dyadic Relationship Satisfaction and Familial Relationship Satisfaction. As the results reported negative but low values of correlation (the highest r value being –.15 for the correlation between the DFRS Dyadic Relationship Satisfaction scale and the WFCS strain-based FIW), we concluded that there is not an association between the two measures.
Given that we found good psychometric properties for the Italian WFCS, we analyzed if there were some demographic-related differences concerning the W-F-C and its components. First, we found that Italian males have higher levels of both WFC and FWC than females, except for time-based FIW, for which males and females do not differ. These findings are in contrast with the numerous studies supporting that females experience higher levels of W-F-C than males (e.g., Erdamar & Demirel, 2014; Leineweber et al., 2012; Todesco, 2013). In literature, the higher presence of W-F-C in females is explained referring to the asymmetry between men and women in the deployment of family roles, which are generally undertaken by females (Alby et al., 2014), and that it was observed in Italy too (Istat, 2010). However, in our sample, it seems that Italian men experience more difficulties than women in conciliating work and family roles. Then, we suggest that future studies should analyze further gender-differences in W-F-C. The changes that are rapidly happening in the work system, such as the job instability and the increasing spread of dual-earner partner, could favor a higher W-F-C in men than in woman.
With regard to differences between people with or without children, we found that people who have children experience a higher level of W-F-C (WFCS total score) and, more specifically, a higher level of time-based and strain-based FWC, compared to people without children. These results are in line with the studies highlighting that parenthood is a challenging and stressful life phase for couples; partners have to face many challenges, which are related, in particular, to the time management and the work and life roles rearrangement between partners (Ford et al., 2007).
Finally, concerning job-related differences, we found that medical doctors and other health professionals experience the lowest level of W-F-C, as regard to both the three kinds of conflict (time, strain, and behavior) and its two directions (WFC and FWC) compared with the other four job categories (i.e., teachers and researchers, employees, manual workers, and self-employed workers). This finding is not in line with previous research, which highlighted a great prevalence of WFC in U.S. nurses instead (Grzywacz et al., 2006), even if they were not evaluated through the WFCS. Moreover, Grzywacz et al. (2006) did not compare the nurses with other job categories as in our study.
We also found that teachers and researchers experience a lower level of time-based and strain-based WFC compared to employees, manual workers, and self-employed workers. Moreover, they have lower levels of behavioral-based WFC and FWC compared with manual workers. Finally, they have a lower level of general W-F-C than both manual workers and self-employed workers. Hence, manual workers and self-employed workers seem to be the two job categories that experience the highest level of W-F-C. This could be due to some characteristics of these jobs (Dierdorff & Ellington, 2008). They could be characterized by a few work resources, which are a protective factor against the W-F-C (Kossek, Pichler, Bodner, & Hammer, 2011; Lu et al., 2009). Manual workers and self-employed workers could have some difficulties in having a flexible work time and, in general, a flexible work arrangement that it is useful in balancing family and work domains (Allen, Johnson, Kiburz, & Shockley, 2013; Valcour, 2007). Moreover, the higher presence of behavioral-based FWC in these workers could suggest that they experience an incompatibility among the behaviors, the expectations, and the rules required by the family and by their job.
Given that we found that manual workers are the workers who experience the highest level of W-F-C, we suggest that future studies should analyze further the W-F-C in this population; moreover, preventive interventions should be implemented in the organizations, so to reduce the risk of experiencing W-F-C, and hence favoring both the manual workers’ health than the organizations’ productivity.
In summary, these demographic-related findings suggest that preventive interventions aimed at favoring workers’ well-being should also be addressed to populations which the literature generally showed to be less affected by W-F-C, namely to males and self-employed and manual workers (and not only to females and medical and health professionals).
Moreover, special attention should be given to workers with children, who seem to have more difficulties in balancing work and family roles, probably due to the increase in family-related duties that children pose to the couple. Having children, indeed, leads to an increase in time, strain, and behaviors (or practical tasks to be done, such as taking children to school, helping the child with school homework, having some free time to dedicate to the partner and the children as well) required by the family role, and these demands might be even more significant when there are two or more children in the family.
Hence, it is critical to develop preventive interventions to be spread in the organizations to improve the management of work and family demands, as this may have positive effects on the worker productivity, as well as on the well-being of the worker and his or her partner and children.
In conclusion, the main strengths of this study are that it provided evidence for the usefulness of the WFCS on the Italian population and that it highlighted some job-related differences in the W-F-C that could inform preventive interventions in the organizations. The WFCS is an instrument widely used in literature, and it is helpful for both clinical and organizational psychologists. This tool could allow analyzing if and how the different components of W-F-C are associated with couple stress, marital conflict, and dissatisfaction, and with workers’ productivity and organizational climate. Moreover, it could be used to develop and evaluate preventive interventions to implement in the organizations, so to reduce the W-F-C that is associated with workaholism (i.e., work addiction), which has negative outcomes for both the individual and his or her family and organizations (Giannini & Loscalzo, 2016; Loscalzo & Giannini, 2015, 2017).
As regard to the limits, this research has been conducted on a convenient sample; in addition, the participants were predominantly Caucasian and middle-class level (though, different jobs characterized them). It would be desirable to analyze the WFCS in a more heterogeneous Italian population further. Moreover, we did not assess the convergent validity of the WFCS. Finally, we investigated differences between groups by means of multivariate analyses; however, comparative analyses of the WFCS scales between groups should be performed through multigroup analyses. It would be interesting if future studies could address these limitations, and also use the WFCS for analyzing other variables that could be associated with it, such as emotional dysregulation, couple communication and couple coping (addressing the individual level), and workplace aggression, workers’ productivity, and turnover (addressing the organizational level).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.