
Abstract
Tobacco use habit is generally viewed as a sole responsibility of an individual, and the entire onus of being or not being a tobacco user is put on the individual himself or herself. But no man lives in isolation and his behavior is constantly determined by various social dynamics surrounding him since his birth and constantly exerting pressures on him. The article is a secondary data analysis of Global Adult Tobacco Survey (GATS) India 2016-2017 having a sample size of 74,037 adults aged greater than 15 years. The smoking and smokeless tobacco use behavior of individuals is studied as a dependent variable in relation to their sociodemographic characteristics (age group, gender, residence, marital status, caste, religion, education, occupation, and material deprivation). A material deprivation index was created and was analyzed in relation to tobacco use habits. The results have shown all these independent variables as very significant determinants of tobacco use (smoking or smokeless) behavior. In India, males are more likely to use tobacco, as compared with females. Also individuals in rural areas are more likely to use tobacco as compared with urban areas. Individuals with no formal education are more likely to use tobacco (smoking or smokeless) as compared with individuals with various levels of education. Moreover, higher the educational levels of individuals, lower the likelihood of using tobacco by them in any form. Material deprivation has also emerged as a strong determinant of tobacco use where higher the levels of material deprivation, more likely individuals were to use tobacco in any form. To conclude, sociodemographic characteristics of individuals as age group, gender, residence, marital status, caste, religion, education, occupation, and material deprivations are major social determinants of tobacco use habit including both smoking and smokeless forms of tobacco use.
Keywords
Background
The World Health Organization (WHO) has described the Social Determinants of Health (SDH) as the “circumstances, in which people grow, live, work, and age, and the systems put in place to deal with illness. The conditions in which people live and die are, in turn, shaped by political, social, and economic forces” (Commission on Social Determinants of Health, 2008, p. i).
Tobacco use is generally considered as a matter of personal choice and thus seen in context of individual responsibility rather than a broad social context. There is a victim-blaming approach in case of tobacco-induced diseases. It is considered that tobacco users have brought these diseases on themselves and it is only their own fault but no one else’s. The common view is that it is up to the tobacco users to change their behavior and quit to avoid adverse effects of tobacco use (Jarvis & Wardle, 2011). Such a belief fails to view tobacco use habit as a response to social circumstances. Mervyn Susser has rightly stated in a series of provocative articles that epidemiology today is restricted generally to clinical epidemiological studies and it is very important to research beyond “individual-level” risk factors and “black-box” epidemiology to a “multi-level eco-epidemiology” (Berkman & Kawachi, 2014). According to Mervyn Susser, “states of health do not exist in a vacuum apart from people. People form societies and any study of the attributes of people is also a study of the manifestations of the form, the structure and the processes of social forces” (Berkman & Kawachi, 2014, p. 5). According to “ecosocial theory” proposed by Nancy Krieger (2001), it is important to study factors responsible for population patterns of health, disease, and well-being.
Health behaviors including tobacco use behavior are not randomly distributed in the population. Rather they are socially and economically patterned and often clustered with other behaviors (Berkman & Kawachi, 2014). There are situations that place individuals “at risk of risks.” Tobacco use behavior is not solely a matter of “individual choice.” Rather, “environment place constraints on individual choice and incentivize particular choices with promises of social, psychological, financial or physical rewards” (Berkman & Kawachi, 2014, p. 8). If our interventions address only individual-level factors by focusing on individual behavior, then even if we are completely successful in this intervention, new individuals will continue to add to the at-risk population because we have not done anything to influence those social forces in the community that altered the individual behavior in the first place (Ruhil, 2016).
The disease outcomes across populations are associated with similar circumstances which are socially and economically patterned and often clustered (Ruhil, 2016). The tobacco use behavior is complex like other behaviors and has its interactions with social and physical environments of people. Such interactions about health behaviors were documented as early as the 1800s. Cassandra Okechukwu and colleagues have mentioned that, “Villerme noted that social factors, such as the standards of living and duration of work, constrained the behaviours of people in different trade, such that different professions were associated with particular behavioural tendencies and even levels of hygiene” (Okechukwu, Davison, & Emmons, 2014, pp. 365-366).
The tobacco use habit has been seen to get influenced by material and cultural disadvantage and deprivation (Jarvis & Wardle, 2011). This article studies (along with other sociodemographic determinants) how tobacco use habit among individuals varied with the level of material deprivation in India. Deprivation as an index of measurement of poverty was first used by Townsend in 1979 among European population and is very well known as “deprivation index” since then (Eroğlu, 2007). The concept of deprivation was a broadening of the concept of poverty and meant that people were deprived of living standards. After Townsend, several researchers worked on the concept of “Deprivation.” Amartya Sen in 1982 emphasized that “feelings of deprivation” should also be taken into account along with the choice of “conditions of deprivation,” while deciding the level of living (Eroğlu, 2007). Piachand in 1981 argued that there is a continuum in deprivation (Eroğlu, 2007). Mack and Lansley (1985), Hallerod (1994), and Veit-Wilson (1987) worked on the concept of “Deprivation” (Eroğlu, 2007).
The eminent epidemiologist Michael Marmot related material deprivation with “Health” in his work “Social Determinants of Health inequalities” published in The Lancet in 2005 (Marmot, 2005). He explained that “psychological pathways” created by conditions of “material deprivation” lead to risky health behaviors. Furthermore, in 2006, the work of Martin J. Jarvis and Jane Wardle showed that rates of cigarette smoking increased by material and cultural disadvantage among U.K.-based populations (Jarvis & Wardle, 2011). Among Indian population, “Wealth-index” was used in an article by Krishna M. Palipudi and colleagues (2012). The Wealth index was a proxy indicator for household ownership of assets. The method of computing “material deprivation index” in my article is different and so the meaning it carries is also different (which is discussed in detail in methodology section). Here the weightage given to various variables is based on “feelings of deprivation” rather than their market value (explained in methodology section). In this way, my research fills the gaps in literature and adds to new knowledge.
The article also studies other sociodemographic determinants of tobacco use like age, gender, residence (urban/rural), marital status, education, occupation, caste, and religion. This article is based on secondary data analysis of Global Adult Tobacco Survey (GATS) India 2016-2017.
The objective of the study is to determine how sociodemographic characteristics (age, gender, residence, marital status, education, occupation, religion, and caste and material deprivation) of individuals influence their likelihood of using smoking and smokeless forms of tobacco.
Method
Study Design
The study design was secondary data analysis of GATS India 2016-2017. GATS is one of the major elements of the Global Tobacco Surveillance System (GTSS). It helps countries in tracking tobacco control indicators and formulating effective tobacco control interventions.
Settings
The primary data of GATS 2 India was collected between August 2016 and February 2017 in a household survey by the Tata Institute of Social Sciences (TISS) with support from Ministry of Health and Family Welfare (MoHFW), Centers for Disease Control and Prevention (CDC), and WHO.
Participants
It included participants aged 15 years and above, on a voluntary basis, after giving informed consent. Participants were included on the basis of three-stage sampling independently in each state/union territories (UT) and within each state/UT, independently in urban and rural areas. In the present study of secondary data analysis, the participants were all smokers and smokeless tobacco users aged 15 and above.
Figure 1 represents a flow diagram of study participants at each stage of study from the GATS India survey data 2016-2017. A total of 74,037 adults aged greater than 15 years were included in the study. Out of them, 21,175 were tobacco users and 52,862 were non–tobacco users. Out of total tobacco users, 15,235 were smokeless tobacco users and 9,499 were smokers (refer Figure 1).
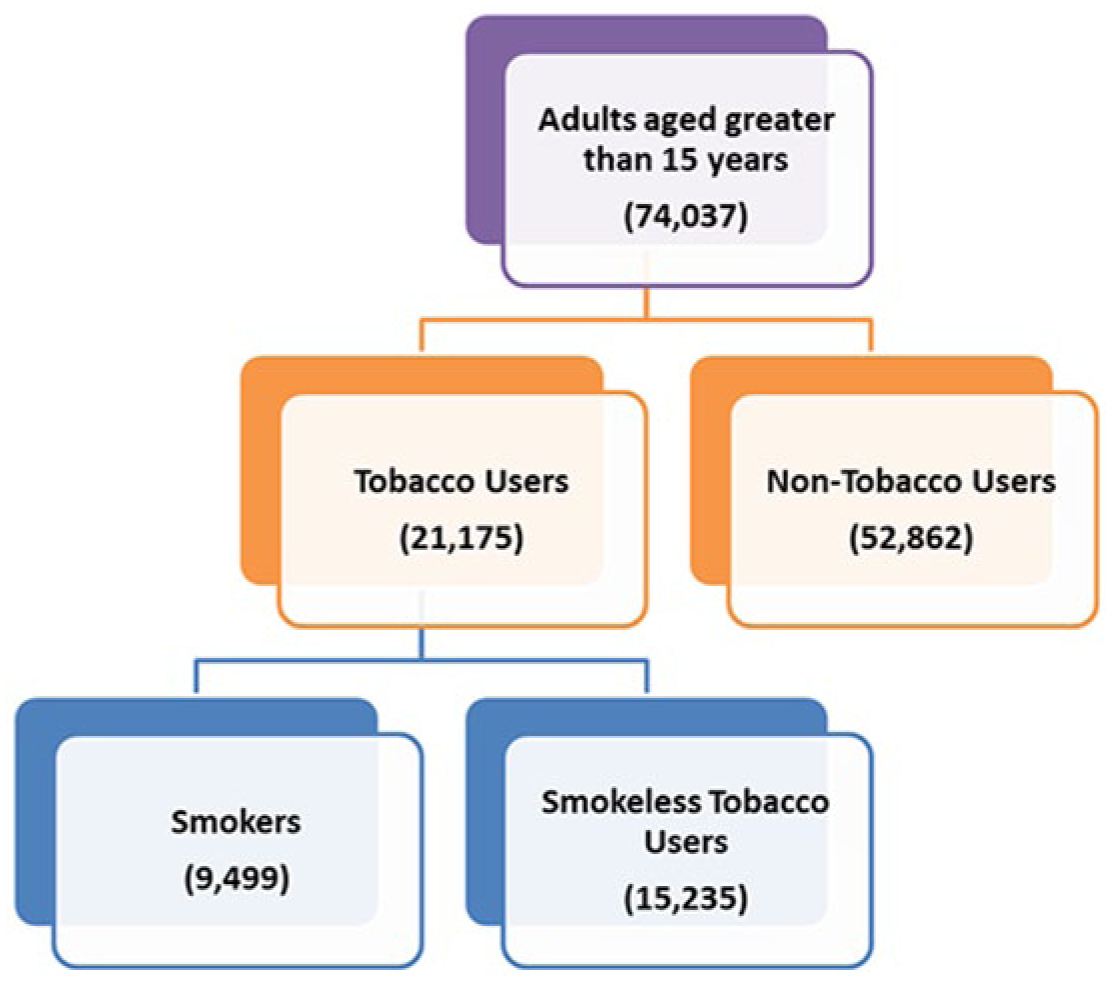
Flow diagram to show study participants at each stage of study.
Variables
The exposure variables for assessing association were
Age group (15-24, 25-44, 45-64, 65+) in years,
Gender (male, female),
Residence (urban, rural),
Education (no formal education, less than secondary school, secondary school completed, higher secondary school completed, college/ university completed, post-graduate degree completed),
Occupation (government employee, non-government employee, self-employed, student, homemaker, retired, unemployed),
Marital status (Single, Married, Divorced, Separated, Widowed),
Religion (Hindu, Muslim, Christian, Buddhism, Jain, Sikh, Other),
Caste (Scheduled Caste, Scheduled Tribe, Other Backward Classes, General), and
Material deprivation (Level 1 to Level 6 where Level 1 is least materially deprived and Level 6 corresponds to most deprived)—This index was computed which is explained ahead in data analysis section.
Outcome variables were the following:
All smokeless tobacco (SLT) users aged 15 and above.
All smokers aged 15 and above.
Data Sources/Measurements
The original data set of GATS India 2016-2017 was used, which is available for public use from the CDC website. The data have been taken from CDC website, https://nccd.cdc.gov/GTSSData/Ancillary/DataReports.aspx?CAID=2
Data Analysis
The analysis of the extracted data was conducted using SPSS (Statistical Product and Service Solution, formerly known as Statistical Package for Social Sciences) version 19 developed by IBM. First, a descriptive analysis of all the variables included in the study was done.
Material Deprivation as a new index was computed using following variables and recoding them in the following way:
Electricity (Absence =3, Presence = 0),
Flush Toilet (Absence = 2, Presence = 0),
Fixed Telephone (Absence =1, Presence = 0),
Cell Telephone (Absence =1, Presence = 0),
Television (Absence =1, Presence = 0),
Radio (Absence =1, Presence = 0),
Refrigerator (Absence =1, Presence = 0),
Car (Absence =1, Presence = 0),
Moped/Scooter/Motorcycle (Absence =1, Presence = 0),
Washing Machine (Absence =1, Presence = 0),
Computer/Laptop (Absence =1, Presence = 0),
Internet Connection (Absence =1, Presence = 0),
Air Conditioner (Absence =1, Presence = 0),
Electric Fan (Absence =1, Presence = 0),
Here the weightage given to various variables (under this index) was based on “feelings of deprivation” as opposite to economic value which was done in wealth index. “Feelings of deprivation” was assessed by the author himself on the basis which is explained ahead. Here, economic value of electricity used or flush toilet may be less than that of an air conditioner or Car or Laptop; but the “feelings of deprivation” in the absence of electricity or flush toilet is more than that in case of air conditioner or car or laptop. Here electricity was given highest weightage because it is a basic necessity in a household without which no other appliance can work. Second highest weightage was given to flush toilet which is again a basic necessity. It was experienced by author that people in slums have dish TVs in their Jhuggis but not flush toilet, and thus in spite of having television their level of deprivation is more. Rest of the variables were given equal weightage. An example for this explanation is that, man in the house may feel deprived without a vehicle, woman may feel deprived without a washing machine, and youth may feel deprived without computer and Internet connection. However, in this methodology, the author was bounded by the variables available in GATS data set.
All these variables were then added and a new index was generated having values ranging from 0 to 17, where 0 means least deprived and 17 meant most deprived. The index was then further categorized into six levels where Level 1 was the least deprived and Level 6 was the most deprived.
Next, an initial bivariate logistic regression analysis was done by searching for associations of exposure variables with the outcome variables.
Then multivariable logistic regression analysis was performed, adjusting for all the confounders. Significance levels for both bivariate and multivariable logistic regression analysis were set at 0.05.
Results
Data analysis have shown how the sociodemographic characteristics of individuals including age, gender, residence, marital status, education, occupation, religion, caste, and material deprivation significantly determine their tobacco use habit (both smoking and smokeless tobacco use; refer Tables 1 and 2).
Sociodemographic Characteristics of Individuals as Determinants of Using Smoking Forms of Tobacco Among Them: GATS India 2016-2017.

Note. GATS = Global Adult Tobacco Survey; OR = odds ratio; CI = confidence interval; SC = Scheduled Caste; ST = Scheduled Tribe; OBC = Other Backward Class.
Sociodemographic Characteristics of Individuals as Determinants of Using Smokeless Forms (SLT) of Tobacco Among Them: GATS India 2016-2017.

Note. SLT = smokeless tobacco; GATS = Global Adult Tobacco Survey; OR = odds ratio; SC = Scheduled Caste; ST = Scheduled Tribe; OBC = Other Backward Class.
Let us first look at the age group. In case of smoking, age group of 45 to 64 had highest odds of being a smoker (Refer Table 1), followed by age group of 65+ and then age group of 25 to 44. Further age group of 15 to 24 had least odds of being a smoker. In case of SLT use, a pattern has emerged, where higher is the age group of individuals, higher were the odds of being a SLT user. There may be several explanations for this pattern which is discussed in “Discussion” section.
Regarding gender, male are more likely to use tobacco (both smoking and SLT) as compared with females. In case of SLT use, being a male had 2.19 times higher odds of using SLT as compared with females. Moreover, in case of smoking, being a male had 15.9 times higher odds of smoking as compared with females.
Regarding Rural versus Urban residence, being residing in urban areas had fewer odds of using tobacco (both smoking and smokeless) as compared with rural areas.
In case of marital status of individuals, being divorced and widowed had highest odds of using tobacco (both smoking and smokeless) followed by being separated and then being married. Here being single or unmarried had least odds of using tobacco (both smoking and smokeless). However, these results regarding marital status may differ with respect to men and women separately. This needs further research in the form of splitting the results gender-wise.
Now coming to educational status of individuals, a clear-cut pattern has emerged which is shown in Figure 2. Here lower was the educational status of individuals, higher were the odds of using tobacco (both smoking and smokeless tobacco) by them. In other words, higher was the educational attainment by individuals, less likely they were to use tobacco in any form (refer Figure 2).

Pattern of OR while showing educational status of individuals as determinant of tobacco use (smoking and SLT) habit among them.
Regarding occupation of individuals, it was found that being a daily wage laborer had higher odds of using tobacco (both smoking and smokeless) as compared with being unemployed. Moreover, in case of SLT use, being self-employed, being daily wage laborer, or being nongovernment employee had higher odds of being a SLT user as compared with being unemployed. On the contrary, being a student or being a homemaker had lower odds of using SLT as compared with being unemployed. In case of smoking, being retired or being a student had lower odds of being a smoker as compared with being unemployed.
Regarding religion, statistical analysis has shown that both smoking and SLT use were more among Muslims and Christians as compared with Hindus. Smoking was also more among Buddhists as compared with Hindus. Both smoking and SLT use were less in Sikh religion as compared with Hindu religion. However, religion of an individual is a sensitive topic and thus requires further research to make any statements.
Regarding caste of individuals, the likelihood of using tobacco (both smoking and SLT) was highest in case of Scheduled Tribes followed by Scheduled Castes, when compared with General castes. However, regarding Other Backward Classes (OBC), the likelihood of SLT use among them was more than General castes, but likelihood of smoking among them was less than General castes.
Regarding material deprivation, some very interesting pattern has emerged from the data in case of both smoking and SLT use. It was found that higher was the level of material deprivation, higher was the likelihood of using SLT or smoking by them. These trends are plotted in the form of graph and are shown in Figure 3. Here results are more significant in case of SLT use, and odds ratios are also higher in case of SLT use. As an example, there are 10.21 times higher odds of an individual with Level 6 of material deprivation, to use SLT, as compared with an individual with Level 1 of material deprivation (refer Figure 3).

Pattern of OR while showing material deprivation among individuals as determinant of tobacco use (smoking and SLT) habit among them.
Discussion
Let us first discuss the pattern observed regarding age group of individuals with respect to tobacco use habit. May be in older age groups, individuals have fewer restrictions and they get freer to use tobacco. Another explanation is that psychological pathways relating stress to tobacco use may become more dominant in older age groups.
The trends regarding gender show that SLT use among females is rather acceptable, whereas smoking among females is a social taboo (Morrow & Barraclough, 2010; Ruhil, 2018; WHO, 2010). Indian culture prohibits women to indulge in smoking and drinking, while there are no such restrictions on men; rather, tobacco use among men is culturally encouraged in certain contexts (Morrow & Barraclough, 2010; Ruhil, 2018; WHO, 2010).
The trends regarding area of residence might be because rural populations are poor, uneducated, and deprived as compared with people residing in urban areas. The Rangarajan (2014) committee estimated that 30.9% of the rural population is poor as compared with 26.4% of poor population in urban areas. Moreover, according to National Sample Survey 71st round, 2014, literacy rate in rural India was 71% as compared with 86% in urban India. These results regarding area of residence and tobacco use may differ for urban slums, urban middle-class, and urban posh areas separately, because urban areas are not homogeneous and it needs further research to get clarity.
The patterns in occupation may be due to ease of living in particular occupations as compared with hardships in other occupations. It is surprising that stress or hardships in being a daily wage laborer may be even greater than being unemployed. Similarly, the socioeconomic status and hardships associated with lives of Scheduled Tribes and castes may be an explanation for higher prevalence of tobacco use among them as compared with General castes.
The results of this study are consistent with the few studies done on the similar subject worldwide. Previous researches done worldwide have shown that likelihood or prevalence of tobacco use decreases with increasing levels of education and the current research also strengthens the same. Lee, Crombie, Smith, and Tunstall-Pedoe (1991) showed high rates of smoking among the unemployed. Jarvis (1997) showed that odds of being a smoker in the United Kingdom were significantly increased in individuals in lower occupational class groups, unemployed, living in crowded accommodations, living in rented housing, without access to a car, and divorced or separated. Also he found a substantial gradient by educational level similar to my study where odds of being a smoker decreased with higher educational levels. Sorensen, Gupta, and Pednekar (2005) also conducted a study in Mumbai, India, where they showed that smoking was associated with various indicators of disadvantage, including educational disadvantage and occupational disadvantage. Also the studies (Bajekal, Primatesta & Prior, 2002; Caraballo et al., 1998; English, Eskenazi, & Christianson, 1994; Perez-Stable, Herrera, Jacob, & Benowitz, 1998; Wagenknecht et al., 1990) have shown that levels of nicotine dependence among smokers increased with increasing deprivation with average nicotine intake being 30% higher in the most deprived as compared with most affluent smokers. Bobak, Jarvis, Skpodova, and Marmot (2000) showed a gradient in intake of nicotine by level of education in Czech smokers. Researchers (Graham, 1987; Smith & Morris, 1994) have shown cigarette smoking as a means of managing stress, regulating mood and coping with the strain resulting from material deprivation. Palipudi et al. (2012) have shown decreasing prevalence of tobacco use with increasing levels of education and also with increasing wealth in 13 low- and middle-income countries.
The main limitation of this study is that only few independent variables could be analyzed which were available in GATS India 2016-2017 data. There is much more to social determinants. The cultural disadvantage and role of ethnicity, inequity, and discrimination could be analyzed as social determinants of tobacco use. Also among the variables which were studied, whole spectrum could be analyzed. For example, government employee was just one category under employment, but being in government job could range from being very stressful like a bus driver, traffic police, or clerk, or it could be more satisfying like a professor, doctor, or teacher. Thus, these are the limitations of being positivist itself that facts are quantified as being Black and White whereas there are actually various shades of Gray. More and more research in this area could probably answer the various questions that have emerged during the course of this research.
Conclusion
To conclude, sociodemographic characteristics of individuals including their age group, gender, residence, marital status, caste, religion, education, occupation, and material deprivations are major social determinants of tobacco use habit including both smoking and smokeless forms of tobacco use. Education has emerged as a very strong determinant of tobacco use. Furthermore, in India, males are more likely to use tobacco as compared with females. Also individuals in rural areas are more likely to use tobacco as compared with urban areas. Here “Material deprivation” has also emerged as a strong determinant of tobacco use. Moreover, various researches done worldwide has also shown the same, and the conclusion got strengthened by this research in case of Indian populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Concerns
The study had no direct involvement with human subjects. The study is a secondary data analysis of GATS India 2016-2017 which is available in public domain and the data source has been cited properly in references. All other sources of information that helped toward completion of this study have been acknowledged properly in references.