
Abstract
A dearth of research exists on the effects of smoking on the relationship between sleep and mental illnesses. To examine the association of mental health problems with days of poor sleep based on whether participants smoked. A secondary analysis of the 2015 Behavioral Risk Factor Surveillance System (N = 16,253) was conducted using linear regressions models. The study found that the associations between mental health and sleep quality, measured as days of poor sleep, varied by the respondents’ smoker status among those who reported having less than 20 days of mental health problems. The difference in days of poor sleep between smokers and non-smokers were greatest among those who experienced 10 to 19 days of mental health problems. Of those with 10 to 19 days of mental health problems in the past 30 days, an average of 8.5 days of poor sleep was estimated among smokers, which was 3 more days than that of non-smokers (p = .001). The differences in days of poor sleep were not significantly different between smokers and non-smokers among those who reported 20 or more days of mental health problems. Days of mental health problems were directly related to days of poor sleep. This relationship was moderated by smoking status. Special attention needs to be paid to those who have comparably moderate levels of mental illnesses because non-smoking status can significantly improve sleep quality. Further research is needed to confirm the impact of smoking on the associations of mental illnesses with poor sleep.
Impact Statement
Literature on the impact of smoking on the relationships between mental illnesses and poor sleep has been scarce.
This study was conducted to examine the moderating effects of smoking on the associations of mental health problems with poor sleep.
This study’s findings will provide helpful information for health professionals who provide care for individuals with insomnia, mental disorders, and tobacco use.
Health researchers who study smoking’s effect on sleep and associations between smoking, sleep, and mental disorders will benefit from this study’s findings and suggestions.
Introduction
Insomnia or sleep disturbances are prevalent among individuals with psychiatric disorders. Depression, anxiety, schizophrenia, and stress have been reported as closely related to insomnia and poor sleep is one of the important diagnostic criteria for major psychiatric disorders (Becker et al., 2017; Cox & Olatunji, 2016; Klingaman et al., 2015; Valerio et al., 2016). Researchers have elucidated the mechanism of the associations between mental illnesses and sleep problems. Poor sleep is not simply a symptom of mood states, but may be a risk factor of the condition (Al-Abri, 2015; Short & Louca, 2015). Dysregulation of the neurotransmitters and pathways regarding the clock genes can influence the pathophysiology of sleep–wake disorders among individuals suffering from schizophrenia (Kamath et al., 2015).
Smoking is another apparent risk factor of sleep disturbance. A number of investigators have reported on higher sleep disturbances among current smokers than nonsmokers (Patterson et al., 2019). For example, Patterson et al. (2019), in a review article on smoking’s impacts on sleep, documented that smokers were more likely than nonsmokers to experience longer sleep latency, shorter sleep hours, and subjective insufficient sleep. They also reported extended or shortened sleep stages among smokers in comparison with nonsmokers, suggesting that cigarette users may undergo lighter sleep stages than nonusers. In addition, people with mental illnesses are influenced with disproportionately higher smoking prevalence than general adults (Szatkowski & McNeill, 2015).
However, the associations between mental illnesses and sleep problems differentiated by smoking status has been under-researched. Thus, research questions arose whether smoking worsens the relationships between mental health problems and poor sleep, and if so, what is the difference in the magnitude of those associations. Identifying this knowledge would provide significant implications for clinical practice targeting the individuals with mental health issues and poor sleep as well as highlighting the importance of smoking cessation strategies for this adult population group. To address this gap in literature, this brief report examined the moderating effects of smoking on the relationships between mental health problems and poor sleep in adults.
Methods
Parent Data
In this study, we conducted secondary analysis using the 2015 Behavioral Risk Factor Surveillance System (BRFSS). The BRFSS is a state-based, random-digit-dialed telephone health behavior survey of adults 18 years or older across the United States implemented by the Centers for Disease Control and Prevention (2019). It is one of the largest national surveys using telephones to collect information about the population’s health status and health behaviors. The survey was administered anonymously without collecting any personally identifying information.
Measures
The dependent variable, days of trouble sleeping (days of poor sleep), was measured using one question: “Over the last 2 weeks, how many days have you had trouble falling asleep or staying asleep or sleeping too much?” Answers ranged from 0 to 14 days and were treated as a continuous variable. In this study, mental health was defined as emotional and psychological well-being. Days of mental health not good (days of mental health problems) was measured with the following question: “Now, thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?” Responses to this question, ranging from 0 to 30 days, were recoded into five levels (0, 1–9, 10–19, 20–29, and 30 days) to minimize bias from a heaping response pattern (Holbrook et al., 2014) and to easily capture its potentially nonlinear relationship with the dependent variable. For current smoking status, the question “Do you now smoke cigarettes every day, some days, or not at all?” was used, and respondents who answered “every day” or “some days” were classified as current smokers.
Analysis Plan
All statistical analyses were conducted considering the survey data analysis module, which accounted for the sampling design (e.g., clusters, strata, and sample weights). We estimated participants’ general characteristics by descriptive statistics using frequencies, percentages, and a mean. Using linear regression models, we examined the main effects of days of mental health problems and smoking status on days of poor sleep, controlling for sociodemographic characteristics. Next, we included two-way interaction terms, days of mental health problem by smoking status to assess whether the relationships between mental health problems and days of poor sleep depend on smoking status. The effects were estimated as regression coefficients with 95% confidence intervals. The significance level was set at <.05. The Stata 14 software program was used for all statistical analyses. The study protocol was waived by the Institutional Review Board at the first author’s university.
Results
The gender and age were relatively evenly distributed across the category except 18 to 24 years. Slightly more than half of the respondents reported some college or more education. 34 percent of participants reported one or more days of mental health problems. Of the respondents, 23% reported smoking intermittently or daily. On average, participants reported 3.77 days of poor sleep in the prior 2 weeks (Appendix Table A1).
Table 1 shows the main effects (Model 1) and interaction effects models (Model 2). In Model 1, days of mental health problems and smoking status were significantly associated with days of poor sleep, controlling for the sociodemographic variables. As the coefficients for the days of mental health problems show, days of poor mental health was strongly associated with days of poor sleep in a nonlinear way. The relationship between the two variables showed a linear increase up to the fourth level of mental health problem days (i.e., 20–29 days) and plateaued at the upper-end categories (from b20–29 days = 5.13 to b30 days = 5.14). The current smokers were more likely than nonsmokers to experience days of poor sleep (b = 1.0, i.e., one more days of poor sleep in the prior 2 weeks).
Linear Regression Models of Days of Poor Sleep: Main and Interaction Effect Models (N = 16,253).

Note. 95% CI = 95% confidence interval.
p < .05. **p < .01. ***p < .001 (two-tailed test).
Model 2 shows significant interaction effects between 1–9 days and 10–19 days of mental health problems and smoking status on the days of poor sleep (b = 1.08 to b = 2.31, respectively). As depicted in Figure 1, the differences in days of poor sleep between those who had 0 days, 1–9 days, and 10–19 days of mental health problems were significantly greater among smokers compared to nonsmokers. In other words, the association between days of mental health problems and poor sleep was statistically stronger among smokers compared to nonsmokers among those who experienced up to 19 days of mental health problems. Of those who experienced 20 or more days of mental health problems, smokers were slightly more likely to experience poor sleep, but the difference was not statistically significant.
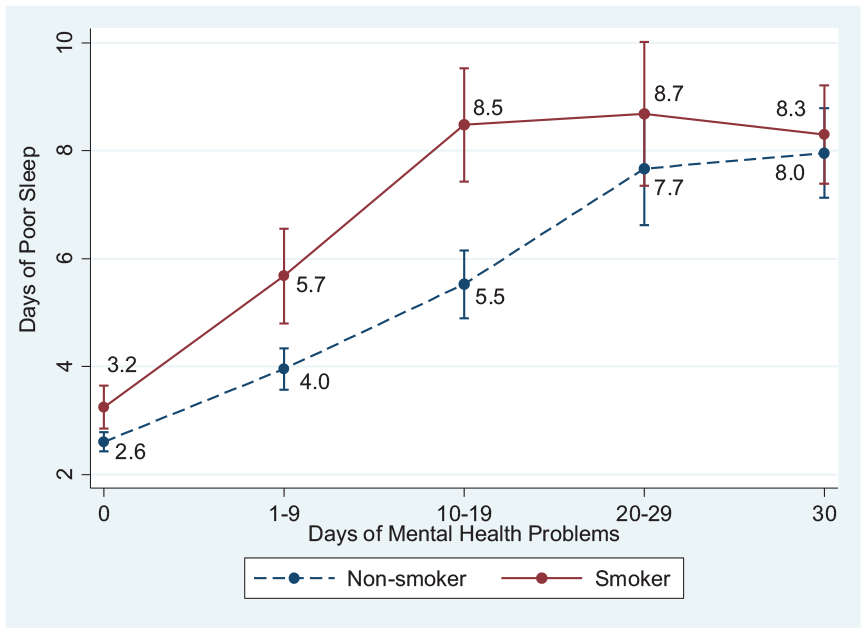
Non-linear pattern of relationships between days of poor mental health and days of poor sleep moderated by smoking status.
Discussion
The findings (Table 1, Figure 1) indicated that overall days of self-perceived mental health problems and poor sleep were significantly correlated. The associations were considerably higher among smokers compared to nonsmokers and the results imply nonlinear correlations (i.e., polygonal slope) between days of mental health problems and poor sleep. This study adds to the body of literature showing a relationship between mental health problems and poor sleep. It is considered that sleep is influenced by cognitive, cortical, and autonomic hyperarousal status, and subjective experience of positive and negative emotions as well as genetic factors and other neurobiological mechanisms (Baglioni et al., 2010).
Interestingly, the finding of this study indicated that the negative effect of mental health problems on sleep was strengthened along with smoking status among those who reported 1 to 19 days of mental health problems in the prior month (Table 1 and Figure 1). Tobacco users frequently complain of poor sleep primarily due to nicotine’s arousal effect, which leads to awakening during sleep, and its craving effect, which causes disturbed sleep (Jaehne et al., 2012). Individuals with psychiatric disorders smoke more than those without such challenges (Becker et al., 2017; Cox & Olatunji, 2016; Klingaman et al., 2015). Moreover, people with mental health problems were reported to be associated with higher nicotine dependence and smoking intensity (McClave et al., 2010). It seems poor sleep among individuals with moderate or less chronic mental health problems is exacerbated by smoking because of a synergic effect of smoking and mental illnesses on sleep.
Another notable finding was that the smoking status difference in the size of the effect of 20 to 30 days of mental health problems on days of poor sleep was not significant (Table 1 and Figure 1). An interesting finding was that the difference in days of poor sleep between smokers and nonsmokers living with more frequent (20 or more) days of mental health problems became narrow compared to those with 1 to 19 days of mental health problems. Given that most mental disorders, such as depression, anxiety, schizophrenia (Becker et al., 2017; Cox & Olatunji, 2016; Klingaman et al., 2015), stress (Valerio et al., 2016), and substance use (Hartwell et al., 2014), are associated with sleep problems, this finding supports that smoking would not affect individuals who may experience severe or chronic mental or emotional conditions as much as those without or with moderate or less chronic mental health problems in relation to poor sleep.
In this study, we placed the days of mental health problems in the independent variable and the days of poor sleep in the dependent variable in analysis. Given that this study worked with the non-clinical and population-based sample, the reverse relationship (days of poor sleep as the independent variable and days of mental health problems as the dependent variable) may be plausible. Researchers have suggested that sleep deprivation can raise risk for or contribute to the development of various mental health disorders including depression, bipolar disorder, anxiety, schizophrenia, and cognitive impairment (Bao et al., 2017; da Silva, 2015; Harvard Health Publishing, n.d.; Kamath et al., 2015; Simon et al., 2016). It is considered that sleep disturbance influences the secretion of neurotransmitters and stress hormones and this may impair emotional regulation and the normal cognitive processes (Harvard Health Publishing, n.d., n.d; Yoo et al., 2007). There is another possibility that sleep quality moderates the association between dose-response smoking use status and mental health problems. Since the reciprocity and complexity between these variables exist, these interplays need to be carefully understood and findings need to be used for the optimal health care implications depending on the focus of the care.
Further rigorous methodological studies are needed to explain the impacts of mental illnesses on sleep quality by smoking status and the mediating effect of sleep quality between smoking status and mental health problems. We did not strictly account for possible covariates that may be directly or indirectly associated with sleep, such as medications, day or night shift work, food, and exposure to light, as well as comprehensive characteristics of smoking such as types of products, years of smoking, and nicotine dependence. Furthermore, researchers need to consider additional mental illness factors (e.g., type, onset, duration, and treatment) to understand smoking’s impact on the associations between mental health problems and poor sleep.
Limitations and Strengths
This study contains several limitations. First, we used self-reported survey data, which is subject to a response bias. Second, because the data were collected cross-sectionally, we were unable to evaluate converse effects and causal effects between mental illnesses and poor sleep. Third, we did not consider more detailed characteristics of mental health problems and smoking patterns. Nevertheless, the study’s sample size was considerably large. Above all, to our knowledge this is the first study to compare the impact magnitudes of days of mental health problems on poor sleep differentiated by smoking status in American adults. We also controlled various demographic and socioeconomic characteristics that may have been related to the outcome variables.
Implications Practice and Research
Healthcare professionals need to proactively consider tobacco use reduction or cessation treatment to improve sleep among patients with mental illnesses. Special attention needs to be paid to those who have comparably moderate levels of mental illnesses because just quitting smoking can significantly improve sleep quality. Future research needs to consider advanced research designs (e.g., longitudinal) and objective measures (e.g., cotinine in plasma or urine or sleep outcomes evaluated by polysomnography). Additional efforts need to be made to investigate why the smoking effect decreases on the association between longer chronic mental health problems and poor sleep. Future research should also examine additional characteristics of mental health status and tobacco use patterns. (e.g., dose-response of tobacco use and e-cigarette use) to better understand the impact of smoking on the associations.
Conclusions
This study was conducted to fill a gap in knowledge regarding smoking’s effects on the associations between mental illnesses and poor sleep and used the 2015 BRFSS data set. We observed significant moderating effects of smoking status on the relationships between 1–9 and 10–19 days of mental health problems and poor sleep. However, no significant moderating effects were found in the relationship between more frequent (20–30) days of mental health problems and poor sleep. Findings did support the negative influence of smoking and mental disorders on sleep. Additional research with rigorous methodological considerations is needed to verify the impact size of smoking on these relationships.
Footnotes
Appendix
Descriptive Statistics (N = 16,253).

| Variables | N | % or mean |
|---|---|---|
| Gender (%) | ||
| Female | 8,245 | 50.73 |
| Male | 8,008 | 49.27 |
| Age (%) | ||
| 18–24 years | 1,662 | 10.22 |
| 25–34 years | 2,608 | 16.05 |
| 35–44 years | 2,829 | 17.40 |
| 45–54 years | 2,981 | 18.34 |
| 55–64 years | 3,047 | 18.75 |
| 65 years or older | 3,126 | 19.22 |
| Race/ethnicity (%) | ||
| Hispanic | 351 | 2.16 |
| Black, non-Hispanic | 2,900 | 17.85 |
| White, non-Hispanic | 12,499 | 76.91 |
| Other | 502 | 3.09 |
| Education level (%) | ||
| Less than high school | 2,394 | 14.73 |
| High school | 5,204 | 32.02 |
| Some college | 5,055 | 31.10 |
| College graduation or more | 3,599 | 22.15 |
| Income (%) | ||
| <$15,000 | 2,175 | 1 < 0.38 |
| $15,000 ≤ $25,000 | 3,339 | 20.54 |
| $25,000 ≤ $35,000 | 1991 | 12.24 |
| $35,000 ≤ $50,000 | 2,443 | 15.03 |
| $50,000< | 6,305 | 38.79 |
| Days of mental health problems (%) | ||
| 0 day | 10,777 | 66.31 |
| 1–9 days | 2,620 | 16.12 |
| 10–19 days | 1,175 | 7.23 |
| 20–29 days | 423 | 2.61 |
| 30 day | 1,257 | 7.73 |
| Current smoking (%) | ||
| Yes | 3,697 | 22.75 |
| No | 12,556 | 77.25 |
| Days of poor sleep (mean/SE) (Range: 0–14) | 16,253 | 3.77 (0.07) |
Note. SE = standard error.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.