
Abstract
This article seeks to address the dearth of evidence on early adolescent understandings and experiences of sexual and reproductive health (SRH) in Ethiopia and Rwanda, drawing on a multisite qualitative research study with 10- to 12-year-old and 14- to 15-year-old male and female adolescents and a range of adult participants. The article is informed by a conceptual framework that draws on Amartya Sen’s capability approach, which calls for investments in a broad set of assets that expand individuals’ capacity to “be” and to “do.” Using SRH as a focal lens, the article considers the role played by gendered social norms in adolescents’ experiences of SRH-related understandings and experiences. Three key interrelated gender themes emerge from our thematic analyses of qualitative evidence generated by our multimethods approach: puberty transitions, sexuality, and victim blaming. In our analyses, we pay attention to diversity (e.g., age, gender, place of residence) among adolescents within and across the two focal countries and consider how discriminatory gendered social norms play a role in hindering the effective uptake of expanding health services. We conclude by emphasizing the need for program designers and implementers to address the role of underlying social norms in a more strategic and context-specific way to help young people navigate their sexual and reproductive lives.
Introduction
Evidence suggests that many adolescents experience discriminatory social norms and practices, linked to their gender and age, which negatively affect not only their short-term well-being but also their life chances and long-term trajectories (Harper, Jones, Marcus, Ghimire, & Bantebya, 2017; Patton et al., 2016). There is relatively little evidence on age- and gender-differentiated adolescent experiences and perceptions of sexual and reproductive health (SRH) in various settings, from household and schools to the wider community. In addition, in many contexts, appropriate channels of response and redress (whether formal or informal) are simply not available (Fulu, Kerr-Wilson, & Lang, 2014; Pankhurst, Negussie, & Mulugeta, 2016; UNICEF, 2014; Yount, Krause, & Miedema, 2017).
This report goes some way to filling the evidence gap by considering how gender and age affect adolescent boys’ and girls’ experiences of SRH in two East African countries: Ethiopia and Rwanda. We define SRH as incorporating aspects of physical and mental health, including awareness of and access to SRH knowledge and services, sexual and gender-based violence, puberty and menstruation, contraception, pregnancy, unwanted pregnancy and abortion, harmful traditional practices, and HIV. Adolescence is a transitional phase between childhood and adulthood; we use the World Health Organization’s (WHO) definition of any person aged between 10 and 19. This article draws on qualitative research in Ethiopia and Rwanda in 2016 with different groups of adolescent boys and girls: those in early (10-12 years), mid (13-15), and older (16-19) adolescence. Interviews were also conducted with adolescents’ peers and caregivers.
The analyses use a conceptual framework that reflects the close connections between the “3 Cs”: capabilities, change strategies, and contexts (Figure 1). Adolescents are situated at the center of this socioecological framework.
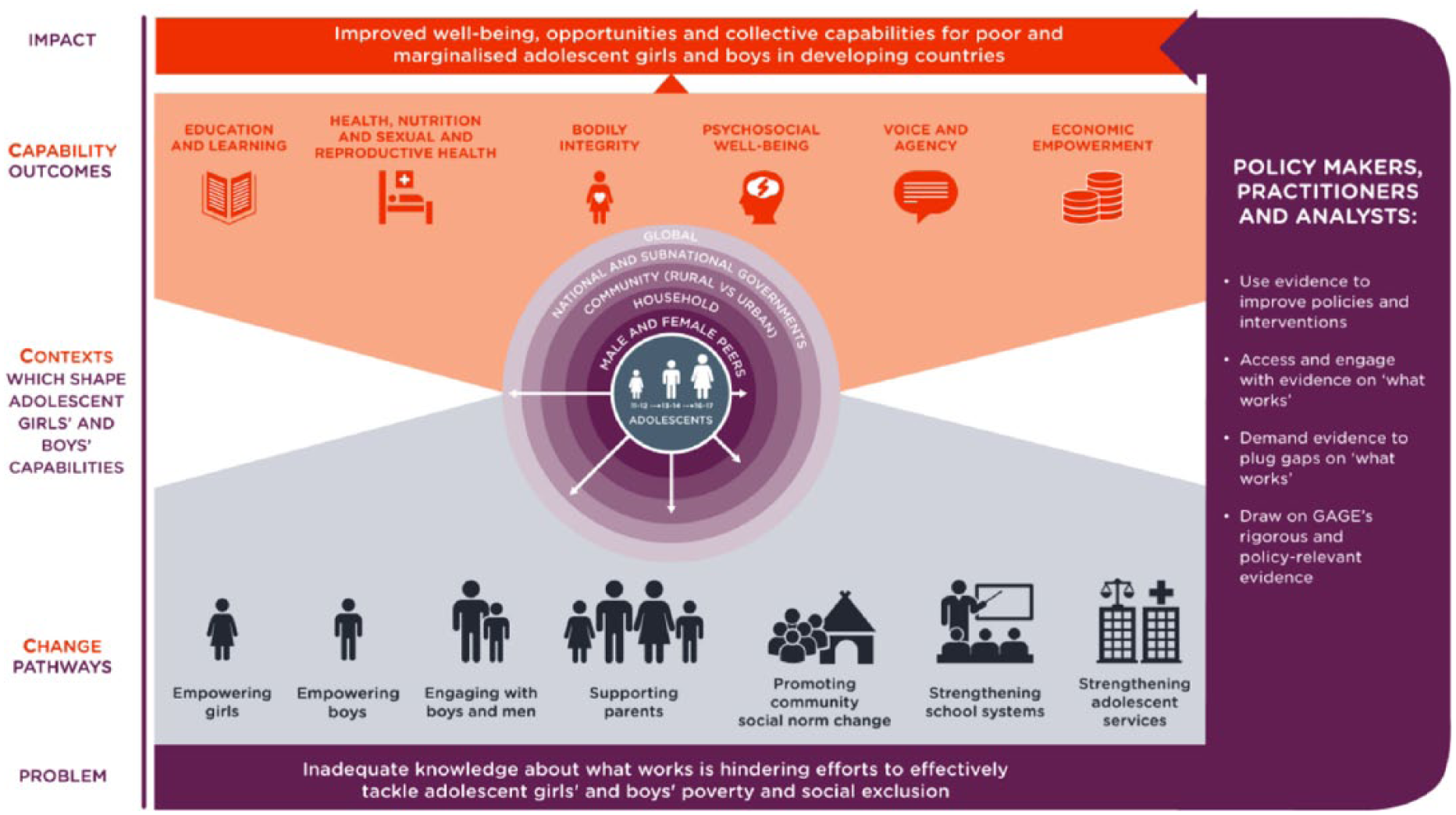
GAGE “3 Cs” conceptual framework.
The framework on capabilities, informed by Sen (1984, 2004), focuses on investments in the person as a whole, but is nuanced to better capture the complex gender dynamics that operate within households and more broadly across society (Kabeer, 2003; Nussbaum, 1997). The broad capability approach has been further developed to explore the different types of assets (social, economic, human, political, and emotional) that increase people’s capacity for “doing and being” in ways that they value. The approach also encompasses the deeply gendered processes by which adolescents acquire key capabilities during this unique life stage, as discriminatory gendered norms become more stringently enforced and more relevant as girls and boys (albeit in different ways) go through puberty. This article, which focuses on the SRH capability domain, looks at how and why young people’s experiences of SRH evolve during adolescence and how their access to information and services can mediate these experiences.
Our framework recognizes that adolescents of different ages have different needs and constraints, which are heavily influenced by a range of factors at the household, community, and state levels. Here, the focus is on two countries with relatively supportive policy and legislative environments, but which face chronic shortages of resources and capacity for implementation at the subnational level. Our analysis is guided by the central research question: How and in what ways are adolescents’ perceptions and experiences of SRH influenced by age and gender in Ethiopia and Rwanda?
Evidence on Ethiopian and Rwandan adolescents’ SRH and well-being is largely limited to those over the age of 15, with the needs of younger adolescents rarely addressed. Norms and customs often compel married couples to prove their fertility soon after marriage, just as they prevent unmarried girls from accessing contraceptives (despite, in some cases, a national policy environment that supports greater access to contraception). Discriminatory norms also prevent girls from being able to negotiate contraceptive use with a sexual partner (Chandra-Mouli, McCarraher, Phillips, Williamson, & Hainsworth, 2014; Harper et al., 2017; Patton et al., 2016). However, because early adolescence is such a formative period cognitively, socially, and physically in the life cycle and is increasingly recognized as a critical intervention window, it is important that we also expand our analytical lens to understand early adolescents’ experiences.
Our study includes very young adolescents (10- to 14-year-olds)—an age group for which there is little evidence on early experiences of SRH in sub-Saharan Africa (Chandra-Mouli et al., 2015; Rankin et al., 2016; Santhya & Jejeebhoy, 2015; Woog & Kågesten, 2017). We also include adolescents from diverse urban, peri-urban, and rural sites to complement the existing evidence base and to highlight diverse adolescent experiences in sub-Saharan African countries.
Context
Ethiopia and Rwanda are two of the fastest growing economies in Africa and also two of the most strongly governed (Kelsall, 2013). Both countries receive substantial amounts of donor support following ideologically led violent conflict and have strong governance structures and ruling elites. There is relatively little work, however, that explicitly compares contemporary experiences within these two countries (Goodfellow, 2017; Kelsall, 2013; Otten et al., 2009; Serneels et al., 2010). Although there have been significant improvements in SRH indicators for 15- to 19-year-olds over the past decade, adolescents in both Ethiopia and Rwanda still face significant challenges in addressing the sociocultural drivers of, and service provision for, SRH, reflected in broader SRH outcomes (see Table 1).
Adolescent SRH Variables, From the Latest DHS Data for Ethiopia and Rwanda.
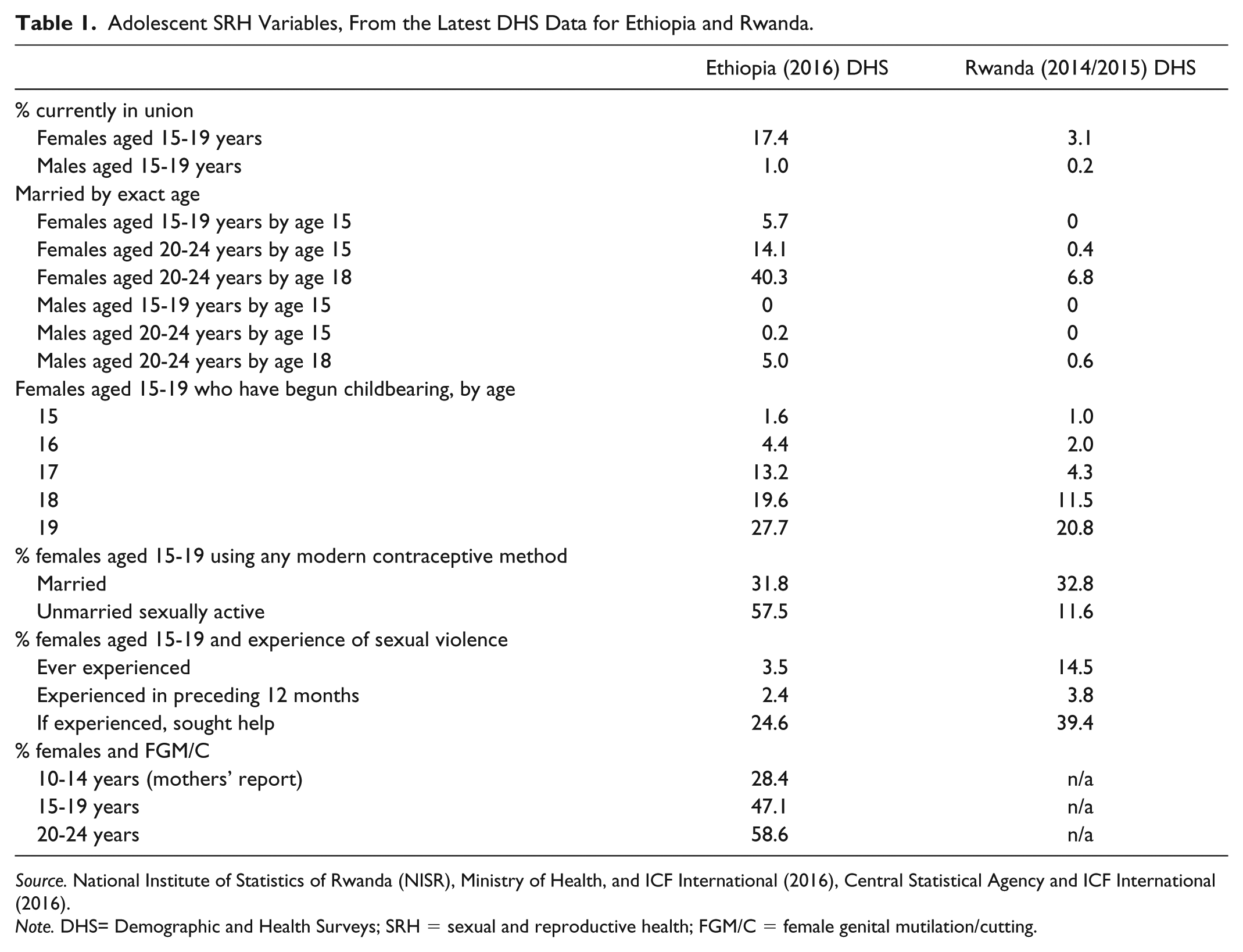
Source. National Institute of Statistics of Rwanda (NISR), Ministry of Health, and ICF International (2016), Central Statistical Agency and ICF International (2016).
Note. DHS= Demographic and Health Surveys; SRH = sexual and reproductive health; FGM/C = female genital mutilation/cutting.
Adolescent pregnancy is common in both countries. A fifth (20.8%) and a third (34%) of girls aged 19 have begun childbearing in Rwanda and Ethiopia, respectively (National Institute of Statistics of Rwanda [NISR], Ministry of Health, and ICF International, 2016). Females aged 15 to 24 in Ethiopia are 5 times more likely than their male peers to have contracted HIV (Central Statistical Agency [CSA] and ICF International, 2016); in Rwanda, older adolescent girls (aged 18-19) are 10 times more likely to contract HIV than their male counterparts (Bloom, Cannon, & Negroustoueva, 2014). In both countries, sexual violence is widely acknowledged to be underreported, and adolescent girls are known to experience a range of harmful traditional practices, including female genital mutilation/cutting (FGM/C) and early/forced child marriage (in Ethiopia), and labia elongation (in Rwanda). These challenges are set against national-level contexts that are—regionally—relatively enabling (Table 2).
National Legislation and Policy Frameworks Relating to Adolescent SRH in Ethiopia and Rwanda.

Note. SRH = sexual and reproductive health; IUD = intrauterine device; FP = family planning; MoH = Ministry of Health; HTP = Harmful Traditional Practice; TOC = Theory of Change.
The Ethiopian government launched a nationwide Health Extension Program in the early 2000s to provide health care workers and services (including free family planning) to populations in rural and remote areas, including adolescents. This was followed by the launch of the 2007 National Adolescent and Youth Reproductive Health Strategy, which recognized the need for quality and tailored reproductive health services for young people. Most recently, these efforts have expanded reproductive, maternal, newborn, and child health interventions to include adolescents, while the government has also committed to expanding youth-friendly services throughout the country as evidenced by Ethiopia’s Family Planning 2020 (FP2020) commitment. The key challenge, however, is implementation, specifically the need to overcome significant structural and social barriers that prevent Ethiopian adolescents from having equal access to family planning and other SRH information, care, and services.
In Rwanda, more than two thirds of families (71.5%) are covered by “Mutuelles de Santé,” a health insurance scheme launched in 2000 to offer affordable access to services (NISR, Ministry of Health, and ICF International, 2016). The Ministry of Health has also extended contraceptive services so that they are now available through community health workers at the village level. To address the lack of SRH services that are relevant to adolescents, and young people’s exclusion from processes of service design, in 2011 the Ministry of Health adopted the Adolescent Sexual Reproductive Health and Rights Policy. This set out measures to give adolescents greater access to information on family planning and health care prior to, during, and after pregnancy. It also introduced measures on cervical cancer, introducing a vaccine for younger girls (10-14 years) alongside information and counseling services (Abbott, Mutesi, Tuyishime, & Rwirahira, 2014; Binagwaho et al., 2013). Despite these recent improvements, there remain significant gaps in service coverage. More than half of girls (55%) reported at least one problem in getting access to health services (NISR, Ministry of Health, and ICF International, 2016). Some girls are not covered by health insurance, and even those who are may face high out-of-pocket costs. Adolescents, as a group, risk being stigmatized if they try to access SRH services and face specific barriers to doing so (Ministry of Health, 2011; 2CV, 2014; WHO, 2005). Indeed, evidence suggests that adolescents’ needs for accurate information about SRH issues are not being met (Abbott et al., 2014; Girl Hub, 2011). And although Rwanda is one of a handful of countries in the sub-Saharan Africa region that has made rape within marriage illegal (Rugege, 2015), there remain high rates of rape and other forms of violence against women (with many violations underreported) (Abbott, 2013; Government of Rwanda, 2014).
Method
This study is a comparative multimethod qualitative design. To ensure comparability across countries and sites, the same qualitative research methods and instruments were used. Evidence was generated from three communities in different geographical contexts (urban, peri-urban, and rural), in three Rwandan provinces (Northern [Musanze District], Eastern [Rwamagana District], and Southern [Nyaruguru District]), and in three of Ethiopia’s states (Oromia [West Hararghe Zone], Afar [Zone 5], and Amhara [South Gondar Zone]). A total of six settings—three in each country—were studied (Table 3).
Study Site Locations and Characteristics.

Note. Ethiopian Penal Code: https://www.wipo.int/edocs/lexdocs/laws/en/et/et011en.pdf. Rwandan Penal Code: https://www.ilo.org/dyn/natlex/docs/SERIAL/93714/109657/F1967095662/RWA-93714.pdf.
Republic of Rwanda (2015, p. 22).
The formative qualitative research included adolescents, their parents, other adults within the community, and key informants at local and provincial/regional levels. In Rwanda, there were 506 participants, including 184 female and 143 male adolescents; in Ethiopia, there were 516 participants, including 290 adolescents. Our sample size reflects the diversity of adolescents (male/female, younger/older adolescents, rural/peri-urban/urban, Ethiopia/Rwanda) whose realities we wanted to understand. For individual interviews where we sought to understand individual experiences and perceptions, our sample size rationale was as follows: In three sites in each country we sampled six adolescents of each gender for two age categories—10 to 12 and 13 to 15—to capture experiences pre- and post-puberty and aimed to get diversity in our sample between in-/out-of-school, working/not working, and married/unmarried. We emphasized evidence generation from and on very young adolescent girls aged 10 to 12 years as the evidence base is thinnest for this cohort. The primary evidence presented here is the result of a range of qualitative research methods with individuals and groups (Supplementary Material). To put participants at ease and to improve data quality, groups were divided according to gender and age, and group facilitators were of the same sex as participants and spoke the local language. Interviews with individuals (key informants) included representatives of the ministries of health, education, justice and gender/women’s affairs, as well as service providers and beneficiaries of adolescent programming.
Research tools used with adolescents included the following:
Individual decision-making charts, to gain insights into the decisions adolescents make about their lives.
A worries exercise, to explore what adolescents are concerned about and coping strategies.
Group interviews, using body mapping as a way to compare what kinds of work girls and boys do and what kinds of risks they face.
Community mapping, to understand how girls’ and boys’ mobility changes with age and the extent to which adolescents access health and other services and their relevance.
A vignettes exercise, to explore how social norms affect adolescent transitions.
For group tools (community mapping, body mapping, vignette exercises) aimed at capturing collective understandings of adolescence, mobility, safety, and related age and gender norms, we worked in groups of five to eight with two age groups in single-sex groups in each community.
Research tools focused on adults included the following:
Family life histories, to understand the broader context in which children make their unique transition through adolescence into adulthood.
Community timelines and institutional mapping exercises, to understand how local context histories and dynamics shape understandings of adolescence as a distinct life stage and the extent to which support services address adolescents’ vulnerabilities.
The research team received ethical clearance from the Overseas Development Institute (ODI) Ethics Review Board, as well as from the Rwanda National Ethics Committee and the Addis Continental Institute of Public Health (Ethiopia). For adolescents, we obtained assent from adolescents aged 17 years and under, and consent from parents or guardians, except in a minority of cases where the households were adolescent-headed. Assent and consent were obtained prior to any individual or group interview; where respondents or parents of adolescent respondents were illiterate or semi-literate, the information was explained orally, and a written sign and an audio-recorded statement of consent were taken. All respondents were provided with a confidential phone number for any concerns. This phone was monitored daily in the field and then checked periodically for 6 months after data collection. Even if families or adolescents lack their own phone, mobile penetration is sufficient for accessibility to be feasible; in communities with lower levels of mobile phone penetration, we additionally left contact details. We identified service providers in each community and informed local service providers or nongovernmental organization (NGO) providers where government services (e.g., for cases of abuse or neglect) were lacking.
Analysis
We developed a thematic code book informed by our conceptual framework and then looked at similarities and differences by cross-cutting variables—gender, age, geographic location, marital status, education status, and work status. The process of arriving at the thematic code book was iterative. We worked from the conceptual framework but then invited comments from all researchers involved in the fieldwork to sense check the codes and add/nuance as appropriate for the local context. Interviews were recorded and transcribed to English, where possible, by researchers who conducted the interviews in local languages. In Ethiopia, we worked with Amharic, Oromo, and Afar native speakers to carry out interviews in our three research sites. Coding was done in MAXQDA qualitative data analysis software. We worked with a limited number of experienced coders who were given common training, and the first 10 transcripts of each coder were shared across coders to check for intercoder reliability, and by spot checks thereafter. Following coding, we then explored the data according to the subareas of SRH of interest in the article to explore similarities and differences across and within country contexts.
Results
Three key interrelated gender themes emerge from our thematic analyses of qualitative evidence generated by our multimethods approach using a lens of SRH: puberty transitions, sexuality, and victim culpability. We draw on a wide range of SRH-related evidence generated by our research to demonstrate how gendered social norms across a range of contexts (Ethiopia vs. Rwanda, urban vs. peri-urban vs. rural) influence adolescents’ understandings and experiences. Particular attention is paid to the intersections of gender, context, and age.
Gendered puberty transitions
The physical transformations wrought by puberty are considered second only to those experienced in infancy and early childhood in terms of their scope and speed, and there is increasing understanding that puberty has impacts that reach far beyond visible sexual characteristics. Considering the gendered language used across contexts to refer to adolescents or adolescence gives clues to how this transition is socioculturally constructed. In Rwanda, these transitions are reflected in gendered language with two key words in Kinyarwanda for adolescence: adolescent male “ingimbi” (a young boy who has started developing secondary sexual characteristics), and female adolescent “umwangavu” (a young girl who has started being aware of cleanliness). These two words are expressing equivalence in terms of adolescence, but contain very different meanings and emphases of physicality for boys and appropriate behavior (being clean) for girls. In Amharic, the terms kobele and konjo refer to older adolescent boys and girls respectively, denoting those who display secondary sexual characteristics. In addition, each term has gendered connotations, with kobele denoting confident, often aggressive masculine behavior for boys, compared with konjo’s focus on being ready for childbearing and having heightened sexuality which needs “controlling” in the case of girls. Prepubertal adolescents are referred to as children using interchangeable Amharic words (mucha, lij, hitsan, kutara).
In our evidence, context affected experiences and outcomes of puberty with profound consequences for some adolescents’ future trajectories. The gendered aspects of the physical changes of puberty were frequently explicitly linked to future fertility, and in broad terms this was framed as something positive: When the girl menstruates . . . it is a good sign that she can give birth. The same for the boy, when he starts his adolescence, he can make the girl pregnant and then have a baby. (Key informant, adolescent program implementer, Rwanda)
However, when parents/caregivers and adolescents—particularly adolescent girls—discussed puberty, this tended to be in terms of the potential future risks. Our findings suggest that adolescents (particularly girls) know very little about puberty, especially periods and menstrual hygiene; because of this, menarche can be a frightening experience for many girls. Adolescents had varied levels of knowledge and understanding about puberty. For boys and girls alike, puberty was associated with changes in their physical appearance and changes in the behavior and roles expected of them by their family, peers, and the wider community: Young children dress the way they want even if their clothes are not clean but for teenagers, it cannot happen. (Body mapping with adolescent girls, 14-15 years, Rwanda)
Parents and caregivers who expressed concerns and fears about their child’s puberty tended to do so in relation to girls rather than boys. In part this can be attributed to menarche—a clearly defined event in puberty and one with implications for future fertility—as opposed to the longer period of adolescent transition. Many parents believe that menarche is a sign of maturity, and until that point, a girl is still a child. Such a clear marker of transition for boys is absent. Adults felt that puberty was now happening faster and younger than they anticipated: I was surprised to see how she was having fast-growing breasts, but now I see that it is becoming normal. (Mother of adolescent girl, Rwanda) In the past menstruation was not seen before you became 15 or 18 but now there are children who see menstruation at the age of 10 years. This is because of their nutritional consumption, when they have better care in their upbringing, they reach puberty earlier. (Adult key informant, health officer, Ethiopia)
The theme of puberty occurring earlier or faster than in the past was often framed by adults against broader changes in society—from urbanization to education to technology—with adults perceiving that intergenerational communication is now much more limited than in the past, meaning that adolescents are less able to benefit from advice from older people: In ancient time, parents used to sit and talk to the children. They used to tell them what might happen . . . Nowadays, it is rare to see parents talking to the children. (Adult key informant, adolescent girls’ program, urban Rwanda) There is a need for sexual reproductive health talks with boys and girls as parents are not talking to their children as before because they are busy. (Adult key informant, Department of Women’s and Children’s Affairs, Rwanda)
In all contexts, evidence from adolescent girls most frequently mentioned menarche and menstruation—not only the physical aspects (e.g., menstrual hygiene management) but also its affective consequences. The burdens, implications, and consequences of menstruation were, unsurprisingly, highly gendered. Younger female adolescents spoke about being scared and anxious about menstruation because they were worried about being teased and humiliated if people found out: When they see blood on us, they make fun of us. They are disgusted of us. They make us leave our seat in the class. They say that we smell. (10- to 12-year-old girl, Ethiopia) It [menstruation] is disgracing, your clothes might be seen when you are among others and when you stand up. (10- to 12-year-old girl, Ethiopia)
The implications of menarche in girls’ life course are highly context-specific. For some girls—particularly in some rural contexts in Ethiopia—menarche could represent an abrupt transition to marriage, raising the stakes (and responsibility) for girls to try to keep menarche and menstruation hidden: We keep it a secret. Otherwise they will marry us to someone we don’t love . . . (10- to 12-year-old girl, Ethiopia)
By contrast, in urban settings, menstruation and menstrual hygiene management did not emerge as a significant issue. Attitudes appeared to be more relaxed and open, and there was no mention of negative impacts on girls’ education: My mother was so open that she advised me about menstruation. She bought me and my sister pants and ordered us to go to toilet and to change it during our menstruation period. (Adolescent girl, urban Ethiopia) I will help my daughter to keep her hygiene and feel free by providing materials needed at that time and tell her this is natural. (Adult, mother, urban Ethiopia)
Lower menstruation stigma in urban areas was also attributed to girls’ clubs in schools: No, this [menstrual stigma] is not a major problem in urban areas. There are girls’ clubs in the school, which play roles in reducing the problems of girls, including on how they manage their menstruation. There is a changing room where the girls can change their sanitary pads when they are at school. (Adult key informant, education officer, urban Ethiopia)
In some communities, adolescent respondents reported getting information on puberty and menstruation as part of the school curriculum; in other communities, these lessons only appeared in the last year or two at primary school, so for many younger children, their only source of information was friends and family. In contexts where girls and boys were receiving information—whether from family members, school, or clubs—the negative affective components of puberty and menstruation appeared to be attenuated. For example, some girls also noted that they received information, support, and materials from schools or clubs, and some spoke of not being worried after having been taught about menstrual hygiene management: They teach us at school about menstruation and what to do. They tell us it is nothing to be ashamed of, that we only need to keep ourselves clean. (Interview, 10- to 12-year-old girl, Ethiopia)
Some of our respondents were in communities with school-based clubs for boys—such as Good Brothers’ Clubs—which were reported to significantly shift boys’ discourse around menstruation: We learn that we have to fully support girls while they are menstruating. We have to explain to girls who see menstruation for the first time that this is a natural phenomenon and she should accept it as a normal condition. (10- to 12-year-old boy, Ethiopia)
There were strongly gendered experiences of seeking and/or receiving information, however, with girls far more alert to the potential consequences of menarche and menstruation than boys. Nonfamilial sources of information were identified as important, with respondents recognizing that some people still believed menstruation was a sign of sexual activity and that this could stop young girls seeking advice from their parents: They [mothers] don’t like us asking about it. She will think I have started sleeping around. She will scold me. (10- to 12-year-old girl, urban Ethiopia)
Sexuality
Sexuality emerged as a cross-cutting theme in our analyses, distinct from—but often linked to—puberty transitions. Here, we refer to sexuality as . . . a central aspect of being human throughout life [that] encompasses sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy and reproduction . . . Sexuality is influenced by the interaction of biological, psychological, social, economic, political, cultural, legal, historical, religious and spiritual factors. (WHO, 2005)
Reflecting the breadth of sexuality, our evidence on sexuality and its gendered expressions ranges from marriage to childbearing to sexual purity to harmful traditional practices including FGM/C and labia elongation. Overall, there were substantially higher levels of monitoring and control of girls’ sexuality compared with boys’, and relatively few opportunities for intergenerational communication (adult-adolescent) about sexuality, reflecting patterns established in the literature (Amuyunzu-Nyamongo, Biddlecom, Ouedraogo, & Woog, 2005; Biddlecom, Awusabo-Asare, & Bankole, 2009) The strongest theme in our evidence from Ethiopia and Rwanda related to the control of girls’ sexuality relative to boys’. The form of that control was highly variable, ranging from advice When parents see that their daughters started being visited by boys, they know that it’s time to start talking to them about how they can protect themselves from problems and tell them that they may get pregnant when they have non-protected sex. (Focus group discussion, fathers, rural Rwanda)
to control of movement: Girls may face different things during the evening. One of these is rape. We do not send female children outside the home during the evening. Sometimes, they rape girls in groups. Only girls working in hotels and bars can stay outside the home during the night. (Adult woman, mother of adolescent girl, Ethiopia)
to threats of violence linked to nonmarital childbearing: My parents always warn me not to bring back a baby. My father threatens me that he will kill me if I bring back a child before marriage. (Body mapping, girls aged 10-12, Ethiopia)
to child marriage: My uncle married a small girl last year. He is an adult man but she is a small child. . .He is a rich man, and her parents wanted her to be married to a rich man. She was nine years old when she was married. (Boy, 11 years, Ethiopia)
In contrast, control of boys’ sexuality was rarely mentioned as problematic, with one exception related to changing technology. Adult concerns about changing society, possibly reflecting concerns about early onset of puberty, focused on changing modalities of information, particularly the Internet and mobile phones. In Rwanda, adults were concerned about the influence of the Internet in exposing their children to information about sex. Most parents and other adults held somewhat negative attitudes toward technology; adults feel that adolescent boys and girls are being corrupted by access to technology, particularly exposure to pornography: There is development and it brought some challenges because those pornographic movies encourage youth to have sexual intercourse because they are curious to know how it feels. (Key informant interview, teacher, Rwanda) When it becomes night they put in pornographic movies, and this attracts young people to do sexual intercourse. They watch how things are done and if someone is interested in practising that he finds another and they go somewhere together. (Key informant interview, teacher, Rwanda)
In addition, mobile phones were highlighted by adults as technology that exposed children to potential risk, particularly girls. In Rwanda, there was a concern about how mobile phones may be used as a way of drawing girls in to becoming sexually active with older men (“sugar daddies”) who have cash and can buy phones and other gifts for girls in return for sex.
Despite substantial legal change in both Ethiopia and Rwanda relating to age at marriage and the sanctions for early marriage, context-specific drivers of practices and norms relating to marriage, including child marriage for some populations, remain strongly embedded, particularly for girls. Despite growing awareness among Ethiopians that child marriage is illegal, it is perpetuated by strong and persistent norms around the need for girls to be virgins before marriage, reinforced by stigma associated with not having married by late adolescence: They want to marry their daughter before they lose their virginity. That is why many parents force their daughters to drop out from school and to marry early. (Key informant interview, District Head of Women and Children’s Affairs, Ethiopia)
In some cases, marriage “brokers” have emerged, who contribute to the problem by helping men trick young girls into marrying. In some Ethiopian communities, the practice of absuma (cousin marriage) persists: The issue of absuma is very difficult. Even if she loves somebody else, she will be married forcefully. Due to this, there are females who commit suicide. (Focus group discussion with fathers of adolescent children, Ethiopia)
Mothers have responsibility for knowing whether their daughter has reached menarche and facilitating marriage: If their menstruation is seen, the family may say “the time has arrived” and they may marry her off. So there is fear for this reason; they may hide it for a certain time, at least until she become stronger. (Adult, key informant, U/R/P-U, Ethiopia)
Evidence from this community suggested that most girls marry at 14 or 15 years, and young adolescents are aware that this is their likely trajectory, with little scope to negotiate: I worry because I am a girl. Had I been a boy, I wouldn’t have had to worry about abduction, early marriage or getting pregnant. Boys go to school and get to choose what they want to do. (Female adolescent, 14-15 years, Ethiopia)
Discussions about boys’ roles in abduction of girls for rape in Ethiopia tended to rationalize these behaviors as a consequence of the rising age of male marriage due to education: We can’t marry them [boys] off like the earliest times because we want them to reach a higher level of education. But then they reach the age (17 or 18) in which they develop sexual desire and want to have sex. At this time, they abduct a girl and rape her. (Key informant interview, community leader, Ethiopia)
By contrast, in Rwanda, the only legally recognized form of marriage is civil monogamous marriage, and the legal minimum age for marriage (for females and males) is 21 years, and people are generally aware of this: First of all, Rwanda and United Nations don’t allow a boy to marry a girl of 14 years old. When it happens in Rwanda, it is a violence case and it is punished. It is in the laws. (Focus group discussion, fathers of adolescents, Rwanda)
However, although many Rwandans know the minimum legal age for marriage, there were also reports of coresidential unions—often as a consequence of pregnancy—before the age of 21: They normally used to get married when a boy was around 25 and a girl was 18 or 19. But they can’t be married under the law, so they live together and wait until both of them are 21 years old or above. (Focus group discussion, fathers of adolescents, Rwanda)
Adolescents’ agency with regard to managing their sexuality in relation to fertility was highly variable, but always focused on girls’ responsibility to prevent pregnancy. In parts of rural Ethiopia, high levels of concern about sexual violence against girls appear to be driving the use of contraception as a way of preventing pregnancy if a girl is raped: The unmarried ones take contraceptives to protect themselves from unwanted pregnancy that comes due to rape and abduction. (Community mapping exercise, girls aged 10-12, Ethiopia).
Elsewhere in Ethiopia, likely reflecting the availability of contraception and safe abortion services, the management of fertility was presented as increasingly normalized: Adolescents of this time are taking contraceptives as soon as they marry. In the past, girls were giving birth immediately. This created birth complications. Nowadays, girls are aware and they are not exposed to such problems. (Adult, mother, Ethiopia) The health centre gives health education in the school and the health centre also gives safe abortion. (Key informant interview, Health Officer, Ethiopia)
In Rwanda, although unsafe abortion is practiced by adolescents, the restrictive abortion law and clandestine nature of abortion meant that it was not mentioned in our evidence. Although the Rwandan Ministry of Health has expanded community-based contraceptive services by trained community health workers, our evidence suggests that the uptake of these services by unmarried adolescents remains low.
In both Rwanda and Ethiopia, among some communities, the persistence of gendered harmful traditional practices, both with strong links to sexuality, was identified. In Ethiopia, this took the form of FGM/C, and in Rwanda, labia elongation. No harmful traditional practices related to boys’ sexuality were mentioned in our evidence.
In Ethiopia, our evidence about FGM/C was highly context-specific because of variations in the age and type of FGM/C, ranging from Type III (infibulation) to Type I (WHO). In areas where FGM/C is carried out in young adolescence (Chiro, Afar), it emerged as a significant bodily integrity concern for female adolescents. Different forms of FGM/C are practiced in other areas (e.g., Ethiopia), where it is done in early infancy, and our evidence suggested growing awareness of associated health risks possibly contributing to a decline in these areas: It was a problem in the past. However, it has greatly declined in the past four years. The government and NGOs have educated the people that female circumcision is a harmful traditional practice. In the past, it was said that uncircumcised girls become tinchat (sexually active). Now no parent organises the circumcision event for his or her daughters. We only circumcise our boys and we do this in the health centre. (Key informant interview with religious leader, male)
Irrespective of the timing and nature of FGM/C, the reasons for its persistence are strongly linked to gendered norms for controlling adolescent girls’ sexuality. This was frequently framed in terms of an uncut girl being considered to be “clumsy,” less likely to be obedient to a future husband, or to have stronger libido: The community is still practising females’ circumcision. Different myths and sayings are associated with it. Some say that uncircumcised females break home equipment. Some also say that they do not obey the will of their husbands. Due to these reasons, the community is widely practising circumcision, although some changes are seen . . . due to the fear of HIV/ AIDS transmission through the blades used for circumcision. (Key informant interview with male district prosecutor, Ethiopia) I swear there will be a problem if she is not cut . . . Her desire for men will be strong and that is a problem. (Mother of adolescent daughter, rural Ethiopia)
In areas with later and more invasive forms of FGM/C, the heightened awareness of the illegality or health consequences was suggested to contribute to the practice’s clandestine persistence: [The girl] got sick because of the circumcision and came to the hospital. She was told not to report as her mother forced her and she told us that she wanted to get circumcised. So the girl could not recover completely. She was bleeding. We do not know what will happen in the future. The people said that they stop it but there are cases and they go to other areas for it. The girls themselves are convinced to hide the situation for us so it creates problem for us to control it. (Key informant interview, District Health Office, rural Ethiopia)
In other areas (e.g., Afar), FGM/C persists, although our evidence suggests a transition to the less invasive (Type I) form of FGM/C known as sunna: I was cut . . . It is recently that parents are allowing their daughters not to be cut . . . But I am sure there are girls who undergo the sunna. [What about your daughters?] All have been cut. They were all born here so they were all cut. (Mother of adolescent daughters, rural Ethiopia)
In Rwanda, although FGM/C is not practiced, our evidence revealed persistence of labia elongation practices, with dissonance in reported attitudes and behavior about its practice. In group discussions, people would often deny that the practice existed; however, evidence from individual interviews suggested that adolescents did undertake the practice, as it is thought to make a woman more attractive. Some mothers reported that their husbands had asked them to suggest their daughters undergo labia elongation. Government officials, often aware of the practice, considered it “not healthy” for girls. Some girls said they knew about labia elongation, and some said they had practiced it; some said their peers had told them it would make childbirth less painful. Other girls said they had been told that it would make them grow up more quickly and make their (future) husband happy with them. Some girls said they had tried the practice but stopped because it was too painful. Within the community—in schools, for example—there were conflicting views. Teachers said they were not supposed to discuss it with students, but some said they felt that girls should know what it involves: I used to encourage the labia elongation practice in my discussions with Primary 6 female students, as the teacher in charge of female students. I considered it as an important culture. However, after I attended a workshop . . . I stopped telling the girls to do labia elongation. (Female teacher, urban Rwanda)
Victim blaming
The final cross-cutting gendered theme to emerge from our analyses is that of victim blaming; this was present across a range of SRH-related experiences and understanding and focused almost entirely on female adolescents’ (or oftentimes their mothers’) culpability. There was much more limited mention of perpetrator culpability, which was frequently linked to the challenges of attributing blame and punishment: Boys will fulfil their desire and deny their child later on. A girl might get raped and carry a child at an early age. She will have to drop out of school. Her life will be over. (Adult mother, focus group discussion, urban Ethiopia) Boys lobby girls to have sexual relationships with them, saying that they will marry them. After she becomes pregnant, the boy leaves her saying that the child does not belong to him. (Key informant interview, district chairperson, rural Ethiopia)
The gendered nature of cross-generational blaming is illustrated by this quote from a mother of an adolescent daughter who had become pregnant: Do you feel how it is painful to be disappointed by a child when she gets unwanted pregnancy . . .? That time you are blamed to be a stubborn mother. (Mother of adolescent daughter, rural Rwanda)
Adolescent girls have to contend with not only the stigma of being sexually active but also the blame for any consequences of their sexuality. This manifests in girls either not seeking SRH care or doing so in a way that minimizes the potential stigma. In Rwanda, health workers described how adolescent girls would seek contraceptive services by visiting the health workers’ home at night, rather than attending health services. Yet adolescent girls were blamed for not using the health services openly: And so when a girl faces an unwanted pregnancy it means she is not using the health services in the community . . . and so she is exposed to unsafe abortion. (Key informant interview, health officer, Rwanda)
Similarly, in Ethiopia, although contraceptive services are mandated to be available to unmarried adolescents, in some rural settings the community-level stigma was too strong—for girls and providers alike: To tell the truth we didn’t give training for the youngest women. Because when you talk about contraceptives, they didn’t have a willingness to communicate. They feel ashamed of themselves. (Key informant interview, health extension worker, rural Ethiopia)
Structural problems related to the justice system were highlighted in both Ethiopia and Rwanda. Despite legal provisions criminalizing rape, sexual violence, and sexual harassment, reporting rates remain low. Low reporting rates were attributed to victim blaming, especially for rape, with girls often blamed for provoking a sexual assault: In a community, it [rape] can happen, but we have a problem with the virginity tests because girls say that they have been raped after many days and the proof can’t be found and the person who was accused directly becomes innocent. (Key informant interview, female teacher, Rwanda)
Across settings and countries there was evidence of preference—perhaps reflecting a lack of any meaningful alternative formal legal option—for families of victims and perpetrators to reach an informal settlement: . . . Let’s say a young girl under 18 years old. You find many families are hiding that, even the young girl who got pregnant is not willing to reveal the father of her expected baby because of unknown reasons. And at the end of the day she may go live with him. So, that is a legal challenge because people don’t want to sue those who have committed offences against them. (Key informant interview, urban Rwanda) Elders settle such cases [rape] saying ‘No harm happened to her as she is mature enough for sex and after all the boy is her age mate.’ In our locality, reconciliation is common for such cases . . .We prefer reconciliation because our society is so connected and community affairs are the main concern. But if there is serious injury to the girl, there is no reconciliation. (Mother of adolescent daughter, urban Ethiopia)
It was clear that attempts to deal with perpetrator culpability in cases of sexual violence were limited. In Ethiopia, respondents described a key legal shortcoming, in that prosecutors have to present evidence “beyond any reasonable doubt,” reported as requiring three people to have witnessed the event. In a focus group discussion with adolescent boys, they discussed a case of a 12-year-old girl seen crying and bleeding after she had been raped. Although she was taken to the police station immediately to report the case and had shreds of the perpetrator’s shirt, because there were fewer than three witnesses willing to testify to what they had seen, the case did not proceed. Similar narratives emerged in Rwanda: Yes, there was a headmaster who raped his student and they put him in prison but after days they freed him because the doctor said there was no proof. (Key informant interview, community leader)
In Rwanda, although rape emerged as a key risk facing adolescent girls, evidence focused in more detail on a different form of sexual violence: intergenerational sexual relationships between young adolescent girls and older men (the “sugar daddy” phenomenon). Such relationship types are well established in the literature (Gerver, 2013; Luke, 2003; Rampazzo & Twahirwa, 2010; 2CV, 2014). In Rwanda, “sugar daddies” (who are usually married men) give girls gifts in return for sex. Adults tended to believe that if a girl was involved with a sugar daddy, it was the girl’s fault. Adolescent girls were blamed for dressing in a certain way (“indecently”) and attracting the type of men that would lead them into these sorts of relationships. In some cases, community members use the “sugar daddy” phenomenon as an excuse to blame pregnant adolescents, claiming that the girl wanted things that her family could not afford and so had sex with an older man purely for cash or gifts. In such cases, becoming pregnant was viewed as a punishment for the girl: You go where others are and they say that you are pregnant, you have a bastard child. For instance, yesterday, there was a woman and her child who insulted me, saying that I’m a prostitute, that I have given birth to a bastard. (Individual interview with adolescent mother, 14-15 years, urban Rwanda)
Discussion and Conclusion
Our comparative analysis shows how—despite considerable advances in many developing countries over the past 20 years in enhancing children and adolescents’ rights to SRH—for many girls and boys, the transition from childhood to adulthood remains fraught (Patton et al., 2016). The social category of gender and its related power relationships (within- and cross-generation) produce wide-ranging consequences for adolescents that operate to affect future life course. In our analyses, the expressions and consequences of these gender relations are shaped by context and mediated by individual capabilities and constraints. By generating evidence from younger (<15 years) and older adolescents in the two countries, our research makes a significant contribution to understanding how perceptions and experiences of SRH are shaped and evolve in early adolescence. Using a capabilities framework, our evidence shows how gendered processes of social exclusion (Kabeer) that differ between younger and older adolescents contribute to the (re)production of disadvantage for some adolescent girls. By comparing two countries with similarly strong governments, and considering contrasting contexts within each country (urban, peri-urban, rural), our evidence allows us to draw out how diverse context factors play a role in shaping the sexual and reproductive lives of adolescents. By emphasizing local variation in gendered sociocultural norms, our analyses show how context—operating at a variety of scale—can have a profound effect on SRH outcomes. At the smallest scale, families and households constitute the critical site in which age- and gender-related norms play out as parents seek to ensure conformity with social norms and enact sanctions for noncompliance. In our evidence, this ranged from exclusion of a pregnant unmarried adolescent to child marriage to traditional ways of sanctioning sexual violence.
At the meso level, our comparative research design (urban, peri-urban, rural) meant that we could take account of an important mediating factor in shaping the community-level opportunities and challenges for adolescents’ SRH. Urban areas appeared to offer reduced stigma around menstruation, combined with relatively higher levels of SRH service provision. Our study sites were drawn from a wide range of sociocultural norms and traditions; while families are often the site of compliance with social norms, community-level influencers (religious and traditional leaders) play a role in shaping or changing those norms and traditions. In Ethiopia, the championing by religious leaders of contraceptive services for adolescents in some settings meant a significant change in the community-level context of such services. In Rwanda, the roles played by some teachers in discussing labia elongation—and the tone of those discussions—were similarly important.
At the macro-level—that of the state—our ecological approach allows us to pay attention to the ways in which governance dynamics and institutions play a role in influencing adolescents’ SRH. In Ethiopia, the facilitating legal environment for abortion, particularly for adolescents aged under 18, stands in stark contrast to the highly restrictive legal environment of Rwanda (Basinga et al., 2012). This was reflected in our evidence from Ethiopia, particularly from adults, that acknowledged safe abortion as one of the ways in which adolescents might manage their fertility.
Both boys and girls in Rwanda and Ethiopia face multiple challenges—including a lack of information—in navigating puberty and its transitions (physical, social, economic, educational). Many girls, particularly in rural areas, are unprepared for menarche and menstruation. In some settings, particularly for in-school adolescents, the presence of school-based clubs that discuss menstruation appears to be game-changing. Although much rarer, boys’ clubs that include information and discussion of menstruation might contribute to breaking the culture of silence and cross-gender understanding of menstruation. Our evidence highlights the stigma and confusion that surrounds menarche, not least because for some girls it represents an abrupt transition to adulthood, signified by marriage and motherhood.
Adolescent girls in particular are highly constrained in their ability to navigate and negotiate sexual and reproductive transitions across a broad range of domains—from menstruation to FGM/C to choices around marriage (age at marriage, choice of partner) to (non)use of contraception and/or abortion to sexual behavior ((non)consensual). Despite substantial national-level progress in policies and frameworks to support adolescents, community-level norms and stigmas combined with services and providers that are either unwilling or unable to meet adolescents’ SRH needs mean that generations of adolescents continue to have sexual and reproductive lives characterized by coercion, stigma, and ill-health. Adolescent girls in age-asymmetrical sexual relationships—whether within or outside marriage—are at an “exceptional disadvantage” (Luke, 2003, p. 68) in negotiating whether or how they have sex in such relationships.
Our evidence shows starkly gendered differences in motivations for behaviors related to sexuality and reproduction. In some contexts in Ethiopia, this is manifesting in practices of abduction and rape of adolescent girls by adolescent boys. Adults in these contexts seek to explain these behaviors as boys’ responses to being unable to marry because they need to remain in education; absent from these explanations were discussions of consensual adolescent sexual relationships outside of marriage because of gendered norms around girls’ virginity at marriage. Evidence from adolescent girls in these contexts suggests that girls are changing their behaviors in anticipation of such sexual violence and are seeking contraception to avoid pregnancy in case of abduction rape. Simultaneously, parents seek to marry their girls at a young age to “protect” them from rape and/or nonmarital childbearing. Although restricted to just one of our Ethiopian study sites, this evidence demonstrates a perfect storm of gendered norms with negative outcomes for adolescent girls.
Adolescents experience a range of social norms and practices that discriminate against them due to their age, gender, or both. The timing of sexual initiation is highly dependent on the timing of marriage—and this is particularly clear in places where child marriage persists in some areas of Ethiopia. Child marriage in Ethiopia is associated with increased odds of suicidality (suicidal ideation and/or attempts; Gage, 2013), underscoring the consequences beyond SRH of this practice. In Rwanda, while marriage is illegal before the age of 21, childbearing and/or cohabitation are common at much younger ages. Frequently, this is driven by unintended pregnancy, precipitating a girl being forced to leave her natal home, either to live alone or to co-reside with the father of the pregnancy (if he “accepts” the pregnancy as his).
Meeting the SRH needs of sexually active adolescents—whether for contraception or maternity care—is a persistent and substantial challenge. In both Ethiopia and Rwanda, adolescent girls’ needs for SRH information remain largely unmet; they generally receive only partial (and often inaccurate) knowledge based on information they get from their peers. Misinformation is particularly common in rural settings where girls are less likely to be in school and where parents usually have lower levels of education and adhere to conservative social norms that largely preclude parent–child communication about SRH matters.
Our research did not focus specifically on abortion, although it was mentioned by research participants. In both Ethiopia and Rwanda, unsafe abortion among adolescents remains a critical SRH issue and is an important area for future research. While Ethiopia has one of the most progressive abortion laws in sub-Saharan Africa, which has been in place since 2004 (Melaku & Zeleke, 2014), legislative reform was more recent (2012) and less progressive in Rwanda (Basinga et al., 2012). Thus, a key question that needs to be addressed concerns the implications of these contrasting legal frameworks for adolescents in different settings within and across countries. Another key and related area for future research, not covered by our study, relates to adolescents’ experiences with maternal health care services, including similarities and differences between the experiences of married and unmarried girls.
Adolescents are not a homogeneous group; at different stages of their lives they need different things and face different constraints, which are highly dependent on a range of factors at the household, community and state levels. There is a pressing need for program designers and implementers in low-income countries in the sub-Saharan African region to address the role of underlying social norms in a more strategic and context-specific way if service provision, uptake, and outcomes are to be sustained. This is vital to ensure that all young people—including younger adolescent girls and boys—can realize their SRH rights and well-being.
Supplemental Material
sage_journals_Ethiopia_and_Rwanda_formatted_article_CLEAN_supplementary_material – Supplemental material for Adolescent Sexual and Reproductive Health in Ethiopia and Rwanda: A Qualitative Exploration of the Role of Social Norms
Supplemental material, sage_journals_Ethiopia_and_Rwanda_formatted_article_CLEAN_supplementary_material for Adolescent Sexual and Reproductive Health in Ethiopia and Rwanda: A Qualitative Exploration of the Role of Social Norms by Ernestina Coast, Nicola Jones, Umutoni Marie Francoise, Workneh Yadete, Roberte Isimbi, Kiya Gezahegne and Letisha Lunin in SAGE Open
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Gender and Adolescence: Global Evidence (GAGE) programme which is funded by UK Aid from the UK Department for International Development (DFID).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.