
Abstract
Abuse of injections, particularly in resource poor countries, remains a challenge evident in the increasing preference for therapeutic injections over oral medication. Objective of this study is to explore factors associated with patients’ preference for therapeutic injection over oral medication in the Volta Regional Hospital, Ho in Ghana. The study is a cross-sectional survey conducted among 200 patients accessing care in Volta Regional Hospital. Data were analyzed using STATA statistical software for data analysis. Univariate probit regression was used to ascertain factors associated with patients’ preference for therapeutic injections over oral medication (main outcome variable of interest). It was found that 74% of the 200 respondents preferred injection to oral medication. More outpatients preferred injectable medication over oral (p = .041); 86% of the respondents said they never experienced complication related to injectable medication. Patients who perceived injection as more efficacious were more likely to opt for it over oral medication (coefficient = 2.22; SE = 0.33; p < .05). It is concluded that patients’ preference for injectable medication over oral remains high in Ghana, and this preference is significantly associated with patients’ perceptions on superiority of injections over oral medication. There is the need to intensify health education for clients and in-service trainings for health providers to control abuse of therapeutic injections and promote patient safety.
Keywords
Plain Language Summary
Abuse of injections, particularly in poor countries, remains a challenge because of the increasing preference for therapeutic injections over oral medication. This research work sought to find out why health care clients prefer injections to oral medications in a major referral hospital in the Volta Region of Ghana.
At the end of the research, it was discovered that two thirds of patients visiting the Volta Regional Hospital (VRH) preferred therapeutic injection to oral medication. Predominant reasons for preference of injection were perceived quicker action, difficulty with oral medication compliance, and addiction to injectable medication. Also, patients who perceived therapeutic injection as more efficacious were more likely to opt for injections over oral medications.
Based on these results, the researchers recommend the need to increase public education for clients and health providers to control the indiscriminate use of injections in health care settings toward promoting the safety of patients.
Introduction
Increasing preference for therapeutic injection over oral medication remains a public health concern to health systems across the globe, especially in resource poor settings such as Ghana. Existing knowledge gaps on medical information among patients coupled with insufficient implementation of health policies aggravates this challenge. According to a World Health Organization (WHO, 2015a) report, every year, billions of injections are used worldwide and over 95% are for therapeutic or pharmacological purposes. Even though therapeutic injection administration is a global phenomenon, its abuse particularly in developing countries remains a challenge evident in the increasing preference for therapeutic injections over oral medication (Poulos et al., 2016). Empirical studies have showed that about 70% of therapeutic injections administered are unnecessary as oral medications could have worked in most cases (Adejumo & Dada, 2013; Fox et al., 2013; WHO, 2015a, 2015b).
Notwithstanding increasing empirical evidence of the side effects and complications associated with therapeutic injections (Onyemocho, Anekoson, & Pius, 2013; WHO, 2015b), some health care clients prefer them to oral medications with varying reasons.
Patients’ preference for therapeutic injections has been attributed to a number of factors including, perceived efficacy over oral formulations and economic benefits of therapeutic injections to providers.
Other factors associated with increasing preference for injectable medications are the weak regulatory policies on therapeutic injection practices in some countries, especially in Africa (Menzin et al., 2013). In Ghana for instance, even though the Ministry of Health (MoH) has internal protocols and guidelines on rational use of drugs including therapeutic injections (MoH, 2014), adherence to these protocols by clients and health care professionals is largely low.
A number of empirical studies have come out with varying conclusions on patients’ preference for therapeutic injection 1 or oral medication 2 (Abdulebar, Tesfaye, Gedif, & Gebre-Mariam, 2007; Al Kanaani, Mahmud, Kouyoumjian, & Abu-Raddad, 2018; Nsimba, Gesase, & Massele, 2011; Nsimba, Massele, & Kayombo, 2011). However, many of these studies were conducted outside Ghana, hence the motivation for this current study. For instance, some previous studies suggest that patients measure the quality of health care they receive by the number of therapeutic injections prescribed and administered (Alhassan et al., 2015; Alhassan et al., 2016; Kermode, 2004; Kotwal et al., 2004).
Furthermore, there is dearth of empirical studies on patients’ preference for treatment choice, particularly, regarding injectable and oral medications in Ghana. This study thus sought to explore determinants of patients’ preference for therapeutic injections over oral medications in the VRH in Ho, Ghana. It is expected findings of this study would help inform policy decisions on client education and enforcement of standard professional practices on rational use of drugs in Ghana and beyond.
Method
Study Design, Population, and Setting
This is a descriptive cross-sectional survey conducted in the VRH, Ho in the Volta region of Ghana. As at 2014, the VRH had a 240 bed capacity, comprising 42 units/departments and staff strength of 542. These staff comprised 232 nursing professionals, 23 medical doctors, and 287 paramedical staff. The VRH had bed turnover rate of 29.3%, and bed occupancy rate of 72.9% (VRH, 2014).
Sampling and Sample Size Determination
Purposive sampling method was used to select inpatients and outpatients who have had therapeutic injection administered to them at least in the last 6 months. The sample frame for this study was inpatients and outpatients accessing health care at the VRH. Based on Krejcie and Morgan (1970) formula 3 for sample size determination for known population, a sample size of 205 was deemed representative of the estimated population of 440 inpatients and outpatients who attend the VRH on daily basis. Subsequently, 205 structured questionnaires were administered to the study participants who met the inclusion criteria.
Inclusion and Exclusion Criteria
All inpatients and outpatients attending the VRH and have had an injectable and oral medication experience in the last 6 months were included in the study. Patients who were also 18 years or more were included in the study. Exclusion criteria included patients who refused to consent voluntarily for the study. Likewise, minors below the ages of 18 years were excluded from the study. Finally, patients who were in critical chronic and emergency medical conditions were not considered because of their health status.
Data Collection
Questionnaire were piloted using 10 patients at the Ho Polyclinic to check for ambiguity, to ensure clarity of questions and relevance of responses. Data collection was done by trained research assistants from the School of Nursing and Midwifery, University of Health and Allied Sciences, Ho, for nearly a month.
Out of the 205 administered questionnaires, 200 were successfully retrieved with complete information representing approximately 98% return rate. The data exported to STATA were further disaggregated into two subsamples of inpatients (n = 50, 25%) and outpatients (n = 150, 75%).
Data Analysis
Data from the field was coded, captured, and cleaned using Microsoft Excel Spreadsheet and subsequently exported to STATA statistical software (version 12.0) for the data analysis. Data coding was done to ensure anonymity of respondents. To promote internal validity of the data collection tool, all questions were informed by research objectives and reviewed literature.
Parametric (univariate probit regression, VCE robust, and independent t-test) and nonparametric (chi-square and Fisher’s exact) tests were used in the data analysis to test various hypotheses as appropriate. Multicollinearity diagnosis was conducted on all the explanatory variables prior to their inclusion in the regression model. The average variance inflation factor (VIF) was found to be 1.31, which is below the 10.0 rule of thumb necessary for exclusion from the regression model (Alhassan et al., 2016; Greene, 2002; Tabachnick & Fidell, 2001).
Findings
Results from the field data showed no significant difference in the average age of inpatients (32.8; SD = 11.1) and outpatients (33.4; SD = 13.5); little more than 60% of the patients interviewed were females, and the remaining were males; 63% of outpatients were from urban areas compared with 37% who were from rural areas (p < .05). Table 1 shows other sociodemographic details of respondents.
Summary Statistics on Patients’ Sociodemographic Characteristics.

Source. Field Data (2017).
Note. n = number of valid responses; f = frequency.
1-sided Fisher’s exact (p < .05).
On exposure to therapeutic injection, it was found that a significant proportion of outpatients (44.6%) had no exposure to therapeutic injection compared with 18% of inpatients (p = .003); moreover, 24% of inpatients indicated they received therapeutic injection more than three times in the last 1 month compared with 8.8% of outpatients (p < .05; see Table 2).
Experiences of Patients With Therapeutic Injections.

Source. Field Data (2017).
Note. n = number of valid responses; CI = confidence interval.
Number of times patients received therapeutic injection in the last 6 months.
1-sided Fisher’s exact (p < .05).
Overall, 49 (24.5%) of the respondents indicated they received therapeutic injectable medication outside a health facility environment. Out of this number, majority were inpatients who mostly patronized pharmacies (80%), chemical shops (10%), and home-based personal arrangements (1%; p < .05; see Table 2).
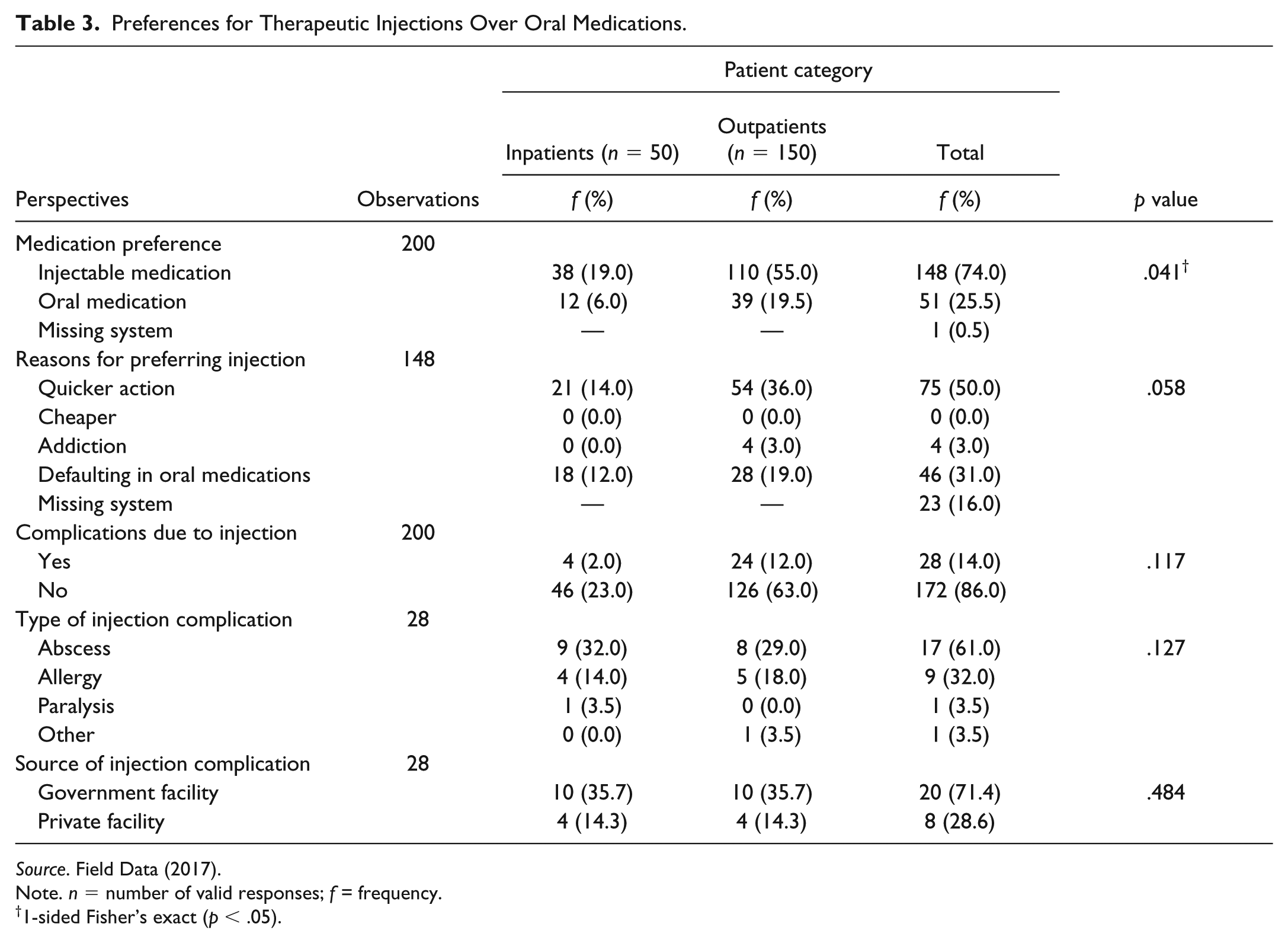
Out of the 200 valid responses, it was found that 74% said they preferred therapeutic injection to oral medication. More than 50% of the outpatients said they preferred therapeutic injection to oral medication compared with 19.5% of inpatients (p = .041). A further univariate probit regression test however showed these differences are not statistically significant even though the Fisher’s exact test suggests otherwise. The predominant reasons given by respondents who preferred injectable medications were perceived quicker action (50%), difficulty with oral medication compliance (31%), and addiction to injection (3%; see Table 3). Majority (86%) of the respondents indicated they have never experienced a complication related to therapeutic injection; 14% said they have suffered complications from injectable medication. Table 3 shows details of patients’ experiences with complications related to therapeutic injections.
Preferences for Therapeutic Injections Over Oral Medications.
Source. Field Data (2017).
Note. n = number of valid responses; f = frequency.
1-sided Fisher’s exact (p < .05).
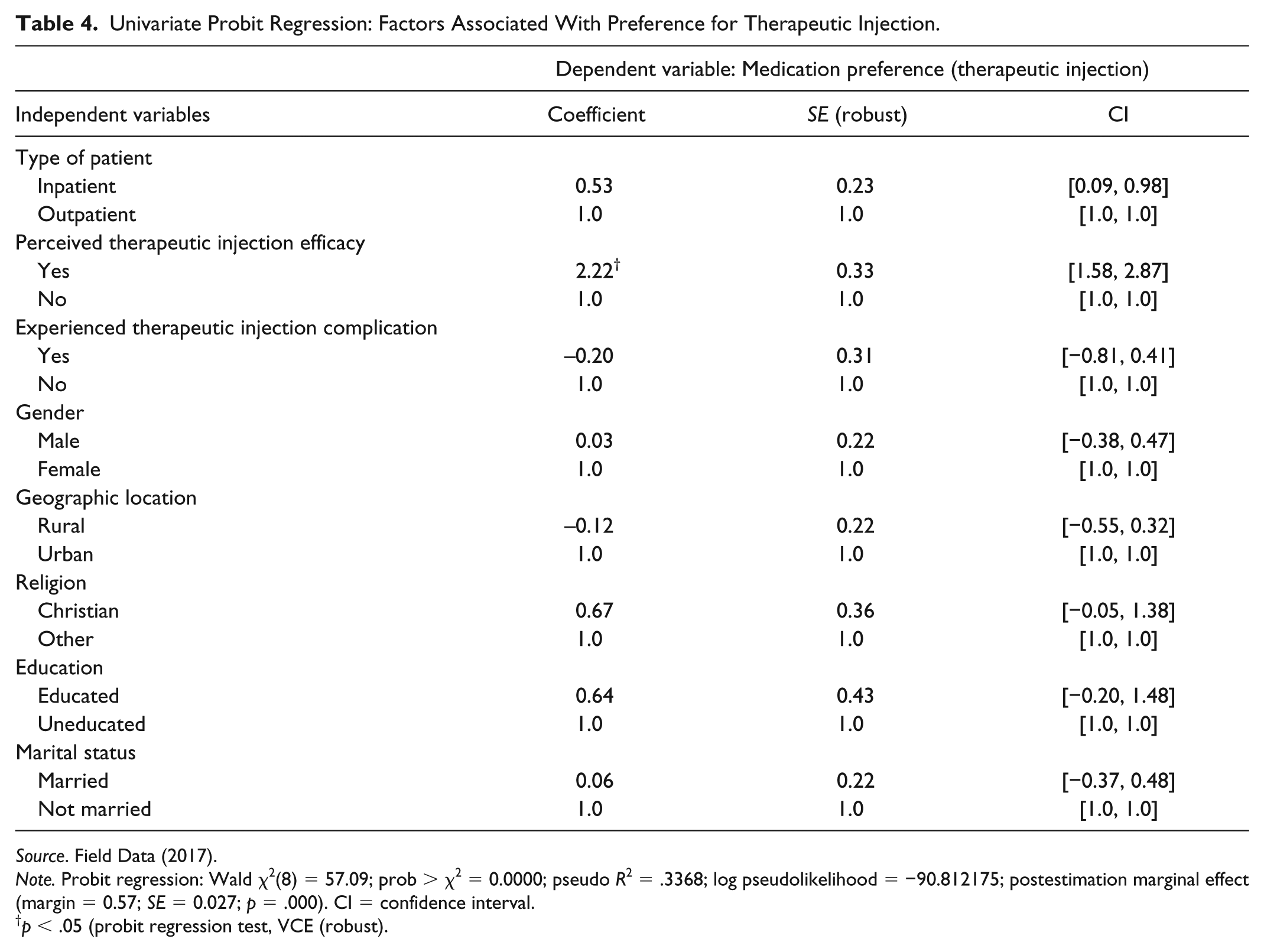
It was also observed that patients who perceived therapeutic injection to be more efficacious than oral medication are more likely to opt for injectable medication (coefficient = 2.22; SE = 0.33; p < .05). Religious affiliation of patients also appeared to have an association with patients’ preference for therapeutic injection over oral medication. It was observed that Christians are more likely to choose therapeutic injection than other forms of religious affiliations even though this association was not statistically significant (see Table 4). Likewise, factors such as gender, rural–urban location, education, and marital status were not statistically significant predictors of patients’ preferences and choice of injectable medication over oral medication.
Univariate Probit Regression: Factors Associated With Preference for Therapeutic Injection.
Source. Field Data (2017).
Note. Probit regression: Wald χ2(8) = 57.09; prob > χ2 = 0.0000; pseudo R2 = .3368; log pseudolikelihood = −90.812175; postestimation marginal effect (margin = 0.57; SE = 0.027; p = .000). CI = confidence interval.
p < .05 (probit regression test, VCE (robust).
Discussion
It was found that contrary to study findings on United Kingdom (Mason, Crosson, Mason, & McGwin, 2017), 74% of the 200 respondents in this study said they preferred therapeutic injection to oral medication. Moreover, significant difference was found in the responses of inpatients and outpatients with more outpatients stating their preference for therapeutic injection than their inpatient counterparts. Likewise, Fallowfield et al. (2006) in a study on United Kingdom found that nearly two thirds of the patients preferred oral tablet medication to therapeutic injection. Convenience and dislike of needles were reasons cited for patients’ preference for oral tables, whereas the few who preferred therapeutic injection cited better adherence and personal preference.
In this study, it was observed that difficulty with oral medication compliance was mentioned as one of the key reasons for patients who preferred therapeutic injection. As found in similar studies (Fallowfield et al., 2006; Mason et al., 2017), perceived quicker action was mentioned by half of the patients who preferred therapeutic injection. These findings, appear to confirm the existing anecdotal claims that many patients in developing countries such as Ghana prefer therapeutic injection to oral medications, contrary to patients’ health seeking behaviour in many developed countries (Fallowfield et al, 2006).
Albeit this study could not access relevant comparative literature, this divergence in findings might be attributed to the differences in study settings as developed countries with better health care systems are more likely to have better informed patients which could influence their health seeking behaviour and treatment choices.
However, it appears this assumption might not necessarily apply to all Western countries. Some studies in the Western world have revealed high preference for injectable medications by patients as compared with other treatment options. For instance, Mason et al. (2017) found greater proportions of diabetic patients who preferred therapeutic injection to laser treatment in the United States.
In terms of actual exposure to therapeutic injection, nearly all the 200 respondents (particularly inpatients) said they received therapeutic injection in the last 6 months. This observation could be attributed to the fact that many inpatients are likely to suffer from chronic and perhaps complicated conditions that demand more radical and invasive treatment options such as injections (Mason et al., 2017). Conversely, many outpatient conditions are usually less complicated and most probably managed with oral medications. In Ghana, this practice is in line with the MoH and Ghana Health Service (GHS) policy guidelines on rational use of drugs where invasive procedures such as therapeutic injections are discouraged for outpatient conditions (MoH, 2014).
It was also found in this study that only a few of the patients who ever received injectable medication knew of the reason for an injection administration. Moreover, significant number of the respondents (largely outpatients) indicated they ever received an injectable medication outside a health care facility. These revelations largely corroborate conclusions in previous studies where patients exhibited significant knowledge deficit on their medical treatment protocol partly due to knowledge asymetry between patients and medical professionals (Alhassan et al., 2015; Alhassan et al., 2016).
Also, reliance on unsafe outlets for therapeutic injection has been found to be prevalent, especially in Africa where poverty and limited medical knowledge compels health care clients to rely on these unsafe sources for therapeutic injection (Nsimba, Gesase, et al., 2011; Nsimba, Massele, et al., 2011). In this study, it was found that patients who took therapeutic injections outside a health care facility did so at either a pharmacy, chemical shop, or at home.
However, this study could not determine specific conditions that warranted the respondents to take their therapeutic injections at home as the case might be with chronic diabetic patients who are put on routine insulin therapeutic injection.
Experience of therapeutic injection–related complications was found to be minimal among the sampled patients; this observation could be attributed to the fact that the study site is a regional referral facility where there are more qualified health personnel which has the potential of reducing the risk of therapeutic injection complications (Alhassan et al., 2016; Obionu, 2007; Reid, 2010). Moreover, there are few published empirical literature on complications due to therapeutic injection in Ghana to form the basis for national level comparison with the current study.
On the determinants of patients’ preference for therapeutic injections, significant differences were observed between inpatient and outpatients with the latter more likely to opt for therapeutic injection. This observation contradicts similar previous findings (Kotwal et al., 2004; Mason et al., 2017) where patients receiving inpatient care expressed higher preference for therapeutic injections than those who were not.
Also, this study found that patients who perceived high efficacy of therapeutic injection were more likely to choose therapeutic injection over oral medication similar to findings in previous studies where perceived efficacy was found to be a key determinant of patients’ preference for therapeutic injection over other treatment options, especially in Africa (Kermode, 2004; Kotwal et al., 2004; Nsimba, Gesase, et al., 2011; Nsimba, Massele, et al., 2011).
Conclusion
Preference for injectable medication among patients remain high in Ghana as found in this study. It was observed that patients’ perception of therapeutic injection efficacy significantly influence their chances of opting for therapeutic injection over oral medication. In light of this health-seeking behavior by patients, there is the need to intensify public education for patients and routine inservice training for health care providers to promote rational and safe use of therapeutic injections. The role of nursing professionals in this discourse is particulalry critical since therapeutic drug administration is a core nursing function in the clincal setting. Additionally existing policy regulations on rational use of drugs should be rigorously enforced to the latter to ensure high compliance by prescribers at the health service delivery points to promote patient safety and quality healthcare delivery.
Limitations
This study was conducted in a regional referral hospital which is likely to influence the caliber of patients visiting the facility and their experiences with therapeutic injections. Also, since hospital was used in the study it poses generalizability challenges to other regions in Ghana whose patients may have different health-seeking behavior because of sociocultural differences.
Finally, the use of purposive sampling technique to recruit the participants might have introduced some level of bias. Nonetheless, adopting a representative sample size based on the known study population gives credence to the findings of this study.
Suggestions for Future Research
Future studies could consider isolating the specific disease conditions of patients and their preference for therapeutic injection as this study did not delve into this nuance. Furthermore, future researchers could attempt a comparative study of patients accessing care in private and public health care facilities to unearth potential differences in the health-seeking behavior of these patients. Finally, a nation-wide study involving selected health facilities in all the 10 regions of Ghana could help understand the regional and cultural dynamics in patients’ preferences for treatment options.
Footnotes
Acknowledgements
We acknowledge the support and cooperation of the inpatients and outpatients of the Volta Regional Hospital. We also express appreciation to the workers and management of the Volta Regional Hospital for granting us the permission to conduct the study in the hospital. We also express our appreciation to the management and faculty of the School of Nursing and Midwifery of the University of Health and Allied Sciences (UHAS) for their peer reviews and recommendations throughout this study. Last but not the least, the following 2016/2017 academic year Level 400 students of the Department of Nursing are acknowledged for their tireless efforts in the data collection, entry, and management. The students are Appiah Bismark Adu-Gyamfi, Gbekor Awoenam, Ayensu Bright, Owusu Angela, and Agbolosu Oliver.
Ethics Approval and Consent to Participate
Administrative ethical approval was given by the University of Health and Allied Science (UHAS) Research Ethics Committee (REC). Questionnaires administration were preceded by informed consents sought from each respondent. Respondents who were illiterates, thumb-printed on the consent form after reading and interpreting the content of the informed consent. Literate respondents however signed to consent for the study. The participants were informed of their right to participate or withdraw from the study without any consequences. Full disclosure of information to participants was made and their confidentiality and privacy maintained throughout the study by anomymising the data with unique codes.
Availability of Data and Materials
All data supporting our findings are contained in the manuscript. There are no restrictions to data sources per se but details of the full data may be accessed through one of the lead researchers, Dr. Robert Kaba Alhassan, email:
Consent to Publish
All authors of this manuscript consented to publishing findings of this study
Authors’ Contributions
A.B.A., A.B., A.O., G.A., O.A., and R.K.A. initiated the conceptualization and writing of the paper. A.B.A., A.B., A.O., G.A., O.A., and R.K.A. collected, entered, and cleaned field data. R.K.A. and E.N. provided advice on the analysis and interpretation of results. R.K.A. and P.P.M. reviewed the manuscript and provided expert advice from the public health and health policy perspectives. All the authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.