
Abstract
Premarital sex and premarital childbearing is a source of stigma in many African communities and can negatively affect adolescent girls’ sexual and reproductive health experiences. This study seeks to provide insight into the strategies adolescent girls adopt to avoid stigmatization due to premarital sex and/or childbearing by their community members and families. Using a mixed methods approach, data were collected from a survey of 500 adolescent girls out of which 20 were purposively selected for in-depth interviews. The strategies adopted by adolescent girls to avoid stigma varied based on the pregnancy status of girls, that is whether they have never had a child (nonpregnant [NP]) or had ever had a child (ever-pregnant [EP]). To avoid stigma associated with premarital sex, some NP girls abstained from sex and others who were sexually active either kept their relationships secret or used contraceptives secretly. For the EP girls, some tried to minimize stigma to premarital childbearing by going back to school after childbirth or learning a trade or a vocation. Some EP girls also got married to the fathers of their babies to avoid stigma. Overall, the desire to feel accepted by community members pushed adolescent girls to adopt strategies to avoid the stigma associated with premarital sex and childbearing. It is recommended that there should be creation of awareness for community members on the need to support adolescent girls to minimize the risk they may be predisposed to in their sexual and reproductive health.
Background
Previously, most societies in sub-Saharan Africa were guided by norms and values that proscribe sex before marriage and thus, adolescent girls were expected to be virgins at marriage. In such societies, girls who became pregnant before marriage were severely punished and this included punishments such as banishment from the community (Bleek, 1981; Sarpong, 1977). In recent times these forms of punishment no longer exist, rather new forms of punishing adolescents who deviate from the societal norms and values have emerged, high among them is stigmatization. Stigmatizing adolescent premarital sex and childbearing depends on the sociocultural context. In Ghana, premarital sex and childbearing is stigmatized among many ethnic groups, despite the fact that society places value on children and the role they play in families and marriages. In societies where premarital sex is proscribed, girls who engage in premarital sex stand the risk of being stigmatized should society find out or see signs that suggest it (Yardley, 2008).
The long wait between puberty and marriage has contributed to the increasing number of adolescents having sex and bearing children out of wedlock (Agunbiade, 2014; Gyan, 2017; Moloney, Hunt, Joe-Laidler, & MacKenzie, 2011; Zwang & Garenne, 2008). Adolescents are postponing age at marriage because of factors such as urbanization, migration, and formal education (Addai, 2000; Awusabo-Asare, Abane, & Kumi-Kyereme, 2004; Biddlecom, Gregory, Lloyd, & Mensch, 2008; Glover et al., 2003; Gyan, 2017). Increasingly, more adolescents are postponing the age at marriage; however, the age at first sex remains low. Ahlberg argues that with the changes taking place in society adolescents are confronted with conflicting values from the traditional, religious, legal, and romantic systems in society (Ahlberg, 1994). The traditional and religious value systems applaud chastity before marriage (Addai, 2000; Ahlberg, 1994; Marston & King, 2006) and the legal value system regulates the age at sexual consent (16 years) and age at marriage (18 years) (Criminal offences Act 29 section 14). The romantic love value system which is more of a personal decision is characterized by romantic ideas of friendship and love (Ahlberg, 1994; Awusabo-Asare et al., 2004). Navigating through these value systems may predispose girls to stigma when they are not chaste before marriage or when they go on with their own value of romantic love.
Stigmatizing premarital sex and childbearing have been observed to have dire consequences on adolescent girls’ sexual and reproductive health experiences (Blanc, Tsui, Croft, & Trevitt, 2009; Morris & Rushwan, 2015). Adolescent mothers may limit or not access or utilize reproductive health services for fear of stigmatization (Morris & Rushwan, 2015). Thus, they may not seek for early prenatal and postnatal care which may lead to late detection of complications that could affect the health and well-being of both mother and child. Sexually active adolescent girls may not seek for information on safe sexual practices or access services that promote safe sexual behavior (Blanc et al., 2009). This notwithstanding, some adolescent girls have adopted their own strategies to avoid the stigma of premarital sex and premarital childbearing to pass as “normal” in their communities. What strategies do nonpregnant (NP) adolescent girls adopt to avoid stigma to premarital sex in their community? What strategies do adolescent mothers adopt to minimize stigma to premarital childbearing in their community? This study seeks to provide insight into the strategies adopted by adolescent girls in a peri-urban community in Ghana to avoid stigma to premarital sex and premarital childbearing. Lessons from the adoptive strategies of girls can help to address the unmet needs of adolescent girls in their sexual and reproductive health experiences.
Stigmatizing Adolescents’ Premarital Sex and Childbearing
In most societies, accessing reproductive health services is associated with sexual relations. This perception tends to affect adolescents who may not want to seek such services for fear of being labeled as engaging in sexual relationships. Stigma, according to Goffman (1963), can be defined as “an attribute that is deeply discrediting” (p. 3). Goffman (1963) distinguishes discredited stigma where the source or cause of stigma is clearly known or visible and discreditable stigma where the source or cause of stigma is not visible and is unknown. Stigma can be classified into abominations of the body, blemishes of individual character and tribal stigma (Goffman, 1963). Premarital sex and premarital childbirth can be classified under blemishes of individual character and tribal character in this study. What is defined as a blemish of an adolescents’ character or tribal stigma is determined by the norms and values of their society (Sawyer et al., 2012). Adolescent girls having premarital sex and having children out of wedlock is an individual character that discredits them and may extend to members of their nuclear family. Adolescent girls’ sexual and reproductive health behaviors are usually stigmatized through labeling, discrimination, stereotyping, separation, and status loss (Imoro, 2009; Link & Phelan, 2001; Morhe, Tagbor, Ankobea, & Danso, 2012). For instance, girls who seek for information on sexual and reproductive health may be labeled as “bad girls” by the service providers, their family, or the community members (Ampofo, 2001; Gyan, Ahorlu, Dzorgbo, & Fayorsey, 2016; Yardley, 2008). Adolescent mothers may face discrimination from institutions such as schools, health workers, and health service providers when they seek their services (Imoro, 2009; Yardley, 2008). This is manifested when they try to access sexual and reproductive health services such as going for prenatal and postnatal care including family planning clinics. In Goffman’s view, the consequences of being stigmatized could be status loss or social rejection. With status loss, the stigmatized person is “reduced in our minds from a whole and usual person to a tainted and discounted one” (Goffman, 1963, p. 3) while social rejection indicates, “the situation of the individual who is disqualified from full social acceptance” (Goffman, 1963, preface). For the sexually active adolescent girls they may be shunned by peers, the elderly in the community, among others. Stigmatizing adolescent premarital sex and premarital childbearing can therefore affect their sexual and reproductive health outcomes.
Adolescent girls try to avoid stigma to pass as “normal” in their interaction with members of their community. Passing as normal involves not departing from the norms and values of the society that encourages being chaste before marriage. Goffman (1963) referred to those who do not depart negatively from the societal expectations as normal. In Goffman’s dramaturgy, he explained that people have front and back stages where they perform in the presentation of the self. The front stage is where actors (individuals in the society) present the idealized part of their lives and therefore tend to hide things that may not meet the expectations of their audiences (society) in the backstage. According to Goffman (1963), people try to present an idealized picture of themselves in their interaction. This impression is managed mainly through concealment of prior activities and errors. In addition, actors may also conceal the process they go through and only show the outcome (Goffman, 1963). For the adolescent girls who are not pregnant and those who are pregnant and mothers, they turn to adopt strategies to manage the impression they create out there to their parents, peers, and community members to pass as normal. This means that adolescents may have knowledge about contraceptives, but they may want to conceal their usage of it. Adolescent may conceal their sexual activities by using methods that are not visible or do things in secret (backstage).
Study Site and Methodology
Fanteakwa District is one of the 21 districts within the Eastern Region of Ghana with Begoro as its District capital. The ethnic composition of the population in Begoro is varied with a total of six ethnic groups. Among the six ethnic groups, the Akans and the Ga-Adangbes are the dominant groups. The other ethnic groups include the Ewes, Dagati, and Frafra. The two dominant ethnic groups in Begoro, the Akans, and the Ga-Adangbes are some of the few ethnic groups that traditionally performed puberty rites for adolescent girls. These customary rites were performed for girls, usually after their first menstruation to usher them into womanhood. These rites required that girls were not pregnant before the performance of the rites, and girls who became pregnant before going through these rites were severely punished including banishment. However, in recent times with most societies increasingly becoming urbanized as well as the introduction of Christian and Islam religions, these customary rites are becoming defunct.
Data for this article was part of a study conducted on adolescent girls’ resilience to teenage pregnancy and motherhood in Ghana for the award of a PhD. The data were collected in 2012 in Fanteakwa District in the Eastern region of Ghana. Using the sequential mixed method approach, the quantitative data were collected and analyzed first, then 3 months later in-depth interviews were conducted with 20 of the respondents who were purposively selected from the survey respondents. For the survey, a multistage cluster sampling technique was used to select the respondents. An enumeration area list was obtained from the Ghana Health Service (GHS) in the district to identify the different clusters in the Begoro community. In the first stage, the enumeration area list from the GHS in Fanteakwa District listing all the outreach sites in Begoro was used. In all, the GHS in the district provided a list of 58 enumeration areas in Begoro out of which four (Belco, Odumase, Akwansrem, and Obuasi) were randomly selected for the study. In every household, adolescents between the ages of 15 and 19 years with the consent of their parents or guardian were sought, after which the individual adolescents gave their assent before engaging them in a face-to-face interview, using the questionnaire. The questionnaires constituted questions that sought to describe and analyze the respondents’ sociodemographic background, pregnancy status, social environments, personal knowledge, and skills, as well as the personal experiences of the adolescents. The main variables analyzed and relevant for this article, where age, educational background, ethnicity, religious affiliation, pregnancy status, and sexual experiences. In addition, the questionnaire had 10 questions for ever-pregnant (EP) and eight questions for NP girls specifically to distinguish between high- and low-resilient girls. For analytical purposes, “NP girls” refer to adolescents who were not pregnant or have had any live births, whereas “EP girls” referred to girls who were pregnant or have child(ren). Based on the resilience scores of the respondents, 20 adolescent girls were purposively selected for further probing. These girls were purposively selected to give detailed insight and explanation of the various strategies they adopted to avoid or minimize stigma to teenage pregnancy and motherhood. The sensitivity of the study as well as the age of most of the respondents, required strict adherence to ethical concerns and as such, the respondents were contacted and interviewed in their homes. The in-depth interviews were conducted by the researcher and therefore had the opportunity to identify wrong transcriptions and amend it accordingly. As the in-depth interviews were conducted in the local language Twi, the audio-recorded responses from the in-depth interviews were transcribed. The transcribed data were translated into English and typed in Microsoft Word. This was followed by a thematic analysis of the transcribed data. To ensure anonymity of the study’s respondents, pseudonyms are used to identify the participants in the findings section of the article.
Findings and Discussions
Sociodemographic Characteristics of Respondents
The sociodemographic background of respondents focused on includes age, level of education, religious affiliation, and ethnic background.
The survey respondents had a mean age of 17 years. The adolescents who fall within the legal age for marriage (between ages 18 and 19 years) were 35.2% (Table 1). While the Constitution of Ghana and the Child Act outlines the designated age for marriage in Ghana to be at age 18 years and consensual sex at age 16, the traditional and religious value systems do not lay emphasis on age for marriage, they discourage premarital sex and out of wedlock childbearing. Ghana’s educational system starts from nursery/kindergarten after which pupils spend 6 years in school for primary education, 3 years for Junior high school (JHS) education and 3 years for senior high school (SHS) education. More than half of the respondents (54%) had or were in JHS, while 23.6% and 14.8% were in SHS and primary school, respectively.
Sociodemographic Characteristics of Adolescents Girls.

Note. JHS = Junior high school; SHS = senior high school.
In this study, the Akans who are the largest ethnic group in Ghana constituted more than 50% of the respondents whereas the Ga-Adangbes constituted 26% (Table 1). There were other ethnic groups apart from the Akans and the Ga-Adangbes, who represented approximately 13% of the respondents. This shows that the study area is a multiethnic society constituting mainly the Akans, the Ga-Adangbes, and other ethnic groups. A large number, 458 out of the 500 adolescent girls in the study, were affiliates of various churches in their community including orthodox, pentecostal, and charismatic. In all, 91.6% of the respondents identified themselves as Christians, while 7.2% indicated that they were Muslims (Table 1). This was not surprising as the 2010 Population and Housing census showed that 71.2% of Ghanaians are Christians and 17.6% are Moslems. The rest of the respondents indicated that they were African Traditional believers or not affiliated to any religion. Associating oneself with any of these religious groups suggest that majority of the adolescent girls were supposed to be guided by Christian or Muslim values.
Pregnancy Status of Respondents
Part of the process of identifying participants for this research was to first identify adolescent girls who were between the ages of 15 and 19 years old. Those who were not pregnant or have not had any live birth or children were presented as the “nonpregnant”. The NP girls in this study may include girls who might have had abortions or miscarriages and sometimes shied away from disclosing this because it was a taboo to mention their misdemeanor given their social context. Those who were pregnant (or) and have had a live birth at the time of the study were categorized as the “ever-pregnant” (Table 2).
Age Distribution by Pregnancy Status.
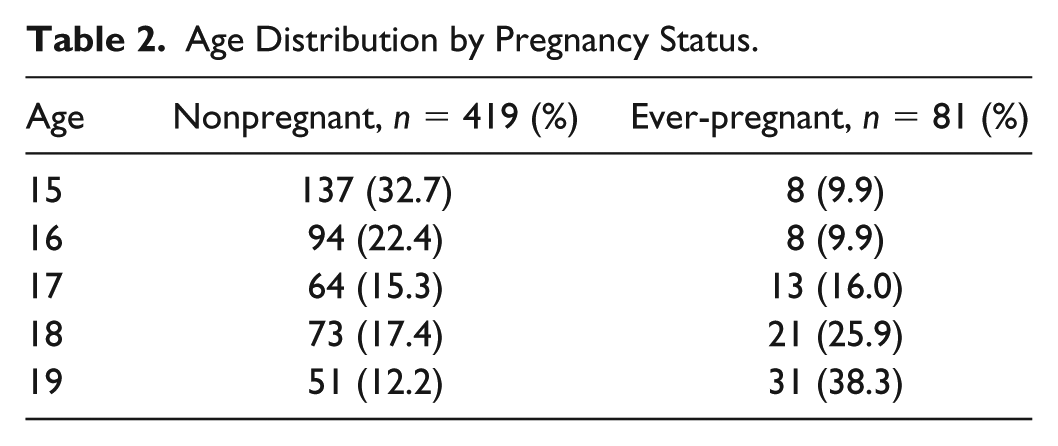
The data revealed that out of the 500 respondents, 81 (16%) were pregnant or already mothers. The proportion of girls who were pregnant or mothers increased as age increased, approximately 10% were 15 years old and 38% were 19 years old (Table 2). However, the proportion of NP girls decreased as age increased, thus approximately 33% of NP girls were 15 years old and 12% were 19 years old.
The proportion of pregnant adolescents and teenage mothers reflects the national data, which also reported that 16% of adolescent girls in rural Ghana have started childbearing (Ghana Statistical Service [GSS], 2008). As the data indicate, girls aged 19 years were more likely to be pregnant or mothers than girls aged 15 years. As the age of girls increased, they get closer to the age for marriage and therefore this explains why the proportion of girls who are pregnant, or mothers increases with age. According to the GSS, 2008, while only 1% of women aged 15 years in Ghana have started childbearing, 29% of women were either mothers or pregnant with their first child by age 19 years.
Premarital Sexual Experience
To find out about the sexual experience of the study participants, they were asked if they have ever had sexual intercourse before. The response indicated that 176 (42%) of the NP girls had experienced sexual intercourse. More so, 17% of the NP girls who were 15 years had experienced sexual intercourse (Table 3). The overall mean age of NP girls who have ever had sexual intercourse was 17 years (Table 3). This suggests that although the NP girls were not pregnant or did not have any live births, 42% had experienced premarital sex.
Age of Respondents who have Experienced Premarital Sex.

These findings suggest that almost half (42%) of the NP girls had sexual experience and have had sexual intercourse. It also shows that having sexual intercourse is not dependent on the age of the individual, all girls aged 15 to 19 years had relatively equal proportions of those having had sex with ages 18 and 19 years having slightly higher proportions.
The trend of girls experiencing premarital sex and premarital childbearing is not different from what pertains around the world and within the Ghanaian community (Agyei, Biritwum, Ashitey, & Hill, 2000; GSS, 2008). It confirms reports that girls are initiating sex as early as age 15 years. The results shows that adolescents’ sexual experience does not follow the legal age of marriage (18 years), the traditional value system and the religious value system that propose chastity before marriage (Ahlberg, 1994; Awusabo-Asare et al., 2004). Therefore, an adolescent’s sexual experience has an influence on her pregnancy status or her exposure to becoming pregnant. Knowing the sexual experience of adolescent girls in this study highlights two important facts about adolescent sexual and reproductive health.
First, it helped to identify girls who are predisposed to premarital sex and teenage pregnancy and second, it showed how girls avoid or overcome the risk associated with their sexual experience. As most of the adolescent girls involved in the study had some level of formal education as well as knowledge about their sexual and reproductive health, the expectation was that adolescent mothers may be stigmatized by teachers and peers when they return to school as found by Imoro (2009). Although Imoro’s (2009) study found that peers and teachers sometimes stigmatized girls who tried to go back to school after child birth, this study found out that some adolescent mothers went back to school after child birth to avoid or minimize the effect of stigmatization. If teachers and peers will be trained to accept adolescent girls despite their new status as mothers, it will help to curb or reduce some of the negative impacts of premarital childbearing. As Christianity and Islam are often against premarital sex and out of wedlock pregnancy, adherence to these religious rules can be both a blessing and a bane for adolescent girls in their sexual and reproductive health experience. Religious values become a blessing when it encourages girls to abstain from sexual activities before marriage (Addai, 2000). This notwithstanding, such one sided values may prevent girls from openly seeking and accessing reproductive health services for fear of being stigmatized by members of their religious group and this can predispose such girls to unsafe sexual practices. This is largely because the religious values of girls, which in most cases proscribes chastity before marriage, may influence girls not to practice safe sex such as using contraceptives to prevent sexually transmitted infections including HIV/AIDS and teenage pregnancy.
Adolescent Girls’ Strategies for Avoiding the Stigma of Premarital Sex
Girls either refrained from being in a relationship with the opposite sex or abstained from sex to maintain a good reputation. Yaayaa’s view in the narrative below is shared by most of the girls: Many men propose love to me, but I turned them down . . . when people see that you have a boyfriend, they conclude that you are having sex and they label you as a bad girl, because of that, I reject proposals from boys so that people would say I am a good girl. (Yaayaa, NP, In-depth interview, Begoro)
Adolescent girls were discreet in their sexual relationship. Sexual relationships were kept as a secret from parents and the community as whole. The data revealed that almost all the respondents who were in a sexual relationship ensured it was not publicly known. Korkor puts up a good behavior by running errands when asked to in order to be classified as a good girl while at the same time she tries to keep her relationship a secret. She explained, To maintain a good reputation, I go on errands for them (community members) and I keep my relationship secret. (Korkor, NP, In-depth interview, Begoro)
However, there was one exception, Frema, who was muslim, revealed she was in a relationship, but it was a secret between her and her mother. Some had confidants in whom they confide in. In her case, she explained that she had to keep her relationship away from her father because she did not want her father to disown her. As such in the eyes of her father, she passes as “normal.” Frema stated, My father has threatened to disown me if I become pregnant because I am not matured enough to have a baby. My mother is the only one who knows I have a boyfriend and it is a secret between us. (Frema, NP, In-depth interview, Begoro)
The issue of secrecy is also applied in accessing and using contraceptives by sexually active adolescents to avoid stigma and continue to be accepted as “normal” in the community. To avoid stigmatization for engaging in premarital sex, adolescent girls secretly use contraceptives in their sexual activities in order not to get pregnant. Thus, in their bid to conceal from the community that they were involved in premarital sex, they use contraceptives to avoid the consequences of having sex. The use of contraceptives is shrouded in so much secrecy such that one of the respondents revealed that she travels to a neighboring town to buy emergency pills whenever she had sexual intercourse. Obaa Yaa stated, People do not really know me well so when you even say something bad about me people will not believe it . . . . I usually buy the pills from Obuasi [Obaa Yaa uses the emergency pill after having sex]. (Obaa Yaa, NP, In-depth interview, Begoro)
In her case Obaa Yaa a sexually active girl passes as “normal” by adopting the strategy of purchasing contraceptives from sources that cannot be traced back to her. Thus, for the NP girls, to pass as “normal,” they refrain from entering any form of relationship with the opposite sex, abstained from sex whereas the sexually active adolescent girls avoided stigma by doing things in secret.
The fear of stigmatization encouraged some adolescent girls to adopt strategies to avoid teenage pregnancy in the first instance. In their quest to be identified as “normal,” they try to meet the expectations of their community which upholds the value of chastity before marriage. To be identified as normal, adolescent girls adopt different strategies such as abstaining from sex, being discreet with their sexual relationships as well as using protection in their sexual relationship when they have sex. Adolescent were discreet in their sexual behaviors because they lived in a homogeneous society where they had little or no privacy (Challa et al., 2018). From the evidence so far, the strategies adopted by adolescent girls to avoid stigma served two major functions on adolescent girls’ premarital sex and premarital childbirth experience. There is the manifest function, which are the observable results where girls in their bid to be accepted by their community members and social networks try to avoid pregnancy by abstaining from sex, staying away from sexual relationships with the opposite sex or using protection when they have sex. In this way, the manifest function here is that it helped girls to avoid pregnancy. For the latent function, the desire to pass as “normal” by avoiding pregnancy which is the obvious expression of a girl not being chaste helped girls to avoid sexually transmitted infections, not disrupting their education as well as avoiding the risk of early motherhood.
Although these strategies according to the adolescent girls helped them to avoid pregnancy which is stigmatized for adolescents, the strategies are not sustainable. The discreet nature of their strategies in some cases could have dire consequences in certain situations. It meant that girls will not have regular access to contraceptives when they have need of it for fear of being labeled as bad girls (Challa et al., 2018). Ampofo (2001) also drew this conclusion. This could explain why although adolescent girls have knowledge about the use of contraceptives, the use of it is still low. However, this study found that despite the fear of being labeled as bad girls for buying contraceptives, adolescent girls averted this by buying from places that they were not known to maintain their anonymity. A girl’s inability to access modern contraceptives for fear of being stigmatized defeats the importance of using contraceptives because girls may end up not having regular access to modern contraceptives when they need it. Judging from these findings, it calls for further understanding into the sociocultural context of the society to help develop health messages that are accurate to leverage the positive aspects of the belief system to support positive behavior change for good health outcomes.
Adolescent Mother’s Strategies for Escaping the Stigma of Premarital Childbearing
For the adolescent mothers, being praised by community members was a sign of acceptance, despite having fallen out of the norms and values that accept childbearing in marriage. One way that adolescent mothers adopt to pass as “normal” in their community is by going back to school and studying hard. Those who had more education, such as JHS and SHS students, tend to strive to go back to school after having a baby. For instance, Boatemaa, who had a baby after her Basic Education Certificate Examinations (BECE), went back to school and has since moved on to SHS. Boatemaa and Sheila observed, By God’s grace after having my baby, I am back in school and next year my baby will start schooling, so people praise me because most teenage mothers do not continue with schooling after giving birth. (Boatemaa, EP, In-depth interview, Begoro) I make sure I take my academic work seriously to secure my future because if I drop out of school people will say that after I had the baby I was not able to continue with my schooling. People use me as an example to advice their children, they tell them of how I have been able to continue with my school after giving birth. (Sheila, EP, In-depth interview, Begoro)
Being able to continue with one’s education after having a baby earned them praises from community members, to the extent that some of them became role models for other girls who became pregnant. As role models, they were used as examples to encourage other teenage mothers to go back to school after having a baby. Some EP girls who dropped out of school because of pregnancy and childbirth went on to trade or learn a vocation to earn money to take care of their financial needs. In her view, Gloria noted, You must make the effort yourself to sell something to take care of your child. (Gloria, EP, In-depth interview, Begoro)
In addition, because EP girls do not want people to stigmatize them because of premarital childbearing as adolescents, such as being unable to take care of themselves and their babies, they strive to take good care of themselves and their baby. Owusua demonstrated this in her narrative: If you don’t take good care of your child and leave him to be moving from house to house in search of food, people will say you are irresponsible but if you are able to take good care of your child they praise you. (Owusua, EP, In-depth interview, Begoro)
Sometimes, NP girls turn to marry when they become pregnant, because of the perception that, having a husband will take away the stigma that comes with premarital childbearing. Tina expressed, They praise me because I have a husband (partner); it is not all the teenage mothers who have a husband (partner). (Tina, EP, In-depth interview, Begoro)
A few of the adolescent mothers had the perception that having a husband on becoming pregnant was a way of earning a good reputation in the society. As such, some associated being accepted as “normal” to the fact that the fathers of their babies marry them. Some adolescent girls after becoming pregnant ended up marrying or cohabiting with their boyfriends/partners which most of them interpret as marriage.
For the EP girls, the desire to feel accepted in the eyes of community members pushed them to do things that would earn them praises despite being pregnant or teenage mothers. As Agunbiade (2014) observed, adolescent motherhood is stigmatized and therefore to minimize stigmatization, they resort to different measures including abortion and marriage. This study found that, some adolescent mothers in their effort to pass as “normal” adopted strategies that in the long run helped them to cope well with teenage pregnancy and motherhood. They took good care of themselves, their babies, went back to school, and took their academic work seriously or even find work to do to make money. This study has shown that EP girls in their effort to prove a point to their community members put up good behavior including working hard and returning to school just to earn good reputations. This is confirmed in adolescent mothers who return to the classroom (Angwin & Kamp, 2007; Hosie & Selman, 2006). They do this not necessarily to “rebel” but to be accepted by society. Carey, Ratliff, and Lyle (1998) described girls who wanted to prove a point to society that they could make it in life despite experiencing teenage pregnancy as being “rebellious.” When girls receive the relevant support from significant sources it can help them to return to the classroom even after having their babies. Thus, in this case to pass as “normal” despite one’s premarital childbearing status, some adolescent mothers adopted these various strategies.
Conclusion
Torn between the various value systems and the tensions between them in their social environment, adolescent girls have adopted different strategies to avoid stigma. The strategies adopted by the adolescent girls to avoid stigma whether to premarital sex or premarital childbearing is an indication that adolescents have unmet needs when it comes to their sexual and reproductive health. These unmet needs include lack of social support to have access to and use sexual and reproductive health services as well as some privacy in their sexual and reproductive life. Adolescents want some privacy in their sexual and reproductive life and therefore interventions aimed at ensuring that adolescents engage in safe sexual relationship must come up with programs and interventions that do not undermine adolescents’ privacy. For the NP girls, to pass as “normal,” they refrained from entering into any form of relationship with the opposite sex or abstained from sex whereas the sexually active adolescent girls avoided stigma by being discreet about their sexual relationship and using protection. The adolescent mothers also tried to avoid stigma by taking good care of themselves and their babies as well as in some cases going back to school, learning a trade, or finding a job. Although, these strategies have helped some girls to avoid or minimize stigma, some of the strategies adopted by the girls may not always be reliable and therefore need to be addressed. For the NP girls their focus was to avoid pregnancy, however, parents, teachers, and health workers should provide girls with information on how to avoid HIV/AIDS and sexually transmitted infections. To assure adolescents about anonymity in their use of sexual and reproductive health services and facilities, they should be handled separately from the older folks. Furthermore, more programs and interventions should target HIV/AIDS interventions and not only focus on preventing pregnancy.
More awareness needs to be created for community members, institutions, and family members to see that as society keeps changing because of migration, formal education, and urbanization, adolescents may postpone marriage but at the same time will continue to engage in premarital sex which can lead to teenage pregnancy and early childbearing. Thus, the need to support them to minimize the risk they may be predisposed to in their sexual and reproductive health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Centre of Competence in Research (NCCR) North-South for funding the study. Commonwealth Scholarship Commission for funding my one-year study abroad at the University of Sussex, UK during my PhD.