
Abstract
Perceived rejection is moderated by a person’s coping orientations and sensitivity to discriminatory behaviors embedded in stigma and unfair treatment within the social space. The current study, therefore, examined the extent to which internalized stigma, anticipated discrimination, and structural violence influence the rejection sensitivity of persons with mental illness. A non-experimental cross-sectional study examined how anticipated discrimination, internalized stigma, and injustice experiences influence rejection sensitivity among 330 outpatients in Sub-Sahara Africa. Hierarchical multiple linear regression results demonstrate the non-significant relationship between anticipated discrimination and rejection sensitivity (β = .015, p = .775, 95% CI [−0.789, 1.057]). However, the relationship between internalized stigma and rejection sensitivity (β = .148, p = .029 [0.119, 2.146]) and structural violence (β = .165, p = .015 [0.014, 0.134]) were significant. While social interactions may threaten the existence of highly rejection-sensitive persons, supportive social interactions act as agents of inclusion and social empowerment for persons with a mental illness. Our study findings have further implications for health care and social welfare policy.
Plain Language Summary
Perceived rejection is influenced by a person’s coping abilities and sensitivity to societal discriminatory behaviors. The current study, therefore, examined the extent to which self-stigma, anticipated discrimination, and social injustice influence the rejection perceptions of persons with mental illness. We collected data from 330 persons over 18 years receiving Mental healthcare in Sub-Saharan Africa. Hierarchical multiple linear regression analysis results demonstrated no significant relationship between anticipating discrimination and rejection perceptions. However, the relationship between self-stigma, rejection perceptions, and social injustice was significant. While social interactions may threaten and affect persons who are highly sensitive about rejection, supportive social relationships act as agents of inclusion and social empowerment for persons with a mental illness. Our study findings have further implications for healthcare and social welfare policy decisions.
Background
Previous rejection experiences tend to increase one’s expectation of rejection from the public, increasing the possibility of rejection by society in general (De Rubeis et al., 2017; Downey et al., 1997). A person’s coping orientations moderate perceived rejection (Feinstein, 2020; Gyamfi et al., 2024; G. B. Link et al., 1989; B. G. Link et al., 2002) and sensitivity to discriminatory behaviors (Downey & Feldman, 1996; Gyamfi et al., 2024; Innamorati et al., 2014; Isaksson et al., 2018) embedded in stigma and unfair treatment within the social space. Rejection sensitivity (RS) is a cognitive-affective processing disposition of anxious expectation in which people readily perceive and react to rejection cues (Downey & Feldman, 1996). According to Downey et al. (1997), who first used the term “rejection sensitivity,” prior experience with rejection situations makes people easily anticipate rejection in most social interactions, leading to social withdrawal (Downey et al., 1997; Rosenbach & Renneberg, 2014; Schaan et al., 2020; Shin et al., 2024), and aggression (Ayduk et al., 2008; Gao et al., 2021; Jacobs & Harper, 2013).
Perceptions of stigma may ignite certain coping methods characterized by guilt, concealment, isolation, and segregation (Crabb et al., 2012), causing the individual to find ways of dealing with the inherent threat to the self. Stigma is an undesirable and discrediting attribute that makes people lose their social status and acceptance and motivates the stigmatized individual to cope by hiding the “mark” as much as possible (Goffman, 1963). The consequence of failed coping and heightened sensitivity to discriminatory acts may result in withdrawal from public interactions as another form of coping to protect one’s self-esteem and reduce associated stress. In all, withdrawal helps stigmatized persons limit social interaction with those who may know about their illness.
Secrecy and withdrawal may be a behavioral response to internalization (self-stigma) and negative public behaviors, including rejection perceptions. B. G. Link et al. (2015) expanded their modified labeling theory. They posited that negative labeling experiences induce what they termed “symbolic interaction stigma,” where stigmatized persons scrutinize other people’s reactions for potential signs of prejudice so they can plan toward curtailing possible rejection. Even though secrecy and withdrawal may be used as coping mechanisms for perceived/anticipated public rejection, heightened secrecy, and withdrawal are harmful and associated with increased cognitive and emotional distress, feelings of guilt, shame, helplessness, sadness, hopelessness (Oexle et al., 2017), and low self-esteem (Singh et al., 2016). In all, rejection sensitivity affects self-esteem (Leary, 2015), social withdrawal (Abrams et al., 2011; Schaan et al., 2020) and increases the person’s stigma stress perception appraisal (Quinn et al., 2015).
Recent research findings also point to personality traits and some demographic characteristics, such as gender, age, education, and income level, among others, as factors that can influence the impacts of rejection sensitivity. Even though there is not enough research evidence that links the influences of demographic variables, such as gender and age, on the rejection sensitivity of persons with mental illness, a few studies have cited gender as a factor that affects the stigma perception and rejection sensitivity of stigmatized individuals (De Rubeis et al., 2017; Downey & Feldman, 1996; Lesnick & Mendle, 2021; Schaan et al., 2020). So far, results continue to be mixed regarding the association between some demographic variables and rejection sensitivity. While some studies claim a relationship, others think otherwise. For instance, Garthe (2020) recently found that race/ethnicity, level of education, and income level significantly influenced rejection sensitivity (especially those with high education (degree) and low income) while age, gender, area of residence (rural or urban) did not significantly influence a person’s rejection sensitivity. In a recent systematic review and meta-analysis, Foxhall et al. (2019) found that childhood trauma, that is, emotional abuse and neglect, was linked with rejection sensitivity and adult illness of borderline personality disorder. Similarly, Nacak et al. (2021) studied 65 persons with somatoform pain disorder. They found that individuals with a history of childhood adversities and repeated traumatic life events expressed high levels of rejection sensitivity alongside severe depressive symptoms. Despite this evidence, it remains unclear how demographic variables affect one’s rejection sensitivity in appraising social interactions.
Recent evidence shows a strong link between social rejection, rejection sensitivity, justice sensitivity, and the internalization of negative outcomes of mental illness regarding pervasive unfair treatment that persons with mental illness (PWMI) experience in the public space (Bilgin et al., 2021; Bondü et al., 2017; Bondü et al., 2020). The enduring negative and unfair treatment of PWMI leads to social suffering and harm due to losing one’s social status and opportunities. The enduring harms that individuals experience due to illness constitute structural violence (Galtung, 1969).
Structural violence appears to trigger rejection sensitivity through stigma and rejection experiences remotely. Justice sensitivity, the tendency to perceive and negatively respond to alleged injustice or unfair treatment (Schmitt et al., 2005), is an outcome of ongoing structural violence perspectives in the social domain. Perceptions of rejection experiences in social relationships may have roots in historical and sociocultural models that shape the development and maintenance of social norms. An individual’s expectations of rejection or acceptance may be influenced by the social context in which they interact, vis-à-vis the social experiences, and changing social relationships regarding support/networks over the life trajectory. Burgeoning injustices against individuals with mental illness not only diminish their chances of equity, equal opportunity, and self-actualization, but they also deepen the power gap while enabling unfair social control in favor of the so-called “normal” (other members of society).
The negative implications brought about by ongoing structural violence perspectives cause harm or even death among marginalized persons due to sustained lack of opportunity and neglect by those at the helm of social policy and implementation, thereby leading to a greater internalization of stigmatizing attitudes over time, including social rejection. Rejection sensitivity has been shown to develop because of traumatic life experiences (Foxhall et al., 2019; Nacak et al., 2021), especially if the rejection was by close social relations such as one’s parents (Rosenbach & Renneberg, 2014) and peers (Pachankis et al., 2014; Rosenbach & Renneberg, 2014). According to Horney (1937), the anxiety associated with maltreatment develops over time through early rejection experiences. Due to previous life experience, people with mental health problems become hypersensitive to social exclusion (Foxhall et al., 2019; Gratz et al., 2013; Renneberg et al., 2012). Such prior experiences predispose the individual to any future rejection and associated pains regardless of how slight the rejection would be, leading to rejection sensitivity, which subsequently contributes to the development of mental disorders and related negative perceptions and sequels of social stigma such as victim justice sensitivity (where the individual perceives injustice toward the self by other people; Bondü & Elsner, 2015; Bondü et al., 2017; Schmitt et al., 2005). Victim justice sensitivity occurs through subtle and sometimes hidden structural violence perspectives embedded in stigmatizing viewpoints of labeling, stereotyping, prejudices, discrimination, status loss, and other social rejection/discrimination outlooks of ostracism and exclusion that thrive in the presence of power differences.
Injustice-sensitive people may easily perceive the devaluation, rejection, and exclusion accompanying structural violence perspectives, but may feel powerless in challenging these unfair treatments. These enduring inequities may eventually contribute to greater social disadvantages, leading to further loss of social status and attendant negative outcomes, including rejection sensitivity. The literature shows that anticipated discrimination prevents people from applying for employment, training, or education, or from forming close relationships (Ucok et al., 2012).
The rejection sensitivity model (Downey et al., 1997) proposes that prior exposure to rejection and associated pain heightens biological and neurological responses, making individuals more sensitive to current and future rejection in social/interpersonal interactions. The rejection sensitivity framework also asserts that individuals high in rejection sensitivity are likelier to have pre-existing expectations for rejection that readily trigger how they make sense of ongoing social interaction cues (Downey & Feldman, 1996; Downey et al., 1998). Based on this assertion, we would argue that experiences of rejection/discrimination are more likely to lead individuals to anticipate discrimination in social relationships.
That notwithstanding, underlying stigma and structural violence theories have established that there is a close association between mental illness and social rejection perspectives. It is also worth noting that most of the studies on rejection sensitivity were conducted with Western populations. To the best of our knowledge, this is the first study that examined rejection sensitivity among populations with mental illness in an African setting. Therefore, we examined the extent to which internalized stigma, anticipated discrimination, and structural violence influence the rejection sensitivity of persons with mental illness.
Hypotheses
Methods and Materials
Study Design
This study was a cross-sectional design that examined the extent to which internalized stigma, anticipated discrimination, and injustice experiences influence the rejection sensitivity of persons with mental illness.
Research Setting
The study was conducted in two public Psychiatric Hospitals in Southern Ghana. Ghana is a Low-Middle Income Country located in West Africa, along the Gulf of Guinea and the Atlantic Ocean, with a total land area of about 239,000 square km. There are three Psychiatric Hospitals, all situated in the Southern part of the country (along the coast). Two of these hospitals are in Accra, the capital city, and the other is in the Central Region of Ghana (about 100 miles away from the capital). The total bed capacity of the three hospitals is about 1,500 (average of 5.5 beds per 100,000 population). Despite the few beds available, each hospital can admit up to 1,200 patients. In Ghana, psychiatrists and psychiatric nurses offer mental health care, including clinical mental health officers, psychologists, community psychiatric nurses, community psychiatric officers, social workers, occupational therapists, and health assistants.
Sampling
Target Population
For this study, the target population was outpatients in two psychiatric hospitals in Southern Ghana (namely, the Ankaful Hospital and Pantang Hospital). Outpatients are mostly individuals who live in the community, have recovered from severe symptoms of mental illness, and are seeking ongoing reviews and further treatment (rehabilitation) at the Outpatient Department (OPD).
Inclusion Criteria
To be part of the study, individuals were expected to be out-patients aged 18 years and above who could articulate their perceptions and experiences in English. Participants with a stable mental health status who offered informed consent were recruited for the study.
Exclusion Criteria
Outpatients experiencing an exacerbation of their underlying mental illness (relapse) were not involved in the study.
Sampling Method
Non-probabilistic convenience sampling technique was used to recruit participants for the study at the OPD of the two psychiatric hospitals. The research team collaborated with the health care providers at the OPD in the study settings to recruit participants. Individuals were included in the study after they had clearly understood the content of the information sheet and consented to it. In all, 330 participants were recruited for the study. To achieve the set sample size, the two hospitals were weighted equally because each has a bed capacity of about 500. Therefore, an average of 165 PWMI were recruited from each hospital, resulting in a sample of n = 330 participants.
Data Collection
The researchers obtained permission from the Western University Research Ethics Board (115773), the Ankaful Hospital (197487), and the Pantang Hospital (102018), respectively. Once granted, the study commenced in accordance with each hospital’s protocol. After explaining the study’s purpose, the researcher and RAs first met and obtained verbal consent from individuals who expressed interest. Interviews were conducted in a secure location of the participant’s choice within the hospital, promoting optimal participation and privacy. Just before data collection began, the risks and benefits of the study were clearly explained to the participant, who had the opportunity to ask questions. The researcher also informed the participants that they had the freedom to withdraw from the study at any time or decline to answer any questions they wished. The researchers further assured participants of anonymity by using a combination of letters and numbers (codes) to represent them. Just before the interview commenced, the participant read the contents of the information section and signed a formal written consent form, granting the researchers the right to collect and publish the data provided. Once the participant signed the consent form, data collection began. Primary data were collected from the recruited outpatients using a questionnaire administered by the researcher and a trained research assistant at both locations. Although self-reports from PWMI in the form of interviews can lead to psychological distress or socially desirable responses, using interviews empowered participants to express themselves regarding stigma issues. Therefore, there was no direct harm to the participants of the study. Primary data were collected from the recruited outpatients once, using questionnaires administered by the first author and trained research assistants (RAs). The researchers first collected socio-demographic data and followed with the questionnaires in other sections. Overall, the data collection process for each participant took about 90 min. Each study participant was appropriately compensated for their time.
Measures
Injustice Experiences Questionnaire
In 2008, Sullivan and colleagues published a 12-item Injustice Experience Questionnaire (IEQ; alpha = .92) to appraise feelings of unfair treatment in the workplace among individuals with musculoskeletal injuries. The IEQ is a 5-point Likert scale instrument that ranges from 0 = never, 1 = rarely, 2 = sometimes, 3 = often, and 4 = all the time. The IEQ has two subscales: the severity/irreparability of loss scale and the blame/unfairness scale (Sullivan, 2008).
To calculate the scale’s total score, we added all 12 items (the total score of the 12 IEQs = 48). Total scores for IEQ subscales were computed by summing up responses under the scale. A high score meant high levels of perceived injustice. Descriptors for different ranges of scores are presented as follows: 34 to 48 = very high range of perceived injustice; 30 to 34 = high range of perceived injustice; 23 to 29 = moderate to high range of perceived injustice; 14 to 22 = average range of perceived injustice; 8 to 13 = low to average range of perceived injustice; 5 to 8 = low range of perceived injustice; and 0 to 4 – very low range of perceived injustice. In our study, the internal consistency of the IEQ items was strong (α = .84).
The Questionnaire on Anticipated Discrimination (QUAD)
Anticipated discrimination was assessed using the Questionnaire on Anticipated Discrimination (QUAD). QUAD is a 14-item, 4-point Likert scale that ranges from 0 (strongly disagree) to 3 (strongly agree). The QUAD assesses the extent to which people with mental health problems anticipate discrimination across various contexts (Gabbidon et al., 2013). The two subscales of the tool have moderate correlation (r = .54), with good internal consistency (alpha = .82; anticipated discrimination from institutions/services), and (alpha = .76; anticipated discrimination in interpersonal/professional relationships), respectively.
A mean score was calculated for the QUAD in addition to a count score of the number of areas of life in which individuals expected anticipated discrimination. To calculate (a) Mean scores, a mean score (range 0 to 3) is calculated by adding each item score (0, 1, 2, or 3) and dividing by the number of answered items in the scale. No items were reverse-coded. (b) Count score – A count score was calculated by counting the number of items for which the participant scored 2 (agree) or 3 (strongly agree) within the 14-item scale. Items that were scored as 0 (strongly disagree), 1 (disagree), or (missing) were not included in this count. High scores indicated strong anticipation of discrimination. The interpretation of scores is as follows: 0.00 to 1.50 = minimal to no anticipated discrimination, 1.51 to 2.00 = mild anticipated discrimination, 2.10 to 2.50 = moderate anticipated discrimination, and 2.51 to 3.00 = severe anticipated discrimination. In this study, the internal consistency of the QUAD items was good (α = .76).
Rejection Sensitivity
The Adult Rejection Sensitivity Questionnaire (A-RSQ) measures a person’s sense of rejection to actual or perceived rejection (Berenson et al., 2009, 2013) in social, cognitive, and affective terms as defined by Downey and Feldman (1996). The A-RSQ was developed by Berenson and colleagues in 2009 after studying adults (N = 685) in an internet survey. The ARSQ is an 18-item bifactor instrument rated on a 6-point Likert scale ranging from 1 (very unconcerned) to 6 (very concerned) for the rejection concern/anxiety portion and from 1 (very unlikely) to 6 (very likely) for the rejection expectancy portion. The scale is scored by calculating a score of rejection sensitivity for each situation by multiplying the level of rejection concern in question “a” by the reverse of the level of rejection expectancy, the response to question “b.” The formula is rejection sensitivity = (rejection) * (7-rejection expectancy). To obtain the overall (total) rejection sensitivity score, you take the mean of the resulting 9, that is, mean = arsq1, arsq2, arsq3, arsq4, arsq5, arsq6, arsq7, arsq8, arsq9. The total score is expected to be between 1 and 36. In the current study, the internal consistency of the items was good (α = .78).
The Internalized Stigma of Mental Illness Scale (ISMI)
The Internalized Stigma of Mental Illness Scale (ISMI) comprised four subscales in a 24-item, self-completed 4-point Likert scale that ranges from 1 (strongly disagree) to 4 (strongly agree). The tool assesses patients’ experiences of internalized stigma (Ritsher et al., 2003). The four subscales include Alienation (6 items), Stereotype endorsement (7 items), Perceived discrimination (5 items), and Social withdrawal (6 items). In this study, the ISMI was used to appraise stigma perceptions. Each score was calculated by adding the item scores and dividing by the total number of answered items. High scores indicated severe internalized stigma. For instance, 1.00 to 2.00 = minimal to no internalized stigma, 2.01 to 2.50 = mild internalized stigma, 2.51 to 3.00 = moderate internalized stigma, 3.01 to 4.00 = severe internalized stigma. In the current study, the internal consistency of the ISMI was also good (α = .89).
Data Analysis
Data Preparation and Screening
To ensure data quality, the researcher checked for completeness by randomly sampling from the data set to check for response sets against the scales for patterns of responses. The researcher also checked for missing values or pages and the consistency and accuracy of responses by conducting logical checks with the demographic data and range checks with the Likert response categories as provided in the questionnaire. Open-ended questions in the demographic data were categorized, each given an appropriate code before being entered into SPSS for analysis. All missing values were given a code of −99 to account for them during analysis. One of the RAs entered data, after which the principal investigator validated the data separately. This helped to reduce any errors. In this study, descriptive and inferential analyses were done using the Statistical Package for the Social Sciences (IBM SPSS v.28.0, 2021).
Results
Participant Characteristics
This study examined how internalized stigma, anticipated discrimination, and injustice experiences influence the rejection sensitivity of persons with mental illness. Means, standard deviations, skewness, and kurtosis values were calculated to determine the general characteristics of the variables and to assist the researcher in assessing the assumptions of the multiple linear regression for possible redress should there be any form of unfavorable skewness or kurtosis, as skewness could affect regression coefficients associated with the model (Malehi et al., 2015). Descriptive statistics of variables are presented in Tables 1 and 2.
Sociodemographic Characteristics of Study Participants.

Descriptive Statistics on Total Scores of Key Measures.

In this study, all participants (n = 330, 100%) reported their demographic characteristics, with most being Christian (270, 81.8%) and with a mean age of 37.11 years (SD = 10.9). About 185 (56.1%) of the participants were male. Regarding marital status, most participants were unmarried (n = 244, 74%). In terms of living situation, the majority (n = 276, 83.6%) lived with someone (i.e., friends, family, or partner). Approximately 154 (46.7%) were employed in government, self-employment, or private industry, while 132 (40%) were unemployed. All participants had some form of formal education, with about 266 (80.6%) holding secondary or tertiary educational qualifications. Among the 196 (59.4%) who expressed knowledge of their illness, approximately 91 (46.4%) had schizophrenia, followed by substance use disorder (57, 29.1%), mood disorders, that is, depression, and bipolar (43, 22%). The rest of the diagnoses included post-traumatic stress disorder (3, 1.5%), Epilepsy (1, 0.5%), and dementia (1, 0.5%). Most participants, 138 (70.4%), who expressed knowledge of their illness, agreed with their current diagnosis. The average treatment duration of participants’ illness was 6.94 years (SD = 3.0). Details of the participant demographic characteristics are reported in Table 1.
Assessing Assumptions of the Multiple Regression
The output from the descriptive statistical analysis of key measures was used to assess if data were normally distributed by assessing skewness (the degree to which a variable distribution was asymmetrical (i.e., Sk > 0 if positively skewed, and Sk < 0 if negatively skewed) and kurtosis (a measure of the peakedness of the distribution). Establishing normality helped the researcher to determine whether the sample recruited for the study was a true representation of the outpatients being studied. In the event of data skewness or kurtosis, the researcher fixed it by performing a square root transformation of the data (to help reduce skewness to acceptable levels). However, normality Q-Q plots of the variables (RSQ, IEQ, ISMI, and QUAD) indicated reasonable straight lines on their respective Q-Q plots. Again, the normality test using stem and leaf and histogram also indicated that the dependent variable (RSQ) and the other continuous independent variables (IEQ, ISMI, and QUAD) were normally distributed, as the skewness/standard error ratio for each variable was less than 2. For instance, for the IEQ, skewness of 0.256/SE (0.134) was = 1.91, while the ISMI, QUAD, and RSQ yielded 0.31 and 0.18, respectively. See Table 2 for details about the means and skewness of the variables.
The investigator also determined if there was any form of multicollinearity between the variables by performing a bivariate correlation analysis. Apart from the QUAD that appeared not to have a significant relationship with the RSQ (.003, p = .962), the IEQ significantly but moderately correlated with the RSQ (IEQ = .252, p = .000), indicating the absence of any form of collinearity among the measures. See Table 3. In addition to the correlation, a more robust test for collinearity was done by calculating the variance inflation factor (VIF) = 1/1−R2 of each independent variable. Each variable, however, had a VIF ≤ 10.00, indicating the absence of multicollinearity among the predictors.
Correlation Matrix of Variables.

Correlation is significant at the 0.05 level (2-tailed). **Correlation is significant at the 0.01 level (2-tailed).
Testing the Study Hypotheses
We conducted a multiple linear regression analysis to determine the extent to which anticipated discrimination (AD), internalized stigma (IS), and structural violence (SV) relate to rejection sensitivity (RS). The variables were subjected to hierarchical multivariate linear regression analysis to determine the most appropriate model to explain the effects of the independent variables on rejection sensitivity.
To ascertain whether gender and age confound relationships between the predictors and rejection sensitivity, gender and age were first entered into the initial model. The model was not significant (F-test [2, 327] = 1.354, p = .250, R2 = .008), indicating that per our study, demographic variables (age and gender) did not play any role in the rejection sensitivity perspectives of participants. In the second stage, the overall score on QUAD was entered into the model. The QUAD and age and gender did not significantly predict rejection sensitivity in any way (F-test [3, 326] = 0.900, p = .441, R2 = .008), indicating that anticipating discrimination within the social space did not necessarily predict rejection sensitivity. In the third stage of the model building, the overall score on ISMI was entered into the model. The ISMI, in addition to the age, gender, and QUAD variables, explained about 7% of the variance in rejection sensitivity (F-test [4, 325] = 5.949, p ≤ .001, R2 = .068). In the fourth step, IEQ was entered into the model. The R2 was = .085. Taken as a set (i.e., age, gender, QUAD, ISMI, and IEQ), the overall regression model was significant and explained about 9% of the total variance in rejection sensitivity (F-test [5, 324] = 6.026, p = .015, R2 = .085).
Out of the four models, the fourth (final) model was chosen due to the following: current research evidence, the significance of the model, the amount of variance explained by the model, and the effects of predictor variables on the dependent variable. In all, only predictors, internalized stigma (ISMI) and structural violence (IEQ), positively correlated and predicted rejection sensitivity (RSQ) to some extent (see Table 4).
Summary of Multivariate Linear Regression Analysis Depicting Effects of Independent Variables on Rejection Sensitivity.
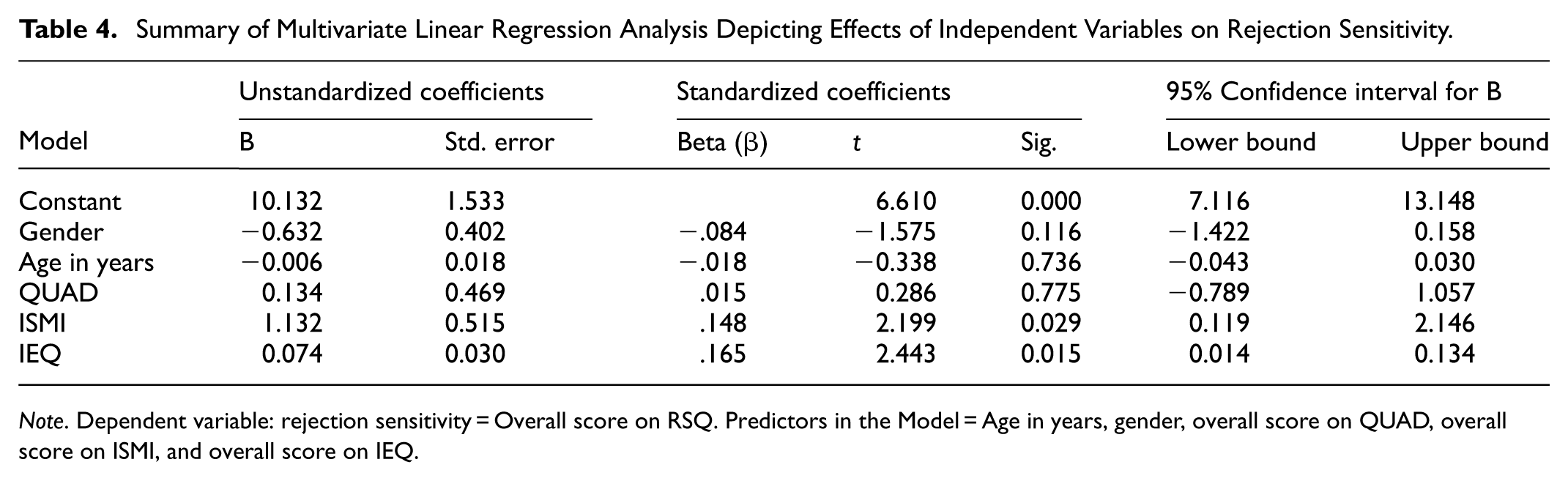
Note. Dependent variable: rejection sensitivity = Overall score on RSQ. Predictors in the Model = Age in years, gender, overall score on QUAD, overall score on ISMI, and overall score on IEQ.
Relationship Between Anticipated Discrimination and Rejection Sensitivity
Anticipated discrimination did not demonstrate any significant effect on rejection sensitivity and, therefore, could not explain any significant variance in the dependent variable even after controlling for age and gender (β = .015, p = .775, 95% CI [−0.789, 1.057]).
Effects of Internalized Public Stigma on Rejection Sensitivity Perspectives
Model results demonstrate a significant relationship between internalized stigma and rejection sensitivity and that internalized stigma predicts a person’s rejection sensitivity (β = .148, p = .029, 95% CI [0.119, 2.146]). The results show that for every unit increase in internalized stigma, there is a 0.148 increase in rejection sensitivity, having controlled for age, gender, and QUAD (anticipated discrimination).
Influences of Structural Violence Outlooks on Rejection Sensitivity
The association between structural violence and rejection sensitivity was significant (β = .165, p = .015, 95% CI [0.014, 0.134]). Standardized coefficients indicate that for every unit increase in perceived structural violence, there is a 0.165 (standard deviations) increase in rejection sensitivity.
Discussion
The study examined the relationships between structural violence, internalized stigma, anticipation of discrimination, and rejection sensitivity in a cohort of outpatients in Ghana. The study results show that structural violence and internalized stigma predict rejection sensitivity among individuals with mental illness. We also found that age and gender did not significantly affect rejection sensitivity among study participants. This outcome adds to the ongoing debate concerning the role of gender and age. It confirms recent findings by Garthe (2020) that rejection sensitivity has no significant relationship with the age and gender of a person.
Earlier on, Ng and Johnson (2013) studied 53 persons with bipolar I. They also found no significant correlations between rejection sensitivity and the demographic variables of participants. Several reasons could account for this finding. For instance, the sample population comprised mainly adults 18 years and above, largely homogenously young. In terms of gender, there were more males (56%) than females. The results may have differed if the sample included a combination of young people (below 18 years) and adults, with equal gender distribution among the participants. It may also be that males and females do not differ in their perceptions of rejection.
The stigma stress perception appraisal model (Gyamfi et al., 2024) posits that even though religious and cultural belief systems and structural violence perspectives are primarily invisible within the social space, they are powerful tools embedded in social governance structures that create and sustain stigma against vulnerable groups in the form of labels, stereotyping and prejudice that culminate in a cognitive separation of the “us” versus “them” situation. Once vulnerable individuals are segregated, they lose their social status, leading to discrimination. Such discriminatory attitudes and behavior from the public lead to maladaptive coping orientations, including rejection sensitivity (a disposition of anxious expectations in which vulnerable persons readily perceive and overreact to social rejection cues). Depending on the extent of rejection sensitivity, the individual may perceive and appraise stigma stress appropriately (as negative or positive) with subsequent impact on their life domains.
According to Downey et al. (1997) – who first used the term “rejection sensitivity,” prior experience with rejection situations makes people easily anticipate rejection in most social interactions, leading to social withdrawal (Rosenbach & Renneberg, 2014; Schaan et al., 2020) and other negative outcomes such as aggression (Jacobs & Harper, 2013). Fundamentally, the rejection sensitivity model (Downey et al., 1997) proposes that prior exposure to rejection and its associated pain and heightened biological responses make individuals sensitized to both current and future (anticipated) discrimination/rejection in social/interpersonal interactions. Therefore, individuals high in rejection sensitivity were more likely to have pre-existing expectations for rejection that readily trigger how they make sense of ongoing social interaction cues (Downey & Feldman, 1996; Downey et al., 1998). Based on this assertion, we hypothesized that rejection sensitivity was positively associated with anticipated discrimination among persons with mental illness. However, our hypothesis was not supported.
We know that increased experiences of stigma and discrimination lead to greater anticipation of discrimination (Gyamfi et al., 2025), devaluation, and internalized negative public behaviors in future social interactions (Quinn et al., 2015). Social interactions act as agents of support and acceptance. At the same time, social interactions may threaten the individual’s existence, depending on how they perceive and respond to their social relationships (Berenson et al., 2009; Downey et al., 1997). We also know that increased anticipated discrimination mediates internalized stigma. Even though no known study has mapped anticipated discrimination to rejection sensitivity so far, we were expecting that once social rejection mediates rejection sensitivity, anticipated discrimination was likely to have a similar association with rejection sensitivity. The fact that anticipated discrimination did not have any significant relationship with rejection sensitivity could be attributed to factors that make us believe that the communal system of living in Africa, and for that matter Ghana, might be a good resource for social support and empowerment for the participants of this study (Gyamfi et al., 2025). We argue further that the individual coping abilities of the participants reduced the anticipation of discrimination even when perceived rejection was present.
Rejection sensitivity is a social, emotional, and psychological/cognitive response to discrimination and stigmatizing behaviors characterized by chronic anxious expectations of rejection that individuals portray during social interactions. In our current study, internalized stigma was found to predict rejection sensitivity positively. This confirms findings from two studies in Africa and America that is (Gyamfi et al., 2018; Rüsch et al., 2009) that have identified persons with mental illness reporting rejection sensitivity about feeling stigmatized by their society. Higher levels of perceived stigma stress appraisal (Gyamfi et al., 2025; Rüsch et al., 2009) and experienced discrimination (Li et al., 2017) may have potentiated the negative relationships between the study participants and community members. Our study also reveals that rejection sensitivity is not only an outcome but also a predictor of further stigma and rejection/exclusion, as well as a coping method for some people to guard against potential threats in their social environments.
According to the Rejection Sensitivity Theory (Downey et al., 1997), individuals who have experienced rejection in the past develop an increased sensitivity to potential rejection. This heightened awareness often results in anticipatory anxiety and defensive responses in social situations. In the context of mental illness, internalized stigma (where individuals adopt and apply negative societal stereotypes to themselves) can further reinforce sensitivity to rejection. Internalized stigma contributes to the cognitive expectation of rejection among PWMIs. Individuals who internalize stigma may perceive themselves negatively, believing that others will also view them as inadequate or unworthy. This perception heightens their sensitivity to potential exclusion, making them more likely to interpret ambiguous social cues (e.g., a delayed response or a neutral facial expression) as signs of rejection (Downey et al., 1997). Consequently, even in neutral or supportive environments, those with deeply internalized stigma may assume they are being judged or excluded. Beyond cognitive expectations, rejection sensitivity is also associated with emotional distress, including heightened feelings of anxiety, shame, and sadness in response to perceived rejection. Because internalized stigma already involves self-devaluation and shame, it may intensify these emotional reactions. To cope, individuals may engage in defensive or avoidant behaviors, such as withdrawing from social interactions to protect themselves from anticipated rejection. However, this withdrawal can reinforce social isolation and further deepen stigma and rejection. Internalized stigma can also contribute to a self-fulfilling cycle of rejection. For instance, individuals who expect rejection may display guarded, anxious, or withdrawn behaviors, leading to strained social interactions. In response, some members of society may engage less warmly or reduce social engagement, which the individual then interprets as confirmation of their initial fear of rejection. This cycle perpetuates both their rejection sensitivity and social isolation, exacerbating more psychological distress associated with mental illness. This finding calls for an expansive public education and enhanced social support to empower marginalized people.
The study proved that structural violence positively influences rejection sensitivity among persons with a mental illness. This unique finding is novel and significant in filling mental illness stigma literature gaps. Structural violence (the systemic social inequalities embedded within institutions, policies, and cultural norms that disadvantage certain groups) plays a significant role in the development of rejection sensitivity. It manifests through discriminatory policies, restricted access to resources, and systemic inequities in critical areas such as healthcare, employment, and education. These systemic barriers contribute to institutionalized exclusion and social marginalization, shaping individuals’ psychological and emotional responses to perceived rejection. One of the primary ways structural violence fosters rejection sensitivity is through the internalization of systemic disadvantage. Individuals who repeatedly experience exclusion and unfair treatment due to systemic factors (e.g., poverty, ableism) may come to perceive themselves as inferior or unworthy, further reinforcing anticipatory anxiety about future rejection. Marginalized groups, including PWMIs, often face systemic discrimination, which strengthens their expectation of being devalued or excluded in both personal and professional settings. According to the Dynamic Stigma Theory, the emotional, religiocultural, moral, and psychological consequences of structural violence are profound, with far-reaching negative impacts on the self-esteem of stigmatized persons (Gyamfi, 2024). For instance, chronic systemic oppression has been linked to heightened emotional distress, increased levels of anxiety and depression, anticipated discrimination, and social withdrawal (Gyamfi, 2024; Gyamfi et al., 2025). Furthermore, exposure to structural violence fosters distrust toward social institutions and interpersonal relationships, prompting individuals to develop guarded, defensive, or withdrawn behaviors as a coping mechanism. In addition to fostering social stigma (Gyamfi, 2024; Gyamfi et al., 2025), structural violence also reinforces the expectation of rejection (Downey et al., 1997). This expectation can lead individuals to behave in ways that can elicit rejection from others, creating a self-perpetuating cycle of exclusion with further adverse outcomes.
The positive relationship between structural violence and rejection sensitivity among the study participants has implications for long-term stigma research as this widens the scope, opens new debates, and adds further evidence to the stigma discipline concerning the treatment of mental illnesses at the meso (institutional level) and the macro (national or global policy formulation) levels. Our study findings assert that structural violence is rooted in historical antecedents that influence rejection sensitivity through incidents of social stigma that create internalized stigma and justice sensitivity phenomena. According to Schmitt et al. (2005), justice sensitivity is the tendency to perceive and respond negatively to alleged injustices or unfair social treatment. As reiterated earlier, the indirect outcomes of structural violence cause people to experience low self-esteem. Once these individuals experience low self-esteem, they become more sensitive to direct social exclusionary attitudes (of social stigma and discrimination), contributing to heightened anticipation of rejection and subsequent rejection sensitivity.
Having gleaned the rejection sensitivity literature so far, one can assert that not only do people anxiously expect rejection due to perceived injustice (justice sensitivity; Bondü & Elsner, 2015; Giovannelli et al., 2018), but they also experience the stress of rejection that is underpinned by stigma outcomes of labels, stereotypes, prejudices, discrimination, isolation, social status loss, alienation/rejection, ostracism, and social exclusionary behaviors or attitudes that contribute to rejection sensitivity in the long run. Per the tenets of the social-cognitive learning theory (Bandura, 1986; Bandura et al., 1961), existing negative social contexts make individuals learn to expect rejection in social relationships. The learned anticipated consequences can make the individual develop biases and cues that enforce the person’s rejection sensitivity (the anxious expectations of rejection in future interactions with others), leading to a cycle of negative events that reinforce each other in the individual’s life domains.
Implications
The current findings have implications for both formal (health professionals) and informal (family) caregivers. As Ng and Johnson (2013) suggested, highly rejection-sensitive persons are more likely to view ambiguous interpersonal cues as rejection signals regardless of their symptom remission. They are, therefore, more likely to respond intensely when rejection occurs. Health professionals are, therefore, more likely to gain the trust and cooperation of their clients by understanding the social-interpersonal-cognitive dimensions of rejection and applying certain tenets of therapeutic relationships where the clients would be involved in decisions concerning their care. Involving clients in their care planning (at the hospital and at home) gives them a voice. It also empowers and demonstrates recognition and acceptance for continued engagement with significant others.
Feeling insecure in social relationships, as faced by persons with mental illness, tends to negatively influence the attachment behaviors of individuals, leading to or worsening both physical and mental health status and the social support they receive from their significant others due to weak relationships that insecure attachment brings. Reducing perceptions of rejection through support is likely to encourage people to remain and engage with their close relations, including caregivers, while sticking to their treatment protocols without coercion. Because cognitive-affective responses have strong links with perceived rejection, health professionals and significant others should use less stereotyping or discriminatory language to motivate the clients to express their views during interactions. Caregivers should be mindful of their facial expressions when interacting with individuals with increased rejection sensitivity to avoid creating wrong and unintended impressions that might reinforce feelings of rejection or emotional distress.
The fact that rejection sensitivity negatively impacts the living situation and well-being of persons with mental illness makes it prudent for researchers to initiate studies that use a combination of public education and social contact as an intervention. This way, individuals’ self-esteem, autonomy, and self-efficacy perspectives would increase to aid their social integration efforts.
Strengths and Limitations
To the best of our knowledge, this was the first study that examined correlates of rejection sensitivity among an African population, and thus, makes the study unique and novel. While the findings may be valuable, results should be interpreted within the confines of cross-sectional designs, where one cannot make causal relationships. Therefore, future longitudinal studies would be necessary to provide more causal relationships and help confirm the findings. Again, using self-reporting measures in our data collection process may have introduced response bias among participants, potentially influencing the study’s outcomes. Although data were gathered through a face-to-face, researcher-administered approach, relying on participants’ subjective reporting presents a limitation, as responses may have been influenced by social desirability or recall bias.
Rejection sensitivity also affects young children and adolescents under 18 (Bondü et al., 2017; Zimmer-Gembeck, 2015). However, the current study examined only adults 18 years and above, making it impossible to make general statements that include young persons with mental illness in the context of the study demography. The fact that we examined only outpatients coming for routine review in the mental health hospital also prevents us from making generalized statements that include all persons with mental health problems vis-à-vis the correlations of rejection sensitivity. Therefore, Future studies should broaden the recruitment scope to involve both inpatients and outpatients, including those receiving services in primary healthcare settings.
Conclusion
To the best of our knowledge, this study is the first to examine the interrelationships among structural violence, internalized stigma, anticipated discrimination, and rejection sensitivity in the context of mental illness. Our findings highlight the significant impact of structural violence, rooted in longstanding historical injustices, on individuals with heightened rejection sensitivity, particularly those who maintain close social ties with partners, family members, or friends. The persistence of entrenched social inequities fosters environments where stigma and discrimination are not only prevalent but also systematically reinforced. These conditions can heighten the psychosocial burdens experienced by individuals with mental illness, diminishing their sense of support and undermining trust, satisfaction, and commitment in interpersonal relationships. As a result, these individuals may face increased social alienation and estrangement. Moreover, perceived inequality and exclusion can increase sensitivity to social threats or signs of disapproval, resulting in maladaptive behavioral responses. This hypersensitivity may further complicate their social interactions and contribute to a cycle of stigma, marginalization, and declining mental health. These findings underscore the need for targeted interventions that address structural determinants of mental health to create inclusive, supportive social environments that mitigate the harmful effects of stigma and discrimination.
Footnotes
Acknowledgements
The authors would like to thank all participants.
Ethical Considerations
The study was approved by the Western University Research Ethics Board (#115773) on June 29, 2020, Ankaful Hospital (#197487) on October 13, 2020, and Pantang Hospital (#102018) on August 15, 2020.
Consent to Participate
Before participating in the study, the researchers obtained written informed consent from each participant. All methods relating to the study were carried out following the REB guidelines and regulations.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Datasets generated and/or analyzed during the current study are not publicly available due to participant privacy, but are available from the corresponding author upon reasonable request.*