
Abstract
The objective of this study is to estimate the impact of Integrated Child Development Services (ICDS) on the institutional delivery and on the nutritional status of children in rural India. Propensity score matching is used to remove selection bias, and then compare the outcome of those who received the ICDS services with those who did not receive. A representative sample of 32,072 women age 15 to 49 years was obtained from the National Family Health Survey-3 (2005-2006). The units of analysis were women who had at least one birth during the 5 years period preceding the survey and the children who were born during this period. In this study, the treatment variable was taken as “during pregnancy, received any nutrition and health education from the ICDS.” The main outcome measures were institutional delivery and the prevalence of undernutrition. After matching, it was found that the among the rural women who received nutrition and health education specifically from the ICDS had 12.3% higher institutional delivery as compared with those who did not receive. However, no positive impact was observed on children’s nutritional status. Thus, for improving the scenario of child nutrition, it is suggested that emphasis be shifted from supplementary feeding to improving environmental hygiene and child feeding practices.
Keywords
Introduction
Even in this age of scientific advancements in technology and medicine, delivering quality health care to pregnant and lactating mothers and their children continues to be a far-fetched dream in India. Annually, around 50,000 mothers lose their lives due to pregnancy-related complications, while more than 1.5 million children die each year before reaching their first birthday. Institutional delivery entails giving birth in a medical institution, under the supervision and care of skilled medical professionals. Institutional delivery helps in the reduction of infant and maternal mortality and is also linked with the overall health status of the mother and the child (Sugathan, Mishra, & Retherford, 2001). In spite of the numerous efforts and programs launched by the Government of India (GoI) to promote institutional delivery, still one fourth of the rural women did not deliver in an institution (International Institute for Population Sciences [IIPS] & Macro International, 2015-2016). Apart from the low levels of institutional delivery, the levels of child undernutrition in India are a matter of grave concern. The rates of malnutrition among under-5 children in India are among the highest in the world and almost 5 times as compared with Sub-Saharan Africa. Around half of India’s children are underweight, and 45% are stunted and 20% are wasted (World Bank, 2013). Undernutrition puts the children at a greater risk of death due to common infection as it results in an increase in the severity of such infections and also delayed recovery. Lack of proper nutrition during the first 1,000 days of a child’s life can result in stunted growth of the child, which is irreversible and associated with impaired cognitive ability and reduced school and work performance. Nearly half of all under-5 child mortality in India is attributable to undernutrition (UNICEF, 2017). According to National Family Health Survey 4 (NFHS-4), the prevalence of stunting, wasting, and underweight among under-3 children in India is 38%, 21%, and 36%, respectively (IIPS & Macro International, 2015-2016).
Launched on October 2, 1975, the Integrated Child Development Services (ICDS) scheme is one of the significant program of the GoI for reducing maternal and childhood malnutrition. Even though the program has undergone numerous changes in its scope content and implementation, but its primary focus of breaking the intergenerational cycle of malnutrition, reduction in the morbidity and mortality caused by nutritional deficiency through reaching out the children, pregnant, and lactating mothers remains unaltered. The program aims at holistic development of children below 6 years, expectant and nursing mothers and adolescent girls through providing the six services-supplementary nutrition, immunization, health check-ups, referral services, nonformal preschool education, and health education as a package through the network of Anganwadi centers (AWC). The Anganwadi workers (AWW) are responsible for providing the supplementary nutrition, nonformal preschool education, and nutrition and health education. However, immunization, health check-up, and referrals are provided by the primary health care infrastructure (GoI, 2011).
Ever since the ICDS was initiated in 1975, there have been many studies, which have tried to assess its success in improving maternal and child health in India. Even though the appraisal of the three decades of functioning of ICDS found the program to be satisfactorily operated (National Institute of Public Cooperation and Child Development [NIPCCD], 2006), existing literature shows that there are conflicting thoughts on the extent of its success. For example, in a study conducted by the World Bank, it was shown that “there is little evidence of ICDS program impact on overall child nutrition status” (Das Gupta, Lokshin, Gragnolati, & Ivaschenko, 2005) and at times a negative impact. This is because in spite of wide coverage, there is lack of optimal utilization (Gupta, Gupta, & Nongkynrih, 2013) and the quality of services needs to be improved to get the desired results Chudasama et al., 2015). A case study in Kashmir revealed that the medical check-up of children below 3 years of age was not up to the mark. Due to lack of proper coordination between the health and ICDS staff, none of the children below 3 years of age were immunized (Bashir, Bashir, Ganie, & Lone, 2014). However, in these studies, conclusions were drawn from primary data collection (Bashir et al., 2014; Chudasama et al., 2015), which were localized in deferent parts of the country and of smaller sample sizes, or from the previous rounds of the NFHS (IIPS & Macro International, 2000, 1995; Das Gupta et al., 2005). A study conducted by Mukhopadhyay (2015) based on NFHS-3 data shows that the presence of ICDS centers in communities helps in reducing child stunting. However, this study had taken into consideration ICDS as one covariate in the conventional regression model. In the present study, an attempt has been made to assess the impact of the ICDS scheme on both maternal and child health by using an improved technique, propensity score matching (PSM), and by using the NFHS-3 (IIPS & Macro International, 2007) data to answer the persisting questions. Our study is restricted to only the rural areas, as the conditions of maternal and child health are considerably poor in the rural as compared with urban areas. The NFHS-4 data clearly show the difference in the scenario of maternal and child health in the rural and urban India. More than half of the women in urban areas had institutional delivery (89%) as compared with only 75% in the rural areas. The infant mortality rate is higher in rural areas (46 per 1,000 live birth) as compared with urban areas (29 per 1,000 live birth). A similar disparity in child undernutrition exists between urban and rural India. Forty-one percent children are stunted, 22% wasted and 38% underweight in rural India, while in urban India, 31% are stunted, 20% wasted, and 29% underweight (IIPS & Macro International, 2015-2016).
Method
The data used for the present evaluation were taken from the latest round of NFHS-3 conducted in 2005-2006 (IIPS & Macro International, 2007). A two-stage sample design yielded a representative sample of 32,072 women in the age group of 15 to 49 years. The units of analysis were women who have given at least one birth during the 5 years period immediately preceding the survey interview and also the children who were born during that period.
However, as we use cross-sectional data here, the subjects have not been randomly assigned to the treatment and control groups, and thus, there exist some systematic differences between those who are treated and those who are not. To eliminate this bias, PSM was used. Each individual receiving the ICDS program was paired with an individual not getting the program, with similar observable background characteristics, and their outcomes were then compared. Now, this technique is an improvement over the conventional regression model on many grounds (Austin, 2011). First, the goodness of fit tests, such as regression analysis, do not give any estimate of the systematic bias removed between treated and untreated groups. Second, PSM, such as randomized control trials, allows one to keep the study design and study analysis separate. Only after the propensity scores are estimated, and an acceptable balance is achieved between the baseline covariates, the treatment effect is estimated. However, while using regression, one has the choice to continually modify the regression model until the level of association that one desire has been attained (Rosenbaum & Rubin, 1983). Furthermore, while comparing the treated and untreated individuals, if there are considerable differences in their baselines, PSM offers the analyst a choice to either abandon the study or go ahead with the analysis using the minority of overlapping individuals. However, while using regression, the analyst does not get to assess the degree of overlap between the distributions of baseline covariates for the two populations. If there happens to be strong differences between the groups, the model estimates by interpolating between the two distinct groups. PSM is also a better option than the conventional matching technique, as matching becomes very difficult and cumbersome, as the number of covariates keeps increasing.
While analyzing, two areas of assessment were defined: mother’s health and child’s health. Each area was investigated taking appropriate outcome variables: institutional delivery among pregnant women and undernutrition among children, and matching on certain preintervention background characteristics as discussed below.
Treatment and Matching Variables
In this study, treatment variable was taken as “during pregnancy, received any nutrition and health education from the ICDS.”
On the basis of literature, certain background variables were controlled for age of mother at first child birth (less than 18 years, equal and above 18 years), combination of religion and caste (Hindu SC, Hindu ST, Hindu Others, and Other Religions), wealth index (poorest, poor, middle, rich, richest), mother’s education in single years, father’s education in single years, preceding birth interval (first birth, less than 24 months, more than 24 months), mother’s current marital status (currently married, others), whether had a terminated pregnancy (yes, no), total number of children, frequency of reading magazine/newspaper (not at all, less than once a week, at least once a week, almost every day), frequency of hearing radio (not at all, less than once a week, at least once a week, almost every day), frequency of watching television (not at all, less than once a week, at least once a week, almost every day), whether the mother is allowed to go to the health facility (alone, with someone else, not at all). Apart from the above mentioned variables, sex of the child (male, female) has also been included while measuring child health outcome. However, regional variations could not be taken into consideration, as balancing could not be achieved during matching.
Outcome Variables
“Place of delivery” variable has been considered to address mother’s health outcome while prevalence of undernutrition in children has been used for addressing the child health outcome. Child undernutrition was assessed with the help of three commonly used anthropometrical indices: stunting, underweight, and wasting. For all three of these indices, the z scores were calculated from the median of the reference population. We define three z scores: height-for-age z score (HAZ), weight-by-age z score (WAZ), and weight for height (WHZ) where
Here, the observed height or weight of a child of a specified age and gender is denoted by
Statistical Reasoning
If we consider

The difference between the potential outcomes had the ith individual received or not received the treatment gives us the impact of the treatment

Now, if we average the impact across all the individuals in the population, we would get the estimate of the mean impact of the ICDS services, termed as the Average Treatment Effect (ATE):

where E(.) represents the average.
However, if we want to know the average impact of the treatment only on those who receive the treatment, we calculate the ATE on the Treated (ATT). It is defined as the difference between the average outcome of those who receive the treatment and the unobserved counterfactual:

Similarly, if we want to know the average impact of the treatment only on those who did not receive the treatment, we calculate the ATE on the Untreated (ATU). It is defined as the difference between the average outcome of those who did not receive the treatment and the unobserved counterfactual:

The nearest neighbor matching method with replacement method was used in conjecture with a probit model. To satisfy the balancing property on all the background characteristics, a “hit or miss” approach was used. Before the application of the PSM, it was ensured that the covariates chosen were observed before the ICDS services were provided (conditional independence assumption) and that persons with the same
Results
The balancing property was satisfied at 1% significance level, for both institutional delivery and undernutrition (Table 1). The region of common support between those who received the ICDS services and those who did not was high, indicating that an individual with a given set of background characteristics would have a positive probability of belonging to either group. Those individuals whose propensity scores lay outside the common support were dropped from the analysis.
Estimated Propensity Scores.
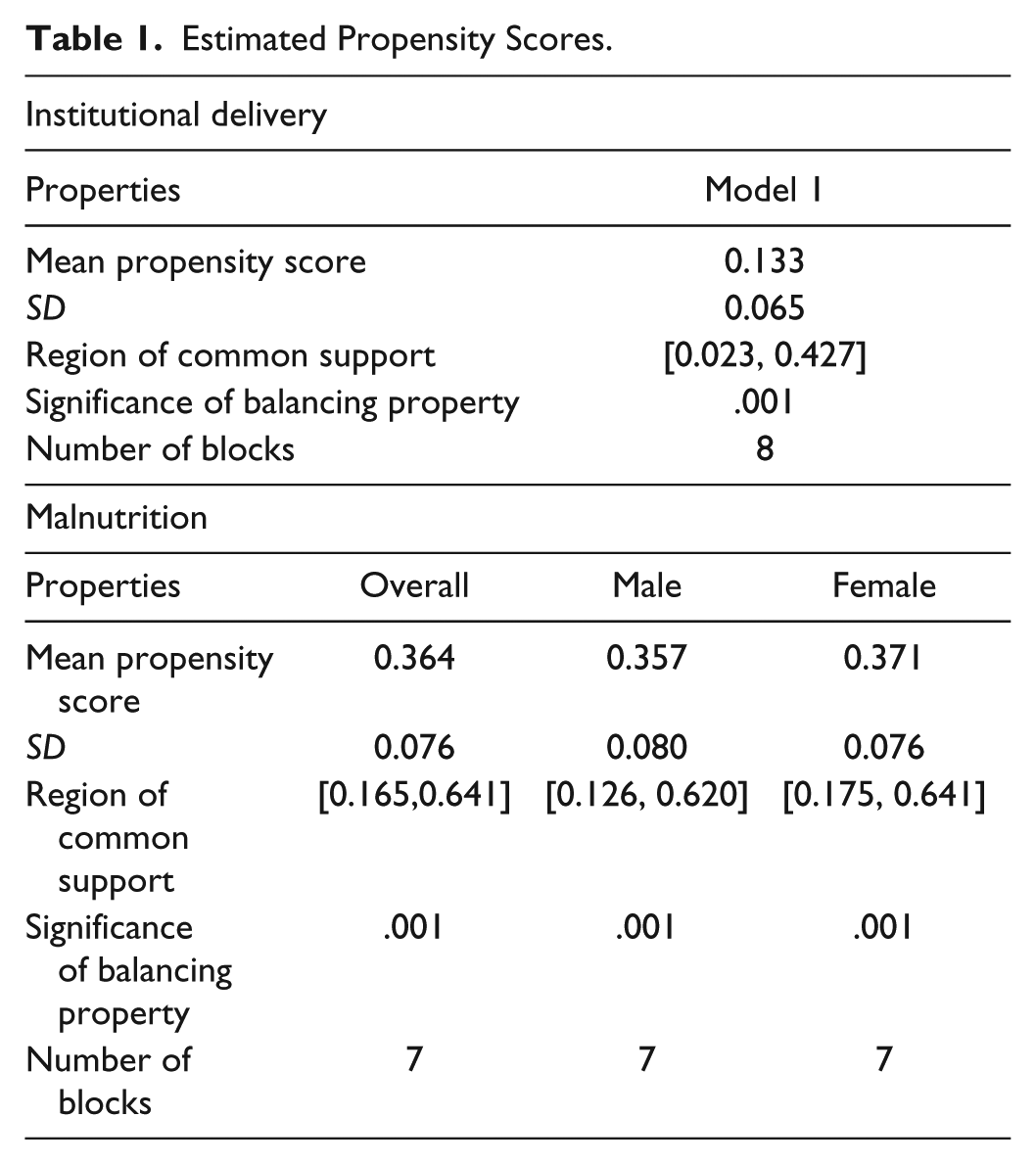
Table 2 shows the matching estimates of impact of ICDS services. For institutional delivery, before matching, there is a 7.7% higher chance for those women who received any nutrition and health education ICDS during pregnancy to go for institutional delivery as compared with those who did not. After matching, it increases to 12.3%. This indicates a positive impact of the ICDS services on institutional delivery; if we do not control for the background variables, then we clearly underestimate its impact.
Matching Estimates of Impact of ICDS Services.

Note. ICDS = Integrated Child Development Services; ATT = average treatment effect on the treated; ATU = average treatment effect on the untreated; ATE = average treatment effect.
In the case of undernutrition, the unmatched sample estimate shows that those children who received the benefits had 1.4% higher chance of being stunted, 6.7% higher chances of being underweight, and 4.5% higher chance of being wasted as compared with children who did not get the services. After matching, we see that those children who received the benefits had 0.1% higher chance of being stunted, 5.3% higher chances of being underweight, and 4.0% chance of being wasted as compared with children who did not get the services. The table also shows that without matching result overestimate the negative impact of ICDS services on child nutrient. This indicates that the ICDS services have a negative impact on overall children’s nutritional status. The results are similar when the analysis is done separately for male and female children.
For male children, the unmatched sample estimate shows that those children who received the benefits had 3.2% higher chance of being stunted, 7.7% higher chances of being underweight, and 4.7% higher chance of being wasted as compared with children who did not get the services. After matching, those who received the benefits had 1.6% higher chance of being stunted, 5.4% higher chances of being underweight, and 3.2% higher chance of being wasted as compared with children who did not get the services.
Similarly, among female children, the unmatched sample estimate shows that those children who received the benefits had 5.7% higher chance of being underweight and 4.3% higher chances of being wasted as compared with children who did not get the services. However, the unmatched sample shows that children who did not receive ICDS services were 0.3% higher chance of being stunted.
After matching, those who received the benefits had 6% higher chance of being underweight and 2.7% higher chances of being wasted as compared with children who did not get the services. In the case of stunting after matching result shows that children who do not receive ICDS services were 0.2% higher chance of being stunted compare with children who get the services.
In Table 3, the overall significance of the model is shown. The pseudo R2 gives us an estimation of how well the predictors explain the probability of the outcome, either maternal outcome (institutional delivery) or child health outcomes (stunting, underweight, and wasting). In all the cases, this value decreases after matching. Also, after matching, the p value of the likelihood ratio test of all the predictors becomes insignificant.
Overall Significance of the Models After Conducting Matching Analysis.

Discussion
The maternal and child heath situation in India is a matter of grave concern. The GoI has tried to address this issue by implementing different programs and schemes, ICDS being one of them. Previous studies have attempted to evaluate the impact of ICDS program in different settings. However, in the presence of selection bias, evaluation of a program in a cross-sectional data is a difficult task. Therefore, the present study has made an attempt to quantify the impact of ICDS services on institutional delivery and child nutrition in rural India with the help of PSM analysis.
The study shows that the ICDS services have a positive impact in promoting institutional delivery in rural India. In the model without matching, the impact of ICDS services on institutional delivery is clearly underestimated. A probable reason for the positive linkages between ICDS services and institutional delivery could be that as the expected mothers are receiving correct counseling provided through the ICDS, they become aware of the health risk associated with noninstitutional deliveries. In line with this finding, a study addressing the progress made in antenatal and perinatal care in an ICDS block of Jaipur district found that there had been a more than 50% increase in institution delivery over a period of 19 years (Kakkar, Gupta, Kakkar, & Malhotra, 2012).
In contrast to institutional delivery, the study did not find a positive impact of ICDS services on child nutritional status in rural India. The children who received the ICDS services were more likely to be stunted, wasted, and underweight as compared with the children not availing the services—either overall, or for male or female children separately. One possible explanation for this could be that the children attending the AWC are usually older than the age at which undernutrition sets in 0 to 3 years (IIPS & Macro International, 2007). Thus, once the condition sets in, the symptoms persist till a later age. Another explanation could be that the supplementary food obtained from the ICDS centers is often taken by many children as the only source of food, rather than an added source of nutrition, which is not enough to battle undernutrition. Furthermore, in many of the centers, this food is not given out regularly. As a matter of fact, in the 12 months preceding the NFHS-3, only 25% of the children of age 0 to 6 years who were receiving any sort of services under the ICDS, reported getting any supplementary food from the AWC (IIPS & Macro International, 2007). Although the ICDS program is well-designed to address the situation of nutrition in India, there exists certain gaps between the program design and its actual implementation which in turn has interfered with the program from reaching its potential. The program puts additional emphasis on supplementary feeding and preschool education of children 4 to 6 years old at the expense of the other components critical for combating undernutrition. The program has not effectively reached the under 3 age group among which the nutrition intervention can be most effective and the vulnerable group that is those belonging from the poor households and lower castes. The poorest states and those with the highest level of undernutrition still have the lowest levels of program funding and coverage. From the program implementation point of view, there is a lack of proper training and management of AWW, proper resource supply mechanism, and food supplementation services (Gragnolati, Shekar, Das Gupta, Bredenkamp, & Lee, 2005).
By controlling for various observed preintervention factors that could introduce bias on the estimates of the effects of the ICDS programs, this article provides an improvement on the previous studies. However, because we could not use panel data about the study participants, the results are not conclusive. Bias could have been introduced through some unobservable characteristics, which were correlated with the placement of the ICDS services or with institutional delivery and undernutrition. For example, program placement in a village might have been influenced by food shortage, in which case we would underestimate the effectiveness of the program.
Thus, we find mixed evidences about the ICDS program meeting its goals in India. Proper program placement and effective use of the allotted funds must be addressed, to fill the existing gaps in the supervision of the program. The program lays an additional emphasis on nutritional supplementation rather than other cost-effective strategies such as adult education and family-based health promotion. Thus, for improving the scenario of child nutrition, it is suggested that emphasis be shifted from supplementary feeding to improving environmental hygiene and child feeding practices. This is because, in many large-scale programs, a direct approach has been found to be largely ineffective (Das Gupta et al., 2005). Along with focusing on supplementary feeding, the program should also put emphasis on family-based feeding and caring behavior, improving child care behavior and educating parents about improving child health and nutrition. Supplementary feeding should be more focused toward the most vulnerable group that is the children below 3 years of age. Thus, it can be hoped that if these changes are incorporated, the considerable resources which are already available to the ICDS can be used more effectively for the betterment of mothers and children all over rural India.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.