
Abstract
Although physical activity is generally thought to be beneficial for individuals with Parkinson’s disease (PD), there is limited information regarding current rates of physical activity within this population. In this study, we measured self-reported physical activity levels of individuals with PD and explored factors that affected physical activity engagement. Sixty-one individuals living with PD completed a modified form of the Physical Activity Scale for Individuals With Physical Disabilities. Reported activity was high and exceeds published guidelines for individuals with limited mobility. Major facilitators of physical activity included (a) positive impact on PD-related symptoms, (b) social motivation, and (c) regularity or predictability of the activity. The major barrier to physical activity was PD symptom severity (e.g., lack of balance, gait impairment, tremor, and fatigue).
Parkinson’s disease (PD) is a chronic, progressive, neurodegenerative disease that affects approximately 55,000 community-dwelling Canadians, of whom 79% are above the age of 65 years (Wong, Gilmour, & Ramage-Morin, 2014). This number is expected to increase to approximately 163,700 by 2031 (Bray, Strachan, Tomlinson, Bienek, & Pelletier, 2014). Not surprisingly, this is expected to have a significant impact on the demand for efficient delivery of optimal health care services for this population.
Although dopaminergic medications are effective at mitigating most of the symptoms of PD, pharmacologic treatment does not stop the progression of the disease (Crizzle & Newhouse, 2006). As the disease progresses, medication is often less effective, and the responses are more variable (Guttman, Kish, & Furukawa, 2003). Furthermore, long-term use of dopaminergic medications may lead to debilitating side effects such as daytime sleepiness (Comella, Stebbins, Brown-Toms, & Goetz, 1994), dyskinesia (Fabbrini et al., 2009), and impulse control disorders (Weintraub & Potenza, 2006). The limitations of pharmacologic treatment point to a need for novel research on topics that help patients better cope with some of the physical, psychological, and social factors associated with PD. One such area of research is the evaluation and promotion of physical activity engagement among individuals with PD. There is a steadily increasing amount of evidence in support of the benefits of physical activity within this population, including improvements in physical functioning, quality of life, strength, balance, and gait speed (Goodwin, Richards, Taylor, Taylor, & Campbell, 2008).
Despite evidence that physical activity is a positive adjunctive therapy for the disease, limited information exists regarding the current rate of physical activity of individuals with PD. To the best of our knowledge, only three studies to date have examined physical activity levels among individuals with PD. Fertl, Doppelbauer, and Auff (1993) found that the physical activity levels of men and women with PD (Mage = 65.6, SD = 8.1) greatly decreased as the disease progressed. This study, however, focused primarily on sporting activities and was conducted using retrospective interviews, which may be subject to recall bias, response bias, and social desirability bias. The authors also failed to specify how these 32 participants were recruited, which makes it difficult to determine how well this sample represented individuals with PD in general.
More recently, Ellis et al. (2011) explored factors thought to be associated with exercise behavior in a large sample (n = 260) of individuals with PD (Mage = 67.67, SD = 9.2), who were classified as either exercisers (n = 164) or non-exercisers (n = 96). Results suggested that, in comparison with non-exercisers, exercisers had significantly better motor subscores on the Unified Parkinson’s Disease Rating Scale (UPDRS), were significantly less depressed, had significantly higher scores on the mobility domain of the Parkinson’s Disease Questionnaire–39 (PDQ-39), and took significantly more steps per day. Unfortunately, the authors did not report on barriers to engaging in physical activity.
Finally, Jones, Wieler, Carvajal, Lawrence, and Haennel (2012) examined the intensity levels of physical activity within a sample of participants with mild-to-moderate PD (Mage = 62.3, SD = 7.3). Results indicated that participants were sedentary for much of their day (19.4 hr/day), but when active, engaged in 2.7 hr/day, 1.1 hr/day, and 0.1 hr/day of light-, moderate-, and vigorous-intensity physical activities, respectively. These results should, however, be interpreted with caution, as this study was small in size (n = 11), and included only individuals who were not being treated with medication and who had a higher health-related quality of life than a community-based cohort.
Given the need to understand current levels of physical activity among individuals with PD, as well as to overcome some of the methodological limitations of previous research in this area, this study aimed to quantify the self-reported physical activity levels of individuals with PD, and identify self-reported facilitators and barriers to engagement within this population.
Method
Participants
Using a convenience sampling strategy, 120 individuals with PD were invited to participate in this study, and were mailed a questionnaire package to complete in their home. These individuals were drawn from a movement disorders clinic that services patients from across Southwestern Ontario, Canada, including both urban and rural areas. Inclusion/exclusion criteria included (a) confirmed diagnosis of PD, (b) not currently hospitalized, and (c) not in a residential care or long-term-care facility. Sixty-one individuals (30 women) between the ages of 52 and 87 years (M age = 69.35, SD = 7.72) agreed to participate. The procedures, questionnaire, and consenting practices described herein were approved by the Health Sciences Research Ethics Board at the University of Western Ontario. All participants provided informed consent.
Instrumentation
To evaluate the amount of physical activity in which participants engaged over a 7-day period, participants completed a modified form of the Physical Activity Scale for Individuals With Physical Disabilities (PASIPD) and returned it by mail. The PASIPD consists of 13 items that document the number of days per week and hours per day of participation in leisure activities, household activities, and occupational activities over the previous 7 days (Washburn, Zhu, McAuley, Frogley, & Figoni, 2002). The scoring process is based on intensity values known as the “metabolic equivalent of the task” (MET). One MET is the ratio of the energy expenditure of an activity over the energy cost of the resting metabolic rate, which is approximately equivalent to consuming one kilocalorie per kilogram of body weight per hour (Taylor et al., 1978). The PASIPD total score is obtained by multiplying the average hours per day spent in each activity, by the MET value associated with the intensity of the activity, and then summing these values to obtain the total score for that week. The maximum possible score on the PASIPD is 199.5 MET hr/day (Washburn et al., 2002). Jimenez-Pardo, Holmes, Jenkins, and Johnson (2015) evaluated the reliability and factorial validity of the PASIPD in a sample of individuals with PD and found the measure to be appropriate for the assessment of self-reported physical activity within this population.
In addition, three Likert-type items were included in the questionnaire package (after the PASIPD): (a) a question inquiring about the participant’s perception as to the effects of PD on his or her physical activity, (b) an item that queried an individual’s satisfaction with his or her current level of physical activity, and (c) a question that evaluated the representativeness (as compared with typical activity levels) of the last 7 days’ worth of activity. In addition to these items, a close-ended (yes/no) question was added to the questionnaire, which was intended to evaluate the survey’s ability to allow participants to describe current levels of physical activity, as well as an open-ended item that asked participants to report the total number of hours per week engaged in physical activity. Finally, five open-ended questions concerning physical activity types, durations (hours per week), capabilities and access, and facilitators and barriers were included to gain insight into the specific needs of individuals with PD. These additional items are presented in Table 1.
Additional Survey Items.

Data Analysis
Descriptive statistics were computed for the PASIPD total score, as well as each individual item score, to determine the amount of physical activity in which the participants usually engaged. Pearson product–moment correlation coefficients between selected items and the total PASIPD score were also examined. Descriptive statistics (means, standard deviations, and percentages where appropriate) were also computed for the additional close-ended items. Open-ended questions were subjected to a thematic analysis, and main themes were extracted and evaluated.
Results
Quantitative Analysis of PASIPD
Six participants (five women) left more than 50% of the questionnaire blank; as such, a PASIPD total score was not calculated for these individuals, and they were excluded from further quantitative analysis, thus resulting in a total sample size of 55 individuals. Eighty-six percent of respondents stated that the activities in which they had engaged over the previous 7 days were representative of their usual level of physical activities. Overall, 76% of respondents reported that their physical activity had decreased since receiving the diagnosis of PD (36% indicated that their levels of physical activity had greatly decreased, and 40% indicated that their levels of physical activity had somewhat decreased). Item descriptives and item-total correlations for the PASIPD are presented in Table 2, along with the MET value for each of the activities queried by the questionnaire.
MET Values, Hours per Day of Physical Activity (Ms and SDs), and/or Correlations With PASIPD Total Score, for 12 Items on the PASIPD and three Supplemental Likert-type Scale Items.
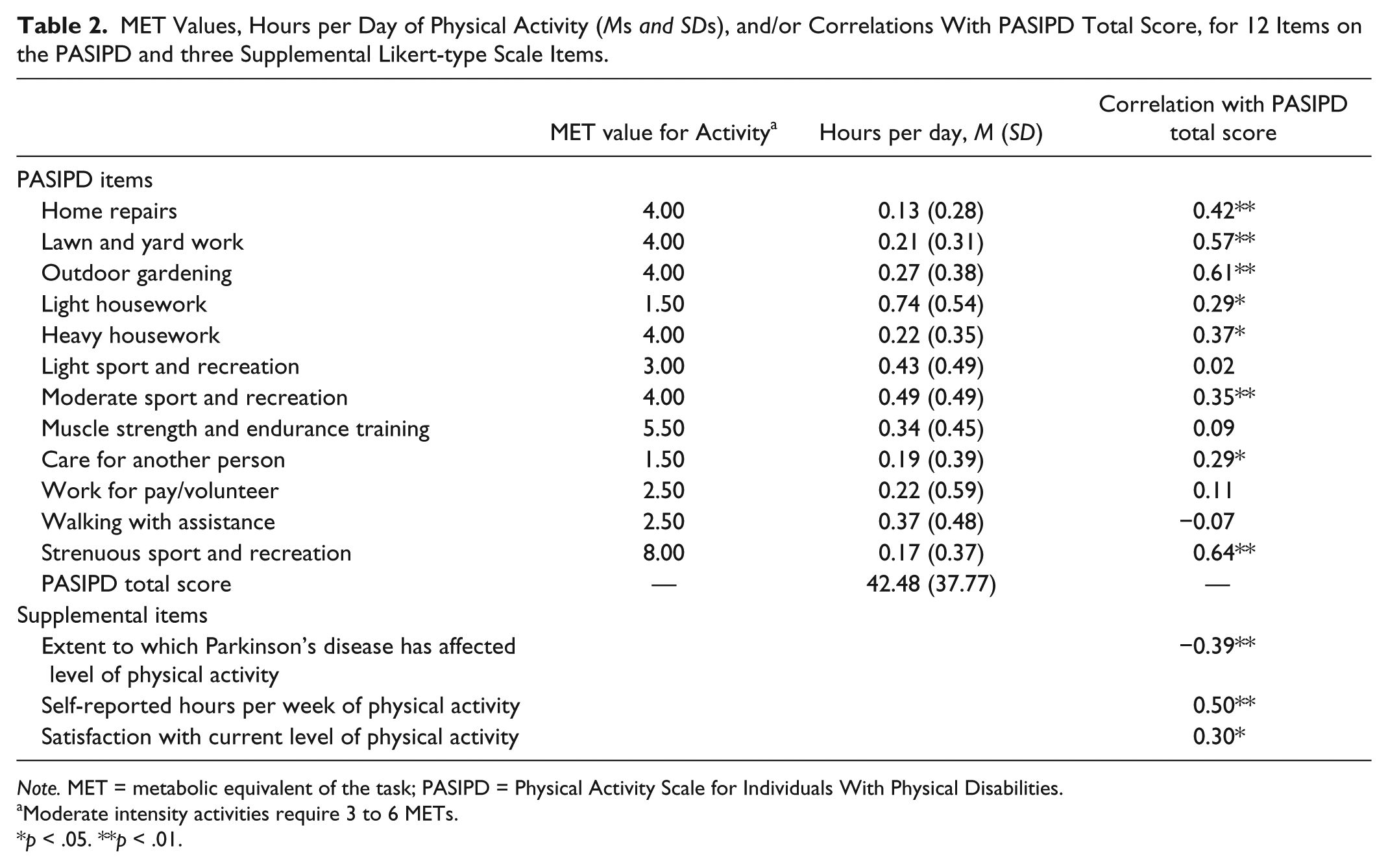
Note. MET = metabolic equivalent of the task; PASIPD = Physical Activity Scale for Individuals With Physical Disabilities.
Moderate intensity activities require 3 to 6 METs.
p < .05. **p < .01.
The mean self-reported physical activity rate within this sample was 42.48 MET hr/day per day (SD = 37.77 MET hr/day). Close to 80% of the subjects obtained a PASIPD total score of 60 or less, which is a third of the possible maximum score of 199.5 MET hr/day.
Correlations between the PASIPD total score and self-report items are also presented in Table 2. Self-reported hours per week of physical activity (M = 11.65, SD = 13.15 hr/week) was significantly positively correlated (.50) with the total PASIPD score. Similarly, levels of satisfaction with the current rate of physical activity had a statistically significant positive correlation (.30) with the total PASIPD score. It should be noted, however, that 58% of respondents disagreed or strongly disagreed with the statement “I am satisfied with my current levels of activity,” suggesting that there is a perceived need among individuals with PD for greater amounts, or more satisfying/pleasurable forms of physical activity.
Qualitative Evaluation of Responses to Open-Ended Questions
Stepwise replication of the results was undertaken, to improve the dependability of the findings. To this end, thematic analysis was conducted independently by two members of the research team (J.J.-P. and A.M.J.). At the outset of the analysis, each researcher read the open-ended responses 3 times to become familiar with the material. A fourth reading of the data was then conducted by each researcher, to identify the most common responses for each item. After the researchers reached consensus as to the themes that emerged from the qualitative data, a frequency count was produced that was used to determine the proportion of individuals that endorsed each theme. The five most popular physical activities reported by respondents were (a) walking (58% of respondents), (b) grocery shopping or going to the mall (53% of respondents), (c) gardening/yard work (47% of respondents), (d) housework (42% of respondents), and (e) formal exercise training (38% of respondents), including activities such as cycling, fitness classes, swimming, or strength training. Other fairly common activities included physical therapy, yoga, and stretching. It is important to note that individuals who participated in formal exercise training tended to engage in more of these “other” activities than the rest of participants. Activities in which individuals would have liked to engage, but did not feel capable of performing, included (a) organized sports and exercise (40% of respondents), including cycling, swimming, fitness classes or outdoor activities; (b) walking (27% of respondents); and (c) golfing (13% of respondents). The most commonly desired, but not accessible, activities were (a) swimming or water aerobics (29% of respondents) and (b) dancing (12% of respondents). It is, however, important to note that a large proportion of individuals (41%) indicated that, overall, access was not an issue. The major facilitators to engaging in physical activity included (a) improvement of PD-related symptoms following increased physical activity (27% of respondents), such as balance, mobility, and gait; (b) social motivation (21% of respondents), including factors such as having an exercise partner; and (c) regularity or predictability of the exercise (18% of respondents). In particular, some participants expressed the desire to attend fitness classes targeted specifically for individuals with PD. In addition, the major barrier to physical activity was PD-related symptoms such as lack of balance, gait impairment, decreased mobility, tremors, lack of strength, and tiredness (59% of respondents). A few participants reported other issues worth exploring in future studies, such as fear of falling, social anxiety related to PD symptoms (e.g., self-consciousness regarding tremor), poor weather, and transportation issues.
Discussion
Understanding physical activity, and the context in which it occurs, is essential for the planning and execution of efficient and effective physical activity programs for individuals with PD. However, the literature provides little information with regard to current levels of physical activity, or the facilitators and barriers to engagement. In the present study, a PD diagnosis was associated with a decrease in physical activity levels (36% of the sample self-reported a profound decrease in physical activity over the course of their disease). Interestingly, however, the individuals with PD in the present study reported relatively high levels of physical activity. Specifically, the mean self-reported physical activity rate within this sample was 42.48 MET hr/day (SD = 37.77 MET hr/day), which is almost 3 times higher than that reported by Washburn et al. (2002; M = 16.5 MET hr/day, SD = 13.40) for the individuals with physical disabilities above the age of 51 years who were sampled to create the PASIPD. It is important to note, however, that the validation sample for the PASIPD included individuals with conditions such as spinal cord injury, paraplegia, amputations, and muscular dystrophy (Washburn et al., 2002), which would produce significantly greater limitations to mobility than that among the community-dwelling individuals with PD sampled within the present study.
The American College of Sports Medicine and the American Heart Association have suggested that to gain health benefits, seniors with chronic conditions that affect mobility should engage in moderately intense activity (3 to 6 METs) at least 5 days per week for 30 min, or in vigorous activity (>6 METs) at least 3 days per week for 20 min, as well as in muscle strength exercise (Nelson et al., 2007). This recommendation is intended to be in addition to engagement in “routine activities of daily living of light-intensity (e.g., self care, cooking, casual walking or shopping), or moderate-intensity activities lasting less than 10 minutes in duration (e.g., walking around the home or office, walking from the parking lot)” (Nelson et al., 2007, p. 1098). To illustrate these recommendations in terms of PASIPD values, a hypothetical score was calculated for an older adult with limited mobility who engaged in (a) 2 to 4 hr per day of walking, 5 to 7 days per week; (b) light sport or recreational activities for less than an hour per day, 5 to 7 days per week; (c) moderate sport or recreational activities for less than an hour per day, 5 to 7 days per week; (d) muscle strength training for less than an hour per day, 5 to 7 days per week; and (e) light housework for 1 to 2 hr per day, 5 to 7 days per week. The PASIPD score for such an individual would be 13.74 MET hr/day. Given that the participants with PD in our study obtained a PASIPD score mean of 42.48 ± 37.77 MET hr/day, and the self-reported average hours per week of physical activity was equivalent to an hour and a half of activity per day, it is evident that these individuals met and considerably exceeded the recommended levels of physical activity for cardiovascular health benefits. The fact, however, that the majority of participants (58%) were not satisfied with their current physical activity levels suggests that there is room for improvement in physical activity rates—and satisfaction with physical activity participation—among individuals with PD. This low satisfaction is possibly due to a perceived lack of improvement in PD symptoms.
The thematic analysis illustrated that walking, grocery shopping or going to the mall, garden/yard work, housework, and formal exercise training were the most common activities undertaken by respondents. In addition, although participants expressed a desire to engage in higher intensity activities such as organized sports, fitness classes, and golfing, they indicated that they felt unable to engage in these activities due to their PD symptoms. Participants indicated that improvement in PD symptoms, opportunities for social interaction, and organizational structure of formal activities (particularly within those activities that are tailored to the needs of individuals with PD) would facilitate their engagement in physical activity. Even though individuals with PD have physical limitations that may restrict their full participation in traditional forms of physical activity, the individuals in our study were eager to engage in more challenging and frequent activities, given the availability of “the right programs.” To this end, better attention to the grading of exercise difficulty may facilitate some of the activities that individuals with PD cited as being difficult to perform. For example, outdoor activities such as hiking, cycling, and golf may be facilitated with appropriate occupational therapy interventions. Outdoor hiking can be made safer through the use of Nordic walking poles that enhance postural stability, and reduce falls risk for individuals with PD. Outdoor cycling is a reasonably safe activity when done on properly maintained trails in appropriate weather—but programming for individuals with PD may be enhanced to encourage indoor cycling first, as a method for building cycling skill and confidence. There are even occupational therapy interventions that may facilitate golfing for individuals with PD—the predominant risk associated with this activity is falling over while bending to place or retrieve the ball, and this risk may be mitigated with the use of a wand to place and retrieve the golf ball from the turf.
Limitations and Directions for Future Research
The presented data are intended to be descriptive of the amount of physical activity engaged in by individuals with PD, as well as the barriers and facilitators to this activity. As such, no control group was evaluated with the questionnaire. Thus, the present study cannot draw direct conclusions as to whether or not the physical activity engaged in by participants is greater than expected, for an age-matched sample, using this measurement tool. Furthermore, the sample was (necessarily) self-selected, as all participants volunteered for participation in the mailed survey. This may have resulted in a sample that engages in more physical activity than is typical within a more general population of individuals with PD. Also, the quantification of physical activity was done entirely via self-reported measures, and so it is possible that participants may have inflated (either intentionally or unintentionally) their physical activity levels. Likewise, it was not possible to collect objective indices of disease severity (e.g., scores on the UPDRS), and this necessitated self-reported measurements of functional impairment. In the future, researchers may wish to evaluate the present findings in the context of more objective measures of physical activity and disease severity. Finally, emotional distress (such as tremor embarrassment and fear of falling) should be further examined as deterrents of physical activity engagement.
Conclusion
Despite the limitations to the present study, these findings provide evidence of the physical activity that is engaged in by individuals with PD, as well as some of the most common barriers and facilitators to this activity. This information may be useful in the establishment of physical activity guidelines regarding types, intensity, frequency, and duration of activities that support PD symptom management, and improve quality of life.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.