
Abstract
We describe an innovative approach to teaching homeless men the critical thinking skills underlying adaptive decision making and self-regulation needed to bolster resilience in the face of multiple and complex personal challenges. Single men living in a transitional housing facility for the homeless were taught the BrainWise curriculum (n = 210) along with other educational, career, and life skills programs, and tested 4 months later. This group was compared with a smaller control group (n = 61) of men from the same and similar facilities. Outcomes were measured through self-reports of executive functions (Behavior Rating Inventory of Executive Function [BRIEF]), problem solving (Wasik Problem Solving Rating Scale [WPSRS]), coping (Coping Self-Efficacy [CSE]), and knowledge of the thinking skills taught through BrainWise (BrainWise Knowledge Survey [BKS]). All measures showed adequate internal consistency reliability and less strong, but significant, test–retest stability. As expected, self-reported skills in executive function, coping self-efficacy, problem solving, and BrainWise knowledge covaried in predictable ways. The attrition between the pretest and posttest was not predicted by any of the major outcome measures. The sample of 108 men in the Treatment Group who were still in the program 4 months later exhibited significant improvements on all BRIEF composites and subscales, CSE, and the BKS, but not on the WPSRS. In contrast, the remaining 37 Control Group men showed many fewer improvements in the BRIEF scores and a decrease in the WPSRS score. The results suggest the efficacy of BrainWise and measurement of these skills in the vulnerable population of homeless individuals; however, challenges of this type of research and limitations of this study are discussed.
The societal problem of homelessness often appears intractable given the number of programs that have been instituted with limited success. In January 2015, there were 564,708 homeless people in the United States (U.S. Department of Housing and Urban Development [USDHUD], U.S. Census Bureau, & U.S. Bureau of Labor Statistics, 2015). 1 An 11% decrease in the rate of homelessness since 2007 has been attributed, in large part, to the billions of dollars in federal funds allocated to programs that assist homeless populations (National Alliance to End Homelessness, 2016). Even with modest declines in national numbers, homelessness remains a social, humanitarian, and economic problem that poses a great challenge to our full understanding of its roots and potential solutions. According to research in the region where the current study was conducted, homelessness is a result of a complex combination of factors. These factors include the lack of access to affordable housing, poverty, unemployment, disabling conditions (including substance abuse and mental illness), lack of access to health care, domestic violence, incarceration, and hospitalization (Metro Denver Homeless Initiative, 2015). With these identified causes of homelessness, it is little wonder that research has focused on systemic social, political, and infrastructure changes as interventions. While identifying the structural causes of homelessness is critical to understanding how to prevent it, examining homeless individuals’ psychological characteristics and personal skills, strengths, and resilience may help to inform interventions to bring individuals out of homelessness. The focus of the current study was to examine whether teaching a critical thinking skills curriculum to men living in transitional housing would result in measureable changes in cognitive and coping skills.
Rivlin and Moore (2001) suggest that personal and psychological support for homeless individuals and families should concentrate on fostering a sense of independence and self-efficacy, both of which have been impacted negatively by the state of homelessness (Epel, Bandura, & Zimbardo, 1999). Relatively high rates of mental illness and substance abuse have been documented among single individuals (primarily males) who are homeless, and while homeless families tend to show lower rates of these characteristics, even mild mental illness and substance abuse can be severely damaging to families and the development of children (McGilloway & Donnelly, 2002). The critical thinking intervention used in the current study, the BrainWise curriculum (Gorman Barry & Welsh, 2007), is designed to provide individuals with the thinking “tools” to use personal resources, make adaptive decisions, as well as to avoid the pitfalls that have led to problematic situations in the past, and have been weakened by the systemic effects of homelessness. Fostering such skills should have the eventual outcome of building a sense of independence, control, and efficacy. BrainWise is a structured, yet flexible, curriculum that teaches critical decision-making skills such as identifying problems, using resources, controlling emotions, planning ahead, and communicating messages clearly, and has been used with a range of populations. In February 2013, the Denver Rescue Mission (DRM) introduced and integrated the BrainWise decision making program for adults into the intervention programs it provides single men living in its transitional housing facility. The objective of this project was to evaluate the effectiveness of this approach and measure the degree to which there is improvement in the self-reported executive functions, problem-solving skills, and coping self-efficacy of the participants, compared with a control group not receiving the BrainWise intervention.
In the field of psychology, the construct of resilience is defined as the dynamic processes by which individuals cope with severe adversity in their lives, and the protective factors in the domains of cognition, self-regulation, and other personal strengths that modify the effects of these risks in a positive trajectory (Luthar & Cicchetti, 2000). The critical thinking skills taught and reinforced through the BrainWise program are hypothesized to build on these protective factors, specifically in the areas of executive functions, coping, and problem solving. Existing research on homeless adults focuses on three domains that appear to promote resilience self-efficacy: time perspective (Epel et al., 1999), religion or spirituality among homeless individuals (Snodgrass, 2014; Torchalla, Li, Strehlau, Linden, & Krausz, 2014), and the influence of social context including access to community support (Wolch & Rowe, 1992). A focus on the time perspective of homeless individuals is particularly relevant to executive functions, the cognitive skills engaged when attempting to attain future goals, and one of the primary outcomes of the BrainWise intervention assessed in this study. Research on time perspective among homeless adults compared the experience of homeless individuals with a future-orientation or a present-orientation and found correlations between individuals’ time reference and self-efficacy (Epel et al., 1999). Those with future-orientation were less likely to be depressed and more likely to have higher self-efficacy and spend more time searching for housing and employment. Those with present-orientation were more likely to find immediate though unstable housing arrangements. Present-orientation was found to be adaptive for survival in homelessness, but did not enable them to move out of their situation. Epel et al. (1999) did not measure these constructs in terms of causation; thus, we do not know if the present-orientation was a result of becoming homeless or if it was a factor that led them into homelessness. The BrainWise program utilized in the current study was designed to teach executive functions, among other critical thinking skills, and it specifically addressed the idea of “time perspective” by teaching individuals the importance of considering the consequences of their actions and how to plan and set goals. Regarding the “social context” aspect of resilience, this was targeted within the BrainWise curriculum when individuals considered their “constellation of support” to help them solve problems. Finally, religion or spirituality as a facilitator of resilience was also relevant due to the focus of the specific living context of the homeless men examined in our study, and the potential that this resilience factor could interact in interesting ways with the BrainWise intervention.
One of the goals of many interventions for the homeless population is to promote self-sufficiency and resilience; that is, the human capacity to adapt to and overcome stress and adversity. Research on resilience in homeless populations has focused almost exclusively on homeless youth, with some information on adolescents who are aging out of foster care (e.g., Kidd & Davidson, 2007; Rew & Horner, 2003). One potential explanation for this dearth of information on resilience in homeless adults is a tendency for researchers to view resilience as a developmental task that evolves into psychological hardiness, a more complex capacity for facing challenges of adulthood (Crowley & Hobdy, 2003). The limited research on resilience in homeless adults homeless primarily involves women or families with small children (Jones, 2006). This could be a result of convenience sampling as researchers often seek participants from temporary or transitional housing, shelter locations most likely to house women and families with children (USDHUD et al., 2015). When resilience has been studied among homeless populations, it is often looked at in direct relation to addiction, an association that implies resilience is not a factor in coping with homelessness; rather, lack of resilience leads to debilitating addiction (Jones, 2006). A construct related to resilience, coping, has also been relatively understudied in the homeless population, but represents one of the outcome measures in this study. Ferguson, Bender, and Thompson (2015) identified different coping styles in male and female young adults that were also predictive of different legal and illegal employment outcomes. The current study fills a gap in the literature on resilience among homeless adults by addressing a cognitive intervention that is designed to teach executive functions and other self-regulation skills to promote self-sufficiency after they have left transitional housing.
Regarding interventions to reduce homelessness, most previous research has focused on providing housing for the homeless, treatment for mental illness, or drug and alcohol abuse interventions (Fischer, 2000; Patterson & Tweed, 2009; Slesnick, Guo, Brakenhoff, & Bantchevska, 2015; Upshur, Weinreb, Bharel, Reed, & Fisard, 2015; Washington, 2002). Forchuck et al. (2008) conducted an intervention for the homeless by providing them with access to and assistance in obtaining and retaining housing immediately after being released from a psychiatric facility. All of the participants in the Treatment Group had been able to retain housing 3 months after release. Only one person in the control group had been able to find housing, a marked contrast from those who had received help. Seidman et al. (2003) found that providing homes may improve the cognitive functioning of previously homeless persons with severe mental health issues. Morse et al. (2006) looked at the treatment of homeless individuals with mental illness and drug addictions and found that the groups receiving drug and alcohol treatment and/or mental health services amassed more days of stable housing than those without either of these treatments. In the case of the current study, the adult male participants were living in a transitional housing facility that provided a variety of services designed to promote adaptive functioning and self-sufficiency for their lives after the program.
A small number of studies have focused on interventions targeting the improvement of a variety of basic cognitive skills to improve adaptation, which generally do not include the critical thinking skills and executive functions that are the focus of BrainWise. Backer and Howard (2007) highlighted some strategies for assisting homeless persons who experience impairments in cognitive functioning, such as behavioral reinforcement, structured skill learning, and cognitive remediation. Burra, Stergiopoulos, and Rourke (2009) note that anywhere between 4% and 7% of homeless persons display generalized cognitive deficits, suggesting that these deficits require interventions in order for the person to function productively in society. In a study of homeless men in a sample gathered from a shelter in Milwaukee, Wisconsin, Solliday-McRoy, Campbell, Melchert, Young, and Cisler (2004) found that 80% showed impaired cognitive functioning, clearly a much higher rate than found by Burra et al. (2009). They noted that standard interventions, such as the provision of housing and drug/alcohol treatment, might not be appropriate for individuals with serious cognitive deficits. Effective interventions, the authors emphasize, consist of behavioral modification strategies, repetition of material, and structured skill-learning procedures (Solliday-McRoy et al., 2004). Washington (2002) noted that the opportunity to learn life skills has enabled formerly homeless people to remain self-sufficient after leaving structured programs. An understanding of the most effective interventions for individuals experiencing homelessness will require a more comprehensive picture of the nature of their cognitive deficits in this population.
As discussed, the enormous adversities that individuals who are homeless face, such as malnutrition, lack of health care, insufficient educational opportunities, and physical and emotional stressors, are likely to negatively impact cognitive functioning. Backer and Howard (2007) reviewed the diversity of cognitive impairments observed in the homeless population that may be the result of mental illness, substance abuse, traumatic or acquired brain injury, progressive neurological disorders, and developmental disabilities. Research has identified impairments in general intelligence (Adams, Pantelis, Duke, & Barnes, 1996; Bremner, Duke, Nelson, Pantelis, & Barnes, 1996; Foulks, McCowen, Duckworth, & Sutker, 1990; Oakes & Davies, 2008; Pluck, Lee, David, Spence, & Parks, 2012), memory (Pluck et al., 2012), and speed of processing (Bremner et al., 1996). In a recent meta-analysis of 10 studies of fair to good quality, Burra et al. (2009) found evidence for specific deficits in verbal and visual memory, attention, speed of cognitive processing, and executive function. It is important to note that a unique feature of the BrainWise intervention is its focus on enhancing individuals’ executive function abilities.
Given that the BrainWise curriculum has been designed to improve problem solving, critical thinking, and executive functions, the performance of homeless individuals on tests of neurocognitive functioning is particularly relevant. In support of a curriculum that targets executive functions, there is evidence that performance on neuropsychological tests of prefrontal functioning is specifically impaired in this population (Davidson, Chrosniak, Wanschura, & Flinn, 2014; Gonzalez, Dieter, Natale, & Tanner, 2001). Of particular relevance to our study of men living in transitional housing, executive function performance on specific neuropsychological tasks has been found to significantly decrease when homeless men are moved to independent housing (and potentially isolated), but improve when they are moved to group housing (Caplan, Schutt, Turner, Goldfinger, & Seidman, 2006; Seidman et al., 2003). It is also challenging to identify neurocognitive deficits that may be related specifically to the condition of homelessness (as either a cause or effect), given that many of the individuals in these studies suffer from comorbid problems of substance abuse, possible brain damage, and/or mental illness (Seidman et al., 1997). In fact, when controlling for current mental illness symptomatology, no differences in overall neuropsychological functioning were found between individuals who were “ever homeless” and those who were never homeless in one study (Bousman et al., 2010).
The purpose of this study was to examine the implementation of the BrainWise curriculum in transitional housing for homeless men and its efficacy for improving the men’s executive functions, problem solving, and coping self-efficacy based on self-reports. As reviewed above, there is a dearth of evidence demonstrating that critical thinking skills can be the target of an intervention for individuals experiencing homelessness and it is a challenge to conduct rigorous research with this population due to its transient nature. The main objective of the study was to explore whether the BrainWise curriculum would be related to positive changes in the self-reported executive functions, coping self-efficacy, and problem solving of single men living in transitional housing, as all three of these skills are likely to contribute positively to resilience and self-sufficiency in the long-term. We also examined three key issues that have implications for interpreting changes that may be observed on the measures: (a) reliability of these self-report measures in a high-risk, vulnerable population that, unlike college students, is unused to taking psychological surveys; (b) associations among scores on problem solving, executive function, coping self-efficacy, and knowledge of the thinking skills taught via BrainWise, and (c) the degree of attrition of participants between the pretest and posttest and potential predictors.
Method
Participants and the Transitional Housing Facility
All participants in both the Treatment and Control groups were enrolled in the New Life Program (NLP), where they received food and shelter for a year or longer. The Treatment Group (n = 210 in pretest phase) resided at a facility formerly used as a hotel/motel located in an industrial area of a city. Control participants (n = 61) came from three sources all affiliated with a single nonprofit organization serving the homeless community, the DRM: (a) the same facility (n = 25); these were men who had come to the transitional housing before the implementation of BrainWise, and were past the phase of NLP where the program was taught); (b) a similar transitional housing facility ( n = 10) located in a smaller city; and (c) dorm-like housing on a farm outside the metropolitan area (n = 26). All men shared a room or sleeping quarters and were required to remain on the facility’s property during the week, with the possibility of weekend passes. Acceptance into NLP in all three transitional housing units involved the completion of a 1- to 3-month intake process at a central facility. Men who successfully completed intake moved to transitional housing and participated in the five-phase NLP program. They followed enforced rules, including no use of drugs or alcohol, and participated in a same slate of courses and activities (with the exception of BrainWise in the Control Group). Although NLP participants could stay for a year or longer, most men left voluntarily after 4 to 6 months in the program.
Demographic characteristics of the men in the Treatment Group and the men in the Control Group are displayed in Table 1. The number of men who remained in the Treatment Group for post-testing was 108 (of the 210 men pretested), and the number of men who remained in the Control Group for post-testing was 37 (of the 61 men pretested). Analyses of Treatment and Control Group differences in demographics and Pretest Phase scores, as well as differences between those men who remained in the program and those who attrited can be found in the Results
Descriptive Statistics for Pretest Phase: Demographics and Outcome Data.

Note. For Ethnicity, n refers to frequency within the larger group. Not reporting ethnicity: Treatment n = 55; Control n = 14. BRIEF = Behavior Rating Inventory of Executive Function; MCI = Metacognitive Index; BRI = Behavior Regulation Index; WPSRS = Wasik Problem Solving Rating Scale; CSE = Coping Self-Efficacy; BKS = BrainWise Knowledge Survey.
Procedures
The men progressed through five phases in NLP: Orientation, Stabilization, Application, Initiation, and Interdependence. BrainWise was taught as the first course in Phase 1 Orientation, followed by classes in counseling, life skills, career training, education, spiritual development, and case management. Each cohort of homeless men entered Phase 1 Orientation together, but progressed through NLP at their own pace. The average time for Phase 1 was 6 weeks, but some individuals took as long as 3 months. In Phase 1, attendance at the sessions was required, and all participants have access to onsite staff members 24/7. The control group received all Phase 1 NLP programs, but not BrainWise.
The BrainWise program and implementation at the transitional housing facility
The program taught the 10 skills (the “Ten Wise Ways”) and explained how practicing these skills builds connections to the cognitive areas of the prefrontal cortex. The men learned that these new pathways divert signals that otherwise would automatically be sent to the limbic system, where the survival instinct responds on emotions and impulse. They received worksheets that include a picture of the brain on which they draw lines showing the connection each skill builds, and learned that if they don’t use the skills, the brain’s survival instinct quickly takes over. For easy retention, the program used the term Wizard Brain for the prefrontal cortex that gradually gains control over the Lizard Brain or limbic system. The other nine skills included building a strong support system, recognizing red flag warnings, managing emotions, separating facts from opinions, asking questions, identifying choices, considering the consequences of choices, setting goals, and communicating effectively (Gorman Barry & Welsh, 2007). The program has been implemented successfully in grades K-12 to regular and at-risk students, children, youth, and adults in outpatient treatment programs, learning disabled groups, welfare mothers, parents, and homeless men. Consistent, positive results have been reported on evaluations conducted across a variety of populations by different researchers (Gati, 2013; Gorman Barry & Welsh, 2007; Norwood et al., 2015; OMNI Research and Training, 2001; Persing, Gorman Barry, Welsh, Cazzell, & Peifer Reyes, 2011; Rosa et al., 2015; Welsh, Gorman Barry, Atwater Jacobs, & Beddes, 2016).
The BrainWise program was taught in the transitional housing facilities by a trained member of the education staff and other trained volunteers. BrainWise was the first life skills class taught to men as they started NLP. The curriculum was taught in two highly interactive 4-hr sessions, and the teachers and other staff reinforced the skills in the context of the career counseling program in NLP and during their frequent follow-up interactions with the men.
Pre- and post-testing
For the Treatment Group, groups of men (approximately 30 at a time) were pretested soon after they entered the facility and before they began learning the BrainWise curriculum in Phase 1 of NLP. Therefore, the treatment men were pretested in about seven waves over the course of about 18 months. The men were given a consent form and a packet of questionnaires in a folder. One of two researchers (M.W. or P.G.B.) read the consent form aloud as the men read it and answered any questions they had. After signing the consent forms, the men took the four questionnaires (see below) in the same order: BrainWise Knowledge Survey (BKS), Wasik Problem Solving Rating Scale (WPSRS), Coping Self-Efficacy (CSE), and Behavior Rating Inventory of Executive Function—Adult Version™ (BRIEF). One of the two researchers read the items on the questionnaires aloud as the men completed them. Post-testing was done approximately 4 months after the pretests were administered and the same four questionnaires were given in the same order. A member of the educational staff administered the posttests to those men who were still at the facility and who agreed to take the posttests, again helping the men read the survey items, if this was needed. The Control Group men were pretested by PGB or a member of the educational staff at those facilities in the same manner as was done for the Treatment Group. An educational staff member post-tested those men who were still in the facility approximately 4 months after the pretest.
Measures
BRIEF–Adult
This is a standardized rating scale created to measure behaviors that are associated with executive functions in adults aged 18 to 90 years (Isquith, Roth, & Gioia, 2006). The inventory consists of 75 items rated on a Likert-type scale and are focused on real-world situations. There are two components: The Behavioral Regulation Index (BRI) that measures inhibition, shifting, emotional control, and self-monitoring. The other component, the Metacognitive Index (MCI), measures initiation, working memory, planning/organization, task monitoring, and organization of materials.
WPSRS
The measure was developed by Wasik and Bryant (1994) and measures one’s self perception of general problem-solving ability in real-world contexts. It is often used as a measure of coping skills. It is a 20-item Likert-type scale that addresses such concepts as problem identification, goal selection, generation of alternative choices, consideration of consequences, decision making, implementation, and evaluation (Wasik & Bryant, 1994).
CSE
This measure (Chesney, Neilands, Chambers, Taylor, & Folkman, 2006) was designed to measure a person’s change in their ability to effectively cope with challenges or threats. It was designed to be consistent with Bandura’s theory of self-efficacy. It is a 13-item self-report measure that has been found to have relatively strong reliability and validity across demographic groups.
BKS
This survey was designed by Gorman Barry and Welsh and includes 18 items pertaining to the specific thinking skills taught in the BrainWise Curriculum, avoiding the unique terminology of the program. Participants respond on a Likert-type scale for each item in terms of how useful they find critical thinking strategies such as planning, seeking advice, and controlling emotion in their daily lives.
Results
Descriptive Statistics and Group Comparisons
The means and standard deviation for the Treatment and Control Groups, for each of the five outcome measures administered during the Pretest Phase, can be found on Table 1. Performance scores for the BKS, WPSRS, CSE, BRIEF-MCI, and BRIEF-BRI, as well as the demographic characteristics of each group are reported. Independent t tests revealed no significant differences between the two groups at the Pretest Phase in age or years of education. Similarly, a chi-square test found no significant difference between the groups in the distribution of men across ethnic group. Finally, independent t tests found that the men in the two groups did not differ in baseline scores on any of the five outcome measures.
Reliability of Measures
The internal consistency of each of the four measures was examined with the Treatment and Control Groups combined both at the Pretest (n = 271) and at the Posttest (n = 145), and all outcome measures were found to be in the acceptable range of reliability. The WPSRS had an internal consistency of alpha =.73 at Pretest and .72 at Posttest. The CSE had an internal consistency of alpha = .93 at Pretest and .96 at Posttest. The entire BRIEF had an internal consistency of alpha = .97 at both the Pretest and Posttest. The self-designed BKS had an internal consistency of alpha = .69 at Pretest and .77 at Posttest. The test–retest stability of these five measures was examined on the sample that completed both the Pretest and Posttest (n = 145), and all measures, with the exception of the WPSRS demonstrated reasonable stability over a period of about 4 months. The CSE demonstrated moderate stability, r(145) = .43, p < .0001, as did the BKS, r(146) = .44, p < .0001, and the BRIEF-MCI, r(143) = .60, p < .0001, and BRIEF-BRI, r (143) = .59, p < .0001. In contrast, the WPSRS showed poor test–retest stability across the 4-month interval, r(146) = .13, p = .06.
Associations Among Measures
Correlations among the five measures were examined at the Pretest and Posttest sessions in the combined Treatment and Control Group samples. As seen in Table 2, the Pretest scores (above the diagonal) on all five measures intercorrelated significantly and in the expected direction. That is, negative correlations were seen between the two BRIEF composite scores (higher scores indicating EF problems) and the CSE, WPSRS, and BKS; and positive correlations were observed among the CSE, WPSRS, and BKS. At the Posttest (below the diagonal on Table 2), all the correlational patterns were the same except in the case of the WPSRS. The Posttest scores on the WPSRS did not correlate significantly with the BRIEF composite scores, BKS, or CSE. Posttest correlations among the measures were also conducted within the Treatment and Control Groups separately, and the same patterns were observed.
Correlations at Pretest Phase and at Posttest Phase Across Both Treatment and Control Groups.

Note. Pretest Phase correlations are above the diagonal and Posttest Phase correlations are below the diagonal. BRIEF = Behavior Rating Inventory of Executive Function; MCI = Metacognition Index; BRI = Behavior Regulation Index; CSE = Coping Self-Efficacy; WPSRS = Wasik Problem Solving Rating Scale; BKS = BrainWise Knowledge Scale.
Correlation is significant below the .05 level (one-tailed). **Correlation is significant at the .01 level (one-tailed).
Attrition
In the Control Group, there was a 39% attrition rate with 37 men remaining in pretest–posttest group of the original 61 Control participants. None of the five main outcome variables, nor age or education, predicted attrition from the Control Group. The Treatment Group demonstrated a 49% attrition rate, with 108 men remaining in the pretest–posttest group of the original 210 Treatment participants. This higher attrition rate was not surprising given that the Treatment Group was almost 3 times larger than the Control Group. None of the five outcome measures nor years of education predicted attrition within the Treatment Group. However, the men who attrited from the Treatment Group were significantly younger (40.84 years) than the men who stayed in the program (44.95 years), t(206) = 2.62, p < .01.
Pretest–Posttest Changes on Measures in Treatment and Control Groups
Because the Treatment and Control Groups were so unbalanced in number of participants (2.9:1, Treatment:Control), an analysis of variance (ANOVA) approach to the analysis of Group and Session effects was ill-advised. Therefore, the two groups were analyzed separately with dependent t tests with Session (Pretest vs. Posttest) as the independent variable with a Treatment Group of 108 participants and a Control Group of 37 participants.
The means and SDs for the scores at the Pretest and Posttest, as well as the analyses of Pretest to Posttest changes in the Treatment Group can be seen in Table 3. Dependent t tests on Pretest to Posttest changes in Treatment Group yielded significant improvements in the BKS, CSE, and the BRIEF-MCI and BRIEF-BRI (as well as on all of the subscale scores of the BRIEF: Inhibit, Shift, Initiate, Planning and Organization, Emotional Control, Self-Monitoring, Task Monitoring, and Organization of Materials). The only measure on which significant improvements were not found was the WPSRS. While it is the case that there was substantial statistical power to find session differences in this group of 108 participants, all tests were significant at p < .02, and most were significant at p < .0001.
Pretest and Posttest Descriptive Statistics for Treatment Group on Outcome Measures.
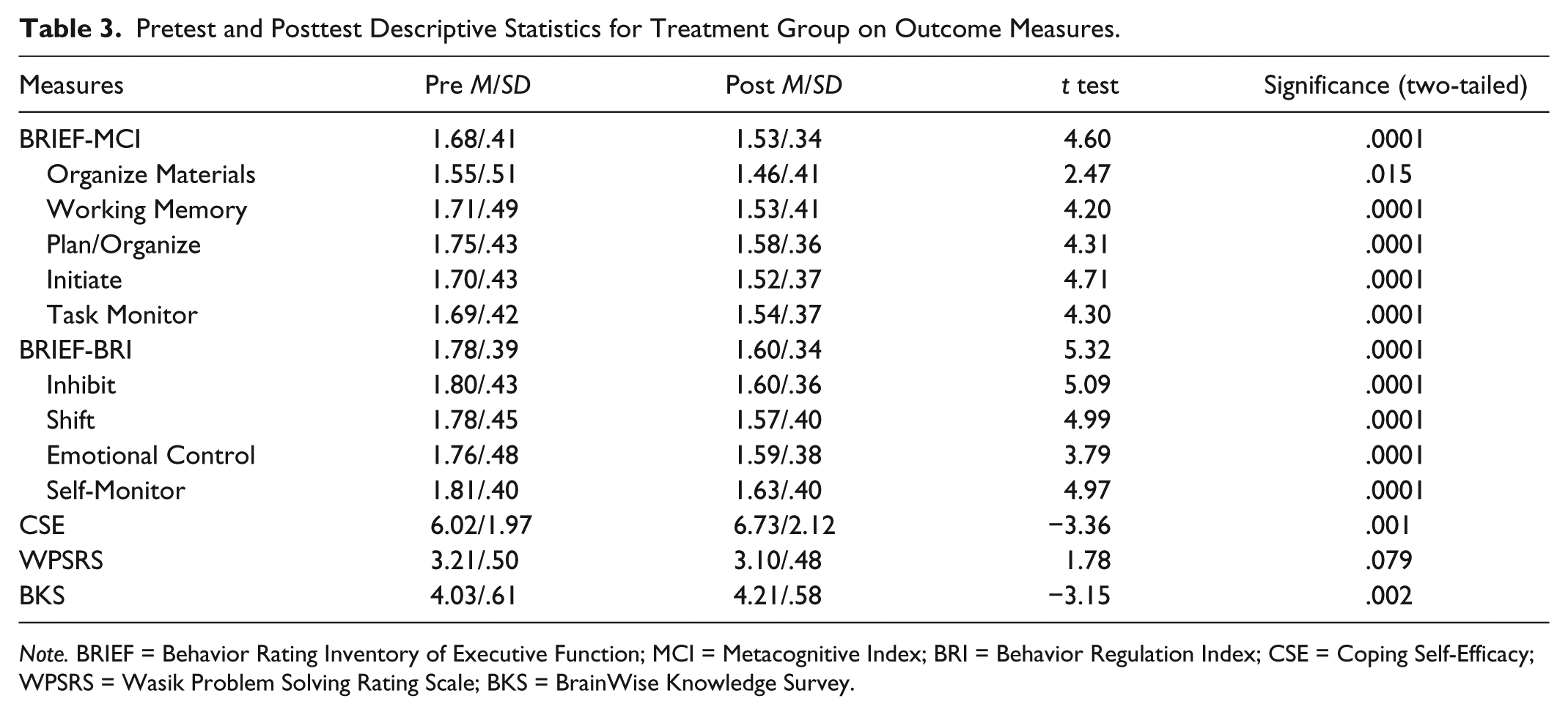
Note. BRIEF = Behavior Rating Inventory of Executive Function; MCI = Metacognitive Index; BRI = Behavior Regulation Index; CSE = Coping Self-Efficacy; WPSRS = Wasik Problem Solving Rating Scale; BKS = BrainWise Knowledge Survey.
The means and SDs for the scores at the Pretest and Posttest, as well as the analyses of Pretest to Posttest changes in the Control Group, can be seen in Table 4. Dependent t tests examining the Pretest to Posttest Changes on all measures in Control Group revealed fewer significant improvements in this group. There were no significant changes in the BKS, CSE, and BRIEF-MCI; however, there was significant improvement in BRIEF-BRI. Among the nine subscales of the BRIEF, significant improvements were observed in the Inhibit, Shift, Initiate, and Planning and Organization, but not in Emotional Control, Self-Monitoring, Task Monitoring, Organization of Materials, BKS, CSE, and BRIEF Metacognition. There was a significant decrease in WPSRS scores from the pretest to the posttest in the Control Group. Again, it is important to note that we had lower statistical power to find differences in the Control Group, and differences in CSE and BRIEF-MCI could be significant with more power. That said, there was sufficient statistical power to reveal some session differences, as well as a decline in WPSRS.
Pretest and Posttest Descriptive Statistics for Control Group on Outcome Measures.
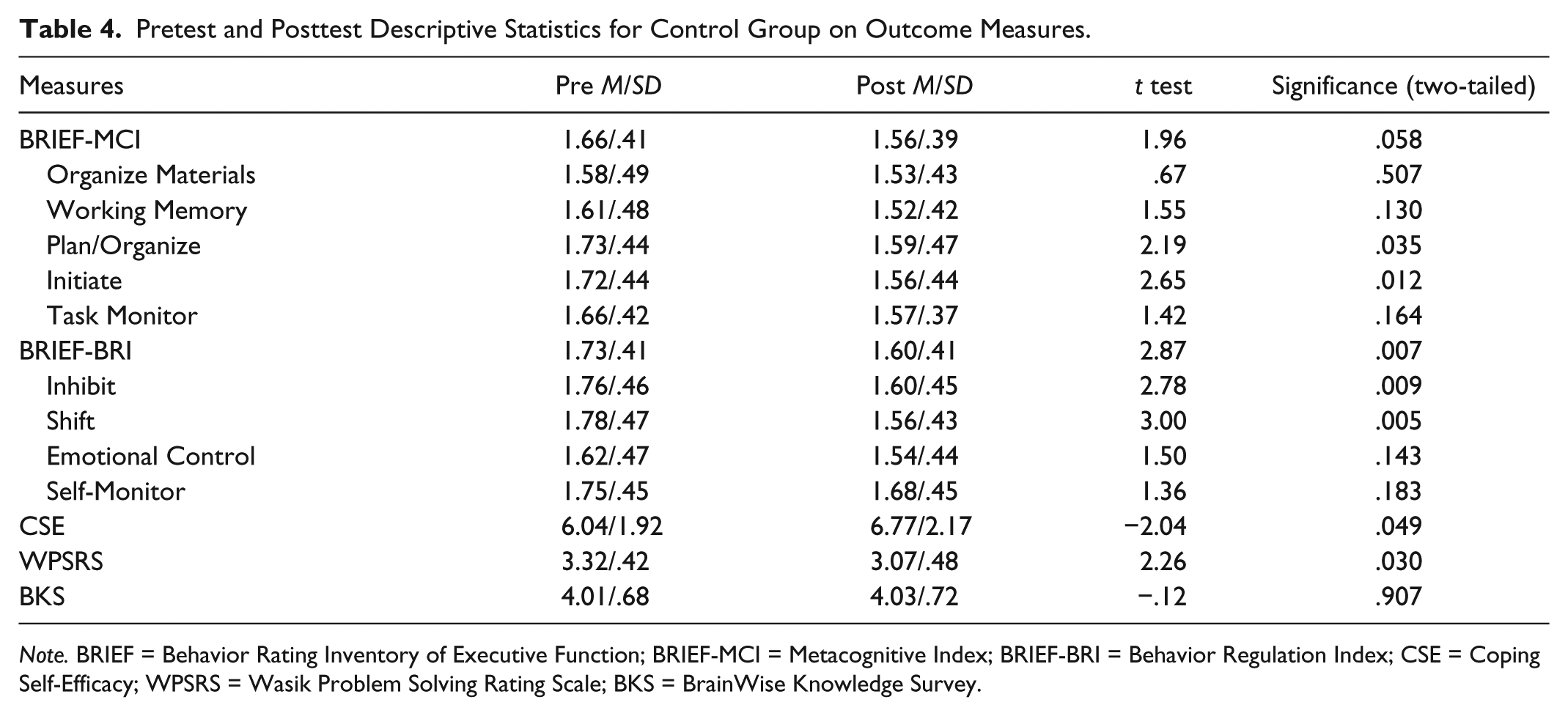
Note. BRIEF = Behavior Rating Inventory of Executive Function; BRIEF-MCI = Metacognitive Index; BRIEF-BRI = Behavior Regulation Index; CSE = Coping Self-Efficacy; WPSRS = Wasik Problem Solving Rating Scale; BKS = BrainWise Knowledge Survey.
Discussion
The purpose of this study was to examine the implementation of the BrainWise curriculum in transitional housing for homeless men and its efficacy for improving the men’s self-reported executive functions, problem solving, and coping self-efficacy. As we have reviewed, there is accumulating evidence of a range of cognitive deficits in the homeless population (e.g., Burra et al., 2009), likely secondary to exposure to a variety of adversities such as poor nutrition, substance abuse, stress, and mental illness (e.g., McGilloway & Donnelly, 2002). In addition to global cognitive impairments, there is emerging evidence of specific neuropsychological deficits in prefrontal cortical function, reflected in decreased executive functions (Davidson et al., 2014; Gonzalez et al., 2001). Links between executive function and adaptive daily functioning have been established in a range of populations (e.g., Cicerone, Levin, Malec, Stuss, & Whyte, 2006; Clark, Prior, & Kinsella, 2002; Gilotty, Kenworthy, Sirian, Black, & Wagner, 2002). Therefore, it was of interest whether a critical thinking skills intervention designed to improve executive functions in daily living, BrainWise, would result in self-reports of fewer executive function difficulties in a vulnerable group of homeless men living in a transitional housing facility.
After a period of approximately 4 months, during which the BrainWise curriculum was taught and reinforced in the context of other interactions with staff at the facility, the Treatment Group of men showed improvement across the entire range of nine executive function skills included in the BRIEF self-report measure. Significant improvements were seen in the following measures: behavioral regulation (Inhibition, Shifting, Emotional Control, and Self-Monitoring) and metacognitive (Initiation, Working Memory, Planning/Organization, Task Monitoring, and Organization of Materials). In contrast, the smaller Control Group exhibited significant improvements in a more limited set of BRIEF components, that is, Inhibit, Shift, Initiate, and Planning/Organization. It is important to note that the men received a range of other educational and job-training programs in both the Treatment and Control Groups that were designed to improve the adaptive functioning of the residents. Therefore, improvements in the Control Group participants would be expected. Moreover, it is difficult to determine the degree to which the improvements in self-reported executive functions in the Treatment Group can be attributed to the addition of BrainWise alone, or the potential interaction of BrainWise with the other programming experienced by the men. In any case, the addition of a curriculum teaching generalizable critical thinking skills to a slate of programs that are targeting specific outcomes (e.g., job training, obtaining a General Education Diploma [GED]), may address the need discussed by Rivlin and Moore (2001) for more personal and psychological support for homeless individuals that facilitates a sense of independence and self-efficacy.
The resilience required to overcome years of homelessness will be strengthened by the opportunity to learn critical and adaptive thinking and problem solving skills from a program such as BrainWise. As discussed in the Introduction, the resilience of homeless adults focuses on three domains, and one of these, self-efficacy in terms of time perspective (Epel et al., 1999), is particularly relevant to the present study. The finding by Epel et al. (1999) that homeless individuals who had a greater future-orientation were less depressed, had higher self-efficacy, and made better decisions with regard to self-sufficiency is interesting in light of the current findings. Executive functions are the skills necessary for future-oriented goal setting and execution of the plans to achieve these goals, and the BrainWise program includes many specific lessons with this future-oriented focus. In addition, the increased self-efficacy of the men in our Treatment Group was also seen in the form of coping self-efficacy (CSE). Increased beliefs in the ability to cope with and overcome adversities are key elements of resilience (e.g., Glennie, 2010; Pölkki, Ervast, & Huupponen, 2005) and one might expect that heightened coping self-efficacy could mediate the execution of the newly acquired BrainWise thinking skills to solve problems as they arise. Indeed, there were significant associations between self-reported executive functions, knowledge of BrainWise thinking skills, and coping self-efficacy, demonstrating the important links between these three measured domains. Our findings that coping self-efficacy improved in the BrainWise group alone represent a unique contribution to a small literature on coping in homeless adults (e.g., Ferguson et al., 2015) which generally does not focus on coping self-efficacy.
Surprisingly, the results for problem solving, as measured by the WPSRS, were disappointing. Although the measure exhibited adequate internal consistency reliability, the test–retest stability was extremely low. The Treatment Group demonstrated no change from Pretest to Posttest on this measure, and the Control Group exhibited a significant decrease in scores, even in light of limited statistical power in this group. The poor stability of this measure clearly indicates unsystematic changes in the scores from Pretest to Posttest, at least in those participants who remained in the full study. It is difficult to know whether this is due to the measure itself, our sample of participants, or some interaction of the two. The WPSRS was moderately correlated with the BRIEF, CSE, and BKS at the Pretest, as would be expected given that these three instruments all included items about daily problem solving. However, at Posttest, the WPSRS was no longer correlated with the other three measures, another indication that this questionnaire operated differently from the others at the Posttest Phase.
As one might expect, the homeless population presents a range of challenges for empirical research, such as the transient nature of group, the many stressors individuals are facing, and the heterogeneity of any sample in terms of educational background, mental illness, and potential brain injuries. Our Treatment and Control Groups each ranged quite a bit in age and in years of education, yet these factors were surprisingly uncorrelated or very weakly correlated with the major outcome measures. Importantly, the population we studied is not one that is accustomed to participating in empirical research; thus, we went to great lengths to make it as easy and palatable for them as possible. Because we had a range of literacy levels, we read the individual items aloud to small groups of men as they completed the surveys, and we answered questions regarding vocabulary that was unclear. Consequently, we were very pleased to see that all the measures had reasonably good internal consistency reliabilities, which was not at all guaranteed given the very vulnerable population that characterized our sample. In addition, we had substantial attrition from the study prior to the 4-month Posttest Phase, and this attrition could not be predicted by education or scores on the executive function, coping self-efficacy, problem solving, and BrainWise knowledge measures, and was related only to age in the Treatment Group. Clearly, there is a myriad of reasons for attrition from our study. While a few men simply refused to take the posttests, the majority of the attrition from the study was due to men who left the facility. The agreement between the men and the organization is that they will stay in the transitional housing facility, attend classes, adhere to the rules, and remain off substances for a period of 1 year, at which point they graduate from the program. Many of the men, both in the Treatment and in the Control Groups, were no longer living at the housing facility at the 4-month follow-up, the vast majority having left voluntarily.
Of particular note, this transitional housing facility provided two of the other resilience components that have been identified in the literature: religion or spirituality among homeless individuals (Snodgrass, 2014; Torchalla et al., 2014), and the influence of social context including access to community support (Wolch & Rowe, 1992). First, the DRM is strongly rooted in a religious tradition and infuses religion and spirituality into many of its programs for the residents. In fact, the instructors of BrainWise at the facility frequently used Bible stories, in addition to problems in the men’s own daily lives, as examples for applying the 10 Wise Ways of BrainWise. Religiosity has been investigated as a coping strategy for homeless individuals, though research on spirituality among homeless populations is scarce (Snodgrass, 2014). Torchalla and colleagues (2014) found that homeless individuals who regularly participated in religious service reported significantly lower rates of alcohol and substance abuse, and Snodgrass (2014) found a relationship between spirituality and expressions of hope and increased ability to manage the negative stereotypes associated with homelessness.
Second, the social context of the transitional housing complex also provides a context for social, emotional, and spiritual support for the men, another potential contributor to their resilience. Consistent with the work by Seidman and colleagues (2003) who found that executive function declines when homeless men are moved to independent housing (and potentially isolated), the group living environment of our current sample may have facilitated their executive function gains. In addition, Wolch and Rowe (1992) found that the experience of being homeless differs based on context (e.g., neighborhood, shelter type, etc.). Mobility patterns of homeless individuals influence the makeup and duration of their social networks, and these networks can be supportive and increase resilience. The fact that men in this study had lived, worked, and took classes together for at least 4 months in a stable, safe environment provided a unique and positive social context for them. Therefore, one would expect these two characteristics of this transitional housing facility to positively impact the self-reported executive functions and coping self-efficacy skills of men in both the Treatment and Control Groups. These factors, as well as all of the other programming available to the Treatment and Control men, highlight that our comparison of the two groups demonstrates potential additional benefits accrued from the introduction of the BrainWise curriculum, and many significant positive changes we did observe in the Treatment Group are encouraging. While the integration of the BrainWise curriculum in this particular transitional housing environment appears to have added value for the residents, one must also acknowledge the potential negative implications of the variety of institutional environments for homeless individuals pointed out by Gowan (2010). According to Gowan, shelters, rehabilitation facilities, and other formal institutions for the homeless can be dominated by what she referred to as “sick talk,” which pathologizes the condition of homelessness. Importantly, BrainWise and other interventions that seek to empower individuals with new and powerful tools for critical thinking would appear to work against this negative messaging.
Three final methodological limitations involve the self-report measures, sample size, and external validity. First, we measured the constructs of executive functions, coping self-efficacy, and problem solving via well-established self-report instruments (including the standardized and normed BRIEF), which is typical in the literature and the pragmatic choice for this population. However, self-report measures do have the potential for a social desirability bias, particularly when the surveys involve sensitive behaviors (Krumpal, 2013). There are two reasons we do not believe social desirability played a strong role in these findings. First, while the surveys did involve items on generally adaptive behavior, these are not considered sensitive behaviors (e.g., questions about drug use, racist behaviors, etc.) that would induce a strong inclination for positive self-presentation. Second, to the degree that a social desirability bias might exist for these measures, there is no reason to believe that it would be stronger at the Posttest than in the Pretest Phase, or in the Treatment Group versus the Control Group. While the participants at the transitional housing facility were involved in a range of programs in which there were incentives to perform well, the consent forms were very clear that survey responses would not impact their treatment at the facilities. As such, there should have been no incentive for the men to alter their responses for a more positive self-presentation on these particular measures. A second limitation was the seriously unbalanced groups with nearly 3 times the number of Treatment participants than Control participants that prevented us from using the preferred ANOVA approach to examine Group × Session interactions on our outcomes. The large Treatment Group and small Control Group clearly biased the study for finding differences in the former and not in the later. Two of the outcomes that were not significant for the Control Group may have been significant with greater statistical power; however, many of the null results were far from statistical trends. The differences observed in the Treatment Group may have been inflated by the statistical power afforded by the large sample size and should be interpreted cautiously until replicated. Finally, with regard to the external validity of these findings, it is important to view them within the particular programming and geographic context of this study. While generalization to other homeless individuals living in other environmental contexts awaits replication, it is important to note that past research evaluating BrainWise in a range of populations (i.e., K-12 students, low income mothers, special needs students) with different behavioral measures has achieved similar improvements in relevant skills (Chilakapati, Swanson, & Sholl, 2009; Persing et al., 2011; Rosa et al., 2015).
In summary, we found that the BrainWise curriculum could be implemented in the context of a transitional housing facility for homeless men and that data can be collected via self-report measures in the Pretest and Posttest Phases. The instruments were notably reliable on a sample that is unaccustomed to taking such measures, and we received excellent cooperation of the men and the staff at these facilities. This work, however, is not without its great challenges, such as high levels of attrition despite the many supportive programs, including BrainWise, made available to the men. With these caveats in mind, the current results nevertheless provide preliminary evidence that a cognitive skills curriculum can be successfully implemented in transitional housing for the homeless and positively influence critical skills for adaptive functioning and resilience. Accompanying an increased sense of control over critical decision making and coping may be an overall elevation of self-esteem, a factor that Kidd and colleagues (e.g., Kidd & Davidson, 2007; Kidd & Shahar, 2008) have identified in their theoretical model to be the single best predictor of resilience in homeless youth. The current findings support that the BrainWise critical thinking curriculum can facilitate executive functions and coping self-efficacy in the face of the many daily challenges and stressors faced by individuals experiencing homelessness. Finally, this project contributes to closing the gap in the literature on the effectiveness of cognitive interventions with this very vulnerable population, and reinforces the positive behavioral outcomes that have been suggested when teaching BrainWise to children, teens, and welfare mothers.
Footnotes
Authors’ Note
The research discussed in this article was originally presented at the 44th Annual Meeting of the International Neuropsychological Society, February 3-6, 2016, in Boston, MA, an abstract of which was published in Meeting Proceedings, Forty Fourth Annual Meeting International Neuropsychological Society, Volume 22, Issue s1, March 2016, pp. i-346.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received internal research grants from the University of Northern Colorado to support this study.