
Abstract
We have previously reported on the findings of a critical realist concurrent triangulated mixed method multilevel study that sought to identify and explain complex perinatal contextual social and psychosocial mechanisms that may influence the developmental origins of health and disease. That study used both emergent and construction phases of a realist explanatory theory building method. The purpose of this article is to present the thesis, theoretical framework, propositions, and models explaining neighborhood context, stress, depression, and the developmental origins of health and disease. The analysis draws on an extensive extant literature; intensive (qualitative), extensive (quantitative), and multilevel studies used for phenomena detection, description, and emergent phase theory development; and the abductive and retroductive analysis undertaken for the theory construction phase. Global, economic, social, and cultural mechanisms were identified that explain maternal stress and depression within family and neighborhood contexts. There is a complex intertwining of historical, spatial, cultural, material, and relational elements that contribute to the experiences of loss and nurturing. Emerging is the centrality of social isolation and “expectation lost” as possible triggers of stress and depression not only for mothers but possibly also for others who have their dreams shattered during life’s transitions. The thesis: In the neighborhood spatial context, in keeping with critical realist ontology, global-economic, social, and cultural-level generative powers trigger and condition maternal, psychological, and biological-level stress mechanisms, resulting in the phenomenon of maternal depression and alteration of the infants’ developmental trajectory.
Introduction
We present here the theoretical framework, propositions, and thesis stemming from a theory building study of neighborhood context, stress, depression, and the developmental origins of health and disease. Our early studies of maternal stress and depression proposed that group-level socioeconomic deprivation, neighborhood environments, social networks, and ethnic diversity had causal effects on postnatal depressive symptomatology and other perinatal outcomes (Eastwood, Phung, & Barnett, 2011). Several recent social epidemiologist commentators have argued for the use of realist philosophy to generate health and social theory (Muntaner, 1999, 2013; O’Campo & Dunn, 2012). Subsequently, we undertook a “critical realist concurrent triangulated mixed method multilevel study that sought to identify and explain complex perinatal contextual social and psychosocial mechanisms that may influence the developmental origins of health and disease” (Eastwood, Jalaludin, & Kemp, 2014). That study used both emergent and construction phases of a realist explanatory theory building method (Figure 1).

Phases of explanatory theory building.
Intensive (qualitative), extensive (quantitative), and multilevel studies were used for phenomena detection and description, and emergent phase theory development (Eastwood, Jalaludin, Kemp, & Phung, 2013, 2014a, 2014b; Eastwood, Jalaludin, Kemp, Phung, & Adusumilli, 2013; Eastwood, Jalaludin, Kemp, Phung, & Barnett, 2012, 2013; Eastwood, Jalaludin, Kemp, Phung, Barnett, & Tobin, 2012; Eastwood, Kemp, & Jalaludin, 2014, 2015; Eastwood, Kemp, & Jalaludin, 2016a).
Drawing on those studies and in keeping with our previously reported protocol (Eastwood et al., 2014), the construction phase undertook abductive and retroductive triangulation of the reported empirical findings and emergent theory development. The methods included “1) defining stratified levels; 2) analytic resolution; 3) abductive reasoning; 4) comparative analysis (triangulation); 5) retroduction; 6) postulate and proposition development; 7) comparison and assessment of theories; and 8) conceptual frameworks and model development” (Eastwood, Kemp, & Jalaludin, 2016b, p. 2; Box 1).
Construction Phase Methods (Eastwood, Kemp, & Jalaludin, 2016b).

Building on the analysis and propositions of the construction phase, we present here the theoretical framework, propositions, and thesis of neighborhood context, stress, depression, and the developmental origins of health and disease.
Theoretical Propositions
Based on the theoretical framework (below) and our published work, we embed a series of realist theoretical propositions. Those propositions will be used for theoretical modeling that will subsequently be utilized in future confirmatory empirical and programmatic studies. The approach taken here will be in keeping with the postpositivist assumption of “impossibility of scientific proof” and the criteria of falsification (Carpiano & Daley, 2006).
From a hypothetico-deductive perspective, Dubin (1969) states that “propositions are often expressed as ‘if a then b’ deductive statements. The hypothetico-deductive approach to theory building requires a ‘closed’ system and that theory be tested within the empirical world with ‘things observable’” (p. 205).
By contrast, as we have previously observed (Eastwood et al., 2016b),
“Critical realism views reality as an ‘open system’ where causative processes are always contextually determined. Critical realism seeks to discover the hidden mechanisms that explain the empirical phenomena.” Thus realist theoretical propositions are about how “mechanisms (M) are fired in contexts (C) to produce outcomes (O).” (Context mechanism outcome [CMO] propositions; Pawson & Tiley, 1997, p. 85)
In addition,
Causal relationships only occur when the generative mechanism comes into operation. Sometimes different mechanisms produce the same outcome. The contextual conditions determine whether the generative mechanism(s) will come into play and the nature of the outcome. The contextual conditions include other mechanisms that may either trigger or counteract the causal mechanism. A graphical representation of the critical realist CMO propositions will be used (Figure 2). (Eastwood et al., 2014)

Graphical representation of critical realist CMO propositions.
Thus, the focus will be on testable realist propositions where “x causes y (in circumstances c).” The explanation may also include comment on the structure that underlies the generative mechanism (structure of X).
Our underlying postulate (untested assumption) is as follows:
Maternal psychological stress is a necessary, but not sufficient, cause of depressive symptoms.
Theoretical Framework
The theoretical framework takes a critical realist perspective of perinatal social context, stress, depression, and the developmental origins of health and disease (Bhaskar, 1975; B Danermark, Ekstrom, Jakobsen, & Karlsson, 2002; Layder, 1993; Pawson, 2006; Sayer, 2000), and builds on the emerging literature on stress process (Aneshensel, 2009; Avison, Aneshensel, Schieman, & Wheaton, 2010; Hogue, Hoffman, & Hatch, 2001; Pearlin, Menaghan, Lieberman, & Mullan, 1981), social isolation (Cacioppo & Hawkley, 2003; Hortulanus & Machielse, 2006), social exclusion (Bonner, 2006; Hutchison, Abrams, & Christian, 2007), social capital (Bourdieu, 1986; Carpiano, 2006; Kawachi, Subramanian, & Kim, 2008; Putnam, 1993), segregation (Acevedo-Garcia & Lochner, 2003; Kramer & Hogue, 2009), acculturation (Berry, 1997; Nauck, 2008), globalization (Florey, Galea, & Wilson, 2007), neighborhood effects on health (Ellen, Mijanovich, & Dillman, 2001; Kawachi & Berkman, 2003; Macintyre, Ellaway, & Cummins, 2002), perinatal adversity (Culhane & Elo, 2005; Matthews & Meaney, 2005; Misra, Guyer, & Allston, 2003), and the developmental origins of health and disease (Barker, 1992; Ben-Shlomo & Kuh, 2002; Gluckman & Hanson, 2006).
We have responded to the call for a realist approach to social epidemiological theory building (C Muntaner, 1999; Raphael, 2006) and draw on the philosopher Bhaskar’s (1975) articulation of critical realism with its ontological stratification of reality. Such a stratified ontological perspective adds theoretical depth to the layered ecological models advanced by earlier social epidemiologists (Kaplan, 2004; Krieger, 2001; Lynch, 2000; Susser & Susser, 1996). The first stratified ontological domain consists of the empirical experienced reality, the actual or possible events if activated, and the real which comprises structures, mechanisms, powers, and agency of participants. The second domain of reality consists of hierarchically ordered levels. Each level has its own specific generative mechanisms that constitute or define a level (B Danermark, 2002). Mechanisms, objects, and events exist at each different strata which I have defined here as biological, psychological, social, cultural, and global economic. The critical realist interpretation also makes a distinction between the real and actual with “generative” or causal powers that may, or may not, be activated depending upon other conditions or context, such as those existing in the “open system” of the social world.
Developmental Origins of Health and Disease
As previously reported (Eastwood, Kemp, & Jalaludin, 2014),
We take as our starting point the proposition that antenatal and postnatal maternal stress and depression adversely impact on the developmental origins of health and disease. We cannot yet be certain of the biological level mechanisms that alter the genotypic and phenotypic response to perinatal adversity but the triggering of genetic, neuroendocrine and physiological mechanisms, and psychological and nutritional stress are regarded as strong contenders. (Gluckman & Hanson, 2006; Matthews & Meaney, 2005; Meaney, 2010)
Maternal stress at the psychological level thus may trigger biological-level mechanisms that alter her unborn infants’ developmental trajectory (Gluckman, Hanson, & Beedle, 2007; Meaney, 2010). The role here of antenatal maternal depression is less clear. It is either an indicator and an outcome of maternal psychological-level stress, or alternatively, an independent trigger of biological-level events as suggested by its impact on infant temperament (Davis et al., 2007).
We have also previously noted (Eastwood, Kemp, & Jalaludin, 2014, p. 1) that “postnatal depression and anxiety have consistently been demonstrated to adversely impact on maternal-infant interaction and attachment (Beck, 1995; Martins & Gaffan, 2000; Murray, Stanley, Hooper, King, & Fiori-Cowley, 1996) and subsequent child cognitive, language, behavioural and psychological problems” (Cogill, Caplan, Alexandra, Robson, & Kumar, 1986; Cummings & Davies, 1994; Downey & Coyne, 1990; Gelford & Teti, 1990; Murray, Hipwell, Hooper, Stein, & Cooper, 1996; Sohr-Preston & Scaramella, 2006). Postnatal depression may also be associated with subsequent maternal and childhood obesity (Herring et al., 2008; Surkan, Kawachi, & Peterson, 2008), not breast fed (Dennis & McQueen, 2009; Henderson, Evans, Straton, Priest, & Hagan, 2003), and maternal health harming behaviors such as tobacco and drug addiction (Cinciripini et al., 2010; Lancaster et al., 2010; Rubio, Kraemer, Farrell, & Day, 2008).
Drawing on the above theoretical position and the findings of our published studies (Eastwood, Jalaludin, Kemp, Phung, & Barnett, 2012; Eastwood, Jalaludin, Kemp, Phung, Barnett, & Tobin, 2012; Eastwood et al., 2015), we have made the following three critical realist (CMO) propositions (Figure 3).

CMO model of maternal depression and outcomes.
Stress and Depression
That depression is caused by psychological stress is increasingly certain (Kinderman, 2005; Stone, Lin, & Quartermain, 2008). Less clear, in critical realist terms, is whether stress is a necessary condition and must be present for there to be depression. The phenomenon of perinatal depression has repeatedly been found to be associated with stressful life events (Beck, 1996, 2001; National Health and Medical Research Council [NHMRC], 2000; O’Hara & Swain, 1996; Wilson et al., 1996). We agree with Beck (1992, 1993, 2002) that depressed mothers experience an “incongruity between expectations and the reality of motherhood,” a sense of pervasive loss, and loneliness. We propose here that this psychologically felt stress, be it internally or externally triggered, is a necessary condition for perinatal depression.
“But stress in itself is not a sufficient mechanism and the tendency of stress to cause depression is conditional on other personal characteristics and social and cultural context” (Eastwood et al., 2013). Following Pearlin et al. (1981), it is argued here “that the generative power of stress is conditioned, or moderated, by personal resources such as coping and by social resources such as social support” (Eastwood et al., 2013). Those personal resources such as mastery, agency, self-esteem, optimism, mattering, emotional reliance, and personal predisposition may themselves be conditioned by social context.
The notion of agency and mastery, from a critical realist perspective of agency (Archer, 1995, p 175), means that mothers themselves have “generative powers,” and may, or may not, be able to influence and control the environmental and experiential forces acting upon them. But the actual outcome will be the result of the interplay between what Archer (1995, p. 175) calls structural, cultural, and agential emergent properties of society, each with its own “generative mechanisms” and relative autonomy. Thus, a mothers individual agency, and ability to “cope,” may be enabled or blocked by her social (structural) and cultural context.
The Triggering Events
Drawing on the stress process model, we further argue that the triggers of perinatal depression are event stressors
such as poor health, childbirth experience, loss of status, loss of financial income, loss of control, unmet expectations, irritable infant and partner behaviour. Chronic stressors may also contribute and include: status strains (i.e. race, sole parent, poverty, and religion), role strains (i.e. wife, motherhood, and daughter), ambient strains (i.e. neighbourhood crime, services, physical decay of environs), and quotidian strains (i.e. loneliness, daily hassle of sole parenthood). (Eastwood et al., 2016, p. 6)
In keeping with a critical realist meta-theory, these triggering mechanisms arise from structural, cultural, and agential generative mechanisms, including income inequality, class structure, social exclusion, social isolation, and access to social services, neighborhood physical environments, and gender roles, cultural expectations of motherhood, ethnic segregation and acculturation.
Building on the above theoretical position and the findings of our previous individual-level published studies, we have made the following three critical realist (CMO) propositions in relation to psychological-level stress and depression (Figure 4).
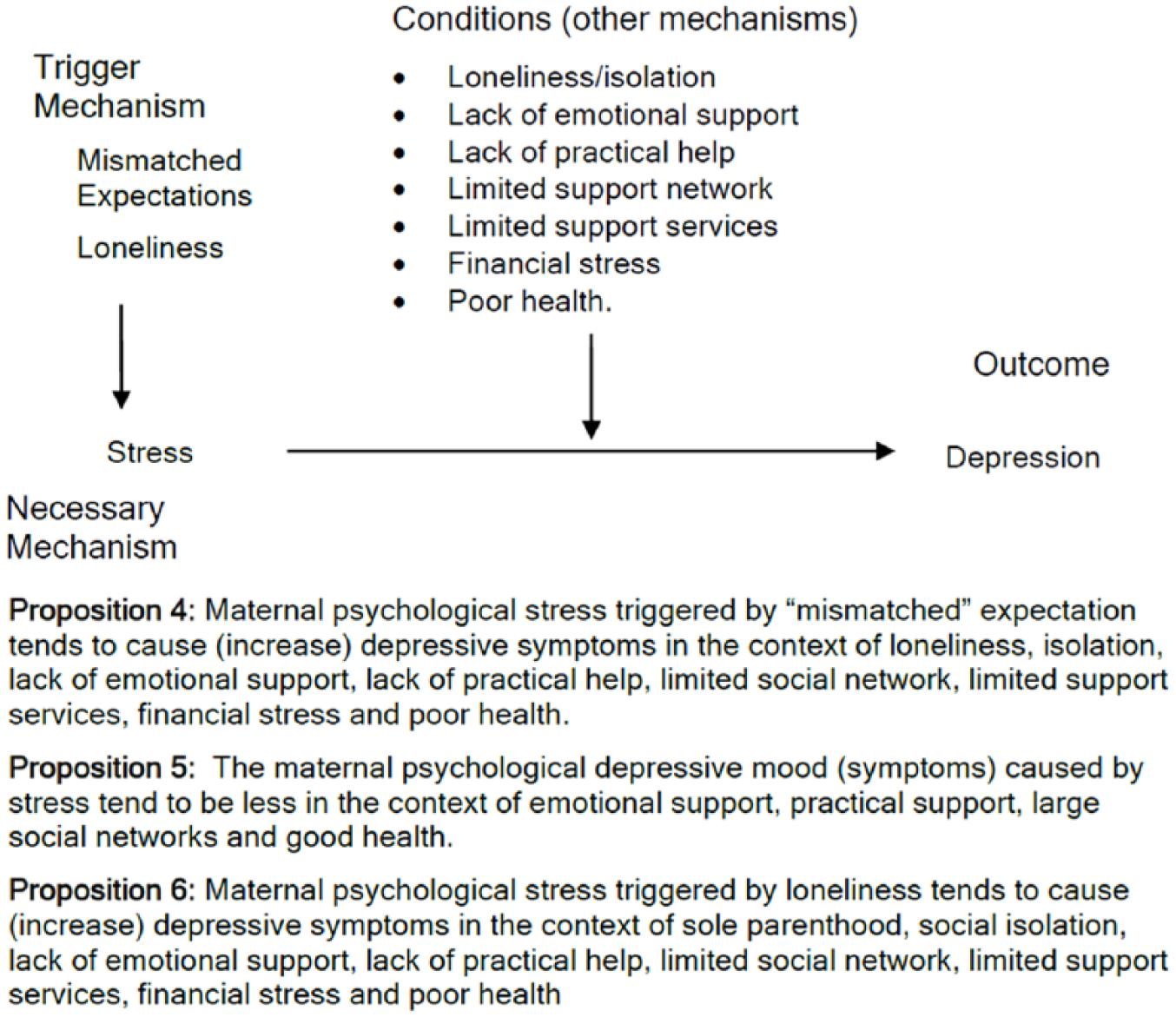
CMO model of psychological stress and depression.
Contextual “Stressor” Mechanisms
Aneshensel (2009) argues that the stress process model provides a means of explaining mental health disparities that arise from people’s disadvantaged placement within a social hierarchy. The emphasis here is on a generative mechanism called social stress that is generated by disadvantaged social status. Social stress is defined as a state of arousal that results from social demands that tax the ordinary adaptive capacity of the individual, or from blocking of the means to attain personal goals. Drawing on social isolation (Hortulanus & Machielse, 2006), materialist (Bartley, 2004), and social exclusion (Millar, 2007) theories, social stress arising from hierarchical placement is joined by theoretical explanations, arguing that mechanisms arising from social and economic structures marginalize individuals and groups from social and material resources, and block attainment of their aspirations. Pregnant women and mothers may be unable to access neighbors, friends, family, services, transport, phone, and their partners’ support. In this social context of exclusion, the expectations and dreams of mothers may be shattered as they lose control and are overwhelmed with pervasive loss.
The social structures generating social exclusion and social stress include occupational class structures, racism, and residential, ethnic, and educational segregation resulting in “depressed communities” with few amenities, decayed environments, and perceived unsafe streets. Business, service, and political structures contribute to the marginalization of “depressed communities” through the centralization of amenities, services, and sporting opportunities. The impact on the lives of mothers is to be “stuck in the middle of nowhere . . . being couped up in a house with a kid 24/7” (Eastwood, Kemp, & Jalaludin, 2014).
Contextual Buffering Mechanisms
The buffering role that support plays, in relation to both the stress process and perinatal depression, is strong and consistently shown (Aneshensel, 2009; Beck, 1996, 2001; NHMRC, 2000; O’Hara & Swain, 1996; Pearlin et al., 1981; Wilson et al., 1996). Studies have consistently shown a negative correlation between postpartum depression, and emotional and instrumental support during pregnancy (Beck, 1996; Menaghann, 1990; O’Hara & Swain, 1996; Richman, Raskin, & Gaines, 1991; Ritter, Hobfoll, Lavin, Cameron, & Hulsizer, 2000; Seguin, Potvin, St-Denis, & Loiselle, 1999). Drawing on our earlier critical realist theory generation, we argue that
the support mechanisms received by mothers are determined by her social and cultural context. Drawing on both Social Network (Crow, 2004) and Social Capital (Kawachi et al., 2008) Theory it is evident that social structures can generate strong social bonds with a clear demarcation between “insiders” and “outsiders.” This “bonding” and “bridging” social capital is generated from complex social structures and has been associated with protection from mental health disorders (Fone, Lloyd, & Dunstan, 2007; Stafford, De Silva, Stansfeld, & Marmot, 2008). However, strong bonding ties within disadvantaged communities also may be a detriment to the health of residents (Kawachi et al., 2008). For migrant ethnic mothers access to support is critical. In this social context they must rely on both ethnic bonding capital and the bridging capital provided by supportive social structures. (Eastwood et al., 2013)
Carpiano (2006) describes neighborhood social capital as a resource inherent within the networks of neighborhood residents, with social cohesion generating the necessary conditions for group members to access those resources. The structural antecedents of both social cohesion and social capital are the local, and surrounding, socioeconomic conditions, residential stability, and ethnic, family, gender, age, and social class composition. Together with policy-level mechanisms such as social and economic interventions, conditions may be created that have a tendency to buffer social and cultural stressor mechanisms.
Drawing on the above theoretical position and the findings of our ecological and multilevel published studies we have made the following two critical realist (CMO) propositions in relation to social stress, psychological stress, and buffers (Figures 5 and 6).

CMO model of social stress, psychological stress, and buffers.
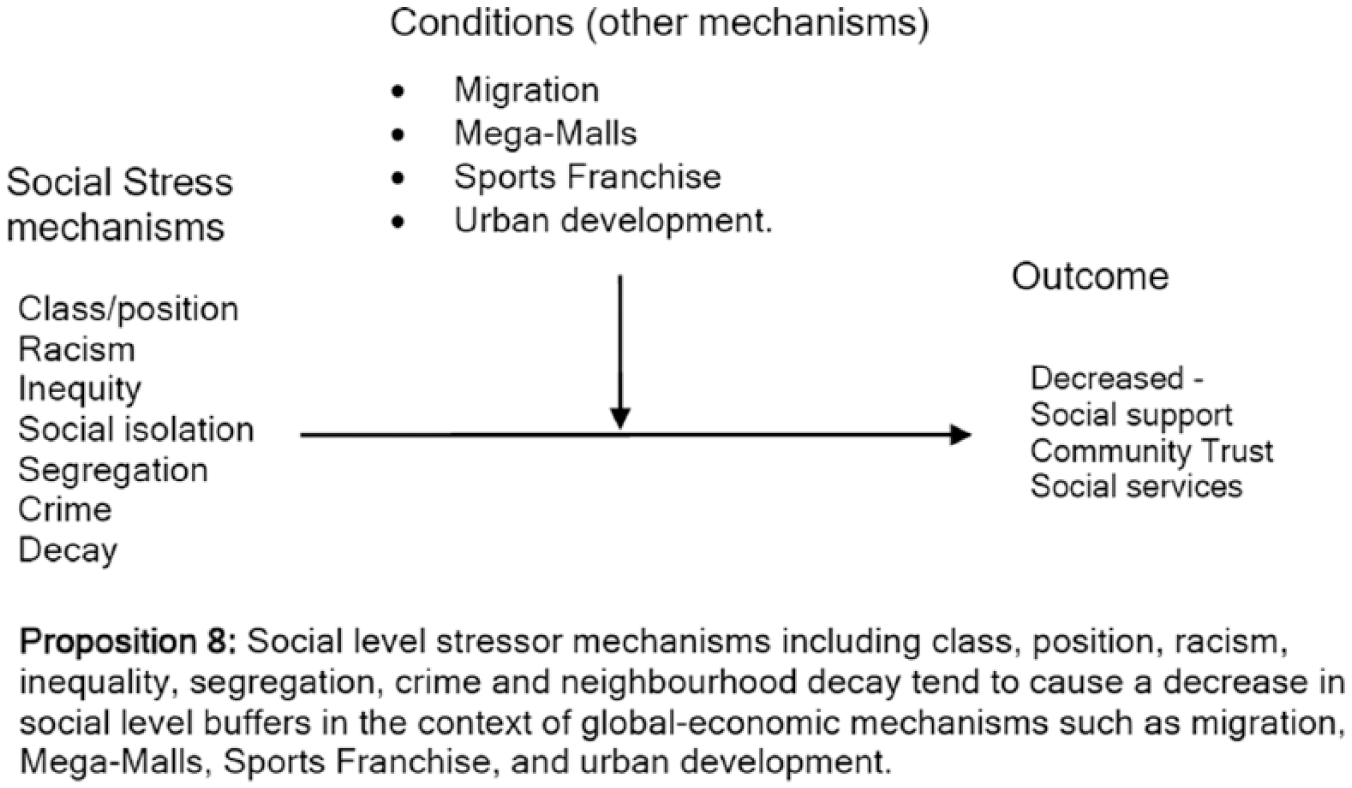
CMO model of social stress and buffers.
Based on the above eight realist propositions, a model of social isolation, stress, and depression is proposed (Figure 7).
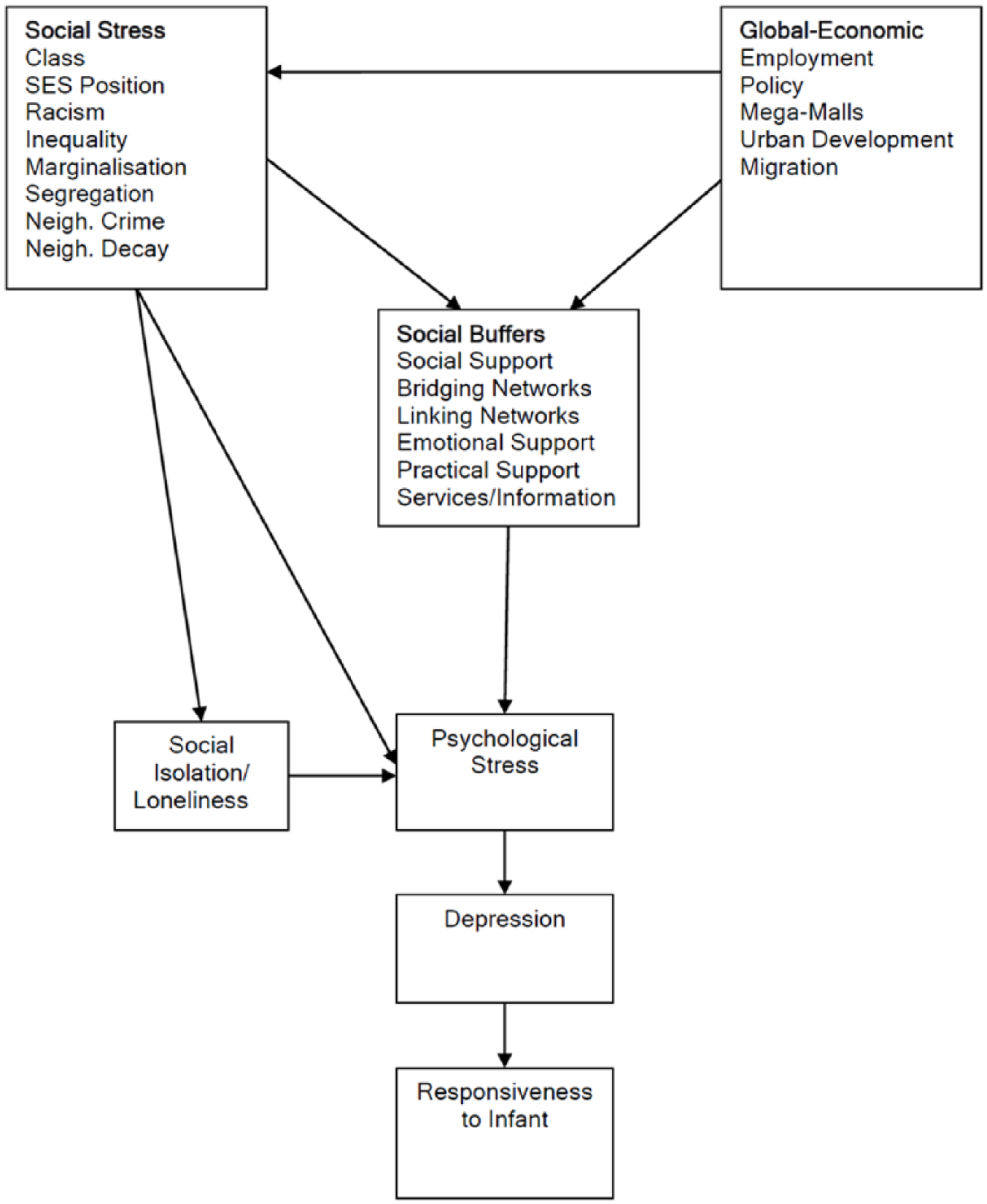
Model of social isolation, stress, and depression.
Cultural Mechanisms
Critical realists define culture as a distinct ontological level (Archer, 1995; B. Danermark & Gellerstedt, 2004). This is consistent with current multilevel cultural and cross-cultural psychological theory (Adamopoulos, 2008). Under this thesis, separate and different mechanisms operate at the cultural level from those at the social or psychological levels. Drawing on Beck’s (2002) concept analysis of postnatal depression, culturally defined expectations of motherhood may be shattered by the reality of a new mother’s lived experience. In keeping with cultivation theory and social expectation theory (McQuail, 1994), global media will play an important role in the “cultivating and acculturation” process, shaping all mothers’ beliefs and expectations of pregnancy, childbirth, and parenting to a selective view of reality.
The cultural differentialism paradigm of cultural theory (Ritzer, 2008) would hold that mothers’ deep cultural practices and expectations will remain largely unaffected by globalization and media. In juxtaposition, cultural hybridization will be occurring within local South West Sydney neighborhood settings producing new and distinctive cultural realities. Within these cultural fluxes, migrant mothers’ family and personal cultural expectations will generate stress. As observed by Beck (2002), these conflicting expectations and experiences of motherhood lead mothers “down the path to becoming overwhelmed, perceiving themselves as failures as mothers, and bearing a suffocating burden of guilt” (p. 470).
We have made the following three critical realist (CMO) propositions (Figures 8-10) based on the above theoretical position and the findings of our migrant multilevel study (Eastwood, Jalaludin, Kemp, Phung, & Barnett, 2013), and the three intensive studies of mothers’ experiences (Eastwood et al., 2016; Eastwood, Kemp, & Jalaludin, 2014; Eastwood et al., 2015).

CMO of migrant mechanisms.

CMO cultural mechanisms—Expectations of mothers.

CMO cultural mechanisms—Mothers’ expectations.
Global-Economic Mechanisms
As observed by Clark (2005), “Everything in the situation both constitutes and affects most everything else in the situation in some way . . . Here the macro/meso/micro distinctions dissolve in the presence/absence” (p. 72). Globalization theory (Ritzer, 2008), and conceptual frameworks of globalization and health (Galea, 2007; Labonte & Torgerson, 2005) describe the global and economic generative powers that will affect neighborhood context and the lived experiences of mothers and their families. In tension are two economic systems of globalization—transnational capitalism and socialist globalization—each with mechanisms capable of influencing migration, media, corporate business, social services, politics, and policy. Drawing on Labonte and Torgerson (2005), the global context will condition, at the policy level, macroeconomic, labor, food security, environmental protection, political power, public provision, and migration and refugee policies. Together, and separately from, the generative powers of corporate business, these policy-level mechanisms will shape urbanization, disparities, community capacity, and service access with resulting impacts on triggers, and conditioners, of maternal stress and depression.
Historical and Spatial Context
The spatiotemporal situation of people and resources affects the nature of social phenomena (Sayer, 2000). With global, policy, social, psychological, and biological processes occurring over time, the historical and life-course context will influence or condition the tendencies of causal mechanisms. Thus, individual histories will unfold inside the larger historical sweep of social (and cultural) evolution (Layder, 1993). Although time has a single dimension and is irreversible, space has three dimensions and movement is reversible. Drawing on Bourdieu (1977; cited by Sayer, 2000), structures, objects, mechanisms, and individuals can reversibly interact within space. Thus, individuals who compose a neighborhood influence that neighborhood and adjacent neighborhood context, which in turn has a reciprocal temporal and spatial impact on those and other individuals who reside or move through the neighborhood. Sayer (2000) argues that in some respects, space or geography is vital, but in others, as illustrated by the ability of things and people to remain the same in different settings, it makes only small differences. The implication of Sayer’s thesis is that spatial conditioning of maternal depression and stress will be in turn conditioned by generative properties of social, cultural, and historical context.
Based on the above realist propositions, a model of social isolation and “expectations lost” is proposed (Figure 11).

Model of social isolation and “expectations lost.”
Thesis
Drawing together the above analysis, we propose the following:
Thesis of Neighborhood Context, Stress, Depression, and Developmental Origins of Health and Disease
In the neighborhood spatial context, in keeping with critical realist ontology, global-economic, social, and cultural-level generative powers trigger and condition maternal, psychological, and biological-level stress mechanisms, resulting in the phenomenon of maternal depression and alteration of the infants’ developmental trajectory.
Conclusion
The purpose of this article was to present the thesis, theoretical framework, propositions, and models explaining neighborhood context, stress, depression, and the developmental origins of health and disease. The article utilized the empirical findings and theory generation of our previous publications.
Global, economic, social, and cultural mechanisms were identified that explain maternal stress and depression within family and neighborhood contexts. There is a complex intertwining of historical, spatial, cultural, material, and relational elements that contribute to the experiences of loss and nurturing. Emerging is the centrality of social isolation and “expectation lost” as possible triggers of stress and depression not only for mothers but possibly also for others who have their dreams shattered during life’s transitions (Figure 11). In these situations, social and cultural context can either nurture and support, or marginalize and isolate.
We will use the theories developed here for future confirmatory studies and realist program theory development.
Footnotes
Acknowledgements
The authors thank Anne Eastwood for her assistance with the qualitative research, and Hai Phung and the Child and Family Health nurses of the previous South Western Sydney Area Health Service (SWSAHS) for their efforts in the collection and maintenance of the IBIS database.
Authors’ Note
The research discussed in this article was originally presented at the 17th International Conference on Integrated Care, Dublin, May 8-10, 2017, an abstract of which was published in the International Journal of Integrated Care.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.