
Abstract
An in-depth understanding of psychological symptoms and mindfulness of men and women with percutaneous coronary intervention (PCI) may help develop sex-specific treatments and outcomes. This study aimed to examine differences in depression, anxiety, stress, and mindfulness between men and women undergoing PCI using a convenience sample of 114 participants (81 men and 33 women) with PCI at a university hospital in 2013. The Depression Anxiety Stress Scales and the Korean version of the Mindfulness Attention Awareness Scale were administered. The depression, anxiety, and stress scores of women were higher than those of men, with no significant differences in mindfulness between the two sexes. The comparison of cutoff scores for severity (normal scores vs. ≥ mild) of depression, anxiety, and stress for men versus women revealed a higher proportion of women in the ≥ mild categories for the three components. Women who received PCI showed greater psychological distress than men. Therefore, awareness of these differences may alert cardiovascular nurses to employ systematic vigilance in assessing and mitigating this distress among cardiac patients, particularly women.
Introduction
Heart disease is the leading cause of death in the US and South Korea, despite the COVID-19 pandemic onset in 2020 (Statistics Korea, 2021; Wadhera et al., 2021). The ratio of death rates in women to men is 1.02 (Statistics Korea, 2021). Moreover, death rates among women are higher than that among men. Compared with men, women are less likely to be treated aggressively for cardiovascular disease (CVD) or less evidence-based treatment. Furthermore, women have unique CVD risk factors and markers (Agarwala et al., 2020; Mauvais-Jarvis et al., 2020). Specifically, biological factors, environmental exposure, and social processes affect sex differences (Bucciarelli et al., 2020). Moreover, differences in sex-related hormones may differentially contribute to anxiety and depression states and the development of CVD (Mahdavian & Abbassian, 2014).
Depression and anxiety are related to coronary artery disease (CAD) and are common in patients with CAD (Celano et al., 2015; Olsen et al., 2018). Depression is associated with a 77% increased risk of all-cause mortality 10 years after PCI (van Dijk et al., 2016). A meta-analysis of unadjusted data showed that depression and anxiety were associated with an increased risk of mortality; however, when adjusting for covariates, the associations were not significant (Celano et al., 2015; Lichtman et al., 2014). The association of anxiety and depression to mortality is likely mediated by other factors such as sex. Indeed, being female is significantly related to anxiety (Oslen et al., 2018), and depression is more prevalent among women than men (World Health Organization, 2017).
Stress is associated with depression and anxiety development, and may also be viewed as a risk factor for CVD (Bangasser, 2013; Seixas et al., 2018). Menand women tend to react differently to stress (Verma et al., 2011) because stress-related receptors of stress hormones shift women more easily into a dysregulated state of stress reactivity following stressful events (Bangasser, 2013). Importantly, when treating patients with PCI, it is essential to understand the differences in stress levels experienced by men and women. Of the 310 participants with stable CAD, the stress in women was higher than in men (Samad et al., 2014). In Eastern cultures, stress is regarded as an inner peace absence, whereas in Western cultures, stress is viewed as a loss of control (Verma et al., 2011). Practices such as meditation may reduce stress, promote mindfulness and inner peace, and mitigate negative emotions.
Mindfulness is purposely paying close attention (in the present and nonjudgmentally) to unfold experiences from one moment to the next (Kabat-Zinn, 2003). Mindfulness can increase self-regulation by enhancing attention control, emotion regulation, and self-awareness, which may affect CVD risk factors (Loucks, Schuman-Olivier, et al., 2015). The mind is trained to act as a meditation tool, a process known as mindfulness meditation (mindfulness-based stress reduction [MBSR]). This may increase parasympathetic activity with a reduction in sympathetic vascular tone and stress hormones; further, it has been found to reduce depression, anxiety, and stress in patients with CVD (Loucks, Schuman-Olivier, et al., 2015). Although mindfulness is important in CVD and cardiac rehabilitation, little is known about mindfulness in men and women undergoing PCI.
Depression, anxiety, stress, and mindfulness linked psychological factors were higher in women than in men. Samad et al. (2014) recommended further study about the association of sex differences in CVD in response to mental stress and outcomes. A mindfulness intervention such as MBSR reduced depression, anxiety, and stress levels in patients with CAD (Marino et al., 2021; Nasiri et al., 2020; Zou et al., 2021). Hypotheses are that depression, anxiety, and stress are higher in women than in men, and mindfulness is associated with depression, anxiety, and stress. Therefore, this study aimed to examine the potential differences in depression, anxiety, stress, and mindfulness. Furthermore, the correlations with these four variables were also examined between men and women.
Methods
Design and Participants
This cross-sectional comparative design study explored anxiety, stress, depression, and mindfulness by sex in patients within a month following PCI.
Participants who had undergone PCI at a university hospital in South Korea were recruited and enrolled. Furthermore, the participants completed study measures as part of a study to investigate the effects of cardiac rehabilitation. The eligibility criteria were as follows: age ≥20 years, had undergone PCI at a university hospital setting a month prior to the study, was ambulatory or physically independent, and had no diagnosed psychiatric conditions. The sample size was calculated by the G*power 3.1 program (Faul et al., 2007), and the required sample size was 109 for detecting a medium effect (d = 0.30), 90% power, and a significance level of .05. A total of 114 participants voluntarily agreed to participate in the study and were included in the analysis. The mean (SD) ages of the participants were 63.5 (7.7) years, their ages ranged from 43 to 78 years, and most participants were men (71.1%).
Data Collection
Self-report questionnaires, including the Depression Anxiety and Stress Scales (DASS-21) and the Korean version of the Mindfulness Attention Awareness Scale (MAAS) were administered.
DASS-21
The DASS-21 evaluates depression, anxiety, and stress levels (Lovibond & Lovibond, 1995). It comprises 21 questions based on a Likert-type scale (0 [not at all] to 3 [most of the time]) and three subscales: depression, anxiety, and stress. Scores for depression, anxiety, and stress are summed for the relevant items and then multiplied by two to calculate the final score, which is equivalent to the full version of the DASS-21. The total scores of each scale range from 0ã 42. The recommended cutoff scores for conventional severity were: depression (normal = 0–9, mild = 10–13, moderate = 14–20, severe = 21–27, and extremely severe = 28); anxiety(normal = 0–7, mild = 8–9, moderate = 10–14, severe = 15–19, and extremely severe ≥20); and stress(normal = 0–14, mild = 15–18, moderate = 19–25, severe = 26–33, and extremely severe ≥34). The cutoff scores for depression, anxiety, and stress severity were divided between normal and ≥ mild in this study. Cronbach’s è for depression, anxiety, and stress in patients with CVD were .90, .82, and .81, respectively (Komasi et al., 2018; Oxlad et al., 2006), whereas in this study, they were .76, .73, and .81, respectively.
MAAS
The MAAS, developed by Park (2006), is used to measure mindfulness and is a Korean version. The MAAS consists of 20 items based on a 5-point Likert-type scale (from 1 [not at all] to 5 [almost always]) and four subscales: present awareness, concentration, nonjudgmental acceptance, and decentered attention. Each subscale contains five items. All items represent levels of mindfulness. Furthermore, participants are asked to rate their level of agreement with the content presented. The possible total score ranges from 20 to 100, and higher scores indicate a higher level of mindfulness. Cronbach’s è for the MAAS at the time of development was .72 (Park, 2006) and .94 in this study.
Ethical Considerations
Ethical approval was obtained from the hospital’s Ethics Committee and was conducted according to the Declaration of Helsinki. All patients provided informed consent before their study inclusion, indicating that they had participated voluntarily and were free to withdraw at any point in the study without penalty. Participant identifiers were not used, and recorded data on paper forms were kept in a private space during the study.
Data Analysis
The IBM SPSS Statistics 23 software was used to analyze the data. The values of the dependent variables of depression, anxiety, and stress were not normally distributed. Moreover, a nonparametric test of the Mann–Whitney U test was conducted to compare dependent variables between men and women. The Chi-square test was used to compare standard cutoff values for severity (≥ mild vs. normal scores) of depression, anxiety, and stress in patients with PCI. Spearman’s correlation test examined the relationship between depression, anxiety, stress, and mindfulness.
Results
The mean scores for depression, anxiety, and stress in men were 7.80, 8.89, and 11.75, respectively. In contrast, mean scores for depression, anxiety, and stress in women were 11.52, 11.52, and 15.15, respectively. Women had significantly higher DASS scores than men (U = 889, p = .005; U = 1013, p = .042; U = 977.5, p = .024). The mean score for mindfulness was 83.68 (84.85 in men and 80.82 in women). Moreover, there were no significant differences between men and women regarding mindfulness (Table 1).
Sex Differences in Anxiety, Stress, Depression, and Mindfulness Scores (N = 114).

Table 2 shows the comparison of cutoff scores for severity (normal scores vs. ≥ mild) of anxiety, stress, and depression. The severity of depression and stress in women was statistically significantly higher than in men (χ2 = 9.29, p = .002; χ2 = 4.19, p = .041, respectively); however, anxiety had no significant differences between the two groups.
Sex Differences in Cut-Off Scores for Severity (Normal and ≥ Mild) of Anxiety, Stress, and Depression (N = 114).

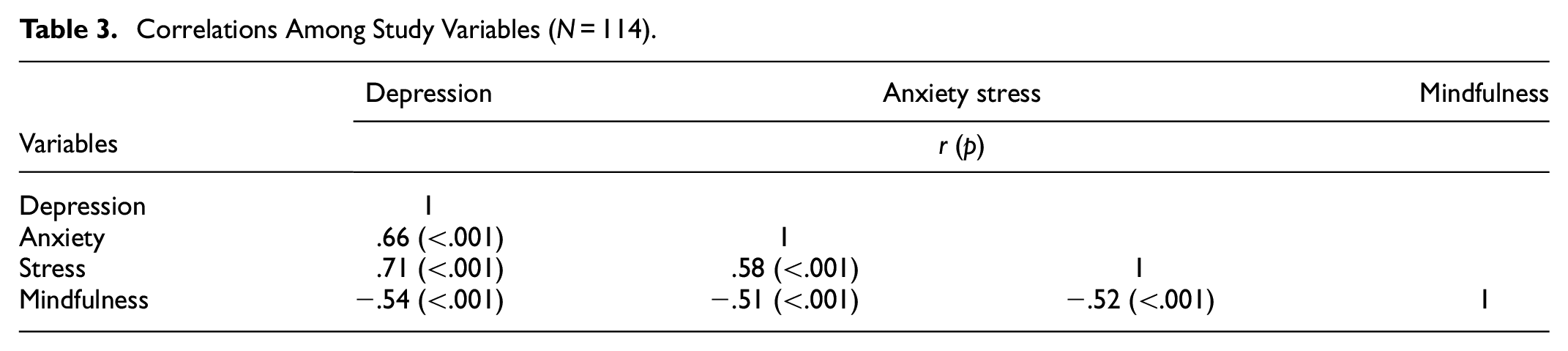
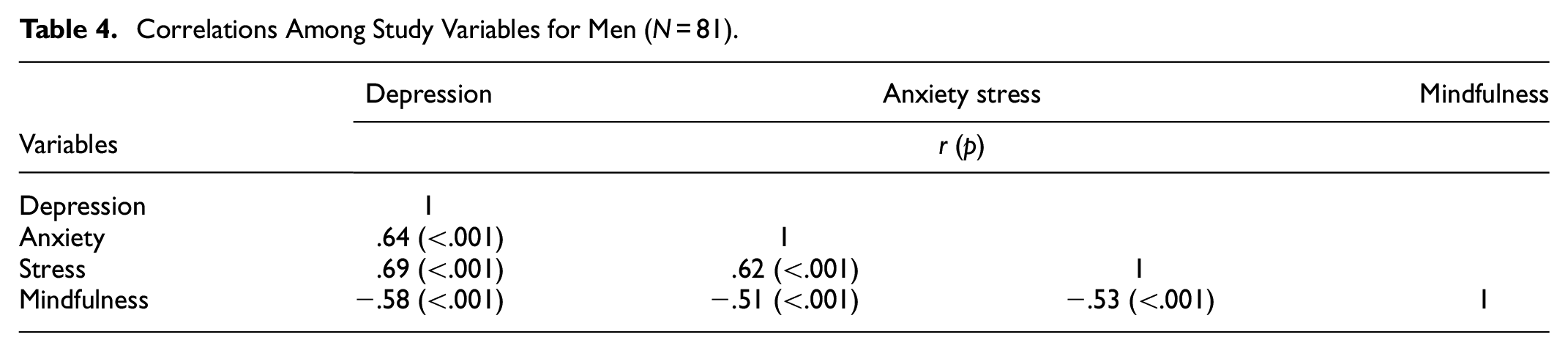
The correlations between depression, anxiety, stress, and mindfulness are outlined in Table 3. There were significant positive correlations between depression and anxiety (r = .66, p < .001) and stress (r = .71, p < .001). In addition, the association between anxiety and stress was statistically significant (r = .58, p < .001). Mindfulness had significantly negative correlations with depression, anxiety, and stress (r = −.54, p < .001; r = −.051, p < .001, r = −.052, p < .001). For men and women, the same pattern as the total correlations was observed (Tables 4 and 5).
Correlations Among Study Variables (N = 114).
Correlations Among Study Variables for Men (N = 81).
Correlations Among Study Variables for Women (N = 33).

Discussion
In our study, the mean scores of women were higher than those of men. Furthermore, the mean scores were all above mild levels of DASS, particularly anxiety (≥ moderate). There is information paucity on DASS levels by sex among patients with CVD, and it is difficult to compare previous studies with this study directly. Regarding depression, we found that the mean scores in women were higher than in men, and the severity of depression among women was significantly different than among men. It may be possible that inflammation contributed to the atherosclerosis development in patients with CAD (Yayan, 2013). Sex differences in depression and socioemotional responses to an inflammatory challenge showed that women were twice as likely as men to develop depression in inflammatory activity, which suggests that women are more sensitive to the affective consequences of inflammation (Moieni et al., 2015). Inflammation may contribute to depression; however, the depressogenic effect of inflammatory activation varies depending on the vulnerability level (Raison & Miller, 2011). Therefore, anti-inflammatory interventions can help decrease depression in women with PCI.
In this study, anxiety level in women (11.52) was higher than in men (8.89); however, differences in anxiety severity of men and women (i.e., those having ≥ mild anxiety) were not significant (60.6% vs.44.4%, respectively). Being female was associated with a higher anxiety risk in patients with PCI for CAD (Olsen et al., 2018; Sreckovic et al., 2017). Moreover, anxiety was strongly associated with various inflammation and coagulation markers, including in the pathogenesis of CVD (Pitsavos et al., 2006). Therefore, patients with PCI are recommended to attend cardiac rehabilitation programs to prevent restenosis. Women were less likely to be referred to cardiac rehabilitation than men (Liet al., 2018). Moreover, compared with men, women were less likely to receive physical activity recommendations (Li et al., 2018). Physical activity is an overly critical predictor of anxiety, and exercise is essential in cardiac rehabilitation (Bener et al., 2016; Kaur et al., 2013). Self-efficacy is a predictor of anxiety in patients with congenital heart disease, and women had significantly lower self-efficacy scores than men (Thomet et al., 2018). Thus, strategies promoting self-efficacy woven into cardiac rehabilitation programs are recommended to increase the participation rate for women.
Regarding stress, we found that the mean scores in women were higher than those in men, and differences in stress severity in men and women (i.e., those having ≥ mild stress) were statistically significant (51.9% vs. 72.7%, respectively). Stress is a risk factor for CVD and may lead to depression and anxiety (Sommaruga et al., 2018). Women with CAD reported more stressful life events during the year after discharge than men with CAD. Moreover, high-intensity evidence-based psychological interventions (e.g., stress management or mindfulness) were recommended (Sommaruga et al., 2018). Additionally, women who participated in a psychosocial intervention had a mortality rate of 7% versus 20% for usual care. Women’s stress was reduced more than men’s because of participation in cognitive behavioral therapy (Orth-Gomér, 2012; Orth-Gomér et al., 2009). Stress was significantly associated with being female (Kaur et al., 2013). As part of their discharge plan, patients with PCI, especially women, should have their stress screened and be provided with cardiac rehabilitation or psychological or psychotherapeutic intervention for stress reduction.
In this study, although women’s scores were lower than those of men, there were no significant differences between men and women regarding mindfulness. Findings from the very limited previous studies using the same instruments and study variables cannot be compared to those of the present study. Moreover, patients with CAD may differ among studies. In 43 Korean patients on hemodialysis, mindfulness scores ranged from 69.11–78.21 (Cho, 2015), which were lower than those of patients with CAD in this study. The examination of mindfulness in women was particularly important for the mindfulness association with cardiovascular health. Specifically, higher mindfulness in women has been linked to better cardiovascular health (Loucks, Britton, et al.,2015). Mindfulness is the psychological process of one’s attention, moment by moment (Kabat-Zinn, 2003; Priya & Kalra, 2018). The practice of mindfulness increases parasympathetic activity and reduces sympathetic vascular tone, stress hormones, and inflammatory markers (Pascoe et al., 2017; Priya & Kalra, 2018). Thus, practicing mindfulness reduces physiological markers of stress (e.g., cortisol, C-reactive protein, and heart rate), decreases depression and anxiety, and increases mindfulness in patients with CAD (O’Doherty et al., 2015). Higher levels of mindfulness in both men and women in our study may be evidence that practicing mindfulness reduces stress and depression. Therefore, programs such as the MBSR can help increase mindfulness.
This investigation found that the correlations between depression, anxiety, stress, and mindfulness were significant in total numbers and were similar in men and women. There is a dearth of information on correlations between depression, anxiety, stress, and mindfulness for patients with CVD. Furthermore, it is difficult to directly compare previous studies with this study. Prior studies, despite different participants, showed that greater mindfulness was associated with lower anxiety in 70 patients with heart failure (Rechenberg et al., 2020), significant negative illness-related parenting stress in congenital heart disease (Bishop et al., 2020), and significant negative depression in 120 nursing students (Song, 2017). These were consistent with the results of this study. High levels of mindfulness predicted lower stress scores (Ede et al., 2020); therefore, strategies must be developed to increase mindfulness in men and women with PCI. MBSR affected depression, anxiety, and stress levels (Lee et al., 2017). Hence, the dramatic interest in stress management in cardiac rehabilitation (Chauvet-Gelinier & Bonin, 2017), such as MBSR, should be applied to men and women undergoing PCI.
Limitations and Recommendations for Future Research
The limitations of this study should be considered when interpreting its results. The hospital where we recruited participants is a major PCI center in South Korea; however, we recruited a small sample of women (n = 33). Therefore, the results may not be generalizable to all patients with PCI and should be considered with precaution. In this study, we did not have a normal distribution of DASS and mindfulness scores from our data, and nonparametric tests were used. Further studies should recruit a large sample from several institutions. We did not consider variables such as comorbidity, education, and employment status affecting depression, anxiety, and stress. Furthermore, additional research is needed to investigate how mindfulness affects men and women using qualitative studies and the predictors, moderators, or mediators of mindfulness in patients with PCI. In addition, as correlations of the four variables showed significant differences, mindfulness interventions such as MBSR would be applied to men and women. Moreover, the effect on psychological variables should be measured.
Conclusion
Higher depression, anxiety, and stress symptom scores and more frequent profiles of relatively worse symptom severity for women compared with men surrounding PCI are troubling. Depression, anxiety, stress, and mindfulness were significantly correlated. Continued attention to the psychological status of those patients with PCI is needed, including screening and intervention. Since men and women differ in terms of hormones, physiology, environment, and culture, cardiovascular nurses and nurse practitioners should understand the potential differences. These differences may be present in the incidence and degree of depression, anxiety, and stress. Thus, differing interventions for men and women or patients with varying severity are warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Statement
IRB No: AMC IRB No., 2012-0738