
Abstract
Despite the existence of several policies and programs, anemia among pregnant and lactating women continues to be a serious concern for public health policy in India. The main objective of this study is to examine the prevalence and determinants of anemia among pregnant and lactating versus nonpregnant nonlactating (NP-NL) women for priority setting in health policies of the country. Data from the National Family Health Survey (NFHS3) conducted in 2005-2006 has been used for the analyses of this study. The results revealed that the prevalence of anemia was higher among lactating women (63%), followed by pregnant women (59%) than NP-NL women (53%). Younger lactating (71%) and older pregnant women (67%) had a higher burden of anemia. Along with socioeconomic factors, demographic indicators such as children ever born and program factors like nutrition advice and supplementary nutrition during anti natal care and postnatal care emerged as significant predictors in the case of anemia among both pregnant and lactating women, while socioeconomic indicators emerged as critical factors in the case of anemia among NP-NL women. Hence, targeting demographic and program factors, along with key socioeconomic and demographic factors in public health policy, is critical in reducing anemia among lactating and pregnant women, while targeting significant socioeconomic factors is the key for reducing anemia among NP-NL women.
Background and Introduction
The World Health Organization (WHO) defines anemia as “a condition in which the number of red blood cells or their oxygen-carrying capacity is insufficient to meet the physiological needs” (WHO, 2011). Anemia is one of the most common and widespread nutritional deficiency disorders in the world. WHO global database on anemia for 1995-2011 estimated a global prevalence of anemia among the women of reproductive age at 29.4%, affecting over 528.7 million women (Stevens et al., 2013; WHO, 2011). Despite a significant decrease in the prevalence of anemia among pregnant women (43% to 38%) and nonpregnant women (33% to 29%) during the 1995-2011, anemia was a leading cause of 68.4 million years lost with disability (YLD) among women (Ezzati, Lopus, Dogers, Vander, & Murray, 2002; Kassebaum et al., 2014; Stevens et al., 2013; WHO, 2011). It causes adverse consequences on maternal and child health outcomes such as low birth weight, neonatal and maternal mortality (Agarwal et al. 2006; Balarajan, Ramakrishnan, Ozaltin, Shankar, & Subramanian, 2011; Goli & Arokiasamy, 2014; Singh, Goli, & Parsuraman, 2014; Goli, Doshi & Arokiasamy, 2013; Kalaivani, 2009; Kassebaum et al., 2014; Kozuki, Lee, & Katz, 2012; McLean, Cogswell, Egli, Wojdyla, & de Benoist, 2009; Sharma, Patnaik, Garg, & Ramachandran, 2008; Steer, 2000; Toteja et al., 2006; Vijayalakshmi & Mercy, 1994).
However, the burden of anemia is not uniformly distributed across regions or countries in the world. Within the pregnant and lactating women, the anemia prevalence gap between developed and developing countries is large. For instance, it is only 14% in developed countries, while it is much higher in developing countries (51%). Among the developing regions, it is highest in Central and West Africa (56% among pregnant and 48% among nonpregnant) followed by South Asia (52% among pregnant and 47% among nonpregnant; Balarajan et al., 2011; McLean et al., 2009; Stevens et al., 2013; WHO, 2015; WHO, 2011; Rana & Goli, 2016). Also, maternal deaths due to anemia were also reported to be highest in developing countries (Balarajan et al., 2011; McLean et al., 2009; WHO, 2008, 2011). In particularly in countries like India, it is as high as 60% to 70% in 2005-2006 (Kalaivani, 2009; McLean et al., 2009; Toteja et al., 2006).
The prevalence of anemia also varies considerably by population characteristics like age, sex, socioeconomic status and biodemographic factors like pregnancy and lactation (Bentley & Griffiths, 2003; Florentino, 2003; Haidar, 2010; McLean et al., 2009; Sharma et al., 2008; Vijayalakshmi & Mercy, 1994; Wadgave, 2011). Women in the reproductive age group are more vulnerable to iron deficiency resulting in anemia, especially during pregnancy and lactation as they are physiologically and nutritionally at a higher risk (Brooker, Hotez, & Bundy, 2008; Elzahrani, 2012; Picciano, 2003). Similarly, a lactating mother requires highly nutritious food to accumulate calories for the production of adequate quantity of milk without deteriorating her health (Picciano, 2003; Raman, Primala, Bhalla, Venkateshwar, & Iyengar, 2001). Yet women in developing countries often fail to consume additional food and supplements required to meet the demands during pregnancy and lactation because of fetal growth, alterations in maternal tissues, metabolism, and breast feeding (Aikawa, Khan, Sasaki, & Binns, 2006; Baig-Ansari et al., 2008; Kotecha, Nirupam, & Karkar, 2009).
Inspite of significance of the problem, anemia among pregnant and lactating women has not received the requisite attention from public health policy in developing countries. In India, the previous study on the prevalence and complications of anemia in pregnancy was in 1998-1999 using large-scale National Family Health Survey (NFHS). This study highlights the maternal anemia contribution to an intergenerational cycle of poor growth of the foetus and low birth weight (Kalaivani, 2009). The focus of other recent studies on this subject was restricted to either small-scale field or hospital-based surveys with limited geographical coverage (Lokare, Karanjekar, Gattani, & Kulkarni, 2012; Sharma et al., 2008; Vivek et al., 2012). In this study, we aim to determine the prevalence of anemia levels and factors associated with it among pregnant and lactating women vis-à-vis NP-NL women in India, a setting where a substantial proportion of the population suffers from food insecurity and a poor social security mechanism (Siddiqui, Goli, Reja, & Shruti, 2017). In particular, through a comparative assessment of levels and factors associated with anemia among pregnant and lactating women vis-à-vis NP-NL women, we have investigated two objectives: first, to highlight the level of physiological disadvantage of pregnant and lactating women compared with NP-NL women in India; second, to identify the factors affecting anemia among pregnant and lactating women vis-à-vis NP-NL women to prioritise specific targets in the policy for these categories of women.
Data and Methods
Data Source and Study Population
We used data from the NFHS3 conducted in 2005-2006 by the International Institute for Population Sciences (IIPS), Mumbai, under the stewardship of the Ministry of Health and Family Welfare (MoHFW), Government of India. The NFHS-3 survey was conducted in 20052006 as part of the global Demographic Health Survey (DHS). It was a nationwide representative sample survey of 109,041 households, 124,385 women in the age group 15-49 years. Including the information on fertility, mortality, morbidity, and maternal and child health, this is the only major survey in India that has collected a comprehensive nutrition data with representative samples from all the 29 states of India, covering more than 99% of the national population. The samples of pregnant (n = 5,911), lactating (n = 21,973) and NP-NL (n = 97,418) women are adequate to carry out the robust statistical analysis.
Outcome Variable
The outcome variable in the study is the presence of any anemia (yes = 1/no = 0). The NFHS used HemoCue blood test to estimate the hemoglobin level in grams per deciliter blood. The anemia status of the surveyed women was classified into severe, moderate, mild, and any anemia based on WHO guidelines (WHO, 2011). Severe anemia level was defined as hemoglobin <7.0 g/dL for both pregnant and lactating women, and <8.0 g/dL among NP-NL women. Moderate anemia was defined as 7.0 to 9.9 g/dL for pregnant and lactating women, and 8.0 to 10.9 g/dL among NP-NL women. Mild anemia was defined as 10.0 to 10.9 g/dL in pregnant and lactating women, and 11.0 to 11.9 g/dL in NP-NL women. Any anemia was defined as the hemoglobin level below 11.0 g/dL in pregnant and lactating women, whereas <12.0 g/dL in NP-NL women.
Predictor Variables
Based on an extensive review of existing literature (Kalaivani, 2009; Lokare, Karanjekar, Gattani, & Kulkarni, 2012; McLean et al., 2009; Sharma et al., 2008; Toteja et al., 2006; Vivek et al., 2012), we considered socioeconomic and demographic factors such as duration of pregnancy (<3/3 to 6/>6 months), age (15-24/25-34/35+ years), total children ever born (no child/one to two/more than two), place of residence (rural/urban), religion (hindu/muslims/others), caste (sc/st/obc/others), education (no education/primary/secondary&above), mass media exposure (no/any), partner’s education (no education/primary/secondary&above), and wealth quintile (poorest/poorer/middle/richer/richest) as demand-side predictors of anemia and pregnancy registration with ANM (Auxiliary Nurse Midwife; yes/no), recieved nutrition advice at least once (yes/no) and receipt of any supplementary nutrition (yes/no) as supply-side predictors of anemia.
Statistical Analyses
Bivariate analyses were carried out to assess the level of anemia among pregnant, lactating, and NP-NL women by socioeconomic and demographic characteristics of women by applying appropriate sampling weights. Chi-square test was used to test the statistical significance of bivariate differences in anemia prevalence across the socioeconomic and demographic characteristics. Furthermore, binary logistic regression models were used to assess the net effects of several confounding factors associated with the occurrence of anemia among pregnant and lactating vis-à-vis NP-NL women. Alpha level was set at 0.05 to determine the statistical significance of variation in the prevalence of any anemia estimated as an adjusted odds ratio with 95% confidence interval across the categories of the predictor variables. All analyses of this study were carried out using STATA 13.
Results
Sample Distribution of Study Population
Table 1 presents the distribution of women by outcome and predictor variables. Out of the total sample of currently married women in the age group 15 to 49 years, around 4% were pregnant while 18% lactating and 78% were NP-NL at the time of the survey. The distribution of women by socioeconomic and demographic profile shows that the majority of women in all three samples were Hindus (81% pregnant, 83% lactating, 86% NP-NL), belonged to the age group of 25 to 34 years (66%), and lived in rural areas (76%). By social group, the results revealed that 40% to 41% of total women in pregnant, lactating, and NP-NL categories belonged to other backward class. Furthermore, the results also show that 46% of total pregnant women had no education, while this figure was 51% and 38% for lactating and NP-NL women, respectively. Around half of pregnant and lactating women had exposure to any form of mass media. The occupation-wise stratification suggested that 23% of the pregnant women, 28% of lactating women, and 39% of NP-NL women were employed at the time of the survey. In terms of health care seeking and nutrition, 43% of pregnant women had registered their pregnancy with ANM, 58% had taken nutrition advice at least once from either doctor or ANM, but only 17% had received supplementary nutrition from the Anganwadi centers.
Percentage of Pregnant, Lactating, and Nonpregnant- Nonlactating Women According to Their Selected Background Characteristics, India, 2005-2006.

Prevalence of Anemia and Its Predictors
Figure 1 illustrates the prevalence of any anemia (in percentage) by age. Older pregnant women have a higher burden of anemia than younger ones. The prevalence of anemia among lactating women peaked at the age of 16 to 18 years (75%) and then showed a decreasing trend up to the age of 20 to 22 years (59%), followed by a steady increase. The prevalence of anemia among these women peaked after age 38 years (70%). Lactating women showed a higher burden of anemia at younger ages, while the prevalence of anemia was steady and varying between 50% and 55% throughout the reproductive span among NP-NL women. Furthermore, on grouping the age into broad categories, the results revealed that older pregnant women (aged >35 years) had a greater prevalence of moderate and severe anemia than middle age or younger women. Lactating women of younger ages (15-24) were found to have a higher burden of mild (48%) and moderate (21%) anemia. Thus, the prevalence of anemia gradually increased with the increase in duration of pregnancy among pregnant and lactating women. It was found to be higher among women in the third trimester of gestation.
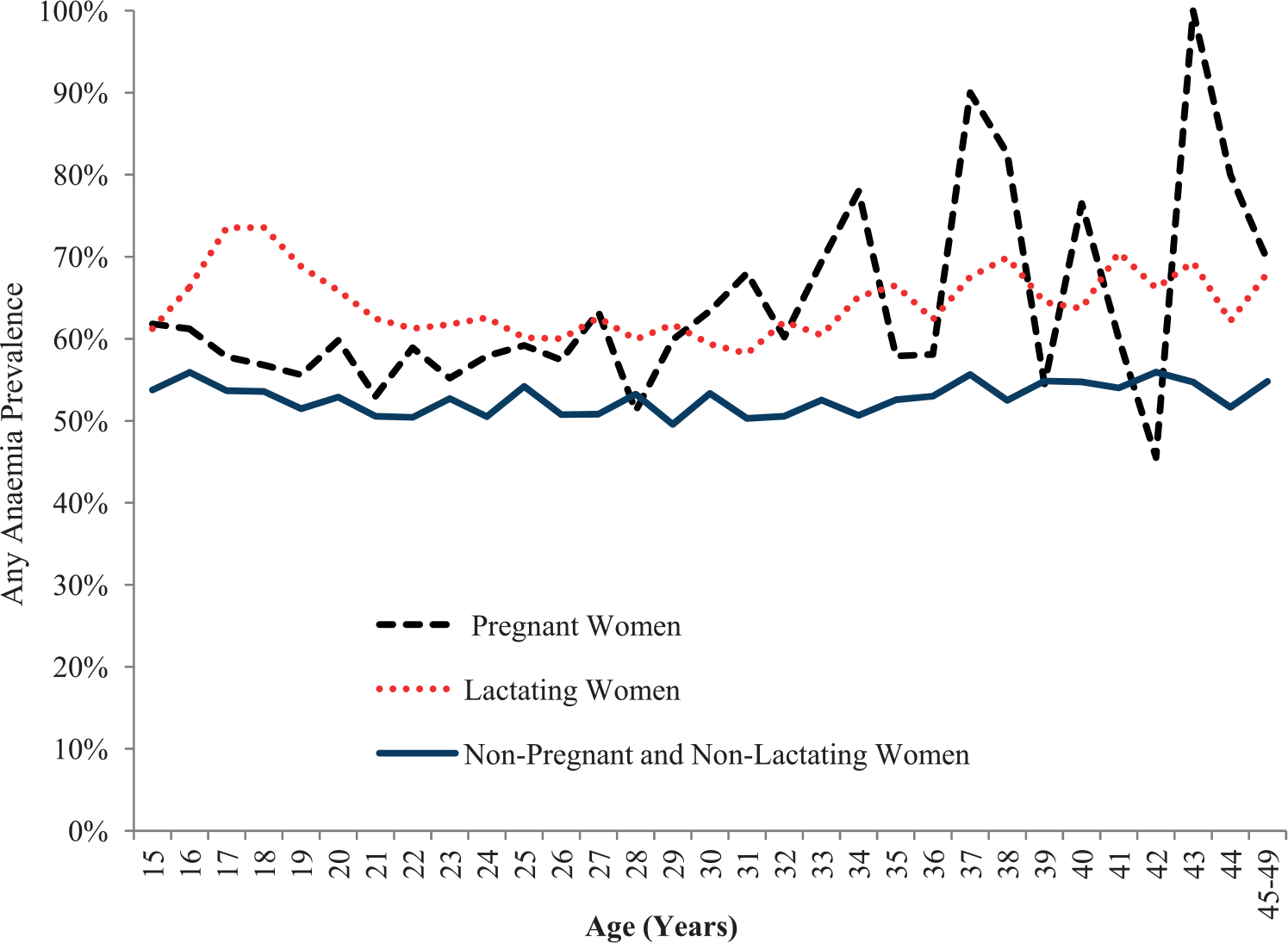
Prevalence of any anemia among pregnant, lactating, and nonpregnant- nonlactating women in India by age in single years, 2005-2006.
The overall distribution of women in different categories by anemia levels showed that pregnant women had a higher prevalence of severe anemia (2.2%) compared with lactating (1.7%) and NP-NL (1.8%). However, the prevalence of any anemia was higher in lactating women (62.9%) than pregnant (58.7%) and NP-NL women (37.8). Across all the categories (pregnant, lactating, and NP-NL women), the rural–urban differences in the prevalence of anemia persist. However, the rural–urban difference in the prevalence of severe anemia was more pronounced in pregnant women (0.7%) than lactating (0.1%) and NP-NL women (0.4%). Women belonging to scheduled caste and scheduled tribe had a significantly higher burden of anemia than other backward classes and Others in all three types of anemia measures. In the case of severe anemia, the caste differences in anemia risk among pregnant women were much greater than lactating and NP-NL women. Differences in the prevalence of any anemia were also observed among different educational subgroups across pregnant, lactating, and NP-NL women. These differences were observed to be higher among pregnant women (2.3%) than lactating (1%) and NP-NL women (0.5%). Likewise, the same pattern was found regarding partner’s education. Furthermore, the proportion of women in all categories who were exposed to mass media had a lower burden of any anemia than those who did not have any exposure. However, these differences were much higher in the case of severe anemia among pregnant women than lactating and NP-NL women.
Differences in prevalence of anemia by employment status were observed across all three categories of women. However, the volume of difference was not uniform across the three groups of women. For instance, a higher percentage of anemia was found among pregnant and lactating women than NP-NL women in currently employed category. Among those suffering from severe anemia, the educational differences were greater in pregnant women compared with lactating and NP-NL women. Although the rich–poor gap in the prevalence of anemia was substantial across the women in all the categories, it was quite substantial in pregnant and lactating women than NP-NL women.
Furthermore, the results on the prevalence of anemia by supply-side factors showed that women who registered their pregnancy with ANM had better hemoglobin levels than their counterparts, although the differences were not significant. However, women who had taken nutrition advice and supplementary nutrition from ANM had lower hemoglobin levels compared with their counterparts (Table 2).
Prevalence of Anemia Level Among Pregnant, Lactating, and Nonpregnant- Nonlactating Women by Background Characteristics in India, 2005-2006.

p < .10. **p < .05. ***p < .01.
Adjusted Odds Ratio of Anemia Prevalence and Its Determinants
Table 3 presents the results of logistic regression analysis of anemia prevalence among pregnant, lactating, and NP-NL women while controlling for background characteristics. The adjusted odds of anemia prevalence was found to be higher among multigravida pregnant women (odds ratio [OR] = 1.4, p < .01) than in primigravida pregnant women (OR = 1). The odds of women having anemia were higher among pregnant women who were employed (OR = 1.33, p < .01) compared with their unemployed counterparts (OR = 1). However, with reference to the women whose husbands were not educated, pregnant and lactating women with educated partners were less likely to be anemic. The possibility of having anemia was less among pregnant women in the richest households (OR = 0.65, p < .05), richer households (OR = 0.70, p < .05), and poorer households (OR = 0.75, p < .05) compared with poorest households (OR = 1). Furthermore, the results revealed that women who registered their pregnancy with ANM were less likely to be anemic. Likewise, the results also show that pregnant (OR = 1.26, p < .05) and lactating (OR = 1.40, p < .05) women who took nutrition advice at least once during their pregnancy were more likely to be anemic compared with those women who took no advice during their pregnancy (OR = 1). Similarly, the results also showed that pregnant women who had received any supplementary nutrition from Anganwadi were more likely to be anemic (OR = 1.25, p < .05) compared with those women who had not received any other supplementary nutrition during pregnancy (OR = 1).
Logistic Regression Estimates: Factors Associated With Anemia Among Pregnant, Lactating, and Nonpregnant-Nonlactating Women in India, 2005-2006.

Reference category.
p < .10. **p < .05. ***p < .01.
Discussion and Conclusion
Despite the fact that India was the first developing country to implement a national program to prevent anemia with notable attention to control anemia during pregnancy and lactation, the severity of the problem remains. Anemia is still a major public health issue of greater magnitude for the country. The recently published fact sheets based on NFHS-4 information from IIPS and MoHFW (2017) suggest that, despite the rigorous efforts of government to reduce the prevalence of anemia in terms of free distribution of Iron Folic Acid (IFA) tablets and free advice on the nutritional requirements during pregnancy and lactation, the prevalence of anemia (50.3%) in India remains one of the highest in the world. The prevalence of anemia among NP-NL women (15-49 year) had increased from 52% in NFHS-1 (1992-93) to 53% in NFHS-4 (2015-16). Unfortunately, the unit level data of anemia in post-2006 is not available in public domain to carry out detailed analyses.
Nevertheless, the unit level analyses based on NFHS-3 data suggest that anemia is not uniformly distributed, rather it is heavily skewed toward disadvantaged group of women. For instance, pregnant and lactating, and NP-NL women living in rural areas, those belonging to a younger age group, and scheduled caste and scheduled tribe are at greater risk of having anemia. These women suffer more because of demand side factors. They have less purchasing power to obtain required levels of supplements, protein, and vitamins during pregnancy and lactation (Agarwal et al. 2006; Goli, Rammohan, & Singh, 2015; McLean et al., 2009; Picciano, 2003). In addition to disadvantaged socioeconomic status, women in vulnerable demographic status such as younger lactating and older pregnant women are also at an increased risk of anemia. Akin to previous studies in other countries (McLean et al., 2009; Picciano, 2003) findings from this study supports that the later stage of pregnancy, concurrent lactation, and higher parity are associated with higher risk of anemia among lactating and pregnant women. However, pregnant women in their first trimester have a lower risk of being anemic as compared with lactating and NP-NL women; this may be because of the ceased menstruation during pregnancy, increase in blood cell volume, minimal growth of the foetus and placental tissues, with additional iron intake and consumption of healthy food during early pregnancy (Agarwal et al., 2006; McLean et al., 2009; Toteja et al., 2006; Vijayalakshmi & Mercy, 1994).
In addition to identifying the demand-side factors, this study also attempted to identify the supply-side factors which determine the prevalence of anemia among pregnant, lactating and NP-NL women, although association is weak and statistically not significant. Anemia is found to be more among those who received program benefits as compared with others. It may be because nutrition advice and supplementary nutrition provided by frontline health workers under Integrated Child Development Scheme (ICDS) is targeted toward disadvantaged women who are already suffering from anemia. Women from better-off households seek nutrition advice and supplementary nutrition from private health care. Nevertheless, these findings give a strong message that the program interventions are ineffective to bring them out of vicious cycle of anemia.
Overall, based on the findings of this study, we emphasize on the importance of varying effects of sociodemographic factors in predicting anemia levels in pregnant and lactating women. In particularly, in a country where the fertility rate is still reasonably high, sociodemographic factors plays a major role in the depletion of women’s iron stores during pregnancy and lactation and lead to anemia Bentley & Griffiths, 2003; Baig-Ansari et al., 2008; Lokare et al., 2012; Rana & Goli, 2016; Vijayalakshmi & Mercy, 1994; Vivek et al., 2012). Thus, the central point as reiterated in the study is that the factors affecting anemia are multifactorial, ranging from disadvantaged socioeconomic and demographic status (poor economic status, no education, early marriage and childbirth, and higher parity) to unavailability of health care provision such as access to free nutritional supplements and dietary advice (Ezzati et al., 2002; Kotecha et al., 2009; Kozuki et al., 2012; Lokare et al., 2012; Sharma et al., 2008). The study also indicate that the factors associated with anemia among pregnant and lactating women may not be the same as factors associated with anemia prevalence among NP-NL women. While improving socioeconomic factors are the key strategy for reducing the prevalence of anemia among NP-NL women, but improvements in both sociodemographic and supply-side factors related to health care programs are crucial to reduce prevalence of anemia in pregnant and lactating women.
In the context, where the successive NFHS (1-4) rounds show that anemia in pregnant and lactating women has dropped only marginally from 58% in 2005-2006 to 50% in 2015-2016 in a period of 10 years, there is a strong need to work around the suggestive measures arising from this study. In particular, strengthening and monitoring the existing programs (e.g., ICDS, Rashtriya Kishor Swasthya Karyakram [RKSK]; Janani-Shishu Suraksha Karyakram [JSSK]; Reproductive, Maternal, Newborn, Child and Adolescent Health [RMNC-A]; National Food Security Act [NFSA]), removing bottlenecks in accessing to programs by promoting awareness and health knowledge among women regarding nutrition and health care is critical for improving anemia among women in India. Anemia as a public health issue in developing country like India can not be eradicated without interventions right form childhood-to-adolescence to reproductive ages rather than targeted programmes at the time of pregnancy and lactation (Goli, Rammohan & Singh, 2015). Moreover, addressing the specific needs of pregnant, lactating, and NP-NL women through effective health care delivery system would help in reducing the prevalence of anemia in India. Increased outreach of health services, training, and motivating frontline health workers not only for pregnancy registration but also for promoting knowledge about balanced nutrition, nutrition rich food, dietary diversity and provision of supplementary nutrition is crucial to prevent anemia among pregnant and lactating women. Similarly, ensuring women’s access to information on risks of early childbirths, lower birth intervals, and higher parities and engaging in risky occupations during pregnancy are also important to reduce anemia among pregnant and lactating women. The government must take proactive efforts to prevent anemia through effective campaign for motivating women to take iron tablets according to the prescribed schedule. Also, tracking anemic children from schools and making interventions will help girls to improve their nutritional status and reduce anemia during pregnancy and lactation. Furthermore, to reduce the burden of maternal anemia, the government should target disadvantageous areas and social groups where the purchasing power, knowledge, and access to health care facilities are minimal. The health care policies must remove bottlenecks and restructure existing interventions to consider the heterogeneous groups of women and their specific nutritional needs. Government has to remove financial barriers in purchasing nutrition-rich food during pregnancy by implementing the NFSA, 2013 in its full spirit. Similarly, different programs aimed at improving the socioeconomic status of the households should also be integrated into the policies of reproductive and adolescent health care to reduce iron deficiency and anemia among women in general and the lactating and pregnant women in particular. The policies aiming to enhance the planning of births by appropriate timing of births, improvement in birth spacing, and avoid unwanted or higher order births through family planning are critical to avoid depletion of maternal fat and tissues in women which make them more vulnerable to anemia.
Footnotes
Authors’ Note
This article is based on the preliminary analysis carried out while conceptualizing and drafting the project “Understanding Pregnancy Nutrition and Health Care among women in rural areas and urban slums of Uttar Pradesh: A Longitudinal study.” The authors would like to thank other team members of the project.
Author Contributions
S.G., M.Z.S., and T.R. conceived and design the experiments. S.G., T.R., and M.Z.S. performed the experiments. M.Z.S., T.R., and S.G. performed the analysis and interpretation of the data. S.G. M.Z.S., T.R., R.D., S.C., C.T., N.P.K., and D.S. drafted the manuscript. Critical revision reagents/materials/analysis tools were provided by M.Z.S. S.G., T.R., R.D., S.C., and N.P.K. Final proof reading and English editing were done by R.D., T.R., S.G. M.Z.S., S.C., N.P.K., C.T., and D.S.
Ethical Statements
Ethical approval for this survey was obtained from the International Institute for Population Sciences (IIPS), Mumbai, India. The informed consent was obtained from all the respondents before conducting interviews. A standard consent form approved by the ethics review committee was read to the respondent in the respondent’s native language. Once the respondent agreed to participate in the survey, the interviewer confirmed this consent and signed on the form acknowledging that the respondent had been read the form, had understood the study and agreed to participate. In preparing the data files for public archiving and distribution, the data producers removed all direct identifiers and characteristics that might lead to identification of data subjects. Hence, no approval by any committee for the protection of human subjects was needed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.