
Abstract
This study utilized a qualitative study design to determine the pregnancy, birth, and postpartum experiences of women who were diagnosed with COVID-19 during pregnancy in Turkey. Interviews were conducted with 14 women using the semi-structured interview technique to evaluate their “pregnancy,”“birth,” and “postpartum” experiences. Data were analyzed using qualitative thematic and content analysis methods. Content analysis of the data revealed four main themes. The themes were as follows: Support for a positive pregnancy experience, uncertainty and fear of the COVID-19 diagnosis, effects of the COVID-19 diagnosis on the birth experience, and effects of the COVID-19 diagnosis on postpartum experiences. The results of this study showed that antenatal care expectations of women during pregnancy could not be met, they could not access reliable information, they experienced disruptions in their follow-ups, they were anxious about their own health and the health of their babies, and they had decreased social interaction.
Introduction
Once the first COVID-19 case in Turkey was detected on the 11th of March, 2020, the pandemic was declared, and some changes were made in maternal care services to reduce infections (Sahin & Kabakci, 2021). Curfews and social distancing became common strategies, and health services were reorganized in a way to minimize the spread of the virus (Akbas et al., 2021). Restrictions were imposed on care partners and visitors in birth, postpartum, and neonatal services of hospitals. All these regulations caused pregnant women to experience many problems (Coxon et al., 2020).
Pregnancy and birth are existential miracles for women. However, the COVID-19 pandemic process caused women to experience anxiety and stress for themselves and the safety of the fetus during pregnancy and birth and worries and anxiety about the health of the newborn in the postpartum period (Aslan et al., 2020). The level of anxiety and stress was even higher for pregnant women who were diagnosed with COVID-19. The data on the COVID-19 infection and its complications during pregnancy are limited (Salem et al., 2021). However, pregnant women were considered a high-risk population after the epidemics such as SARS and MERS. Hence, the COVID-19 pandemic caused women to experience fear, stress, and anxiety in the pregnancy and birth processes (Eri et al., 2022). According to the sixth version of the guidance on Coronavirus Infection in Pregnancy by the Royal College of Obstetrics and Gynecology, the coronavirus pandemic increased perinatal anxiety and depression (RCOG, 2020).
The Intrapartum Care Guide published by the World Health Organization indicates that a positive birth experience is an important indicator for the short-term and long-term well-being of women and babies (WHO, 2018). Sustainable Development Goals aim to reduce the global maternal mortality ratio to less than 70 per 100.000 by 2030. Most maternal deaths can be prevented when health solutions to prevent or manage complications are known well (Moran et al., 2016; WHO, 2018). Therefore, the right management of prenatal, birth, and postnatal processes of pregnant women who were diagnosed with COVID-19 and the prevention of the existing or potential complications are part of Sustainable Development Goals.
In many countries including Turkey, many qualitative studies have investigated pregnant women’s experiences during the COVID-19 pandemic (Eri et al., 2022; Garcia-Silva et al., 2021; Montgomery et al., 2023; Sahin & Kabakci, 2021). However, the literature includes a limited number of studies that investigated the birth experiences of pregnant women diagnosed with COVID-19 during birth (Fumagalli et al., 2022; Nespoli et al., 2022), and no studies were found to have investigated the pregnancy, birth, and postpartum experiences of women who were diagnosed with COVID-19 during pregnancy using qualitative methods. In this regard, the present study is believed to provide an important contribution to the literature. Current study results indicate that receiving insufficient care in the prenatal, birth, and postnatal periods due to the COVID-19 pandemic affected women’s health negatively (Fumagalli et al., 2022; Montgomery et al., 2023; Nespoli et al., 2022; Sahin & Kabakci, 2021).
The purpose of this study is to determine the pregnancy, birth, and postpartum experiences of women who were diagnosed with COVID-19 during pregnancy during the pandemic period in Turkey. The results of the study can shed light on beneficial measures to be taken about the problems experienced in the antenatal period, which is an important period for women, during COVID-19 quarantines and future disasters/pandemics.
Methods
Study Design
This study utilized a phenomenological approach, which is one of the qualitative research designs. The phenomenological approach focuses on a phenomenon that we are aware of but can have no in-depth or detailed information. It enables to investigate of individuals’ experiences(O’Brien et al., 2017). Standards for Reporting Qualitative Research (SRQR) utilized in reporting the qualitative studies were followed while conducting the study and reporting the results.
Sample
The sample of the study was composed of women who agreed to participate in the study, could speak and communicate in Turkish, were diagnosed with COVID-19 during pregnancy, had a baby aged 0 to 6 weeks old, and were aged 18 years and over. Diversity was aimed while choosing the participants in terms of characteristics such as socio-demographic features (age, family type, education level, occupation), the city where they lived, gestational week, number of pregnancies, and mode of birth (Table 1).
Socio-Demographic Characteristics of the Participants.

Women who got pregnant via assisted reproductive technique.
Since it was not possible to conduct face-to-face interviews in different cities in Turkey to determine the experiences of women who were diagnosed with COVID-19 during pregnancy, participating women were interviewed on the phone. Responses of the women who met the research inclusion criteria were filled in by researchers RD/EG. Women to form the study group were accessed using the snowball method. Interviewed women diagnosed with COVID-19 during pregnancy were not known by the researchers, and they were not from their environments. The women interviewed were asked “Can you recommend someone you know to interview about this issue?” to determine the next participant (Patton, 1990).
“Saturation” is an important guide to determining the sample size in qualitative studies (Saunders et al., 2018). The sample size was considered sufficient when the information given by the participants began to repeat and the statements were used repeatedly. Data saturation was reached, and the data collection process was completed when 14 women were interviewed. Data collection and analysis phases of this study were completed within 6 months after ethics committee approval was obtained.
Location of the Research
Women diagnosed with COVID-19 during pregnancy were selected from different cities in Turkey. Participating women were accessed from state hospitals, university hospitals, gynecology and obstetrics hospitals, private hospitals, and family health centers (primary care health service).
Data Collection
Data were collected through a semi-structured questionnaire prepared by the researchers in line with the literature including nine close-ended questions about pregnant women’s socio-demographic and obstetric features and general characteristics about the issue and a questionnaire form that is composed of eight semi-structured questions about their experiences during pregnancy, birth, and postpartum periods (Fumagalli et al., 2022; Montgomery et al., 2023; Nespoli et al., 2022; Sahin & Kabakci, 2021). For content validity, expert views (one lecturer in the field of educational sciences, one lecturer in the field of midwifery, and two experts in the field of statistics) were received for the content, order, and comprehensibility of the questions in the questionnaire form. One of the interview questions was changed in line with the expert views. Due to the pandemic, interviews to be conducted with women were conducted on the phone. The questionnaire had six sections. While the first section was composed of questions about socio-demographic characteristics, the second part included questions about obstetric characteristics. The third section of questions about women’s knowledge and attitudes about the pregnancy process during the COVID-19 pandemic (What do you think about the coronavirus pandemic? How did this condition affect you? How did you spend the pregnancy process in the pandemic period?). The fourth section included questions about pregnancy follow-ups, knowledge, attitudes, and behaviors about the infectiousness of coronavirus to the unborn fetus (Were you able to have your follow-ups regularly during the COVID-19 pandemic and when you were diagnosed with COVID-19?). Did you have any changes in your pregnancy follow-ups in this period? What do you think about the effects of coronavirus on your baby’s health? What do you think about the infectiousness of coronavirus to the unborn fetus?). The fifth section included questions about the experiences in the birth process (Did your COVID-19 diagnosis have any effects on your mode of birth preferences? What mode of birth should pregnant women diagnosed with COVID-19 have? How did you realize your birth? Did you experience any problems?), and the last section included questions about the process experienced after birth (Can you give information about the process you experienced after birth? Can you explain how your doctor, midwife/nurse guided you in this process, did you communicate with them?). To test its comprehensibility, the questionnaire was administered to two participants with characteristics similar to the sample group before the study was started. These participants were not included in the study. Other participants were reached after the first participant was reached by the researchers. Telephone numbers and names of the women suggested by the participants were shared with the researcher through messages. All the women interviewed had been informed by the participants who were interviewed. They were informed about the study by the researcher again and reminded that their telephone conversations would be voice-recorded. The participants were asked to be in a quiet, convenient, and comfortable place where they could speak without being affected by other factors in the environment. Calls were done by phone using the teleconference method, with the participation of participants and two researchers. While one researcher conducted the interviews, the other researcher noted down her observations about the interviews. Interviews were completed in about 25 to 30 min.
Analysis
We used an inductive analytical approach that follows Braun and Clark’s six-step process (Braun & Clarke, 2019; Braun et al., 2016). Data analysis in qualitative studies includes preparing and organizing the data, coding the data, bringing codes together and reducing the data to themes, and then presenting the data with figures, tables, or discussions (Creswell, 2018). Data obtained from this study were analyzed within the framework of thematic analysis and content analysis methods.
Thematic analysis and content analysis: Thematic analysis is a method that is utilized for determining, analyzing, and reporting the themes in the data obtained and enables the organization and description of the smallest units of data (Boyatzis, 1998). The phases of the thematic analysis include gaining familiarity with the data, transcribing and (re)reading the data, creating the first codes, collecting the codes under themes, defining and labeling each theme, selecting exemplary quotes, analyzing the data and associating with the research question, and reporting analyses (Braun & Clarke, 2019).
Content analysis is the systematic, objective, and if possible, quantitative analysis of the content of various documents (Bilgin, 2006). The main purpose of content analysis is to access concepts and relationships that help to explain the collected data. While thematic analysis enables to evaluate participants’ descriptive data, content analysis enables to analyze the content of participants’ views systematically (Karataş, 2015). Steps of the content analysis include determining the research goals, creating the sample, determining the codes and categories, determining the frequencies of the codes and categories quantitatively, if necessary, analyzing the relationships between categories, evaluating, inferencing, and interpreting (Bilgin, 2006). Initially, voice records obtained from the interviews were transcribed. Written interview data were put in the MAXQDA 2020 program (Kuckartz & Rädiker, 2019). An inductive approach was utilized for the analysis of the data transferred in the MAXQDA 2020 program. The data were read repeatedly, and the first codes were formed. Codes associated with each other were labeled by collecting them under themes. Then the obtained themes were explained in a comprehensible way for the readers. Finally, the researcher interpreted the findings to give meaning to them and used various visuals to support the findings (Figure 1). Table 2 demonstrates the themes and subthemes obtained from the data.
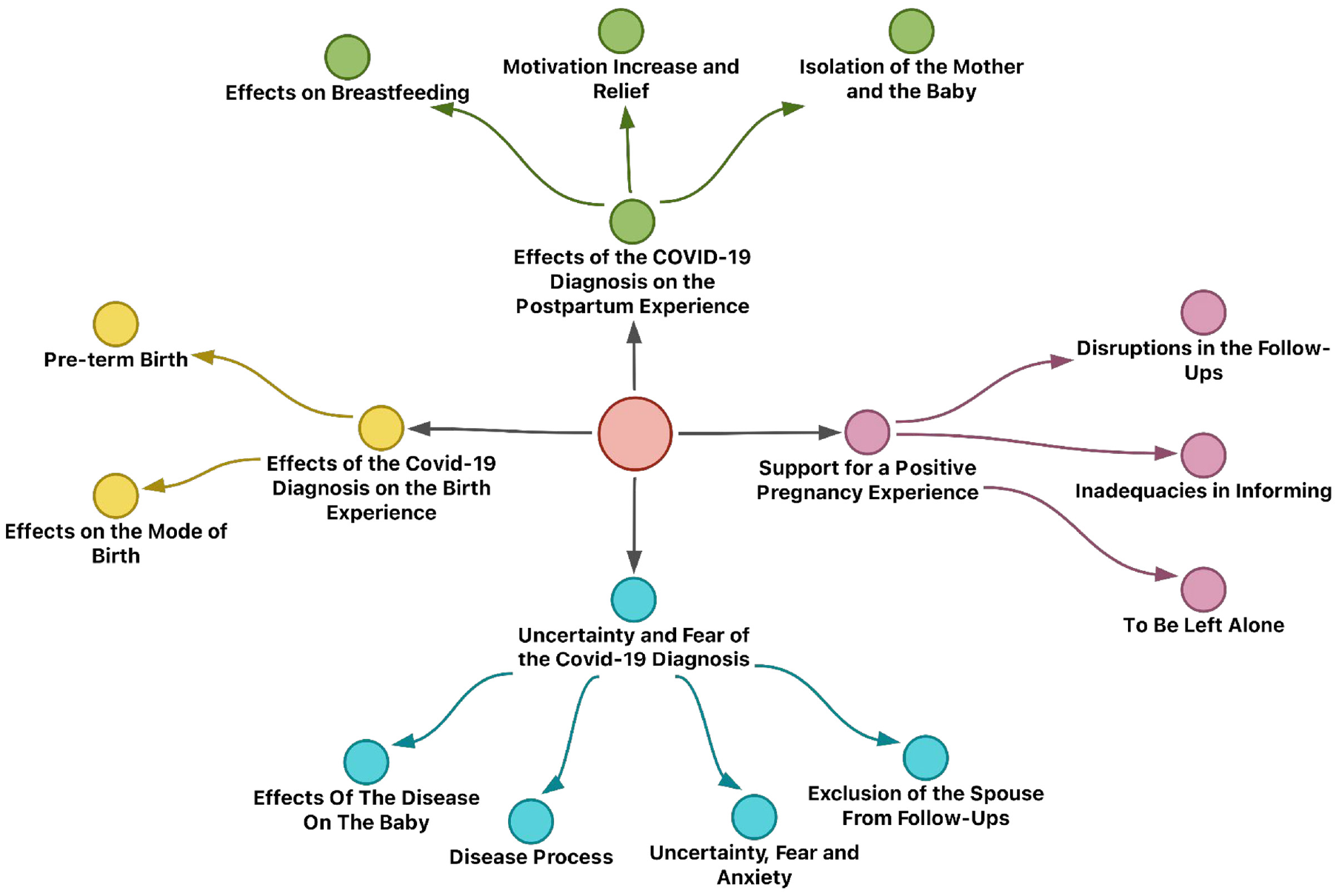
Themes and sub-themes.
Themes and Sub-Themes.

Findings
THEME 1: Support for a Positive Pregnancy Experience
Disruptions in Follow-Ups
The participants reported that they had their pregnancy follow-ups regularly during the pandemic period, yet this process was disrupted, and receiving information became difficult during the time they were infected. After they were infected, their doctors warned them not to go to the hospital unless they had any compulsory examinations, tests, or problems.
I had my regular follow-ups during the pandemic period, but doctors did not examine me during the time I was ill… You are not examined at a time when you need to hear and receive information about your baby the most… I told them that my baby did not move anymore. They told me to go on monitoring for some more time. Being unable to receive any news from my baby…It was one of the most difficult feelings caused by my disease. (P4) I went to the hospital in regular intervals at dates referred by my doctor. I was in quarantine at home throughout the time I tested positive. That’s why I was examined after the quarantine process. (P12)
The participants reported that they were turned back from the hospital when they wanted to be examined as they did not feel the movements of their babies, which caused them to feel anxious.
When I had the diagnosis, I went to a state hospital to be examined because I did not feel the movements of the baby. They turned me back and did not examine me because I tested positive. I felt very much offended (P6)
Inadequacies in Informing
The participants stated that they wanted to receive information about their baby throughout the time they were infected, telephone conversations were not sufficient in eliminating their anxiety, and they could not benefit from pregnancy schools. They also reported that they needed to benefit from pregnancy schools more during the time they were infected.
I was going to join the pregnancy school at the hospital but I could not. I tried to receive information from the internet to get ready for the birth, but it was not very effective. I could not find a website where I can find answers to all my questions. (P8) Maybe because I tested positive, doctors, midwives, nurses, etc. tended to finish the procedures quickly and send me away from the hospital. We had little time to speak…No, I did not go to a pregnancy school. There was reportedly a pregnancy school, but it was closed. Therefore, we could not benefit from it. (P9)
To be Left Alone
The participants stated that being isolated increased their worries about their own health and the health of their babies. They reportedly felt stressed and unhappy during the time they were isolated.
We ate our meals separately. My husband was not with us. He brought our needs to the door and left. I was so anxious in this process. (P3) …My family used to bring food to the door and leave. I had no one with me. My husband worked in a faraway place. My mother took care of my son. Spending this process alone was so sad and tiring. I felt stressed, I cried, and I felt very sad. I was so anxious about my baby. (P14)
THEME 2: COVID-19 Uncertainty and Fear of COVID-19 Diagnosis
Effects of the Disease on the Baby
The majority of the participants reported that although the virus was not directly transmitted to their baby, the disease affected them and thus their baby was also affected indirectly.
Although the virus is not directly transmitted, there is a disease process you suffer from. Hence, babies must also be affected. (P3) It can certainly affect my baby’s health. After all, even our stress affects the baby. You suffer from a disease with severe symptoms that also affect you psychologically. Even if it is not transmitted directly, it must have effects. (P4)
Disease Process
The participants stated that their immunity was weak during the pregnancy process, and being infected with the COVID-19 virus affected them more than it did other individuals. They also reported that they got through the disease harder as they could not use medicine when they were infected.
I suffered a lot from this disease. I was so bad; I was sick in bed. I did not lose taste completely, but it decreased. I got a hoarse voice. I could not produce secretion. Then I began to feel better slowly. (P3). I think pregnant women suffer from the disease more because they cannot take any medicine used by normal people. Let alone medicine, even most herbal remedies are forbidden during pregnancy. That’s why I had great difficulties. (P6)
Uncertainty, Fear, and Anxiety
The participants reported that they felt responsible and guilty for their babies. They stated that the pandemic process was frightening, and pregnant women were more vulnerable in this process. They also reportedly experienced uncertainty and anxiety, particularly about their babies.
Fear had existed all the time. I took all measures to get protected. I had been contacted many times before I was diagnosed with COVID, but I was not too restless. (P5) Coronavirus scares me a lot. As pregnant women are more vulnerable and have weak immunity, they may be affected more. They are more at risk compared to normal individuals… Spending this process alone is very sad and tiring. I was stressed, I cried a lot, and I was so unhappy. I was anxious about my baby, too. (P14)
Exclusion of the Spouse from Follow-Ups
The participants stated that they valued the companion of a spouse or a support person during antenatal visits. Some participants stated that they felt sorry because they could not share this unique experience as their spouses were not with them during examinations.
The doctor let only me inside while he was examining me. They did not let my spouse in. My husband missed many experiences. In my first pregnancy, he felt so happy about watching the baby’s movements, but I could only show the photos of the baby during this pregnancy. Emotionally, he did not feel very excited in this pregnancy of mine. Seeing my belly grow was the only thing that excited him. (P5) I wish I could have the chance to go to follow-ups together and feel the excitement of seeing our baby grow. My husband could not be with me when I went for the follow-ups. (P8)
THEME 3: Effects of the COVID-19 Diagnosis on the Birth Experience
Effects on the Mode of Birth
The participants stated that having cesarean section was normal during the pandemic process. The doctor was the primary person to decide the mode of birth.
I had cesarean section. Actually, our decision was to have a vaginal birth, but our doctor recommended cesarean section because of the pandemic period. The pandemic period was a very hard process. Therefore, I think that our doctors can make decisions. (P7) I was thinking of having vaginal birth, but the disruptions experienced caused me to have cesarean section, but I do not think that it affected the birth. I had no problems during birth. (P10)
Pre-Term Birth
Some of the participants stated that they had a hard disease process after they were COVID-19 positive, and although there was no pre-term birth risk before being infected, they had to have cesarean section during the COVID-19 disease process.
Before I was diagnosed with COVID-19, I had regular follow-ups. I also visited the Family Health Center when our midwife called me. I had my tests done, but I was in the 30th gestational week when I had COVID, and it caused me to have pre-term birth. (P2) I had COVID in my 34th week…There could also be toxemia during pregnancy. Then I was diagnosed with COVID-19. I was worried. I was so scared. They told me that I should have cesarean section. I thought that my baby was so little. My baby was born prematurely. I was so afraid, thinking that something bad could happen to my baby. I got prepared quickly. Even my serum had not finished yet. I had a cesarean section. (P11)
THEME 4; Effects of the COVID-19 Diagnosis on the Postpartum Experience
Isolation of the Mother and the Baby
Some of the participants, particularly those who had pre-term birth, stated that they were exposed to a compulsory isolation process with their babies. They reportedly felt fear and uncertainty when they were away from their babies.
I thought I would die after birth. I suffered a lot. I already had cesarean pain; severe coughs due to COVID increased my cesarean pain. It was so painful. The surgery, problems caused by it, COVID problem… They were unbearable… I was so anxious about myself and my baby… My baby also stayed in neonatal care for 20 days. (P11) After I was moved from the intensive care unit, I felt like I revived again. I spent days imagining my baby’s smell and vision. I wrote down my feelings in this process… I had a little notebook, and I wrote there. I felt better as I wrote. I felt more hopeful. My motivation increased. I prepared our home for our baby. I also prayed a lot. This is how I handled my fears. Now I have my baby with me. Thank God that my baby is good. (P2)
Effects on Breastfeeding
The participants generally experienced no problems that prevented them from breastfeeding. However, two participants stated that they could not breastfeed because their babies were in the neonatal unit for a long time.
I would certainly want to breastfeed, but unfortunately I could not. (P2) I could not breastfeed. My baby was away from me for a long time. I put a lot of effort to breastfeed when we got back home. I could not breastfeed. My baby was so stubborn and thus had baby formula. (P12)
Motivation Increase and Relief
Some of the participants stated that their motivation increased and they felt relieved after they were discharged from the hospital after birth. They stated that motherhood feelings increased their spiritual power and they felt very good when they got back home.
I felt very good after I was discharged from the hospital and came back home. (P3) The real recovery happened after I saw my baby. We went to see my baby after the quarantine process. I cannot express how relieved we felt after my husband and I saw that our baby was good. We became so happy. (P12)
Discussion
This study aims to investigate the pregnancy, birth, and postpartum experiences of women who were diagnosed with COVID-19 during pregnancy in Turkey. The participants in this study were found to encounter important barriers to access to obstetric services such as disruption in their follow-ups and lack of receiving information. Similar problems were also reported in a limited number of qualitative studies published (Meaney et al., 2021; Sahin & Kabakci, 2021). One of the key components of quality motherhood care is to access care at an appropriate and right time (Hayes-Ryan et al., 2017). A study conducted in Canada reported that social support was a key factor in encouraging access to maternal services and participation in these services in vulnerable populations (Thapa et al., 2020). The participants stated that they were worried about their own health and the health of their babies in the quarantine process when they lacked social support and were generally alone. Meaney et al. (2021) reported that pregnant women needed additional social support because of the isolation and loneliness they experienced (Meaney et al., 2021). This study found that for a positive pregnancy experience, pregnant women diagnosed with COVID-19 needed additional support in terms of both social aspects and the presentation of health services. The current literature findings also support our study results (Fumagalli et al., 2022; Meaney et al., 2021; Sahin & Kabakci, 2021).
One of the biggest sources of anxiety caused by the COVID-19 infection during pregnancy was whether the virus was transmitted from the mother to the baby. The first study including six pregnant women who had mild to severe symptoms investigated the possibility of transmission of the COVID-19 infection to the fetus reported to encounter no virus in the cord blood, amniotic fluid, or the newborn throat swab samples (H. Chen, Guo, et al., 2020). Studies conducted later also reported that COVID-19 infection had no vertical transmission, and transmission to the fetus was uncertain (Kimberlin & Stagno, 2020; Y. Li, Zhao, et al., 2020; Wang et al., 2020; Wu et al., 2020). The participants stated that they did not have sufficient information about transmission to their babies throughout the time they were diagnosed with COVID-19. Hence, this uncertainty caused an increase in women’s anxiety and fear. A qualitative study conducted in Turkey reported that pregnant women did not have sufficient information about the transmission of COVID-19 infection to their babies and they experienced fear and anxiety due to insufficient information (Sahin & Kabakci, 2021). The literature reports that the psychological condition of pregnant women diagnosed with COVID-19 should be monitored carefully and acknowledge that they are a vulnerable group at risk (Fumagalli et al., 2022; Nespoli et al., 2022). The study conducted by Puertas-Gonzalez et al. investigated how the psychological impact of the COVID-19 pandemic on pregnant women and found that depression, phobic anxiety, and perceived stress were high in pregnant women affected by the pandemic, in addition, insomnia was a predictive component for depression and perceived stress and the fear of COVID was also predictive factor for the phobic anxiety. Thus, the COVID-19 pandemic could adversely affect the mental health of pregnant women by increasing psychopathological symptoms and stress in pregnant women (Puertas-Gonzalez et al., 2021). Besides, the importance of screening and evaluating pregnant women diagnosed with COVID-19 in terms of factors affecting their psychological condition during pregnancy and postpartum period was also emphasized to decrease depression rates and improve maternal-infant attachment (Fumagalli et al., 2022; Montgomery et al., 2023; Nespoli et al., 2022; Sahin & Kabakci, 2021).
Some of the participants experienced clinical symptoms such as fever, cough, sore throat, and muscle pain. Although current evidence confirms that pregnant women are more susceptible to COVID-19 infection (Rasmussen et al., 2020), the findings are reported to be similar to those of the general population (Breslin et al., 2020; Zhu et al., 2020). However, study results indicate that the process should be maintained in a more controlled way in pregnant women (D. Chen, Yang, et al., 2020; Yu et al., 2020).
The inclusion of fathers and other support people with midwives is reported to have benefits for women and babies (Rominov et al., 2017). Receiving no news about the well-being of the mother or the baby triggered fathers’ anxiety during the COVID-19 pandemic (Montgomery et al., 2023). Fathers felt disturbed due to insufficient communication with health professionals, and they felt very unhappy and helpless when they could not communicate with them during birth (Sanders & Blaylock, 2021). Some of the participants in this study reported that they could not feel safe as their spouses or support people were not with them during birth. The results of this study are similar to the results reported in the literature (Andrews et al., 2022; Fumagalli et al., 2022; Nespoli et al., 2022).
Some participants claimed that having cesarean section was normal during the pandemic process. The presence of COVID-19 infection is not accepted as a cesarean indication by international authorities. However, in case of serious deterioration in general condition due to COVID-19 or the presence of pneumonia, it is recommended to realize birth via cesarean section (N. Li, Han, et al., 2020). Two participants interviewed stated that although they had no pre-term birth risk before being infected, they realized their birth via cesarean section during the COVID-19 disease process. Wang et al. (2020) reported that one woman who had a healthy pregnancy and went for her regular follow-ups before the COVID-19 infection diagnosis had pre-term birth in the 30th gestational week (Wang et al., 2020). It is not clear if these results are associated with maternal infection. However, pre-term birth has been proven to be the most common negative pregnancy outcome seen in pregnant women diagnosed with COVID-19 (Di Mascio et al., 2020). A retrospective cohort study conducted in California reported an increase in the pre-term birth risk of pregnant women diagnosed with COVID-19, particularly in those who had medical comorbidity (Karasek et al., 2021).
In our study, pregnant women who had pre-term birth were reported to have a compulsory isolation process with their babies. They reportedly felt fear and uncertainty during the time they were away from their babies. Although the isolation of the baby decreases the risk of transmission, it can cause negative outcomes for the mother and the baby. For instance, lack of skin to skin contact, increased stress on the mother, disruption of breastfeeding and infant nutrition, and increased stress on the newborn affect the maternal-baby attachment negatively (WHO, 2020). Two participants stated that breastfeeding was not possible since their babies were in neonatal care for a long time. There is no evidence indicating the transmission of the virus via breastfeeding. Antibodies in human milk and other important immunity factors help the baby to get protected against infections. Besides, when the mother or the baby is infected, substances in human milk protecting the baby against infections are reported to be activated. Therefore, it is emphasized that babies must certainly be breastfed during this period (Chua et al., 2020). The participants generally had no problems that prevented them from breastfeeding. Women’s being able to breastfeed their baby increased their motivation and helped them to feel relieved. A study involving five countries reported that women’s breastfeeding intentions were positive and their breastfeeding success was high during the COVID-19 pandemic (Chien et al., 2022). A study conducted in Australia and New Zealand reported that breastfeeding during the COVID-19 pandemic increased women’s well-being and enabled comfort (Sakalidis et al., 2022). Studies also support our findings (Chien et al., 2022; Sakalidis et al., 2022).
This study has some limitations. Firstly, interviews with the participants were conducted on the phone, and the conversations were only voice-recorded. Hence, it was not possible to observe nonverbal clues with body language reflections. Secondly, it is important for the participants that their names are not known to the researcher so that they can feel safe. However, although the participants were not addressed by name during the interviews, their names were known by the researchers due to the nature of the snowball method, yet this was not indicated to the participants. In addition, the findings of this study are unique to this sample group and the results cannot be generalized to the whole population.
Conclusions and Recommendations
The results of this study showed that antenatal care expectations of women diagnosed with COVID-19 during pregnancy could not be met, they could not access reliable information, they experienced disruptions in their follow-ups, they were anxious about their own health and the health of their babies, and they had decreased social interaction. Women’s fear and anxiety were found to increase due to factors such as lack of social support, lack of information about the effects of COVID-19 infection on themselves and their babies, experiencing severe symptoms, and lack of a companion such as spouses or support people during follow-ups and birth. Besides, in case of the presence of the COVID-19 disease, cesarean section was considered to be necessary by participating women, and a few participants had pre-term birth and could not breastfeed their babies. On the other hand, breastfeeding women were found to feel very good with the increase in their sense of motherhood and spiritual strength.
In line with these results, women’s need for reliable information and support increases during pandemic periods. Particularly in the isolation processes, midwives and nurses need to maintain pregnant women’s follow-ups and care and provide them with information and support through mobile communication tools. In line with the holistic care understanding, midwives and nurses need to maintain physical health, support breastfeeding, and take protective measures not only in the period when COVID-19 diagnosis was made, but also in the antenatal, birth, and postpartum processes. In addition to all these, awareness should be raised about the maintenance of mental health and when necessary, cooperation should be done with mental health professionals. The results of this study can be taken into consideration for the preparation of birth service guidelines during COVID-19 quarantines and future pandemic/disaster cases. In addition, it is recommended to conduct further studies to investigate pregnancy, birth, and postpartum experiences of women who were diagnosed with COVID-19 and gave birth in different societies as well.
Footnotes
Acknowledgements
We would like to thank all the participants.
CRediT Authorship Contribution Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval was obtained from the University Scientific Research and Publication Ethics Committee of X University (number: 2022.01.07/52-118; date: January 22, 2022). The women who were reached were given information about the purpose of the study as well as the voice recording of the interviews and the confidentiality of the data obtained. The participants were assured that participation was on a voluntary basis and that they could withdraw from the study at any time they wanted. Voice recordings and transcriptions were saved in password-protected computer files.
Data Availability Statement
The data of this study are available from the corresponding author upon reasonable request.