
Abstract
It is widely acknowledged that the survivor’s psychological response to the traumas of mass conflict can affect adversely other family members. Yet, the focus of past epidemiological studies in the field has been confined to the individual survivor’s posttraumatic stress symptom (PTSS) response. We report the first study of its kind in a postconflict country, in which we examine the effects of trauma exposure in one member of conjugal couples on the PTSS of the other. The study involved 677 conjugal couples drawn from a community survey (n = 1,354) in postconflict Timor-Leste. We used culturally adapted and psychometrically tested measures of traumatic events (TEs), preoccupations with injustice, explosive anger, family conflict, and PTSS. A multilevel actor–partner interdependence model (ML-APIM) demonstrated individual pathways involving exposure to murder and atrocities, preoccupations with injustice, explosive anger, and family conflict, leading to PTSS in both men and women when examined separately, with minor variations in paths by gender. Preoccupations with injustice in male survivors contributed to PTSS in the female partner, but not vice versa. Women may have a gender-specific propensity to identify with the male partner’s preoccupations with injustice following exposure to murder and atrocities. Our findings offer novel clues to the possible factors contributing to the higher rates of PTSS among women.
Keywords
Introduction
Close to 60 million persons have been exposed to the traumas of mass conflict and displacement in recent times (UNHCR, 2015), events that commonly affect more than one person in the family, either directly or indirectly. Yet, with a few exceptions (Kerstis, Engstrom, Edlund, & Aarts, 2013; Kerstis et al., 2014; Rottmann et al., 2015), past epidemiological studies in the field have focused on the posttraumatic stress symptom (PTSS) response of the survivor as an individual. We report a multilevel dyadic modeling analysis conducted on a large sample of conjugal dyads in postconflict Timor-Leste, in which we examine whether trauma exposure and its effects on one member of a conjugal couple influences PTSS in the other.
In designing our path model, we draw on existing theory and empirical findings to examine the intermediary factors that may influence dyadic pathways to PTSS. In particular, we focus on explosive anger based on our past studies in Timor-Leste, which found that the reaction is a common outcome of trauma exposure (Brooks, Silove, Steel, Steel, & Rees, 2011; Rees et al., 2013; Silove et al., 2009) and may result in family conflict, potentially exacerbating PTSS both in the survivor and the partner (S. Rees, Thorpe, Tol, Fonseca, & Silove, 2015; Rees et al., 2013). In addition, studies in high-income countries have identified a process of vicarious traumatization in which PTSS is transmitted from male combat veterans to their female partners (Ben Arzi, Solomon, & Dekel, 2000; Dekel & Solomon, 2006; Greene, Lahav, Bronstein, & Solomon, 2014; Klaric et al., 2012), possibly as a consequence of the spouse’s overidentification with the survivors’ traumatic experiences (Franciskovic et al., 2007; Klaric et al., 2012; Solomon et al., 1992; Zerach, Greene, & Solomon, 2015). A related, but as yet unexamined, mechanism of transmission may involve identification of the spouse with the injustices suffered by the survivor, particularly where the trauma is associated with human rights violations. Studies in the Former Yugoslavia (Basoglu et al., 2005), Kosovo (Lopes Cardozo, Vergara, Agani, & Gotway, 2000), and South Africa (Kaminer, Stein, Mbanga, & Zungu-Dirwayi, 2001) indicate that preoccupations with injustice (manifesting variously as hatred, resentment, and unwillingness to forgive) may contribute to PTSS in the survivor. Our studies in Timor-Leste and among West Papuan refugees (Rees & Silove, 2011; Rees et al., 2013; Silove et al., 2014) have shown a consistent pattern of association between a persisting sense of injustice and PTSS and related symptoms, including explosive anger in the survivor (Tay, Rees, Chen, Kareth, & Silove, 2015). An important question, therefore, is whether, within conjugal dyads, exposure to preoccupations with injustice in the survivor can affect the PTSS of the partner.
In collective societies, human rights violations committed against others may be particularly potent in provoking feelings of injustice. There is evidence, for example, from South Africa, that witnessing murder and atrocities is particularly potent as a trigger of PTSS in the survivor, a finding attributed to the interdependent nature of the culture (Atwoli, Platt, Williams, Stein, & Koenen, 2015). That finding may be especially relevant to Timor-Leste, which remains a strongly collectivist culture in which family and kinship ties are of paramount importance. During the prolonged Indonesian occupation of Timor-Leste (1975-1999), it was common for the indigenous population to be compelled to witness murder and other atrocities as a form of intimidation and repression (Modvig et al., 2000), with both men and women being so exposed (Silove, 1999). In our dyadic model of PTSS, we therefore, focus on murder and atrocities as a common form of trauma that may precipitate preoccupations with injustice in both men and women.
Women are more vulnerable than men to developing PTSS (Breslau, 2001), particularly following exposure to interpersonal forms of trauma, including events causing harm to others that occur remotely to the survivor (Bangasser & Valentino, 2014). It is possible that this propensity reflects the higher level of interpersonal sensitivity exhibited in general by women (Breslau, 2001; Franciskovic et al., 2007; Tolin & Foa, 2006). These findings may suggest that women may be at greater risk of vicarious traumatization and/or sensitivity to the injustices experienced by their partners. However, existing data cannot answer these questions given that past studies have been restricted to spouses of male combat veterans, allowing examination of only unidirectional effects from males to females (Ben Arzi et al., 2000; Greene et al., 2014; Klaric et al., 2012).
Our aim was to identify individual and dyadic pathways leading from the experience of witnessing murder and atrocities to PTSS within conjugal couples in Timor-Leste. We included a sequence of intermediary variables (preoccupations with injustice, explosive anger, and family conflict) based on the aforementioned theoretical and empirical considerations. We hypothesized that preoccupations with injustice would play a pivotal role, either directly or via explosive anger and family conflict, in the individual pathways to PTSS. In addition, we examined whether these intermediary factors (preoccupations with injustice, explosive anger, and family conflict) exerted dyadic effects, that is, were involved in pathways leading from one partner to the other in relation to PTSS; and if so, whether there were gender differences in these effects.
Method
Participants
Between May 2010 and November 2011, we undertook a total household survey of men and women 18 years and older, who were residents of a rural and an urban administrative village (suco), one site being a suburb of Dili, Timor-Leste’s capital, the other, a 1-hr distance by road from the city. A single chief (chefe) administers each suco, which comprises geographically contiguous hamlets (aldeias). We used Global Positioning System (GPS) coordinates and aerial maps used in the general population census to identify all dwellings. The two villages were heavily affected by conflict during the Indonesian occupation (1975-1999) and the subsequent period of internal violence occurring in 2006-2007.
Of the 3,597 individual respondents, 2,964 completed interviews, an 82.4% response (those who did not respond included refusers [n = 81], people we could not contact after three visits [n = 387], and those too incapacitated to be interviewed by virtue of severe intellectual impairment or physical illness [n = 165]). All relationships were recorded, allowing us to identify 677 dyads (n = 1,354), comprising men and women living in conjugal relationships in the same household.
Ethical approval for the inquiry was provided by the Human Research Ethics Committee (HREC) of the University of New South Wales as well as by the Timorese Ministry of Health, and relevant village chiefs.
Measures
Witnessing Murders
The traumatic event (TE) domain of witnessing murders and atrocities was assessed by items included in the Harvard Trauma Questionnaire (HTQ; Mollica et al., 1992; Silove et al., 2014) adapted to the historical context of Timor-Leste. Four traumatic items covered witnessing murder of a family member, murder of friend/community member, serious injuries inflicted on others, and atrocities. To focus respondents’ memories, we dated TEs to two well-defined historical periods, the Indonesian occupation commencing in 1975 leading up to the humanitarian emergency of 1999, and the period surrounding and following independence in 2002, extending through the internal conflict of 2006 to 2007. In analyzing the data, we generated a total trauma count for witnessing murder and atrocities based on a summary score in which each of the four constituent items was scored 1 if the event had occurred at any time across both the relevant historical epochs and 0 if there was no exposure.
Family Conflict
We previously developed an inventory of family conflict (Rees et al., 2013) based on two items indicating conflict with husband or wife and conflict with other family members. Each item was scored 1 if endorsed as a serious/very serious problem, or 0 if rated as not a serious/a less serious problem, the range of summary scores for each individual being 0 to 2.
Preoccupations With Injustice
To assess preoccupations with injustice, we asked respondents to identify and describe the worst acts of injustice they had experienced for each of three defined historical periods, the Indonesian occupation, the period of internal conflict, and in contemporary times. Qualitative data were collected to characterize the events nominated (full details to be reported elsewhere). The most common events nominated related to politically motivated murder or harm perpetrated against family or others. Participants were asked whether they continued to have persisting preoccupations related to injustice associated with the nominated event and whether these memories continued to cause distress. Scoring of responses for the designated time period was as follows: 0 = no event nominated, 1 = an unjust event recorded, 2 = an event accompanied by preoccupations of injustice, and 3 = an event, preoccupations of injustice, and accompanying distress. The index we used in our model was a composite of the scores for the three designated historical periods.
PTSSs
PTSS was measured using the widely applied Harvard Trauma Questionnaire (HTQ) (Mollica et al., 1992). The instrument consists of 16 symptoms rated by frequency as 0 = none, 1 = some of the time, 2 = a lot of the time, and 3 = most of the time. The scale demonstrated sound internal reliability (α = .95). A past convergence study based on a stratified sample of 97 Timorese compared the HTQ administered by trained Timorese lay interviewers with a clinical diagnosis of posttraumatic stress disorder (PTSD) made independently by experienced Australian psychologists (Liddell et al., 2013). The field measure showed a sound level of convergence with the clinical interview (area under the curve [AUC] = 0.82, 95% CI = [0.71, 0.94]). A score of 2.2 best represented the balance of sensitivity (77.3%) and specificity (87.5%), correct classification being a high 83%. In the path model, we use the continuous total PTSS score generated by adding scores for individual items.
Explosive Anger
We have reported the development of our index of explosive anger previously, a series of qualitative and quantitative tests being applied to ensure its cultural and contextual relevance and psychometric properties (Rees et al., 2013). We drew on the definition of anger attacks as sudden episodes of subjective rage commonly associated with aggression. The measure was assessed in the aforementioned convergence study against the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) category of Intermittent Explosive Disorder (IED) on the Structured Clinical Interview for DSM-IV Mental Disorders (SCID) (Liddell et al., 2013), yielding a high level of convergence: AUC = 0.90 (95% CI = [0.83, 0.98]). We applied a dimensional index of explosive anger by adding endorsed symptoms (1 = present, 0 = absent), yielding a range of scores for each individual from 0 to 4.
We translated and back-translated all measures into Tetum, the widely spoken indigenous language using international guidelines (Van Ommeren et al., 1999).
Analysis
Descriptive statistics are presented for sociodemographic characteristics and prevalence of TEs, PTSD, and explosive anger for men and women partners. We applied McNemar’s test to assess for differences in sociodemographic variables, TE exposure, family conflict, preoccupations with injustice, and mental health outcomes between women and men across dyads. In accordance with the multilevel approach to dyadic modeling (Campbell & Kashy, 2002; Kenny & Cook, 1999; Kenny, Kashy, & Bolger, 2005), we first examined the degree of nonindependence of the outcome variables within men and women dyads. We then applied a multilevel, actor–partner interdependence model (APIM; Cook, 1998; Ledermann & Macho, 2009) to examine for dyadic effects of predictors (TEs, preoccupations with injustice, family conflict, and explosive anger) on PTSS. Analytic approaches described in the literature to derive dyadic models are based on structural equation modeling (SEM; Cook, 1998) and multilevel modeling (MLM; Campbell & Kashy, 2002; Cook & Kenny, 2005). We examined a series of APIM models within the MLM framework, allowing for two equations (one for each member of the dyad) to be estimated simultaneously (Campbell & Kashy, 2002). Specifically, we applied the approach developed by Raudenbush, Brennan, and Barnett (1995) in which actor and partner effects for men and women partners nested within a dyad were estimated as separate parameters using MLM (Raudenbush et al., 1995). MLM takes into consideration the hierarchical structure of the data and associated nonindependence of observations (Kenny, 1999). We tested a random-intercept multilevel model in which the intercepts for y (represented by men and women partners’ PTSS mean scores) were allowed to vary across clusters (set to be random at the between level). The variance in the dependent variable was partitioned into within- (individual) and between-level components (dyadic), indicating the proportions of variance in men’s and women’s outcome variables explained by each component.
In the multilevel random-intercept APIM model restricted to main effects, we examined for individual and dyadic relationships between witnessing murder and atrocities, preoccupations with injustice, explosive anger, family conflict, and PTSS (the continuous score based on the summation of all item scores). We first applied constraints to test for equality, that is, whether a person’s actor effect is equal to the partner effect (Cook & Kenny, 2005). The base-saturated APIM model showed a significant difference in the covariance pattern of the effects of individual men and women on partners’ effects, indicating that there were potential differences by gender. Building on the foundation of the base model, we then examined for actor and partner effects within men and women dyads. Regression coefficient estimates adjusted for the nonindependent nature of the data were calculated for men and women actor effects, respectively, and for dyadic (partner) effects in which men’s predictors (TEs, family conflict, injustice, and anger) were regressed on women partners’ PTSS and vice versa (Kerstis et al., 2014; Kerstis et al., 2013; Rottmann et al., 2015).
We applied maximum likelihood estimation with robust standard errors to estimate parameters of the multilevel API model. MLR standard errors are robust to nonindependence and computed using a sandwich estimator (Muthén & Muthén, 2014). The criteria we applied to evaluate model fit (Barrett, 2007; Hu & Bentler, 1999) were a nonsignificant chi-square test, the comparative fit index (CFI; >0.90), the Tucker–Lewis index (TLI; >0.90), the root mean square error of approximation (RMSEA; <0.05), and the standardized root mean square residual (SRMR; <0.05). Stata SE version 13 (StataCorp, 2013) and Mplus version 7.2 (Muthén & Muthén, 2014) were used to perform all analyses.
Results
Descriptive Statistics
Table 1 reports sociodemographic characteristics, prevalence of witnessing murders and atrocities, ongoing family conflict, preoccupations with injustice, explosive anger, and PTSS, stratified by men and women across the 677 dyads. The mean age was 43.5 years (SD = 12.47 years) for men and 38.9 years (SD = 12.1 years) for women. Women were more highly educated. Although men had higher levels of employment overall, more women had paid work either in the private sector or in government offices. Women had higher rates of threshold (≥2.2) PTSS compared with men.
Sociodemographic Characteristics, Family Conflict, Witnessing Murders, and Mental Health Outcomes Analyzed According to Gender Across Whole Sample of Dyads (n = 677).

Note. PTSD = posttraumatic stress disorder.
One-way ANOVA indicated evidence of nonindependence between spousal experiences of witnessing murders of strangers (F = 0.02, intraclass correlation [ICC] = .02, p = .02), preoccupations with injustice (related to the Indonesian occupation; F = 4.55, ICC = .04, p = .04), and spousal reports of family conflict (F = 3.81, ICC = .02, p = .02).
Multilevel APIM (ML-APIM)
Actor Effects
Table 2 reports the fit statistics of the ML-APIM models tested. Model 1, which constrained actor and partner effects to be equal, produced a significant chi-square, indicating that the two covariance estimates were not equal (χ2 = 123.89, df = 52, p < .0000). Model 2 in which explosive anger was specified as the endpoint, that is, following PTSS in the model, indicated a poor fit, χ2(50) = 235.54, p < .000, CFI = 0.81, TLI = 0.66, RMSEA = 0.07, SRMR = 0.07. The final ML-APIM model (Model 3) examining for actor and partner effects in which PTSS was the endpoint within and between dyads achieved a good fit: χ2(46) = 47.79, p = .40, CFI = 0.99, TLI = 0.99, RMSEA = 0.01, SRMR = 0.02.
Goodness-of-Fit Indices for Multilevel Actor–Partner Interdependence (ML-APIM) Models Tested.

Note. Model 2 tests equality of the actor and partner effects in within each role in which a person actor’s effect is equal to his or her own partner effects. LogL = log likelihood; CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; SRMR = standardized root mean square residual.
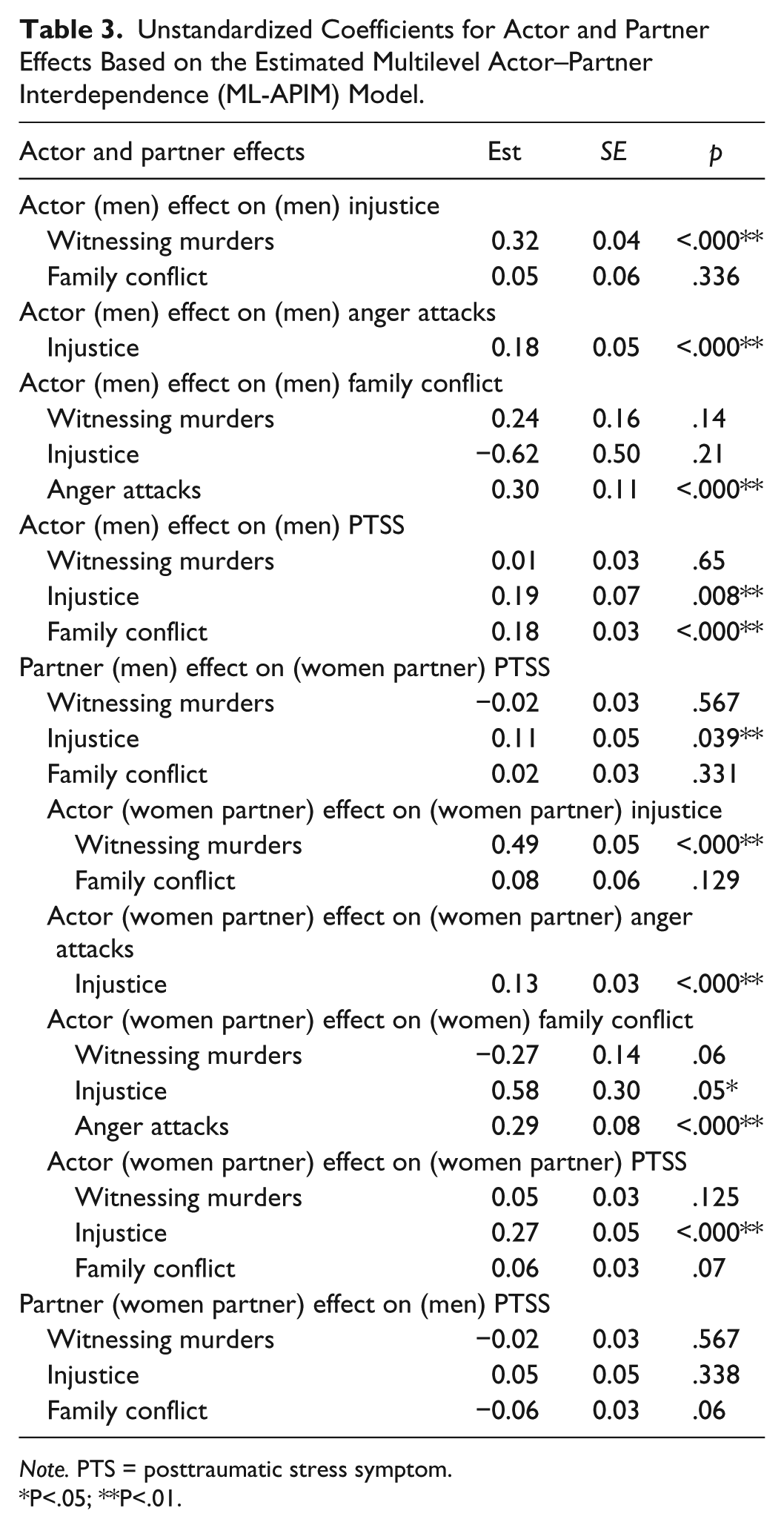
Table 3 reports unstandardized coefficients for actor and partner effects based on the estimated ML-APIM model. Among men, witnessing murders and atrocities led directly to injustice (α = .32, p < .000), injustice led to explosive anger (α = .18, p < .000), and explosive anger led to family conflict (α = .30, p < .000). There were direct paths from family conflict (α = .18, p < .000) and injustice (α = .19, p < .000) to PTSS.
Unstandardized Coefficients for Actor and Partner Effects Based on the Estimated Multilevel Actor–Partner Interdependence (ML-APIM) Model.
Note. PTS = posttraumatic stress symptom.
P<.05; **P<.01.
Most paths for men were replicated for women, in that witnessing murders and atrocities led to injustice (α = .49, p < .000), injustice led to explosive anger (α = .13, p < .000), and explosive anger (α = .29, p < .000) led to family conflict. The paths for women differed, however, in that preoccupation with injustice was associated with family conflict (α = .58, p = .05) and the effect of family conflict on PTSS fell below statistical significance (α = .06, p = .07). The final MLM-API model is represented diagrammatically in Figure 1.

A multilevel actor–partner interdependence model (ML-APIM) examining actor and partner effects of witnessing murders, injustice, anger on (PTS) symptoms among 677 spousal dyads (all paths are significant).
Partner Effects
The single dyadic effect identified involved a path leading from preoccupation with injustice among men to PTSS in women partners (α = .49, p < .000). In contrast, there were no significant dyadic paths from women to male partners. The variances in relation to the cluster means represented by men’s and women’s PTSS scores at the between level were not significant (men: p = .40; women: p = .949), indicating that PTSS scores did not vary significantly across dyads.
Discussion
To our knowledge, our dyadic analysis is the first application of its kind in the postconflict field of mental health. Men and women were largely comparable in their individual pathways leading to PTSS, the sequence commencing with exposure to witnessing murder and atrocities and progressing via intermediate variables of preoccupations with injustice, explosive anger, and family conflict. Gender differences included a second path from preoccupations with injustice to PTSS among women, and a significant association between family conflict and PTSS among men. The single but striking dyadic effect was that there was a unidirectional pathway from men’s preoccupations with injustice to women partners’ PTSS.
In interpreting the findings, it is important to evaluate the strengths and limitations of our methodology. The historical context of Timor-Leste provided an opportunity to test gender differences in our dyadic model, a comparison precluded by the design of past studies, which focused exclusively on male partners, usually combat veterans exposed to trauma (Dekel & Solomon, 2006; Franciskovic et al., 2007; Greene et al., 2014). In addition, our study was exceptional in being large, involving systematic recruitment from the community, achieving high response rate. We systematically adapted all measures to the context, and translated and back-translated according to contemporary guidelines. Our measures of PTSS and explosive anger were tested against gold standard clinical interviews, demonstrating sound levels of convergence.
Although we included a measure of family conflict, we did not assess explicitly for intimate partner violence (IPV), an important possible contributor to PTSS in the woman (Coker et al., 2002). There always is a risk of recall bias in recording trauma events, although the nature and range of events reported correspond to the details of the history of conflict in the country (Modvig et al., 2000). The study is cross-sectional, and hence, causal inferences can only be tentative in the absence of longitudinal data.
Caveats notwithstanding, our findings provide support for our proposed theoretical model by showing a broadly consistent sequence of paths in men and women leading from exposure to murder and atrocities of conflict via preoccupations with injustice, explosive anger, and family conflict to PTSS. In both genders, we found a pathway from preoccupations with injustice to explosive anger and then from the latter factor to PTSS, but in women, there was an additional path from preoccupations with injustice to family conflict. Of key relevance is that preoccupations with injustice in men contributed to PTSS in their female partners, the converse condition not being the case, that is, preoccupations with injustice in women affecting PTSS in men.
Our findings raise important questions as to why men’s preoccupations with injustice influence women’s PTSS but not vice versa. One general factor may be that women exhibit greater interpersonal sensitivity (Bangasser & Valentino, 2014; Gardener, Carr, Macgregor, & Felmingham, 2013; Tolin & Foa, 2006), which in turn may increase their tendency to identify with the injustices experienced by close others. A broadly consistent finding from a U.S.-based study was that the extent to which husbands regarded the world as a benevolent place played a moderating role in the association between women partners’ worldviews and their PTSS (Monson, Fredman, & Dekel, 2010). Although speculative, it is possible that women’s traditional roles (Öhman, 2000; Williams et al., 2007) in maintaining the family bond and comforting those in distress increases their sensitivity to preoccupations with injustices or grievances in close others. An overarching factor is that women have a greater propensity to develop PTSS, particularly in response to interpersonal traumas and losses, the domain of TEs assessed in our study (Creamer, Burgess, & McFarlane, 2001; Kessler et al., 2014). It is intriguing to consider that this increased prevalence of PTSD may relate to women’s sensitivity to interpersonal issues, particularly the sense of injustice in their partner. A further contextual factor, which may be relevant to Timor-Leste and other traditional, conflict-affected societies, is that fear of stigma and rejection oblige women to keep private their experience of abuses such as rape and sexual slavery, thereby precluding the possibility that their preoccupations with injustice can be shared by their male partner. Finally, it is possible that men who have experienced extensive trauma associated with injustice are at risk of perpetrating IPV, an independent contributor to PTSS among their female partners. Future studies, therefore, should measure the presence of IPV to define more clearly the relevant pathways from preoccupations with injustice to PTSS in each gender.
Our findings suggest that the PTSS reaction is shaped by factors that extend beyond mortal threat to the domains of interpersonal interactions and a sense of justice (Silove et al., 2017; Tay & Silove, 2016). Maercker and Horn (2013) have given particular emphasis to interpersonal processes as being instrumental in the genesis and perpetuation of the PTSS response in the individual, the dyad, and the wider social level (Maercker & Horn, 2013). There is growing evidence that threats or disturbances in the close interpersonal sphere may be particularly relevant to the pathogenesis and perpetuation of PTSS among women. From an evolutionary perspective, the PTSS response may represent a more complex survival reaction than the atavistic phobic reactions, for example, in response to snakes and spiders (Bracha, 2006). Whereas snakes and spiders are almost invariably dangerous, the response to other humans requires discrimination in that these conspecifics can be either a source of protection or of threat (Bracha, 2006). Hence, although speculative, rehearsing memories of past experiences of threat involving conspecifics may assist the person to decide how to react when confronted with the same or similar situation in the future (Silove, 1998). Given the traditional role of the carer of close family, a heightened interpersonal sensitivity to threat or vulnerability not only in the self but also in close others, may make women more attuned to preoccupations of injustice or grievance in family members, given that these cognitions represent a signal of the possible source of future threat. Such signals are particularly important in a community, such as Timor-Leste, where perpetrators and survivors live in close proximity.
These considerations add to calls to expand contemporary approaches to PTSS assessment and treatment (Silove, 2004, 2013) to focus not only on the threat component but also on the interpersonal (Markowitz, Lipsitz, & Milrod, 2014; Markowitz et al., 2015; Monson et al., 2010) and injustice/existential dimensions of the trauma reaction (Resick & Schnicke, 1992). From a clinical perspective, our data therefore underscore the importance of undertaking a comprehensive assessment of the interpersonal domain when assessing a survivor of trauma with PTSS, particularly women. The assessment should extend to key issues in the intimate partner, such as his trauma history, state of preoccupation with past injustices, and the level of identification/sensitivity that the survivor manifests in relation to these issues. In selective instances, a dyadic assessment may throw light on the woman’s PTSS by providing insight into the effects of trauma on her male partner. The use of interpersonal therapy (IPT) may be particularly relevant to treating PTSS among women for whom relationship issues loom large as an exacerbating or perpetuating factor (Markowitz, 2010; Markowitz, Milrod, Bleiberg, & Marshall, 2009). Our findings also encourage interest in pursuing dyadic approaches to psychotherapy for PTSS adapted to postconflict settings, possibly drawing on the extant couple treatments developed in the United States (Monson et al., 2010; Nelson Goff & Smith, 2005). The approach specifically encourages the couple to focus on both their individual and shared feelings of injustice, associated symptoms of explosive anger, and concerns arising from family conflict, all factors shown in our model to contribute to PTSS.
At a broader policy level, addressing shared preoccupations with the sense of injustice arising from the history of human rights abuses in the society as a whole is important to fostering communal recovery in countries such as Timor-Leste. Although a truth commission (the CAVR; Comissão de Acolhimento, Verdade e Reconciliação de Timor Leste) was conducted soon after national independence in Timor-Leste in 2002, there is evidence of widespread dissatisfaction with the outcome, particularly because the majority of the perpetrators of murders and atrocities fled to Indonesia and were never apprehended (Silove, Zwi, & le Touze, 2006). Although there are no simple remedies to overcoming the pervasive feelings of injustice concerning past murders and atrocities in postconflict countries such as Timor-Leste, a range of social initiatives may assist the process of recovery, including regular acknowledgment of the sacrifices made, the conduct of memorial and religious services that are consonant with the traditions and culture, and the provision of appropriate material compensation for survivors, strategies that have been implemented to a lesser or greater extent in more recent years in Timor-Leste (Silove, 2013).
Footnotes
Acknowledgements
We thank our field staff and the Alola Foundation for their support and input.
Authors’ Contributions
A.K.T. contributed to the conceptual foundation of the study, conducted data analysis, took a role in interpreting the findings, and drafted and revised the article. S.J.R. assisted in the conceptualization of the analysis and in the drafting and revision of the article. N.T., E.S., and Z.M. conducted the data collection. D.S. contributed to the conceptualization of the study, the interpretation of the data, and to the writing and revision of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support from the National Health and Medical Research Council Australia (Grant No. RM08333).