
Abstract
This study sought to identify factors associated with doctors’ intention to provide lifestyle counseling to cancer survivors and provide an evidence base for developing an intervention to maximize counseling behavior in cancer management programs. A cross-sectional survey based on the Theory of Planned Behavior (TPB) was conducted. Participants were 210 medical doctors recruited from two hospitals in Nigeria. Participants completed questionnaires containing all the theoretical constructs of TPB. Structural equation modeling was used for data analysis. Goodness-of-fit indices indicated adequate fit for the final structural models. Attitude and subjective norm, but not perceived behavioral control, were identified as significant predictors of intention to provide lifestyle counseling. Intention also significantly predicted counseling behavior. This evidence informs the design of a behavioral intervention to improve lifestyle counseling behavior in cancer management programs.
Background
Long-term survivorship is the new mantra for cancer management. Many studies have assessed strategies that may enhance physiological outcomes and palliate the varying range of debilitating symptoms associated with cancer and its treatments (Calfas et al., 1996; Davies, Batehup, & Thomas, 2011; Gray et al., 2013; Jones, Courneya, Fairey, & Mackey, 2005). Particular attention has been given to basic lifestyle factors including weight, physical activity, and diet. These lifestyle factors among others have been held culpable for cancer progression, recurrence, and development of new events/diseases (Davies et al., 2011; Rock et al., 2012). Though the relationship between these lifestyle factors and cancer outcomes are still unclear, it has been estimated that 27% to 39% of cancers can be prevented by improving diet, physical activity, and body composition (World Cancer Research Fund, 2009). Many advanced countries are incorporating self-management support centered on these lifestyle factors into their cancer care system as an adjunct therapy to surgery, chemotherapy, and other treatment options (Jones et al., 2005; Loh, Yip, Packer, & Quek, 2010). This support involves counseling survivors on lifestyle behavior changes and providing them with necessary resources to promote adherence. Counseling support is recommended as best upon diagnosis, when the diagnosed are vulnerable and willing to learn and play a more active role in their health care (Davies et al., 2011; Demark-Wahnefried, Aziz, Rowland, & Pinto, 2005; Jones, Courneya, Fairey, & Mackey, 2004). Policies and guidelines on nutrition, physical activity, and weight management which provide a global perspective on self-management strategies to improve cancer outcomes and quality of life have been developed (American Cancer Society, 2012; World Cancer Research Fund, 2009).
Nigeria, the highest populated country in Africa (Central Intelligence Agency [CIA], 2015), is only at the infancy stage of cancer management. Its field of oncology is rife with problems ranging from no national cancer policy to lack of oncology specialists, finances, and resources, to mention a few (Oluka, Shi, Nie, & Sun, 2014). Besides the control of reproductive cancers which is included in the National policy on reproductive health and strategic framework as well as in the policies on food, nutrition, and health promotion, the government has yet to approve any cancer policy (Federal Ministry of Health, 2004; Kolawole, 2011). Also, in a country of more than 170 million people with cancer incidence of about 74,000 for both males and females in 2014, there are approximately nine radiation centers, 30 radiation oncologists, 100 pathologists, and less than 100 oncologists (CIA, 2015; Kolawole, 2011; World Health Organization, 2014). Treatment of cancer, where available, is expensive and in a country, known to be “rich with poor people,” most of those diagnosed are poor and cannot afford treatment (Health Reform Foundation of Nigeria, 2006). This is compounded by the lack of a system of health care financing and shared risks, which has led to families bearing cancer care costs through spending savings and investments, borrowing at high economic and social costs, and sale of resources like homes and investments, thereby making cancer an important risk factor in poverty and loss of social status among the middle class (Adebamowo, 2013). Ultimately, rather than pay for recommended treatment methods, survivors fall prey to a host of unreliable and harmful herbal remedies as well as other unorthodox treatment options (Oluka, Shi, et al., 2014). In the face of these issues, cancer mortality rate is over the top and strategies for long-term survival are nonexistent (Ferlay et al., 2010). While policies are still being tendered to the government for approval and financing, self-management strategies have been proposed to enable cancer patients cope effectively and reduce the long-term impact of cancer (Oluka, Shi, et al., 2014). These strategies, though not a replacement for treatment, costs little or nothing and will serve as an immediate response to disease management, and improve long-term survival and quality of life. The concerted effort of a team of multidisciplinary health care providers was recommended to ensure implementation of these strategies (Oluka, Shi, et al., 2014).
The Theory of Planned Behavior (TPB) has been employed in many cancer management–related studies (Courneya et al., 2004; Di Sarra et al., 2015; Jones et al., 2005; Wade, Smith, Hankins, & Llewellyn, 2010). It is a social-cognitive model which postulates that performance of a particular behavior is determined by intention which is in turn, influenced by three constructs: attitude, subjective norm, and perceived behavioral control (PBC; Ajzen, 1991, 2012). Intentions are subjective judgments about how individuals will behave in future and has been used as a surrogate measure of future behavior in many studies (Giles et al., 2007; Tan, 2013; Wade et al., 2010). Attitude refers to an individual’s positive or negative evaluation of performing a behavior. Subjective norm is the individual’s perception of social pressure to/not to perform a behavior. PBC reflects an individual’s perceived ease or difficulty to perform a behavior and is assumed to have both indirect (through association with intention) and direct influence on behavior. The theory further postulates that these three determinants of intention may be measured directly (based on individual overall beliefs) or indirectly (based on individual specific salient beliefs; Ajzen, 1991; Francis et al., 2004).
Oncology specialists are in a key position to provide lifestyle change support to cancer patients. Oncologists especially, have intimate knowledge of the patients’ health status, and are better placed to help them choose behavior changes that are appropriate, safe, and feasible (Oluka, Shi, et al., 2014; Sabiston, Vallance, & Brunet, 2010). This personal touch may not only encourage lifestyle behavior change but may also ensure adherence. In fact, many studies have provided preliminary evidence consistently demonstrating oncologist approval as a powerful tool in predicting intention and facilitating health behavior change among cancer survivors (Blanchard et al., 2003; Courneya & Friedenreich, 1997; Jones et al., 2004; Rock et al., 2012). Based on the TPB, the oncologist’s approval is termed a normative belief and has been reported to translate into feelings of approval and support (favorable subjective norm), belief that the behavior may be useful (positive attitude), and greater motivation/intention to perform the behavior (Jones et al., 2005). However, as Nigeria has a limited number of oncology specialists as is common with many low- and middle-income countries, it was recommended that rather than wait for more specialists to be trained, a cost-effective strategy would be to recruit physicians, regardless of their specialty, to provide lifestyle counseling to cancer patients (Oluka, Shi, et al., 2014).
In this study, the TPB is used to identify the predictors of a physician’s intention to provide lifestyle counseling to cancer survivors during treatment consultation, with the objective of providing an evidence base for developing an intervention to maximize lifestyle counseling behavior in cancer management programs.
In this article, the terms cancer patient or survivor, and doctor or physician are used interchangeably.
Method
In this study, we hypothesized that a physician’s attitude, subjective norm, and perceived behavior control would predict intention to counsel cancer patients. Furthermore, intention and PBC would predict actual lifestyle counseling behavior.
Participants and Design
We employed a cross-sectional survey design. Participants were medical doctors working at two major federal and state government-owned hospitals (University of Nigeria Teaching Hospital [UNTH] and Enugu State University of Science and Technology Teaching Hospital [ESUTH]) in Enugu, Nigeria. Ethical approval and permissions were obtained from the Ethics Review Boards of Tongji Medical College, Wuhan, China; UNTH; and ESUTH. Convenience sampling method was employed in the selection of study participants; however, only certified doctors with at least 1 year of experience were eligible to participate. Self-administered questionnaires and informed consent forms were given to willing participants. A total of 350 questionnaires were distributed and 210 medical doctors recruited.
Measures
A lifestyle counseling questionnaire, modeled based on the TPB, was employed in this study. The questionnaire, containing questions on all the TPB constructs and demographic characteristics had been previously validated in a pilot study on participants from the same population as this study (Oluka, Apio, Phiri, Nie, & Sun, 2014). Both direct and indirect measures of TPB were employed.
The direct measures included two attitude items (ATT), two items on subjective norm (SN), three PBC, and three intention (INT) items. Responses were scored on a 7-point Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). Individual item scores were averaged to produce a composite score for each construct.
Indirect measures included five behavioral beliefs for attitude (ATB) and their corresponding outcome evaluations (10 items in total), five normative beliefs (NB) and their corresponding motivation to comply (10 items total), and two control beliefs (CB) and their corresponding strength of belief (four items total). Responses were either unipolar, 1 (extremely unlikely) to 7 (extremely likely), or bipolar, −3 (extremely undesirable) to +3 (extremely desirable). Each belief was multiplied with its corresponding outcome to obtain weighed scores which were summed to create composite scores for each construct so that possible ranges of total scores were −105 to +105 for ATB and NB and −42 to +42 for CB. For both direct and indirect measures, high summary scores consistently reflect stronger or more positive beliefs toward the target behavior.
Actual lifestyle counseling behavior was assessed based on a single question with a “yes/no” response format employed.
Data Analysis
Descriptive statistics were calculated to describe the characteristics of the study population. Internal consistency for the reliability of each item relating to the direct TPB measures was assessed using Cronbach’s alpha. Content validity of indirect measures was confirmed using simple bivariate correlations between direct and indirect measures of the same construct.
Structural equation modeling (SEM) was conducted to determine the association between TPB variables and lifestyle counseling. Confirmatory factor analysis (CFA) was first conducted to determine whether there is empirical support for the hypothesized theoretical factor structure. Based on the confirmed factor structure, SEM was then carried out to identify the potential relationships among all TPB variables.
Maximum likelihood method was used to estimate parameters in the SEM analysis and model fit assessment was based on absolute model fit indices using chi-square (χ2), χ2/df ratio (<2.25), p value (>.05), and relative fit indices using goodness-of-fit index (GFI > 0.95), Tucker–Lewis index (TLI > 0.95), comparative fit index (CFI > 0.95), and root mean square error of approximation (RMSEA < 0.08). All statistical analysis was performed using SPSS statistical package 20.0 and Amos version 20.
Results
Of the 350 questionnaires distributed, 210 were returned fully completed (60% response rate). Thirty-five additional questionnaires were incomplete. Of the 210 participants, 136 were male (64.8%) and 74 (35.2%) female. Most work at UNTH (n = 118, 56.2%) and average number of years qualified is 7.6 years (SD = 4.78; range = 1-34 years). Oncologists represented only 7.1% of the population, general practitioners (GPs) 16.2%, and other specialties 76.7%.
The research framework of this study consists of three directly measured (ATT, SN, and PBC) and three indirectly measured (ATB, NB, and CB) exogenous variables. It also consists of two endogenous variables (intention and behavior). The mean values of the directly measured exogenous variables, including intention, ranged from 5.39 to 6.54 with standard deviations ranging from 0.84 to 1.28. The indirectly measured variables had means ranging from 13.09 to 49.07 (SD = 11.2-30.09) due to the multiplicative approach used to calculate the measurement scale (Francis et al., 2004). Mean scores were highest for both directly and indirectly measured attitude indicating that Nigerian doctors consider lifestyle counseling for cancer patients to be a worthwhile behavior. Test for normality using the Shapiro–Wilk test indicates normal distribution of data (p values > .05) for the indirect TPB measures but not the direct measures.
As recommended by Francis et al. (2004), bivariate correlations between the direct and indirect measures of TPB were carried out to determine the content validity of the indirect measures. Due to the violations of the assumptions of normality and linearity by the direct measures of TPB, Spearman Rank correlation method was employed with significant correlations observed between directly measured attitude and indirectly measured attitudinal belief (r = .468, p < .01). Direct (SN) and indirect (NB) measures of social norms were also significantly correlated (r = .136, p < .05); however, no significant correlation was observed for both the direct (PBC) and indirect (CB) control measures.
Convergent Validity
Upon conducting CFA, convergent reliability of the measurement items were assessed. Convergent validity establishes that measures that should be related are in reality, related. According to Fornell and Larcker (1981), this can be assessed based on item reliability of each measure, reliability of each construct, and the average variance extracted (AVE). Item reliability was assessed based on the factor loading of each item on its underlying construct. In this study, the “cut-off” point chosen for significant factor loading is 0.30 based on our sample size of 210, a recommended minimum by Hair, Black, Babin, Anderson, and Tatham (2006). Construct reliability was measured using composite reliability (CR), AVE, and Cronbach’s alpha with values of .6, .5, and .6 or higher, respectively, deemed significant (Fornell & Larcker, 1981; Nunnally, 1970).
As shown in Table 1, the remaining number of items for each construct is as follows: Attitude (two items), SN (two items), PBC (two items), Intention (three items), ATB (three items), NB (four items), and CB (zero items). Control belief (CB) was excluded entirely from further analysis of the indirect TPB model as the factor loadings of its observed variables were too low and it had no statistically significant correlation with other latent variables in the model.
Confirmatory Factor Analysis.

Note. AVE = average variance extracted.
The AVE for PBC and NB were slightly below 0.5, suggesting that the latent factors may not be well explained by their observed variables. Otherwise, all requirements for convergent validity of the proposed constructs are adequate. Cronbach’s alpha for the indirect measures were not calculated as people can logically hold both positive and negative beliefs about the same behavior, thereby making it inappropriate to assess their reliability with an internal consistency criterion (Ajzen, 2006; Francis et al., 2004).
Discriminant Validity
This establishes that measures which are not supposed to be related are in reality, not related. In particular, the variance shared between a construct and any other construct in the model, should be less than the variance that construct shares with its indicators (Fornell, Tellis, & Zinkhan, 1982). In this study, discriminant validity was assessed by comparing the square root of the AVE for a given construct, with the correlation between that construct and other constructs (Hair, Black, Babin, & Anderson, 2010). A significant result, suggesting that a construct is more strongly correlated with its indicators than with other constructs in the model, is obtained when the square roots of the AVEs are greater than the interconstruct correlations. As shown in Table 2, all proposed constructs had satisfactory discriminant validity.
Discriminant Validity.
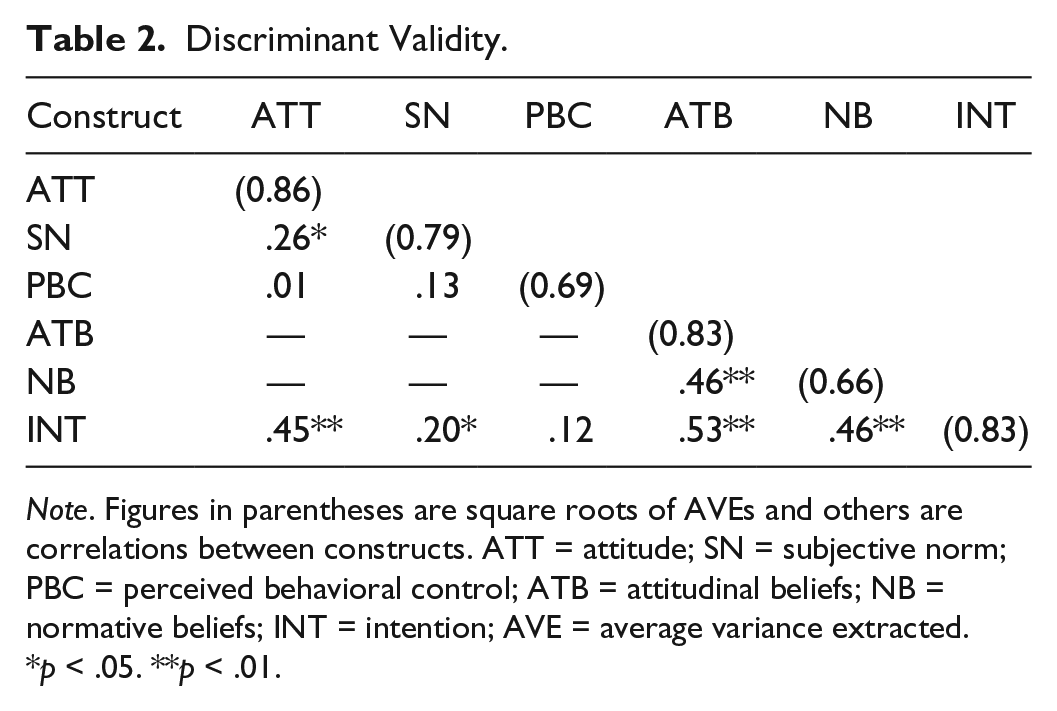
Note. Figures in parentheses are square roots of AVEs and others are correlations between constructs. ATT = attitude; SN = subjective norm; PBC = perceived behavioral control; ATB = attitudinal beliefs; NB = normative beliefs; INT = intention; AVE = average variance extracted.
p < .05. **p < .01.
Goodness-of-Fit Indices
Goodness-of-fit indices for the CFA of the direct TPB measures were χ2/df = 30.12/22 = 1.37; p value = .12; GFI = 0.97; TLI = 0.98; CFI = 0.99; RMSEA = 0.04. Indices for the CFA of indirect measures were χ2/df = 56.46/32 = 1.76; p value = .005; GFI = 0.95; TLI = 0.96; CFI = 0.97; RMSEA = 0.06. The CFA results are satisfactory and suggest that the linear structural model is appropriate for our data (Hair et al., 2006; Hu & Bentler, 1999).
Structural Model
Power analysis for the SEM(s) was calculated based on the number of latent and observed variables in each model, the anticipated effect size, desired probability, and statistical power levels (Cohen, 1988; Soper, 2014). The recommended minimum sample size to achieve a power of 0.80 for the indirect TPB model structure was 116 participants which is well below our study sample size of 210. However, the direct TPB model would have required 288 participants.
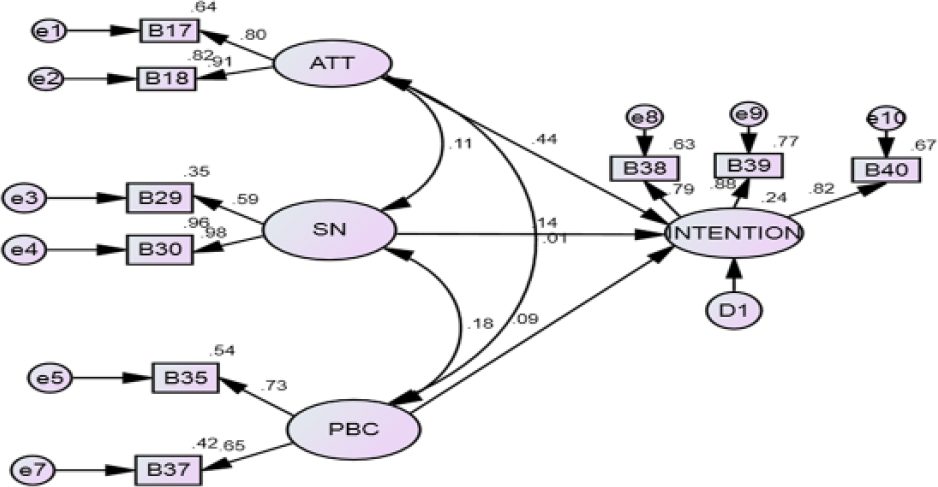
The SEM results and explanations are based on the final or generating structural models after the CFA. However, the hypothesized models for both the direct and indirect models are presented in Figures 1 and 2, respectively, to provide a clearer picture of the modeling process. Measured variables with low factor loadings in the hypothesized models were excluded, and the multivariate Lagrange Multiplier (LM) test—a modification index indicating possibilities for improving model fit—was also employed to decide which variables significantly improve model fit.

Hypothesized direct model.
Hypothesized indirect model.
The final direct model (Figure 3) had a reasonably good fit with the absolute fit (χ2), p value > .05. Only attitude had a significant direct effect on intention (standardized estimate [SE] = .44, p < .001) to provide lifestyle counseling. SN and PBC were not significantly related to intention. This contradicts previous findings which identified both social referents influence and control factors as key predictors of behavioral intention (Ajzen, 2002). Approximately 24% of variance (R2) of intention was explained by the three latent variables.

Final direct TPB model.
The final indirect model included only attitudinal belief and normative beliefs. Though the p value for the χ2 of the model was <.05, the model was not rejected as absolute fit p value is always likely to be small for large enough samples (Collins & Carey, 2007). Other relative goodness-of-fit indices were adequate (Figure 4). As observed in the direct TPB model, ATB (SE = .40, p < .001) was the best significant predictor of intention to provide lifestyle counseling. NB also significantly predicted intention (SE = .27, p = .004) unlike SN in the final direct model. The proportion of variance (R2) in intention explainable by ATB and NB is approximately 33%.

Final indirect model.
Predicting Behavior
According to the TPB, behavior is expected to be predicted by intention and PBC (Wade et al., 2010). However, behavior was excluded from the SEM analysis as it was assessed using only one question with a yes/no response and so cannot be accurately estimated using Amos (Albright & Park, 2009). Logistic regression of behavior on intention, PBC, and control beliefs was conducted and indicated intention as the only statistically significant predictor of behavior with odds ratio (OR) of 2.231 and 95% confidence interval (CI) = [1.058, 4.706] (p < .05). This suggests that the odds of providing lifestyle counseling among respondents with high intention are 2.1 times greater than the odds for those with low intention. PBC and CB were not significantly associated with behavior.
Discussion
In this study, we assessed the ability of the TPB to predict intention and lifestyle counseling behavior among doctors. To our knowledge, this study is the first to assess lifestyle counseling behavior for cancer survivors among physicians. Previous studies have examined other health behaviors in relation to cancer survivors but not physicians (Graves, 2003; Jones et al., 2005). Overall, our results showed that TPB constructs integrated into the structural models accomplished model fit and showed significant direct effects on intention.
This study included both direct and indirect measures of TPB, a controversial issue in the operationalization of the theory. Direct measures of TPB have been proven effective in predicting intention in many studies (AL Ziadat, 2014; Wade et al., 2010). Indirect measures have also been evidenced as providing insight into the underlying cognitive foundation of each TPB construct (Giles et al., 2007; Valois, Desharnais, Godin, Perron, & Lecompte, 1993). However, Francis et al. (2004) recommends that both measures be included in TPB studies as they are expected to be positively correlated when measuring the same construct.
In both the final direct and indirect TPB models, results indicated that attitude best predicted intention. This result is similar to those of past studies (AL Ziadat, 2014; Collins & Carey, 2007; Tan, 2013). This indicates that those with positive attitude are likely to engage in lifestyle counseling for cancer patients.
Interestingly, subjective norm predicted intention in only the indirect TPB model but not in the direct model. This attests to the recommendation that both measures be used as neither approach is perfect (Francis et al., 2004). The result implies that while doctors may believe counseling cancer patients to be a worthwhile behavior, social referents including colleagues and patients among others may have an influence on their intention to do so.
Perceived control had no significant effect on intention in either structural model, making it the only aspect of TPB that was not confirmed in this study. PBC was, however, found to have moderate significant correlations with SN in the final direct model. This provides empirical evidence that it is an important extension of TPB. Also, this correlation may have suppressed the effect of PBC on intention and so should not be ignored (Collins & Carey, 2007; Wade et al., 2010).
Both direct and indirect measures of PBC also had no significant association with actual counseling behavior. This result is somewhat surprising in light of previous research that found PBC to be a significant predictor of intention and behavior (AL Ziadat, 2014; Jones et al., 2005).
Intention was a significant predictor of behavior, replicating results in previous studies (Ajzen, 2002; Collins & Carey, 2007; Downs & Hausenblas, 2003; Tan, 2013). Specifically in this study, stronger intentions to provide counseling were predicted by more positive attitudes and possibly the positive influence of social referents regarding lifestyle counseling. Thus, doctors acknowledged feeling relatively positive about providing lifestyle counseling but also indicated that the opinion of social referents may influence their behavior. It is worthy of note that 72.9% of participants reported providing lifestyle counseling to those diagnosed with cancer in the past. This finding corresponds with that of the pilot study and raises the possibility that past behavior may influence future behavior (Collins & Carey, 2007; Oluka, Apio, et al., 2014; Ouellette & Wood, 1998).
Comparing the R2 results of the final TPB models, the indirect model explained 9% more variance in intention than did the direct model. Based on this finding and the fact that only the indirect model was able to show significant direct effect of SN on intention, it may be surmised that the indirect model in this study may be statistically superior to the direct model in predicting lifestyle counseling behavior.
Ultimately, the application of TPB to understand counseling behavior showed that intention was mediated by attitude and subjective norm; and actual counseling behavior mediated by intention. As such, attitude and subjective norm are appropriate modifiable targets to increase lifestyle counseling intention and behavior among doctors. The results also suggest that Nigerian doctors of various specialties are willing to contribute to cancer care in the face of limited oncology specialists. The challenge is to develop and implement strategies to help doctors maintain this positive intention and actually translate it into practice during treatment consultations. As lifestyle counseling is probably the easiest and least expensive aspect of cancer management, development of strategies to maximize the behavior should be prioritized. For example, attitude and SN can be improved by training or providing doctors with resources that would improve their knowledge and awareness on the benefits of healthy lifestyle changes. In addition, the national medical council (or/and other influential bodies) endorsement could make provision of lifestyle counseling more likely. Development of a lifestyle counseling intervention may provide the much-needed improvement in cancer outcomes for patients in Nigeria and other low/middle-income countries.
Some limitations of this study deserve mention. Actual counseling behavior was assessed with only a single question on past provision of lifestyle counseling which may have been insufficient to fully assess the construct. Next, our study sample size of 210 did not ensure adequate power to optimally test the direct TPB model; thus, future studies using SEM to replicate this study should aim for a larger sample size. Furthermore, the current study population consisted of doctors in one city in Nigeria and may require replication in several other cities to enhance generalizability of the results. Finally, we used a cross-sectional study design and therefore cannot infer causation.
Conclusion
Despite the limitations in this study, the TPB model proved effective in predicting intention and lifestyle counseling behavior for cancer patients among medical doctors. The findings suggest that theory-based interventions focused on enhancing attitude, subjective norm and intentions may have positive impacts on lifestyle counseling among doctors.
Future research may assess strategies to improve doctors’ intentions to provide counseling. Also, a lifestyle counseling intervention for cancer survivors in general practice is warranted.
Clinical Implications
This study recommended provision of lifestyle counseling in routine cancer care as a feasible self-management strategy which will improve the quality of life and overall survival of Nigerian cancer patients, while costing little or nothing. The results provide evidence that Nigerian doctors of various specialties are willing to contribute to cancer care in the face of limited oncology specialists. However, strategies to improve physician’s attitude and influence of social referents on lifestyle counseling behavior may be required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.