
Abstract
Cancer is the most dreaded and chronic disease with its treatment lasting almost lifelong with an uncertainty of cure. This not only adversely affects the quality of life among patients but also poses a psychosocial burden among family members, especially caregivers of the patient. This study was conducted with the objectives to assess the psychosocial burden on caregivers of cancer patients and to find out the association of various sociodemographic characteristics with the level of burden among caregivers. Caregivers of 205 cancer patients were interviewed. Information on sociodemographic characteristics of caregivers, cancer details of patients, and psychosocial burden among caregivers was collected using Zarit Burden Interview (ZBI) scale. Descriptive statistics were used to analyze the baseline data. Chi-square test was done to find out the association of burden with various sociodemographic and disease variables. A p-value of <0.05 was taken as statistically significant. The median (interquartile range) ZBI was 20 (10, 34). Fifty percent of the caregivers had no or minimal burden and only 2% had severe burden. Age of the caregiver was a significant determinant of their psychosocial burden.
Introduction
According to National Cancer registry in India, cause of cancer is multifactorial, burden of cancer is multidimensional, and treatment is multidisciplinary (Taneja, 2011). It is the second leading cause of death worldwide. Nearly one in every six deaths is due to cancer (Plummer et al., 2016). According to National Institute of Cancer Prevention and Research, there are about 2.5 million people living with cancer in India (Cancer statistics, 2018). In 2016, about 813,000 patients died due to cancer (Dhillon et al., 2018). The number of cases of cancer detected in India is increasing every year without a significant increase in the number of specialized cancer hospitals (Lukhmana, Bhasin, Chhabra, & Bhatia, 2015).
Cancer is a chronic disease with its treatment lasting almost for lifetime. This leads to mental and social burden on the caregivers. Disease per se has bad impact on the family of the patient due to poor prognosis and lifelong treatment (Grunfield et al., 2004). It not only results in mental distress among the patients but also the prolonged treatment results in burden among the family members, relatives, and friends, especially if they are caregivers (Lukhmana et al., 2015). Recent advances in the treatment modalities have led to more ambulatory care on an outpatient basis. Impact of the disease and its management on an ambulatory basis increases patient’s dependency on caregiver for symptom management, treatment, monitoring of medication and adverse reactions, and other daily routine and moral support (Girgis & Lambert, 2009; Lewis, 2006; Lewis, 2009). The caregivers on the contrary are emotionally unprepared for the care (Girgis & Lambert, 2009). This makes them vulnerable to physical, psychological, social, and financial burden, which affects the respective dimensions of health. Caregivers cannot take sufficient time for themselves, are unable to attend social gatherings, and in some extreme cases, not even able to sleep properly (Girgis & Lambert, 2009). Advanced stage of cancer renders the patient even more dependent on caregivers (Delalibera, Presa, Barbosa, & Leal, 2015).
In developed countries, studies have focused on caregiver’s health perspectives. However, there is paucity of the same in developing countries. Various research studies have shown the association of burden of caregiver with age, gender, relationship to the patient, unemployment, income of the caregivers, lack of family and social support, duration and stage of disease, previous care experience, and care for another sick patient (Lee et al., 2013; Lukhmana et al., 2015). In Indian culture, mostly the care to patients comes from families, extended families, and other care providers (Isaac, 2016). This caregiver’s burden not only affects their behavior, health and mental status, but also indirectly affects patient’s health as well (Higginson & Gao, 2008). Literature review conducted in the scope of this study revealed limited previous literature assessing psychosocial burden among caregivers of cancer patients in India. Hence, we assessed the levels of psychosocial burden and associated factors among caregivers of cancer patients.
Materials and Methods
Study setting: Study was conducted in a tertiary care teaching hospital, which is a 600-bedded multidisciplinary specialty center well known for its medical expertise and quality of care at an affordable cost. The oncology unit has a hospital-based cancer registry since 2015. It caters to the population not only within the state but also from other neighboring states. Medical oncology, surgical oncology, and radiation oncology along with palliative care services are offered.
Study design: A hospital-based cross-sectional study
Study population: Caregivers attending patients at the time of data collection.
Inclusion criteria: Caregiver of the patient who consented for the interview.
Sample size: The sample size is calculated based on the previous study done by Kim and Schuz (2008), in which the proportion of caregivers with high burden was found to be 67.3%. Using the formula 4pq/d2 taking 10% as the relative precision and 95% confidence interval, the sample size comes to be 189; assuming 10% as non-response rate, 209 caregivers were approached.
Sampling: Non-probability sampling (Convenient sampling)
Study duration: Two months (April–May 2017)
Data collection tool: A pre-tested, pre-validated semistructured questionnaire was used. To assess the psychosocial burden Zarit Burden Interview (ZBI) scale was used. The questionnaire was translated and back translated in local vernacular language for translational validity. Questionnaire comprised the following sections:
Section A: sociodemographic characteristics, socioeconomic status was assessed using modified Kuppuswamy scale (Singh, Sharma, & Nagesh, 2017).
Section B: Disease details.
Section C: Burden on caregivers of cancer patient using ZBI scale.
ZBI: It is a brief 22-item instrument (Cronbach’s alpha: .92) It is a widely used instrument with excellent psychometric property. Each item is asked to the caregiver in the form of a sentence, and response is recorded using 5-point Likert-type scale ranging from 0 to 4. The following score range depicts the level of burden: 0 to 21 little or no burden, 21 to 40 mild to moderate burden, 41 to 60 moderate to severe burden, and 61 to 88 severe burden (Zarit, Reever, & Bach-Peterson, 1980).
Operational definition: Informal Caregiver: “A person who provides support and assistance, formal or informal with various activities to the person with long term conditions without financial remuneration” (Wajnberg et al., 2016).
Data collection methodology: After obtaining ethics committee clearance, permission from Medical Superintendent of the hospital was obtained before approaching the caregivers of cancer patients in the hospital (inpatient department [IPD], day care and outpatient department [OPD]). The purpose of the study was explained to them in their vernacular language, and a written informed consent was obtained.
Data analysis: Data analysis was done using SPSS version 25. Data were summarized using median and interquartile range (IQR), and percentages. Chi-square test was performed to find the association. p < .05 was considered as significant.
Results
A total of 209 caregivers were approached out of which 205 consented to participate in the study. Mean (SD) age of the caregivers is 42.4 (14.5) years. One fourth of them belonged to the age group of 40 to 49 years (24%), most of them were males (52%), married (76%), had a nuclear family (51%), were resident of rural area (50%), educated till high school (44%), employed (73%), belonged to a middle or above socioeconomic status as per Kuppuswamy scale (52%), had a below poverty line ration card (71%), and most of the caregivers were children of the patient (38%) as depicted in Table 1.
Sociodemographic Characteristic of Caregivers of Cancer Patients in a Tertiary Care Center in Coastal South India. a

Note. APL = above poverty line; BPL = below poverty line.
Numbers vary in different variables as those data were not available.
The mean (SD) age of the patients was 52.6 (12) years. Half of the patients belonged to age group of more than 50 years (56%), most of them were females (65%), had advanced stage of cancer (53%), were undergoing chemotherapy (39%), were diagnosed within past 6 months (53%), were availing the facility of OPD (56%), and receiving care from the caregiver since the time of diagnosis (53%), and mean (SD) time spent by the caregivers with the patients was found to be 19(6) hr (Table 2).
Characteristics of Cancer Patients and Their Disease Details.
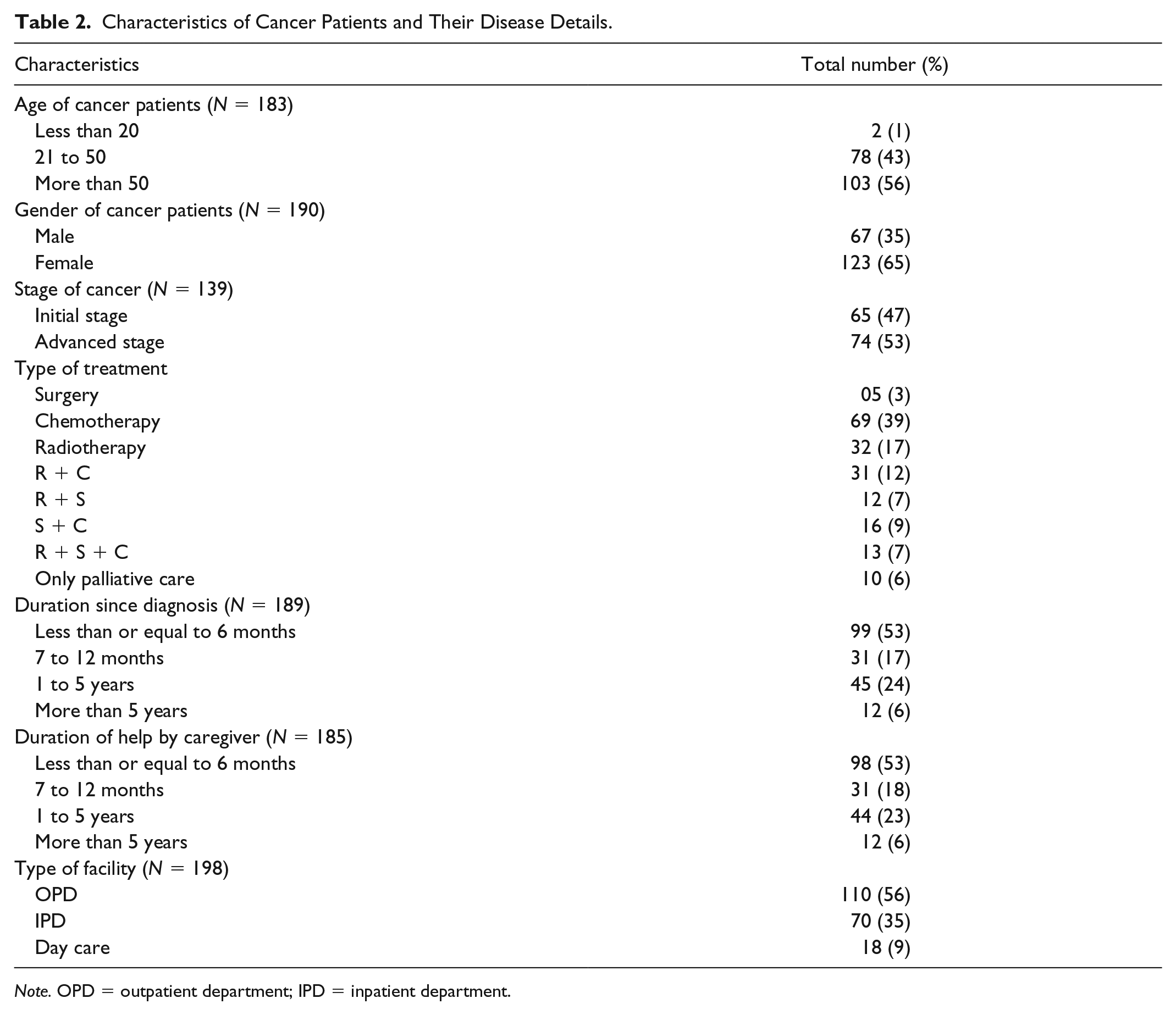
Note. OPD = outpatient department; IPD = inpatient department.
The median ZBI score obtained was 20 (10, 34), which corresponds to no to minimal burden. One third of the participants had mild to moderate burden. Moderate to very severe burden was seen in 16% (Table 3).
Caregiver’s Burden According to Zarit Burden Interview Scale.

Caregivers of patients who were of older age (56%), females (56%), and unemployed (58%) had moderate to severe burden, and those who were younger (63%), males (52%), and employed (55%) caregivers had no to mild burden. The age of caregivers was found to be significantly associated with the burden (p value: .039). None of the patient’s sociodemographic characteristics were found to be statistically significant with the levels of burden in caregivers (Table 4).
Association of Caregiver’s Burden With Their Sociodemographic Characteristics.

Note. APL = above poverty line; BPL = below poverty line.
Discussion
Diagnosis of cancer in one of the family members itself is a major event. It not only has a psychological impact on patient but also on the family. Currently in the Indian scenario, the level of the burden is not known. As the girth of the problem is not measured, there are no intervention under national programs to tackle this issue. Health care system provides curative services and less of preventive and counselling services that too only to the patient. Also, under the control program for cancer there is no provision of financial assistance to hire a formal caregiver for patient, in which case the responsibility comes to one of the kin, mostly spouses or children and in some cases friends and neighbors (Wajnberg et al., 2016). Hence, we conducted this study to highlight and assess the levels of psychosocial burden using ZBI among caregivers of cancer patient taking treatment from tertiary care hospital in Coastal South India.
In this study we found that almost half of the caregivers had psychosocial burden, with 14% with moderate to severe levels of burden. This finding shows that a significant number of caregivers are burdened because of caregiving and should be given attention at the earliest. Other studies elsewhere had varied levels of burden among the caregivers. One study conducted in Delhi found that most of the caregivers had no to mild burden (Lukhmana et al., 2015), and studies conducted outside India showed levels of mild to moderate degree of burden (Goldstein et al., 2004; Higginson & Gao, 2008). A case–control study done in Iran among caregivers of breast cancer showed highest levels of psychosocial burden, contrastingly a no to mild level was found among the caregivers in the studies by Bahrami and Farzi1 (2014) and Garlo, O’Leary, Van Ness, and Fried (2010). These different levels of burden might be because of difference in the health care services, health care seeking behavior, and family culture in different parts of the world. This also highlights the need for region-specific interventions to reduce the burden among caregivers.
The mean (SD) age of caregivers was 42.4 (14.5) years, similar to studies done in Delhi and Singapore (Lukhmana et al., 2015; Ting-Chua et al., 2016). However, the age group of caregivers in the western world is on the higher side (Goldstein et al., 2004). Age of caregivers was found to be significantly associated with levels of burden. We found that young caregivers had mild burden, whereas older caregivers had moderate to severe burden. Other study has also similar finding where they found age as one of the determinants of burden among caregivers (Hiremath et al., 2017; Souza et al., 2017). Older caregivers usually find themselves less energetic and they themselves have their own health issues, this might cause higher burden in older caregivers (Adelman, Tmanova, Delgado, Dion, & Lachs, 2014; Hiremath et al., 2017).
In this study, most of the caregivers were male (52%) similar to other studies (Bahrami & Farzil, 2014; Garlo et al., 2010; Idiok & Auarado, 2014). But most of the burden was felt by female. Women’s coping mechanism is not much effective to mitigate the burden. This could be because females have a larger role to play in a family and do multitasking. They also are emotionally weak as compared with males (Lutzky & Knight, 1994).
In this study, most of the caregivers were married (76) comparable with other studies (Chindaprasirt et al., 2014; Garlo et al., 2010; Goldstein et al., 2004; Liu et al., 2018; Lukhmana et al., 2015; Seibl-Leven et al., 2018). Married caregivers were less burdened than others (comprising unmarried, widower, and divorced). This finding was similar to that of other studies (Gaston-Johansson, Lachica, Fall-Dickson, & Kennedy, 2004; Park et al., 2012; Yusuf, Adamu, & Nuhu, 2011). Unmarried caregivers might face excess burden due to lack of support and lack of partner to share problems. In this study, most of the caregivers were employed (74%) as in other studies (Garlo et al., 2010; Liu et al., 2018; Lukhmana et al., 2015). Most of them were the sole earning member in the family. However, burden was more among the unemployed caregivers. This could be due to additional economic burden.
Conclusion
Half of the caregivers had some level of psychosocial burden. Age was one of the determinants which was found to be significantly associated with the burden of caregivers. Hence, we recommend a counseling center at all cancer hospitals and public health care facilities (those providing cancer-related services) for caregivers, which can reduce their psychosocial burden.
As it is a cross-sectional study, a temporal association cannot be established between factors determining the psychosocial burden among patients. This study was conducted in hospital setting where the patients who avail services hail from Karnataka and neighboring states of Kerala and Tamil Nadu, hence the results can be generalized to the same population. An analytical study design like case–control or cohort study should be conducted to find out the determinants of psychosocial burden among caregivers of cancer patients, preferably multicentric.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.