
Abstract
Family is a crucial factor to determine the amount, the duration, and the complexity of children’s sport activities. This study aims at comparing the beliefs concerning the involvement in sport activities among parents of children with Down syndrome (DS) and parents of typically developing children (TDC). A phenomenological theoretical framework was adopted to realize semistructured interviews with the parents. The participants were 35 parents: 19 with children and adolescents with DS and 16 with TDC. The main facilitation/barrier themes identified by the parents of children with DS were the family and the expert at Adapted Physical Activity (APA) instructors. Conversely, the parents of TDC identified social factors related to family as the only barrier. One of the issues that emerge from this study is the lack of home-based physical activity (PA) intervention programs aimed at involving families and children.
Introduction
The present study extends previous research, which aimed to explore parental beliefs concerning involvement, facilitators/barriers, and benefits of physical activity (PA) in young people with Down syndrome (DS; Alesi & Pepi, 2015). Specifically, the sample was enlarged to compare beliefs concerning the involvement in sport activities among the parents of children with DS and the parents of typically developing children (TDC).
Benefits of regular PA in people with DS have recently been addressed in several research (Alesi, Battaglia, et al., 2014; Golubovic, Maksimovic, Golubovic, & Glumbic, 2012; Palisano et al., 2001; Vogt, Schneider, Abeln, Anneken, & Strüder, 2012). Population with DS was found to have typically sedentary lifestyle, to participate less in sport activities, and to fail the Chief Medical Officer’s (2011) recommendation of 60-min moderate to vigorous PA a day (Frey, Stanish, & Temple, 2008; Gonzalez-Aguero et al., 2010; Phillips & Holland, 2011; Shields, Dodd, & Abblitt, 2009; Temple & Stanish, 2009). The direct consequence is the risk of intensifying clinical diseases by developing specific health-related complications such as the accumulation of bone mass, the type 2 diabetes, and motor functional impairments (Barr & Shields, 2011). Similarly, high levels of inactivity are stated in typically developing people despite data demonstrating physiological and psychological gains from PA. A 60% of inactivity is reported in Italy, as shown by data from the Special Eurobarometer 412 (March 2014) on the issue “Sport and Physical Activity.”
Nevertheless, the participation in sport activities is a multidimensional construct that involves a variety of facilitators and barriers. The first are positive factors enhancing the participation of people with DS in PA, for example, parental support, opportunities and programs for participation, accessible transportation, access to resources, and so on. The latter, the barriers, are adverse factors that limit this participation, such as narrowed information about PA; developmental delays; health problems; lack of transport and independence; beliefs about the disability of parents, coaches, and teachers; insufficient programs of social inclusion; few adapted equipment; and so on.
A number of research investigating factors underlined the engagement in PA by the adapted model of the Youth Physical Activity Promotion (YPAP) designed by Welk (1999). In the original model, higher predictors of child engagement in PA are the predisposing factors, such as child’s self-efficacy, attitudes and personal beliefs on PA, and physical self-competence. Moreover, reinforcing factors are conditions supporting PA behaviors in childhood, such as family, peer, and teacher/coach influence. Equally important are enabling factors such as the child’s physical skills and fitness level as well as the access to gyms and environment. Indirect influence is played by personal demographics, such as age, ethnicity, and socioeconomic status. Recently, an adapted model of the YPAP was developed by Downs, Boddy, Knowles, Fairclough, and Stratton (2013). It included enabling, predisposing, and reinforcing factors to PA for children with DS. Enabling factors involved environment, seasonal variation such as decrease in PA during winter months, access and transport, level of fitness and kind of activity (swimming, trampolining, dance, bowling), skills, and independence. Predisposing factors to PA engagement included enjoyment and play, social interaction, understanding of PA, and to be able to follow the instructions. Finally, reinforcing factors to PA were support and opportunities, and parents and care providers’ education about the importance of PA.
So, as for children with intellectual disability, three main category factors influence the engagement in PA: individual, familiar, and environmental variables (Downs et al., 2013; Mahy, Shields, Taylor, & Dodd, 2010). Individual characteristics include age, gender, the level of sport motivation, motor and cognitive abilities, and the kind and the severity of disability. Females, older individuals, and people with lower level of education and higher level of severity of disability are more likely to show decrease in variety, frequency, and duration of PA (Kristen, Patriksson, & Fridlund, 2002; Lippold & Burns, 2009). Therefore, personal factors which encourage greater participation are higher level of self-esteem or self-determination and mastery motivation to face challenging motor tasks (Badia, Orgaz, Verdugo, Ullan, & Martìnez, 2011; Hutzler & Korsensky, 2010; Kwan, Cirney, Hay, & Faught, 2013). Second, family variables that might encourage greater participation in PA are mainly emotional and economic support. The first arouses the children’s sense of competence and determination, while the latter allows to bear the costs of Adapted Physical Activity (APA) programs (George, Shacter, & Johnson, 2011; Trost, Kerr, Ward, & Pate, 2001). Finally, environmental characteristics might concern the availability of APA programs for children with DS (Badia et al., 2011; Barr & Shields, 2011). From now on, PA and APA will be used in an interchangeable way. As compared with traditional, the APA is an individualized PA that is specifically modified to address the needs of people with disabilities in accordance with the international classification of functioning (ICF) model (World Health Organization [WHO], 2001). It enhances the acceptance of individual differences by promoting the access to active lifestyle and sport encompassing gymnastics, dance, movement, exercise, sports, games, recreation, and physical education. Consequently, the APA employs adapted methods, such as peer tutoring, in the context of large size class teaching; adapted equipment and rules, such as bigger balls to enable bouncing; adapted environmental variables such as a lower net height for the volleyball; and qualified and expert at different kinds of disabilities coaches (Hutzler & Sherrill, 2007).
To sum up, personal, familiar, and environmental characteristics are interrelated by reciprocally reinforceing links. For example, the few number of gyms offering APA exercise programs can oblige families to move for long distances by enhancing the costs of transportation and, in the long run, decreasing the motivation to engage in PA.
However, barriers and facilitators are to be found by focusing on factors influencing parents’ decisions to stimulate their children in sport participation. Family support revealed to be a crucial factor influencing the choice of sport and leisure activities and the subsequent maintenance of compliance to exercise programs in the population with DS (Inglis, Lohn, Austin, & Hippman, 2014).
Menear (2007) investigated parental beliefs concerning PA needs in DS by interviewing parents of children with DS from preschool age to adolescence. She compared themes derived from four focus groups (preschoolers’ parents, elementary-age children’s parents, teenagers’ parents, and mixed age groups). Four themes were quite frequent across all four of the focus groups: (a) short- and long-term health benefits of PA on their children, (b) social benefits from relationship with peers, (c) sport opportunities to play an individual sport for teenagers, and (d) need to receive parent education concerning home-based PA intervention programs or to enhance community-based PA programs delivered for children with DS. So, Menear pointed out the need to educate parents and care providers on the benefits of PA and active lifestyle.
Based on these issues, this study aims at comparing the beliefs on facilitators and barriers to participation in PA among parents of children 1 with DS and parents of TDC.
A phenomenological theoretical framework was chosen to carry out semistructured interviews with the parents.
Method
Participants
The participants were 35 families subdivided into two groups: the first group was composed of 19 families with children and adolescents with DS and the second one was composed of 16 families with TDC. In the first group, there were 11 mothers and 8 fathers. The parents’ median age was 54.59 years (range = 37-69; ±8.82). The children were 10 boys and 9 girls with a median age of 20.94 years (range = 7-31; ±9.5). All the children had the diagnosis of Trisomy 21 and from early childhood had been engaged in structured speech therapy or psychomotor activities or music therapy. Parents’ inclusion criteria were (a) to be a parent of a child with DS, (b) to have present or past experience with their children’s engagement in sport activities, (c) to be an Italian speaker, and (d) to be Caucasian race.
In the second group, there were 13 mothers and 3 fathers. The parents’ median age was 40.54 years (range = 25-43; ±7.23). The children were eight boys and eight girls with a median age of 8.25 years (range = 5.2-10.11; ±4.5). All the children were typically developing. These parents were matched to those of the first group along with their children’s, here hypothesized, cognitive profile. We chose this criterion, despite their chronological age, because of the big difference in lifestyle among adolescents and young ones with DS and typically developing peers.
All the parents were from medium socioeconomic level.
The parents of children with DS were recruited through gyms or nonprofit associations offering support and community resources for people with DS and their families. They were invited to meet with researchers, to become familiar with the goals of the study and its procedures. Following this first meeting, the participation rate to the interview was of about 60%, while the parents of TDC were recruited through schools attended by their children.
Prior to the start of the study, appropriate local ethics committee approval provided by the University of Palermo was obtained.
Interview
A semistructured interview was developed to investigate the parental beliefs on facilitators/barriers to activities as well as physical and psychological benefits of sport in children.
First, data were collected on the children’s history and the family background by the evaluation of parameters such as parents’ academic history and jobs. Second, the interviewer followed a schedule of focused and open questions on facilitators/barriers and benefits of PA.
All the interviews were conducted by the same researcher and lasted no more than 25 min.
Data Analysis
All the interviews were transcribed to allow the thematic analysis of answers. Transcripts were read independently by two researchers to identify quotes revealing meaningful themes and remove inappropriate quotes. Consequently, the accepted quotes were clustered into categories highlighting common themes which were classified on the basis of their frequency of occurrence to identify the most important themes as facilitation or barrier. Similar procedure was followed for both the groups.
The identified themes were displayed into four figures: Two figures show facilitators to PA identified by the parents of children with DS and TDC (Figures 1 and 2), and two figures show barriers to PA identified by the parents of children with DS and TDC (Figures 3 and 4).

Facilitators to PA identified by the parents of children with DS.

Facilitators to PA identified by the parents of TDC.
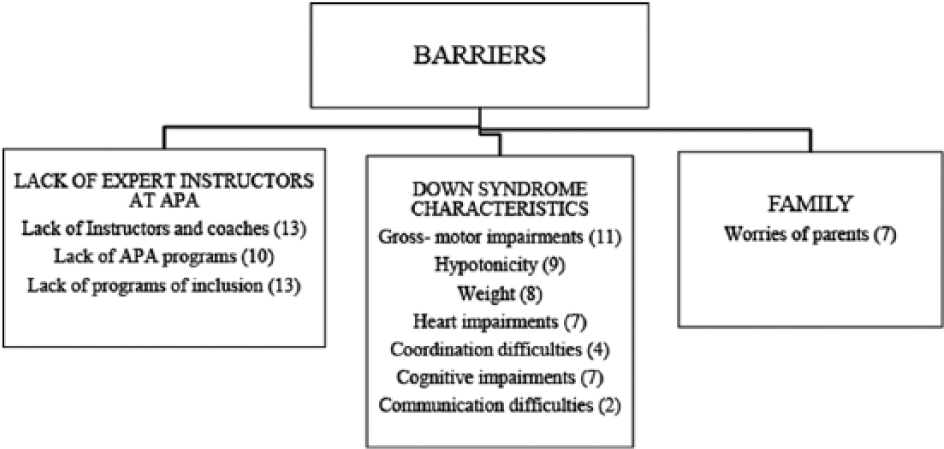
Barriers to PA identified by the parents of children with DS.
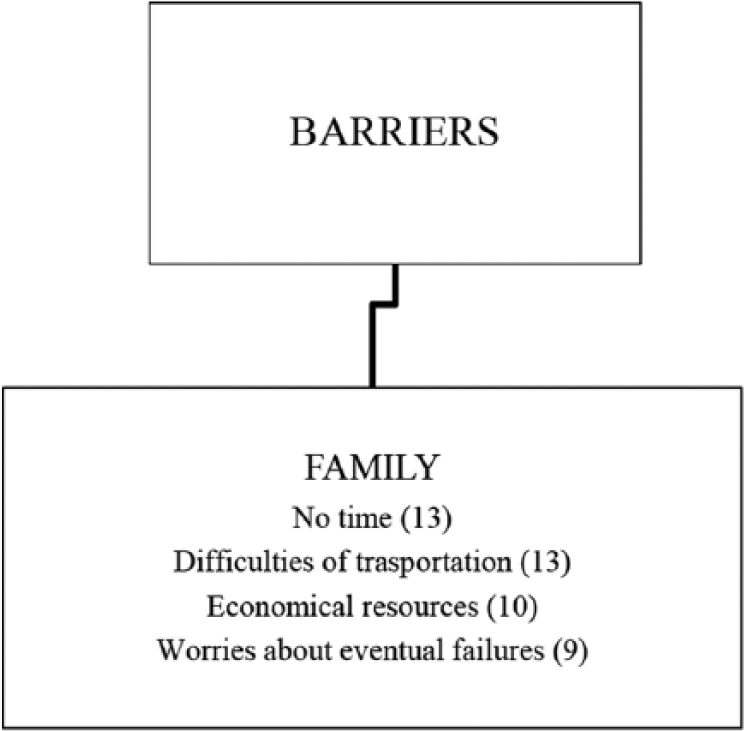
Barriers to PA identified by the parents of children with TDC.
Results
In the group of parents with children with DS, three main facilitation themes were identified: (a) the support from family, (b) the presence of expert at APA instructors and coaches and the availability of gyms, and (c) the challenging nature of sport activities (Figure 1).
The family revealed to be considered the first facilitator. The parents of children with DS showed to recognize the key role of siblings (11) and themselves (18) to motivate their children in sport participation. However, the majority (13) of them judged not relevant to their personal engagement as a model for children. The second facilitator was the availability of instructors able to train children with DS using the APA (18). This factor was strictly associated to gyms with specialized sport machines and without architectural barriers (13). The last facilitating theme identified in our interviews was the nature of PA: socialization (19), challenging (15), or enjoying (11). Sport activities were considered as an opportunity to experiment successes by facing up to themselves and the others with similar characteristics.
In the group of parents with TDC, two main facilitation themes were identified: (a) the support from family and (b) the characteristics of sport activities (Figure 2).
In this group, the family revealed to be considered the first facilitator. The key role of siblings (5) and themselves (16) to motivate their children in sport participation and to act as a model (11) was recognized. The second facilitator was the expertise of instructors at PA (14) as well as the nature of PA characterized by challenge (13), enjoyment (10), experience of success (13), and agonistic activity (5).
With concern to the barriers, the parents of children with DS identified three main themes: (a) the lack of expert at APA instructors and coaches, (b) the DS characteristics, and (c) the worries of parents (Figure 3).
Parents argued that the lack of adapted exercise classes (13) and programs of inclusion (10) for children with DS were the main barriers. Moreover, the scarce presence of expert at APA coaches was acknowledged (13).
Another significant barrier concerned the physical and medical characteristics of DS, such as gross motor impairments (11), hypotonicity (9), weight (8), heart impairments (7), and coordination difficulties (4). With regard to psychological domain, limited cognitive abilities (7) were considered as a barrier to the engagement in sport more than the limited communication abilities (2). Taken together, these factors increased the worries of parents (7) by creating an extra obstacle.
The parents of TDC recognized the family as the main barrier: no time to spend for sport activities (13), the difficulties of transportation (13), the economical resources (10), and the worries about eventual failures (9) (Figure 4).
Finally, similar physical and psychological benefits were advanced by all our interviewed parents (Figures 5 and 6). For the parents of children with DS, the physical benefits included reducing the obesity (12) and improving the motor coordination (9). The psychological benefits concerned increasing self-esteem (16) and self-image (13), and improving socialization skills (13) and cognitive functions such as memory and attention (8).

Benefits identified by the parents of children with DS.

Benefits identified by the parents of children with TDC.
For the parents of TDC, the physical benefits were reducing the obesity (15), improving the motor coordination (16), preventing the diabetes (15), and decreasing the insomnia (12). The psychological benefits included increasing self-esteem (16) and self-image (16), and improving socialization skills (16) and cognitive functions such as memory and attention (16).
Discussion
The main goal of the described study was to investigate the parental beliefs concerning facilitators/barriers and benefits of PA among the families of children with DS and the families of TDC.
On the whole, all the interviewed parents stated that family plays a key role to influence children’s engagement in PA. The parents of children with DS recognized the role of family both as facilitator and barrier to the participation of children in PA. This result is consistent with previous research, which demonstrated how parents deliver emotional/motivational and economic support. These are necessary to face challenging tasks as well as the transportation and the costs of activities (Badia et al., 2011; Downs et al., 2013; Mahy et al., 2010; Shikako-Thomas, Shevell, & Schmitz, 2013). The costs of sports programs, the equipment, and the transportation are expensive and rely on family available economical resourcess (Cordes & Howard, 2005; Van Naarden Braun, Yeargin-Allsopp, & Lollar, 2006).
However, as previously mentioned, family is considered as a barrier at the same time because of parental worries regarding gross motor impairments, hypotonicity, overweight, heart impairments, and limited cognitive and communication abilities linked to the specific disability of their children. All these factors may increase the family overprotection by limiting the participation to sport activity in their children (Frey et al., 2008). These parents, as opposed to the parents of TDC, did not recognize their role of model to influence the starting and maintaining compliance to exercise programs by their children. Research describes the family modeling as an important factor in determining the amount, the duration, and the complexity of their children’s sport activities (Temple & Stanish, 2011; Trost et al., 2001).
The study findings showed that the availability of expert at APA instructors and coaches is another main factor, both as facilitator and barrier, which plays a crucial role in the engagement in PA by children with DS. This staff was required to be specifically trained for the special needs of their children. Our parents identified that a support staff may initiate and sustain the participation in PA over the time. These findings are in agreement with other research that found a close relationship between the limited opportunities to participate in PA and the lack of specific training programs addressed to people with DS (Mahy et al., 2011). Moreover, this barrier is often strengthened by the lack of accessible services and facilities such as gyms and buildings with specialized sport machines and without architectural barriers.
Other differences in parental beliefs between our two groups emerged in the perception of features characterizing sport activities. The parents of children with DS evidenced characteristics such as socialization, challenge, and enjoyment. This result agrees with research on this issue. Socialization features derive from social opportunities in sport including cooperating with others, respecting rules, mastering new skills suitable for everyday life, experiencing personal achievement, and obtaining the encouragement of other people with the same disorder (Battaglia et al., 2013). PA is also judged enjoyable because of the opportunity to experiment leisure experiences and execute lovely and exciting exercises with music and games (Mahy et al., 2011). Nevertheless, the nature of sport allows to develop independence skills by facing challenging tasks and experimenting the sense of competence and self-empowerment (Badia et al., 2011; Downs et al., 2013).
The parents of TDC introduced in this category two new characteristics such as having successful experiences and participating in agonistic activities. This last result is explained as the product of stereotypes widely spread in Western societies which associate sport and values such as success, power, competition, and the importance of winning.
All our interviewed parents stated the physical and psychological benefits of PA. For the parents of children with DS, physical benefits were the prevention or the control of medical diseases such as obesity and motor coordination impairments. Specifically, the control of the obesity was considered the main benefit. It is now largely recognized how high levels of overweight and obesity among people with intellectual disability are closely associated to higher level of inactivity and unhealthy dietary practices (Battaglia et al., 2013). So, PA was acknowledged by parents as a worthy weight control intervention as an alternative to medicine therapies (Slevin, Truesdale-Kennedy, McConkey, Livingstone, & Fleming, 2014).
For the parents of TDC, physical benefits were more generalized. They not only included the prevention of overweight, but they also take account of other factors such as the prevention of diabetes and the decreasing of insomnia. On the whole, the great importance attributed by all parents to PA in the control of overweight confirms the awareness of the crucial role of family in the weight management by controlling the quantity and the quality of food, making the rules on food and meals, and outlining a healthy home environment (Prussing, Sobo, Walker, & Kurtin, 2005).
Psychological benefits concerned for all parents the increase of self-esteem and self-image, as well as the improvement of cognitive functions such as memory and attention. The main difference between the two groups was that the parents of children with DS attribute more importance to motivational benefits rather than cognitive improvements. In recent years, researchers have shown how regular PA is useful to face the fear of humiliation, the low athletic self-perception, and low self-efficacy because it allows self-evaluation by comparing oneself performance with others on a variety of physical and motor tasks (Alesi & Pepi, 2013; Pepi & Alesi, 2005).
Moreover, parents of TDC stated positive effects of PA on memory and attention. This is consistent with results from studies using magnetic imaging techniques (functional magnetic resonance imaging [fMRI]) which demonstrated how regular aerobic exercises modifie the brain function in the anterior cingulate cortex withimprovements in cognitive performances such as speed of processing, working memory, planning and control strategy employ (Alesi, Bianco, et al., 2014; Best, 2010).
On the whole, the current findings are added to a growing body of literature on the parental beliefs of PA as a key factor to contribute to well-being of their children. It is widely accepted by researchers and practitioners that a sedentary lifestyle is an important risk factor able to exacerbate medical diseases and enhance welfare assistance and use of medical services. So, high economic health costs are the consequence.
The main shortcoming of this study is the age range of the children which is widely disparate, with young adults included in the group of people with DS, and only children younger than teen age years in the TDC group. However, this may be the strength of this study as the results within each group are homogeneous. What parents think about PA may not be influenced by the age of their children but by their developmental age and disability. All parents recognized the physical and psychological benefits associated with children’s participation in PA. However, the primary benefits identified by the parents of children with DS concerned physical themes as reducing obesity or improving motor coordination as well as psychological gains like increasing self-esteem, self-image, and socialization skills. These parents wished for APA intervention programs that better met their children’s needs and encouraged their participation. On the contrary, the parents of children with TDC stated other benefits as decreasing the insomnia or increasing memory and attention. So the findings of this study, although preliminary, suggest some interesting implications on the educational field for future practice. First, it is crucial to organize settings aimed at encouraging the sport participation in typical and atypical population. Second, it would be decisive to develop specially designed programs and training aimed at increasing participation in PA involving both children with DS and their parents.
Footnotes
Acknowledgements
The author thanks all families who participated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.