
Abstract
Despite the detrimental impact of apathy on the cognition, functional abilities, and quality of life of older people, it is often under-rated and under-managed. This integrative review provides a comprehensive overview of the barriers as well as potential facilitators to optimal care for older adults with apathy. A systematic search for relevant literature using Whittemore and Knafl’s framework was conducted to identify factors that inhibit or facilitate optimal detection and intervention for apathy in older people with and without dementia. Four key barriers were identified including lack of standardized definition of apathy, lack of awareness, overlap with other disorders, and methodological limitations of clinical trials. Key facilitators included involvement of the dyad (persons with apathy and their families/formal caregivers), education, training and experience, and adoption of new and innovative method of screening and intervention. To provide optimal care for older people with apathy, there is need to adopt a multifaceted approach, including the development of precise definition of apathy, consideration of person-centered approach, caregiver training, and best practice guidelines for management of apathy. Future research and practice into effective interventions for management of apathy in older adults, and enhanced education and training for healthcare professionals, are needed to ensure quality of care for older adults with apathy.
Plain Language Summary
This study looked at the challenges and factors that can help improve the care for people with apathy. The researchers reviewed many previous studies to gather information. They found four main obstacles to effectively detecting and treating apathy: the lack of a clear definition, limited awareness about the condition, confusion with other disorders, and problems in the way research is conducted. The absence of a standard definition makes it hard to measure and understand apathy accurately. Many doctors and caregivers are not aware of apathy as a distinct problem, which leads to underdiagnosis and inadequate treatment. Apathy can also be mistaken for other conditions like depression, making it difficult to address properly. Additionally, the way studies are conducted can have limitations, such as recruiting enough participants or using unreliable tools for measurement. The study suggests a few ways to improve care for apathy. Involving both the person with apathy and their caregivers in the assessment process can provide valuable insights. Educating healthcare professionals and the public about apathy is crucial for better recognition and support. New screening and intervention methods, including innovative technologies, can help with more accurate assessments. The study has some limitations, such as a lack of diversity in the samples used and limited qualitative research. However, it provides important insights into the challenges and solutions for apathy care. It highlights the need for clear definitions, increased awareness, and better research approaches. The findings have practical implications for healthcare providers and call for further research in this field.
Introduction
Apathy is a prevalent behavioral and psychological symptom of dementia (BPSD) that is observed across various forms and stages of dementia, including mild cognitive impairment (MCI), Alzheimer’s disease (AD), frontotemporal dementia (FTD), and vascular dementia. It is also seen in other neurodegenerative and psychiatric disorders such as Parkinson’s disease (PD), schizophrenia, stroke, multiple sclerosis, traumatic brain injury, and major depression (Borsje et al., 2018; Ishii et al., 2009; Selbæk et al., 2013). Apathy is defined as a disorder of motivation or lack of interest characterized by diminished goal directed behavior, cognitive activity, emotional display, and social interaction (Marin et al., 1991; P. Robert et al., 2018). Thus, individuals with apathy typically have diminished motivation or interest in goal directed behaviors, such as initiating or participating in conversations, performing activities of daily living (ADLs), or seeking social activities (Mizrahi & Starkstein, 2007; Stanton & Carson, 2016). They experience loss of interest in more complex instrumental activities of daily living (IADLs) such as cooking, shopping, financial management, traveling, and medication management, and appear to be emotionally unconcerned about important life affairs (Marin, 1990; Mizrahi & Starkstein, 2007; Stanton & Carson, 2016).
Apathy has been investigated using various criteria and is considered a symptom or a syndrome (Harrison et al., 2016). Traditionally, apathy is thought to be a symptom of a wide range of disorders including neurocognitive, medical, and psychiatric disorders (Ang et al., 2017; P. Robert et al., 2018), but there is evidence to suggest that it affects healthy older adults, and hence it is considered a syndrome (Brodaty et al., 2010; Marin, 1991; Onyike et al., 2007). The prevalence of apathy can vary widely based upon the type of scale and population being studied. In one study, for example, 1.4% of individuals who are cognitively intact, 3.1% of those with a mild cognitive impairment, and 17.3% of those living with dementia were found to experience apathy (Onyike et al., 2007). It has also been reported that the prevalence rate of apathy among people with dementia can be as high as 84% (Zuidema et al., 2009), while ranging between 27 and 36% among those without dementia (Brodaty et al., 2010). Apathy is one of the mood disorders shown to lead to rapid cognitive decline and heightened risk for mortality among older people with dementia (Lavretsky et al., 2015; Nijsten et al., 2017; van Reekum et al., 2005).
Apathy has been associated with diverse adverse effects in older adults, especially those with dementia or other neurogenerative disorders, including poorer interpersonal relationships, and deteriorating quality of life (Mjørud et al., 2014; Palmer et al., 2010; van Almenkerk et al., 2015). Apathy can negatively impact caregivers (formal and informal), as people affected might be difficult to engage with and become uncooperative with care and may require more attention and supervision. This can culminate in increased workload, caregiver burden, and increased healthcare costs (Nijsten et al., 2019; Stanton & Carson, 2016).
Despite the prevalence and negative impacts of apathy on older people, it is often under-recognized and under-managed (Leone et al., 2013; Mele et al., 2019). However, when optimally detected, apathy is treatable pharmacologically (Beasley Cm et al., 1997; Blundo & Gerace, 2015; Frakey et al., 2012; Masanic et al., 2001; Padala et al., 2010, 2020; Rosenberg et al., 2013) and non-pharmacologically (Goris et al., 2016; Holmes et al., 2006; Theleritis et al., 2017). The purpose of this review is to describe the various factors that serve as barriers and facilitators to optimal care for people with apathy in terms of its early identification and management in older adults. A comprehensive understanding of these factors is essential to developing effective interventions and enhancing healthcare services for older adults with apathy (Mele et al., 2020). Further, this review aimed to inform practice recommendations for improvement in the care of people with apathy.
Methods
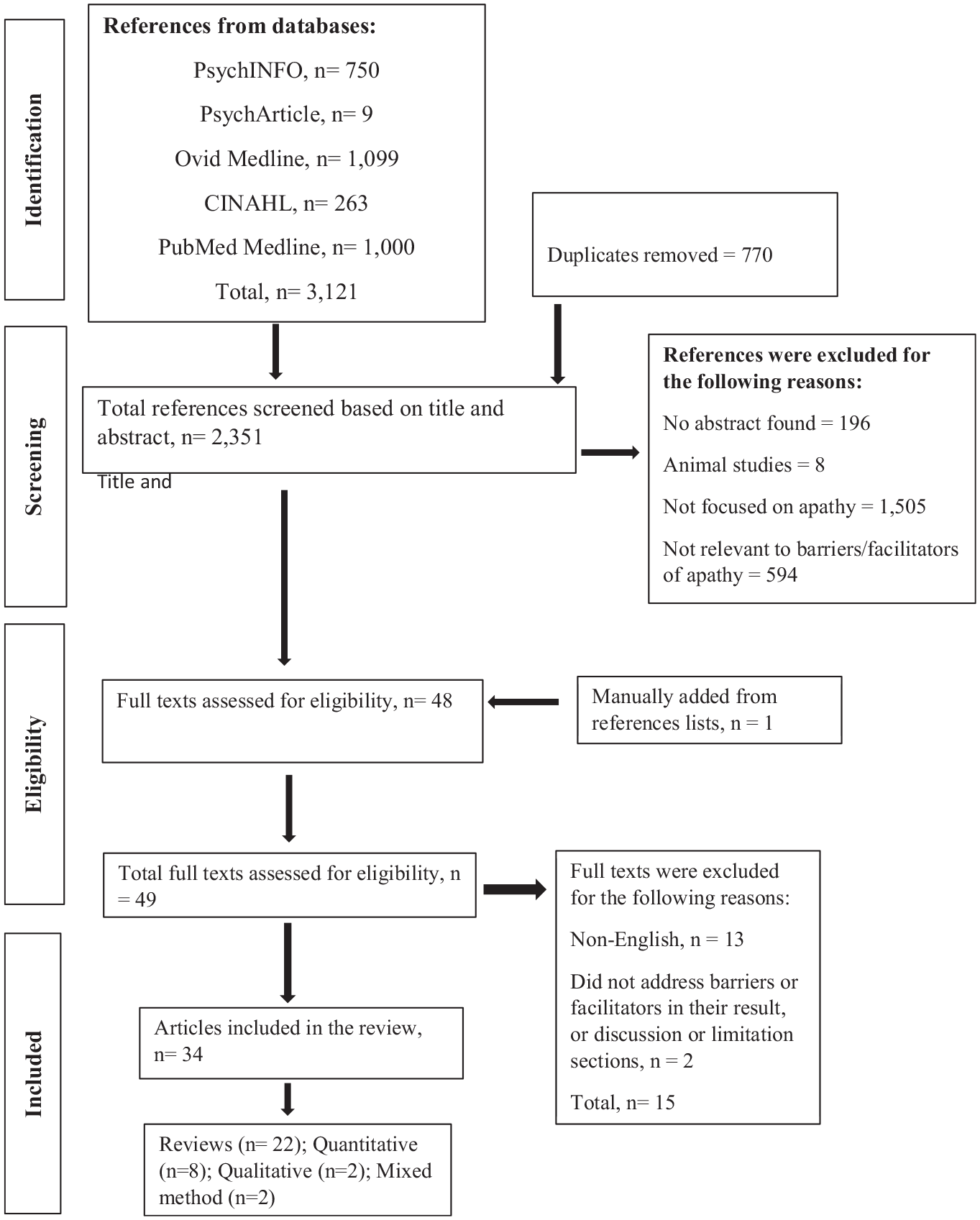
This review was guided by Whittemore and Knafl (2005) framework for integrative reviews. An integrated review allows for the integration of various types of methodologies and the synthesis of their findings including qualitative studies, quantitative studies, case reports as well as theoretical literature (Whittemore & Knafl, 2005). The framework consists of five phases, including problem formulation, literature search, data evaluation, data analysis, and data presentation (Whittemore & Knafl, 2005). The review followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) (see Figure 1) which provided an overview of the selection process and justified the exclusions made in the review (Moher et al., 2015).
PRISMA flow chart.
Problem Formulation
The overarching questions that guided the search were: (a) what are the barriers to optimal detection and intervention for apathy among older adults? and (b) what are the facilitators that have been or could be identified for optimal detection and intervention for apathy among older people?
Literature Search
Search Strategy
The search for relevant literature was conducted on March 14th, 2023, by one reviewer (AA) using five databases including PsychINFO, CINAHL, MEDLINE (OVID), PUBMED, and PsychArticles databases. The search terms were developed in consultation with the librarian who has an expertise in systematic searches. Search terms used consist of both keywords and Mesh terms and included “barrier*” OR “challenge*” OR “problem*” OR “hinder*” OR “motivator*” OR “driver*” OR “facilitator*” OR “enabler*” AND “older adult” OR “aged” OR “elderly” OR “geriatric*” OR “senior*” OR "older people" AND "apathy” OR "indifference" OR "lack of motivation” OR “lack of interest.” The selection process was recorded in the flow chart (see Supplemental File). The inclusion and exclusion criteria were also developed with help of a university health sciences librarian (see Table 1). No additional filters were applied.
Inclusion and Exclusion Criteria.

Data Evaluation
Study Selection
Title and abstract screening were performed by two independent reviewers (AA and SF). A third reviewer (DBL) resolved the conflicts that arose during the screening process. Full text screening was performed by one reviewer (AA) and accuracy check was conducted by a second reviewer (SF). Any papers directly or indirectly discussing barriers and/or facilitators encountered during research or assessment or intervention for apathy in clinical practice were included. Articles were also included if the sample consisted of people who had apathy aged 60 years and above and written in English language. Analysis of retrieved reference lists was also performed manually to find relevant articles that might have been missed during the full text screening. In total, 3,121 citations were retrieved, of which 770 were duplicates and 34 articles met the inclusion criteria (see Figure 1). The search results from all databases were directly imported into Endnote Version 20 (Peters, 2017).
Quality Assessment
Given that integrative reviews involve gathering of data from multiple sources, evaluating the overall quality of studies can be complex and papers do not necessarily need to be excluded based on quality criteria and assessment of data quality can be done based on the criteria relevant to the review (Whittemore & Knafl, 2005). As this review included qualitative, quantitative, mixed method and review papers, two quality assessment tools were used including the Critical Appraisal Skills Program (CASP) (2018) for systematic reviews and the mixed method appraisal tools (MMAT) (Pluye et al., 2018). Quality assessment was performed by two reviewers (AA and SF). Overall scores for these tools were interpreted using a 2-point Likert scale (high and low quality) as suggested by Whittemore and Knafl (2005). In this case, articles that scored ≤2 on the MMAT tool were rated as low quality while papers with a score ≥3 were considered high quality. With regards to CASP tool, articles with total score of ≤6 were considered low quality while papers with ≥7 were rated as high quality. Most studies that met the inclusion criteria were rated as high quality (see Table 2). In addition, given the heterogeneity of the selected studies’ methodologies, meta-analysis was not conducted.
Data Extraction Matrix.

Data Analysis
The ordering, coding, categorizing, and summarizing of data was performed using NVivo 12 software (QSR International, 2018) and Microsoft Excel software was used for organization. Identified barriers and facilitators were further reviewed, organized into themes, and conclusion drawn (Braun & Clarke, 2006). In addition, data pertaining to the study location, participants, and research design were extracted where applicable (see Table 3).
Critical Appraisal of Included Papers.

Y = yes, N = no, CT = can’t tell; H = high quality; L = low quality.
Data Presentation
Study Characteristics
Out of 3,121 articles that were retrieved, 34 studies met the inclusion criteria for this review (see Table 3). The studies came from three continents including Europe, Australasia, and North America. Most studies were reviews (n = 22), eight were quantitative studies, two employed mixed method and the remaining two were qualitative studies. Included studies were published between 2007 and 2023. The focus of most of the studies was on assessment and intervention for apathy. Only one study directly addressed barriers and facilitators to diagnosing and managing apathy. In studies that employed qualitative or quantitative methodologies or both, sample size ranged from 30 to 665 and included people with different types of diseases including dementia of all types, Parkinson’s disease, stroke, medical and psychiatric disorders. Some of the studies also include caregivers and healthcare practitioners including doctors, nurses, and allied health professionals such as technical staff, certified nursing assistant and activity staff.
Results
Barriers to Optimal Care for Older People With Apathy
The barriers to optimal care for older people with apathy were grouped into four main themes: lack of standardized definition of apathy; lack of awareness; overlap with other disorders; and methodological limitations of clinical trials (see Figure 2).
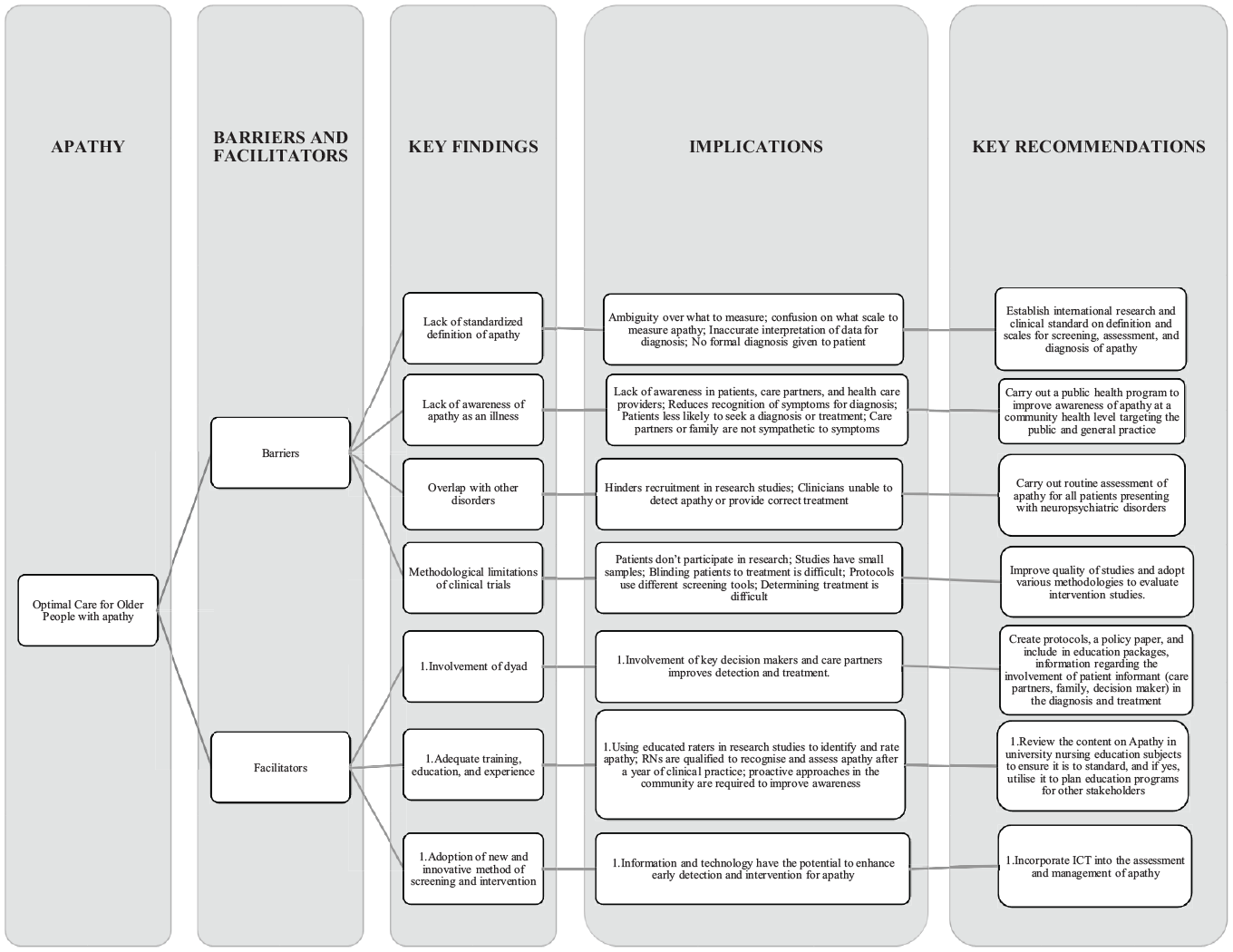
Diagrammatic representation of key recommendation for optimal care for older people with apathy.
Lack of Standardized Definition of Apathy
Lack of standardized definition of apathy were cited in most studies (Burgon et al., 2021; Caeiro et al., 2013; Chase, 2011; Clarke et al., 2011; Cummings et al., 2015; Drye et al., 2013; Herrmann et al., 2008; Leone et al., 2013; Matmati et al., 2022; Mele et al., 2019, 2020; Stanton & Carson, 2016). Despite the increasing effort to establish a commonly accepted diagnostic criteria for apathy (DCA), disagreement continues to exist over its precise definition and description (Drye et al., 2013; Lanctôt et al., 2021). In different fields, the words and meanings associated with apathy can vary and become isolated within specific areas of expertise (Thant & Yager, 2019). There is no category for apathy in the most recent edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V), and the likelihood of its inclusion in the next edition of the DSM is the subject of much debate (Matmati et al., 2022; Miller et al., 2021; Tay et al., 2021). Apathy is not listed in the International Classification of Diseases 10th Revision (ICD-10) (Drye et al., 2013; Stanton & Carson, 2016). The lack of standardized definition and conceptualization of apathy can cause ambiguity over what to measure and the appropriate scale to develop or use when measuring apathy in older adults. Consequently, apathy can easily be overlooked or some of its dimensions being missed during assessment (Clarke et al., 2011; Matmati et al., 2022). For example, participants in a qualitative study investigating the barriers and facilitators to diagnosing and managing apathy in persons living with Parkinson’s disease reported that they have never received or offered a formal diagnosis of apathy. In addition, the lack of unified definition of apathy can lead to inaccurate interpretation of data in terms of over-reporting or under-reporting of apathy (Mele et al., 2019). Caeiro et al. (2013), for example, noted that the wide range of prevalent rates of apathy (15.2%–71.1%) reported in their study was likely due to the absence of a clear definition and clinical criteria for apathy assessment. Similarly, Flavell and Nestor (2022) found a wide range in the prevalent rate of apathy in their study due to the variability in the assessment tools used to measure apathy. In a recent study by Dickson and Husain (2022), it was observed that despite the evidence for the social domain of apathy, most scales that have been used over the past three decades only focus on the cognitive, behavior and emotion domains of apathy implying that the social domain of apathy has been neglected over the years. Lanctôt et al. (2021) also observed that although there is a strong overlap between the Dementia Apathy Interview Rating (DAIR) scale (a rating scale for assessment of apathy in dementia) and DCA, some participants who scored high in DAIR were not considered apathetic by the DCA. The explanation was that the DCA does not include emotional domain of apathy while the DAIR does. The implication is that apathy in dementia can easily be missed when using the DCA.
Lack of Awareness
Lack of awareness of apathy as an independent disorder or a symptom that manifests in other brain disorders is a major barrier to the optimal detection and intervention for apathy (Drye et al., 2013; Jao et al., 2019; Leone et al., 2013; Mele et al., 2019). The lack of awareness is not limited to informal caregiver, but also healthcare practitioners and persons with apathy themselves (Jao et al., 2019). For example, Mele et al. (2019) identified that healthcare practitioners seldom offer a diagnosis of apathy because they do not recognize it as a distinct disorder and likewise, participants with apathy did not seek for a formal diagnosis of apathy or seek for treatment because they lacked insight and often perceive their symptoms of apathy as part of the natural aging process. Lack of awareness by informal caregivers can lead to apathy being misinterpreted as laziness or oppositional behavior (persistent patterns of hostility, and negativity) or part of aging process or response to other illnesses (Drye et al., 2013; Stanton & Carson, 2016), and consequently, they might find it difficult to detect or seek for interventions for their relatives with apathy.
Overlap With Other Disorders
The presence of neurodegenerative disorders (e.g., dementia and Parkinson’s disease) and psychiatric symptoms such as depression or anhedonia or cognitive impairment can serve as an impediment to the optimal detection and provision of appropriate treatment for apathy as these symptoms mimics the symptoms of apathy (Cummings et al., 2015; Drye et al., 2013; Jao et al., 2019; Mele et al., 2019). This was expressed by Cummings et al. (2015) who commented that the overlap of apathy with other neuropsychiatric disorders such as Alzheimer’s dementia and Parkinson’s disease was a significant confounder in their study and had limited the clinical benefits of the result of their findings. Drye et al. (2013) discovered that due to overlap of apathy with depression, excluding participants who are on antidepressants hindered recruitment and limited the generalizability of their results. This barrier was also highlighted in Mele et al. (2019) study where healthcare practitioners stated that due to the overlap of apathy with Parkinson’s disease, they were unable to detect or provide appropriate treatment for their patients who presented with apathy symptoms. In addition, overlap of apathy with depression in neurodegenerative disorders such as dementia, Huntington’s disease (HD), and Parkinson’s disease can lead to apathy being misconstrued as depression and subsequently, anti-depressant being used to treat apathy. However, research has shown that anti-depressants lead to worsening of apathy (i.e., selective serotonin reuptake inhibitors [SSRI]-induced apathy syndrome) (Padala et al., 2020).
Methodological Limitations of Clinical Trials
Methodological problems were reported frequently, with some authors noting lower than expected recruitment rate in randomized controlled studies (Cummings et al., 2015; Drye et al., 2013; Goris et al., 2016; Harrison et al., 2016; Manera et al., 2020; Starkstein et al., 2016; Tay et al., 2021; Theleritis et al., 2018). Low response rates resulted from participants’ refusal to participate in research and unavailability of suitable informants (Drye et al., 2013; Jao et al., 2019; Padala et al., 2010; Padala, Padala, Lensing, Jackson, et al., 2018; Starkstein et al., 2016); difficulty in randomizing or determining the suitable method to blinding participants to treatments (Clarke et al., 2007; Drye et al., 2013; Leone et al., 2013); use of variable scales to and difficulty in determining appropriate test treatment (Drye et al., 2013; Roth et al., 2007; Saredakis et al., 2020). For example, in a recent randomized controlled trial conducted by Padala, Padala, Lensing, Jackson, et al. (2018) which included a sample size of 60 male participants (treatment group = 30; placebo group = 30) to compare the effects of Methylphenidate (a drug commonly used in the treatment for apathy) with placebo, it was concluded that although, the treatment effect of Methylphenidate on apathy was statistically significant (p < .001), the small sample limited the clinical relevance and generalizability of the findings. Burgon et al. (2021) concluded that the lack of systematic approach and transparency when developing apathy scales made it difficult to draw valid conclusion about the content validity, reliability, and internal consistency of most of the scales used to measure apathy during clinical trials. Some authors have also alluded to the fact that methodological limitations of clinical trials have hampered the approval of licensed medications for the treatment of apathy in clinical settings (Chase, 2011; Steffens et al., 2022).
Facilitators for Optimal Care for Older People With Apathy
The facilitators for optimal care for older people with apathy were grouped into three themes: involvement of the dyad; education, training, and experience; and adoption of new/innovative method of screening and intervention (see Figure 2).
Involvement of the Dyad
Involving the persons who have apathy and informal/formal caregivers (dyad) in the assessment of apathy both clinically and in research is key to optimal detection and intervention for apathy (Clarke et al., 2007; Drye et al., 2013; Jao et al., 2019; Mele et al., 2019, 2020) because of the discrepancies that may occur between raters. For example, physicians’ ratings of the clinician version of the AES were found to be less accurate when compared to the informant version (AES-I) (Clarke et al., 2007). In that study, it was noted that physicians’ training and experiences with the use of apathy scale may have affected the reliability of apathy measurement and it was recommended that raters of apathy should know the person well or spend sufficient time to observe the person’s behaviors prior to assessment. Similarly, Jao et al. (2019) examined the relationships among AES ratings for three raters including families, certified nursing assistants (CNAs) or activity staff, and licensed practical nurses (LPNs). They found that families performed better at apathy ratings than LPNs and CNAs or activity staff. They also noted that family members are knowledgeable about the individual’s past behaviors and as a result, were able to accurately detect deviation in behavior. Jao et al. (2019) further recommended that family’s input should be sought during assessment of apathy as those affected may not be able to understand or answer some of the questions asked.
Education, Training, and Experience
Accurate assessment of apathy in clinical settings is dependent on the level of education, training, and experience of the raters (Carrozzino, 2019; Clarke et al., 2007; Drye et al., 2013; Jao et al., 2019). Clarke et al. (2007) alluded to the fact that raters of apathy should obtain a minimum of bachelor’s degree in health-related field to accurately assess apathy. Jao et al. (2019) argued that registered nurses (RN) are better positioned to assess apathy in long term care facilities than other healthcare staff, including LPNs, CNAs or activity staff, because of their educational attainment (typically 4 years of formal education) and experiences with clinical assessments. Admittedly, Carrozzino (2019) stated that some researchers who don’t have clinical experience tried to increase the value of the alpha coefficient of rating scales by adding as many questions as possible to their rating scales. Unfortunately, this resulted in rating scales with similar or unnecessary questions that do not provide any new clinical information (Carrozzino, 2019). Carrozzino (2019) recommended that clinicians with experience are needed to establish the clinical validity of apathy assessment tools. Furthermore, Clarke et al. (2007) recommended that for healthcare practitioners to accurately assess apathy, they need to have at least a year of experience working with people who have apathy and a minimum of 6 hr of experience in apathy assessment.
The need to increase awareness through education to overcome the barrier to the optimal intervention for apathy was highlighted by a few studies (Drye et al., 2013; Leone et al., 2013; Mele et al., 2019). As reported by Drye et al. (2013), educating the local community about apathy helped to overcome the barrier to participant’s recruitment for their study. Likewise, the focus group study by Mele et al. (2019) corroborated these findings, noting that educating healthcare practitioners about apathy as a symptom distinct from other neurodegenerative disorder, such as Parkinson’s disease, may help to increase awareness. Leone et al. (2013) observed that educating long term care staff was effective at raising awareness about apathy and led to a change in staffs’ perception that apathy is the least behavioral problem among the other neuropsychiatric symptoms resulting in implementation of evidence-based strategies to mitigate apathy.
Adoption of New and Innovative Method of Screening and Intervention
Over the past few years, researchers have come up with different ways to measure apathy. However, these methods are not very useful at detecting apathy optimally because they rely on human observation (König et al., 2014). To facilitate more objective measures of apathy, the use of information and communication technologies (ICT) was alluded to by some authors (König et al., 2014; Lanctôt et al., 2017; Manera et al., 2020). For example, in a narrative review of ICT tools for apathy assessment, König et al. (2014) commented that those technologies such as ambulatory actigraphy (a small device containing a piezoelectric accelerometer which tracks motor activity), automatic facial emotion recognition or electrodermal conduction could be better at detecting apathy than the conventional apathy scales including the AES and NPI. In terms of intervention for apathy, technology such as repetitive transcranial magnetic stimulation (rTMS) has been proposed (Lanctôt et al., 2017; Tay et al., 2021).
Discussion
Provision of appropriate care in terms of assessment and management of apathy in older people, especially people with comorbidities, such as dementia, stroke, schizophrenia, and Parkinson’s disease, can be challenging (Clarke et al., 2007). A clear understanding of the factors that inhibit or facilitate its optimal detection and intervention is necessary to prevent the negative consequences of apathy. As noted by many authors in this review, apathy has only been listed as a symptom in various disorders, including neurological, psychiatric, and medical disorders. The fourth and fifth Diagnostic and Statistical Manual of Mental Disorders (DSM-IV and DSM-V) have not provided a formal definition nor a universally agreed diagnostic criteria for detection and management of apathy in clinical settings (Clarke et al., 2011; Thant & Yager, 2019). It is also not listed as an ailment/disease in The International Classification of Diseases 10th Revision (ICD-10) (Drye et al., 2013; Stanton & Carson, 2016). The fact that apathy has not been widely accepted as a clinical condition that requires treatment has likely played a role in why there are varying terms and concepts used to describe it across different fields of study. For instance, in psychiatry, the terms “apathy” and “abulia" are commonly used to describe apathy (Thant & Yager, 2019, p.707). Meanwhile, in psychotic disorders, the terms “negative symptoms” and “avolition” are preferred (Thant & Yager, 2019, p.707). In cannabis and other substance use, personality, depressive, and psychotic disorders, the term “amotivation” is often used (Thant & Yager, 2019, p. 707). In ADHD and some learning disorders, the term “boredom” is more commonly used (Teixeira et al., 2021; Thant & Yager, 2019, p. 707). In the absence of formalized definition and conceptual operationalization of apathy, there continues to be lack of consensus on essential items to include in apathy scales for clinical diagnosis and research studies. Healthcare professionals may continue to face uncertainty over the right type of diagnostic tool to use when measuring apathy (Clarke et al., 2011). Inappropriate selection of apathy measurement scales can lead to inaccurate interpretation of research findings and clinical data and subsequently, flawed conclusions. To mitigate this inaccuracy, Harrison et al. (2016) suggested that a more rigorous approach is needed in evaluating apathy treatments. This includes better documentation of the study population, baseline apathy diagnosis and severity, and the consideration of confounding factors. Additionally, there should be a focus on both clinically and statistically significant effect sizes, utilization of apathy-specific measurement scales, caregiver input, and an adequate study duration to assess the sustainability of treatment effects and detect meaningful improvements (Harrison et al., 2016).
Furthermore, uncertainty over the best tool to select can lead to the abandonment of the existing apathy assessment scales by healthcare practitioners and increase their reliance on self-report or proxy account of apathy (Mele et al., 2019). Relying solely on family or proxy accounts or self-report of apathy may lead to inconsistent information and impose limits on the treatment provided to people who have apathy (Cummings et al., 2015; Jao et al., 2019; Mele et al., 2019). This reinforces the need to develop international consensus on the definition and conceptual operationalization of apathy.
The complexity of apathy, especially its similarities with other neuropsychiatric and neurodegenerative conditions, makes it crucial to distinguish it clearly from these disorders. Misunderstanding or misdiagnosing apathy can lead to unsuitable treatments, affecting care for older people with apathy. To address this misunderstanding, researchers have advocated for a more comprehensive approach to apathy assessment (König et al., 2014). This approach includes a blend of structured evaluations of cognitive functions to identify specific deficits, in-depth discussions with family or caregivers who can provide insights on behavioral shifts, and direct clinical observations to assess the patient’s real-time behavior (König et al., 2014). Additionally, a thorough review of the older persons’ medical history can offer insights into potential triggers or patterns of apathy (König et al., 2014; Manera et al., 2020).
Although this review identified education and training of healthcare staff as important elements in the optimal detection and intervention for apathy, chances are that apathy will be overlooked by healthcare staff after being trained. This may be due to what Villar et al. (2021) referred to as “common practices” (p. 614). Common practices are how staff are managing apathy in their day-to-day practices as opposed to best practices (how they think apathy should be managed) (Villar et al., 2021). Common practices are behavior-focused or no intervention strategies where care staff provide any kind of activity to stimulate people with apathy without considering their needs and personal preferences or ignore the situation and do nothing while best practices are person centered strategies. In their cross-sectional study involving technical staff (nurses, physiotherapists, psychologists, and occupational therapists) and care assistants, Villar et al. (2021) found that even though most health care workers recognize that person-centered care strategies are the best ways to manage apathy, they continue to implement common practices for addressing apathy. This will highlight the importance of considering the staff’s previous experiences and common practices when designing training programs (Villar et al., 2021). In other words, reflection-based training should be implemented.
The integration of ICTs, such as ambulatory actigraphy, has been proposed as a pivotal tool in the precise assessment of apathy (König et al., 2014; Kuhlmei et al., 2013). These technologies offer the potential to capture real-time data and provide insights that might otherwise be overlooked (Kuhlmei et al., 2013). However, a critical aspect that warrants attention is the influence of diurnal fluctuations on such measurements. Diurnal fluctuations refer to the inherent variations that occur between daytime and nighttime activities and behaviors. These fluctuations are primarily driven by circadian rhythms, which are the body’s intrinsic timekeepers governing our sleep-wake cycles, alertness, and overall activity levels (Adan & Guàrdia, 1993). It is noteworthy to mention that the impact of these circadian rhythms can be more pronounced in older people (Duffy et al., 2015). As people age, there might be alterations in their sleep patterns, activity levels, and responsiveness to environmental cues, all of which are regulated by the circadian system (Duffy et al., 2015). Consequently, when assessing apathy or any other behavioral or physiological parameter in older individuals, it becomes imperative to account for these diurnal variations. In light of this, any evaluation or intervention aimed at older people with apathy should be meticulously designed. It’s crucial to consider individual differences, not just in terms of their baseline apathy levels, but also in their daily rhythms. The timing of measurements and the nature of interventions should be tailored to each person, ensuring that the data captured is both accurate and representative of their true state. This approach not only enhances the validity of the findings but also ensures that interventions are more likely to be effective and beneficial for the target population.
Limitations of the Study
A limitation of the current literature review is that included studies tended to use focused homogenous samples that consisted of participants who had experienced with a specific health condition such dementia, stroke, and Parkinson’s disease. Therefore, the results described in this review may not be generalizable to the healthy older adult, underscoring the importance of including larger and more diverse sample populations. A further limitation includes the gap of in-depth understanding garnered from use of qualitative methodology. Of note, only one qualitative study directly addressed this topic. Some of the findings reported were extracted from either from the discussion or limitation sections of the included studies. As a result, the barriers, and facilitators discussed may not be exhaustive.
Clinical Implications
From a clinical perspective, findings of this study highlight the absence of a unified definition and conceptual operationalization of apathy, both of which should be incorporated into subsequent updates to the Diagnostic and Statistical Manual of Mental Disorders. Specific training/education on apathy assessment should be provided for healthcare staff working with older people including LPNs, CNAs and activity staff on how to accurately detect and manage apathy. For the training to be effective, resources should be standardized and accessible by adopting online format or a blend of online and offline method (Saredakis et al., 2020). Education should also be made freely available for informal caregivers and older adults on how to recognize symptoms of apathy. Since apathy is often associated with depression and dementia, older adults presenting with these symptoms should be routinely assessed for apathy. In addition, older adults with decline in functional abilities should be offered assessment for apathy. When assessing apathy in older adults and people with dementia, apathy specific scales such as the AES and LARS, should be considered given that these scales have sufficient reliability, content validity and internal consistency (Burgon et al., 2021). It is worthy of note that medication interventions for apathy should be tailored to the type of disorders associated with apathy as treatment options which are effective in one disorder may not be effective in another disorder (Azhar et al., 2022).
Implications for Research
Future research exploring apathy should focus on the efficacy of both pharmacological and non-pharmacological interventions for apathy using a rigorous clinical trial approach (Ferrero-Arias et al., 2011). More qualitative research is needed to increase understanding about individuals’ lived experiences of apathy. This may broaden understanding of apathy and help inform consensus on how apathy should be conceptualized and defined (Mele et al., 2019). In addition, longitudinal studies should be considered by future researchers to better understand the pattern of changes in individuals with apathy. This might help in drawing valid conclusions about effective care, preventative interventions, and treatment approaches for those experiencing apathy. In addition, the efficacy of ICT for apathy assessment needs to be further investigated and validated with larger population sizes and stronger methodologies (König et al., 2014). An automatized fusion of sensor measurements should be developed to capture all sub symptoms of apathy and provide immediate visual feedback to clinicians, caregivers, and patients (König et al., 2014). The integration of early intervention strategies, such as serious games or robotics, with ICT detection of apathy symptoms could further advance the field (König et al., 2014).
Recommendations
Based on the findings of this review, the following key recommendations are made to improve the optimal care provision for people with apathy:
Establish international research and clinical standard on definition and scales for screening, assessment, and diagnosis of apathy.
Develop a guideline on the prevention, assessment, and treatment of apathy among older adults.
Carry out a public health program to improve awareness of apathy at a community health level targeting the public and general practice.
Adopt multidisciplinary and person-centered approaches to assessing and managing apathy in older people.
Improve quality of studies, and the range of study methodologies which are accepted as clinically valid (RCTs are not the only reliable option).
Review the content on apathy in universities offering nursing and medical education subjects to ensure it is up to standard, and if up to standard, utilize it to plan education programs for other stakeholders.
Conclusion
Without a gold standard and universally accepted definition of apathy, its assessment and management remain complex and challenging. The findings of this review suggest that optimal detection and treatment can occur with increased effort at arriving at a consensus in the conceptualization of apathy and recognizing it as both a symptom and a syndrome. Interventions aimed at mitigating apathy for older people should specifically consider addressing these barriers by increasing awareness of the signs and symptoms of apathy as well as enhancing availability and accessibility to educational resources and technologies to support more accurate detection of apathy by healthcare providers.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241241882 – Supplemental material for Apathy in Older Adults With and Without Dementia: An Integrative Review of Barriers and Facilitators to Care
Supplemental material, sj-docx-1-sgo-10.1177_21582440241241882 for Apathy in Older Adults With and Without Dementia: An Integrative Review of Barriers and Facilitators to Care by Aderonke Agboji, Shannon Freeman, Davina Banner, Annie Duchesne, Joshua Armstrong and Melinda Martin-Khan in SAGE Open
Footnotes
Acknowledgements
Our gratitude goes to Trina Fyfe, the librarian, for her guidance during the selection of relevant keywords and appropriate databases for this review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
Not applicable
Supplemental Material
Supplemental material for this article is available online.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.