
Abstract
This study aimed to investigate the referrers (including educators) and reasons children were referred to an audiology clinic for central auditory processing (CAP) evaluation, to identify a referral pathway for listening problems and professional development needs. A case file audit was used to examine the intake questionnaire completed by 150 parents whose child was diagnosed with central auditory processing disorder (CAPD). School staff were the most common referrers, followed by medical/allied health professionals, and family members. The most common concerns leading to referral were literacy, speech, language, and academic underperformance, followed by hearing, listening, and processing difficulties and emotional-behavioral issues. Significant correlations were observed between the referral sources and concerns. Results suggest that CAPD is primarily conceptualized as part of a more general educational concern. Continuing education and informational counseling is required to ensure that CAP referrals continue to be appropriately made.
Keywords
Introduction
Concerns raised by children’s listening difficulties or underperformance at school prompt a range of referrals for special education, psychological, medical, and allied health evaluations. Less frequently, deficits in central auditory processing (CAP) are directly raised as a possible etiological basis for these difficulties, especially when hearing loss has been excluded as a possible cause. Yet, central auditory processing disorder (CAPD) is a diagnostic category associated with an array of difficulties in a variety of academic and life domains (American Academy of Audiology, 2010). This retrospective study investigates educators as a referral source for CAP evaluation and also presents a compilation of the other most common referrers and concerns that precipitate children’s referrals to an audiology clinic for CAP evaluation, resulting in an eventual diagnosis of CAPD.
Interest in CAPD is topical and has received significant attention from a variety of research and clinical perspectives. Although a universally accepted definition and set of diagnostic criteria are still lacking, audiologists primarily conceptualize CAPD as a perceptual disorder related to dysfunction of central auditory structures in the central nervous system (CNS; Stach, 2003). In this article, the American Speech-Language Hearing Association (ASHA) definitions of CAP and CAPD are adopted. CAP is
the auditory mechanisms that underlie the following abilities or skills: sound localization and lateralization; auditory discrimination; auditory pattern recognition; temporal aspects of audition, including temporal integration, temporal discrimination (e.g., temporal gap detection), temporal ordering, and temporal masking; auditory performance in competing acoustic signals (including dichotic listening); and auditory performance with degraded acoustic signals. (ASHA, 2005, p. 2)
CAPD refers to “difficulties in the perceptual processing of auditory information in the CNS as demonstrated by poor performance in one or more of the above skills,” despite normal peripheral hearing thresholds (Chermak, 2002, p. 2).
Debate about the definition, nature, and symptomatology of CAPD has undergone a fluctuating trajectory historically with a resurgence (particularly in the audiology literature) of CAPD as a distinct diagnostic entity. The heterogeneous nature of the extensive list of associated behavioral features has evoked criticism since CAPD defies definition and specification on the basis of a unique cluster of diagnostic signs reflecting some underlying mechanism (DeBonis & Moncrieff, 2008). For example, Ferguson, Hall, Riley, and Moore (2011) compared the communication, listening, and behavior of normally developing children to two groups of children, one group with specific language impairment (SLI) and one with CAPD. These authors concluded that the groups of children with SLI and CAPD displayed similar behavioral and parental report profiles, thereby suggesting that differential diagnosis based on their referral route rather than diagnostic outcome is impossible. Furthermore, high levels of comorbidity with other language, literacy, cognitive and behavioral disorders further confound attempts at delineating the boundaries of the impairment based on behaviors and symptomatology (Hamaguchi & Tazeau, 2007).
CAPD is a controversial label and, although it is a preferred diagnostic label to other labels such as language and phonological disorders (Kamhi, 2004), it has attracted debate and criticism among professionals. Foremost among these controversies is whether CAPD is primarily an auditory deficit or attributed to or comorbid with other deficits such as language processing (Medwetsky & Musiek, 2011) or attention (Moore, Ferguson, Edmondson-Jones, Ratib, & Riley, 2010) deficits. Burkhard (2009) acknowledges that there is diversity in the field of CAPD since there is a lack of consensus regarding its definition, the battery of tests used for its diagnosis and the rehabilitation measures used for its management. Notwithstanding the controversies surrounding the label, CAPD is considered a complex multifaceted auditory deficit usually diagnosed by an audiologist using specific audiological tests designed to assess CAP skills (such as defined in the ASHA, 2005, definition), although its implications converge with domains addressed by numerous medical and allied health professionals (M/AHP), including medical specialists (such as otolaryngologists or neurologists), speech-language pathologists (SLPs), occupational therapists, psychologists, and educators.
Behavioral characteristics associated with the impairment are descriptive and exhaustively described, and include difficulty comprehending speech in competing or reverberant environments, requests for repetition of information often using nonspecific clarification requests, misunderstanding messages, inconsistent or inappropriate responses, delays in responding to oral communication, difficulty following complex auditory directions, difficulty with sound localization, inattentiveness, distractibility, and literacy difficulties (Hamaguchi & Tazeau, 2007). A point of confusion for professionals (specifically those working in a school environment) is the issue of exclusivity, since many of the above behavioral manifestations may also be evident in children with other disorders such as those with language difficulties, memory or attention deficits among many other disorders. Ehren (2009) suggests that in many instances, the curriculum demands facing school aged children are fundamentally based on language knowledge and skills, and may contribute to a child’s listening and auditory processing difficulties leading to difficulty with separating out the symptomatology “supposedly” specific to CAPD. Moreover, comorbidity of CAPD with other disorders such as language-learning difficulties may result in difficulty with differential diagnosis and needs to be accounted for in the assessment of children suspected of having CAPD so that appropriate diagnoses can be made and management can be sought (Geffner & Ross-Swain, 2007).
CAPD as a modality specific perceptual dysfunction as questioned by Cacace and McFarland (2005) has been widely challenged (Katz & Tillery, 2005; Musiek, Bellis, & Chermak, 2005; Rosen, 2005). The diversity of functional deficits that make up CAPD and associated deficits across life domains necessitate a holistic approach to identify reasons for referral for CAP evaluation. Interacting language, literacy, and auditory processing systems contribute to the complexity of identifying specific behaviors leading to a CAPD diagnosis. Numerous scenarios are therefore possible. It is possible that children who will eventually be diagnosed with CAPD have poor listening skills and poor skills in other domains such as language, in which case, it is difficult to separate CAPD symptomatology from symptoms arising from other difficulties. CAPD thus may be present but overlooked. It is also possible that children’s good language or literacy competency may mask potential CAP symptomatology and deficits (Heine & Slone, 2008). The interacting systems of language, literacy, memory, and attention stress the need for further investigation in regard to the referral concern and the referral sources best positioned to detect signs and symptoms that warrant further investigation.
It is anticipated that a wide variety of people in the educational system and community (including family) would refer a child to an audiologist and possibly other M/AHP for CAP evaluation. Listening or hearing difficulties (Johnson, Benson, & Seaton, 1997), difficulty with the acquisition of literacy as in reading and/or spelling, learning difficulties including suspected dyslexia, slow academic progress, or language difficulty may alert educators about the need for further investigation of CAP skills. Although teachers are potentially excellent referral initiators for CAP testing as they observe children’s listening and academic skills and behaviors in a variety of listening environments, they may not have the knowledge to pinpoint CAPD as a possible feature of children’s language-learning and literacy-based problems, which could lead to under referral for CAPD evaluation.
Allied health professionals such as SLPs may also conceptualize CAPD as another disorder such as receptive language disorder or be unable to differentiate CAPD from another disorder (Heine, Joffe, & Greaves, 2003). Hence, they may not be referring children with potential CAPD to an audiology clinic for CAP evaluation. Furthermore, comorbidity with other deficits such as attention deficit hyperactivity disorders, Asperger’s Syndrome, or sensory integration disorder (Medwetsky & Musiek, 2011) may misguide professionals in referring a child for audiological CAP evaluation. For families, usually a child’s listening difficulties or behavior evident in the home and social environment may necessitate referral. For example, difficulty following instructions or communicating effectively with others as displayed by frequent requests for repetition (Heine, 2003).
Although a universally accepted definition and set of diagnostic criteria for CAPD is still lacking, the general public is becoming increasingly more aware of the concept of CAPD and referrals for CAP assessment continue to increase (Bellis, 2011). Most research has concentrated on debates around definitions and criteria, terminology and constructing assessment instruments. While it is reported that certain behaviors in children warrant referral for a CAP assessment (e.g., listening difficulties; Bellis, 2011), no research has been conducted on who is referring for CAP assessments and why they are referring. The determination of the referral concern most frequently leading to referral for CAP evaluation and resulting in a CAPD diagnosis will assist and alert future referrers in regard to the behaviors that could necessitate referral to an audiologist for CAP evaluation. In addition, the identification of referral sources would highlight the referral concern specific to the referral initiator and determine which if any referral initiators are in need of further informational counseling so that children with CAPD can be identified and managed. Information regarding referral concerns and referral sources will also provide insight into the decision-making process that professionals and families consider when referring a child for audiological evaluation.
The aims of this case file audit were to identify the referral sources and concerns that necessitate a child’s referral to an audiological clinic for CAP evaluation, whether educators are the primary referrers of children for a CAP evaluation, and examine the relationship between referral sources and concerns.
Materials and Method
Participants
Data were collected over a 6-month period (beginning in July 2015) from the files of 150 children diagnosed with CAPD since January 2013. These children had completed a full battery of hearing and CAP tests at an audiology clinic that specifically specializes in CAP evaluation. At the time of the assessment, the parents/guardians of these children completed a short generic questionnaire that was routinely used in this clinic. The questionnaire (adapted from Northern & Downs, 2002) enquired about each child’s demographics, referral information, schooling, prior professional consultations, medical history, family history, and developmental history. The referred group of children comprised 94 boys (62%) and 56 girls (37.3%), aged 7 to 11.1 years (M age = 8.19, SD = 2.55). Participants were of mixed demographic backgrounds (Australian or an immigrant group, such as from the United Kingdom, New Zealand, or South Africa) and socioeconomic class (attending both state and private schools) and derived from urban or rural population groups (living in Metropolitan Melbourne or surrounding areas in Victoria Australia).
Participants were excluded from this study if the parent did not fully complete the demographic or referral question parts of the case history questionnaire; if they did not sign informed consent for the use of their child’s information for research purposes; if the child’s home language was any language other than English, because English as a second language can influence the results of CAP testing, and if they were not diagnosed with CAPD after completing the audiological testing.
Instruments
Hearing and CAP evaluation
The hearing evaluation consisted of otoscopic examination, pure-tone air-conduction threshold audiometry, speech audiometry, and acoustic immittance testing. The measures used to assess CAP were selected according to ASHA (2005) guidelines and included evaluation of monaural low-redundancy speech, dichotic listening, and auditory temporal processing (see Table 1). The children in this study were diagnosed as having CAPD if they received a score of 2 standard deviations below the mean on two or more tests (as recommended by ASHA, 2005).
The CAP Test Battery Completed in This Study.

Note. CAP = central auditory processing; ASL = Auditec of St. Louis, USA; NU = Northwestern University, dBHL = decibel hearing level, MU = Maquarie University, NSW, Australia; RNC = right ear non-competing, RC = right ear competing, LNC = left ear non-competing, LC = left ear competing, W&S = Wilson and Strouse (1998); Normative data were obtained from Bellis (2003); Criteria for failure = 2 standard deviations or more below the mean on any two auditory processing tests; All dBHL values were as per the dial setting on the audiometer.
Case history questionnaire
Parents completed a case history questionnaire (see the appendix) in which the following information was provided: demographic data (including child’s date of birth and age, gender, home address, language spoken at home), referral information (the referral source initiating the referral for this evaluation and the reason for the referral), schooling (school attended and year level), medical history (general medical and ear specific history), and family history and developmental history (pregnancy, birth history, and developmental milestones).
Referral sources and referral concerns questions
The parents completed the referral sources and concerns section of the questionnaire by responding to questions that aimed at identifying the presenting concern necessitating the CAP evaluation and the referral source initiating the CAP evaluation. The following questions were asked (see the appendix): Did anyone refer you to this clinic (Yes/No)? If yes, who referred you? If no, how did you hear about this clinic? Please describe the concern/s that led you to contact this clinic.
On observation of item analysis, it was noted that referral sources could be delineated into three broad categories. One category was comprised of educators (the principal, assistant principal or vice principal, teachers, and special education personnel). The second category worked in the M/AHP (including doctors, otolaryngologists, pediatricians, neurologists, psychologists, occupational therapists, SLPs, and other professional personal). The final category comprised family members (which included family and friends as the referrer). In this way, referral sources were categorized as “school staff,” “M/AHP,” and “family.” There were no instances of more than one referrer.
A range of referral concerns was also reported. These were clearly delineated into concerns describing “hearing, listening, and processing” problems, such as “difficulties listening in noise” or “slow processing speed.” The second category was comprised of concerns describing literacy, speech, language, and academic problems, such as “difficulty with reading or spelling” or “receptive language difficulties.” The third category constituted items describing emotional-behavioral symptoms (including attention and concentration problems), such as “difficulty concentrating on tasks” or “difficulty sustaining attention.” For each child, the primary (first) reported concern as well as any further (secondary) concerns was categorized into one of the three categories. Following this allocation, the total number of reports per category was tallied, producing a total score in the categories “hearing, listening, and processing” problems; “literacy, speech, language, and academic” problems; and “emotional-behavioral” problems. There were 45 instances of children referred for two concerns and seven instances of three concerns per child.
Procedure
The same procedure was adopted for all children attending the clinic. Parents and their children attended the CAP clinic at a pre-arranged appointment date and time. They completed the case history questionnaire and informed consent form which takes approximately 5 min. Children’s hearing and CAP skills were then evaluated by a qualified audiologist in a sound-proof clinic room adjacent to the waiting room. The peripheral hearing evaluation was conducted using a Heine Otoscope, Earscan Immittance Meter, and Itera diagnostic audiometer with TDH-39 headphones. Peripheral hearing testing was followed by the CAP test battery evaluating, in order of test presentation, monaural low-redundancy speech testing, dichotic listening, and temporal processing (see Table 1).
Following this evaluation, a case discussion took place between the audiologist and the parents.
Data Analysis
The data were analyzed descriptively and statistically using χ2 tests at the p = .05 level of significance.
Results
Descriptive Statistics
As an initial step in data analysis, descriptive analyses were conducted. School staff was the primary referral source (61.0%), followed by M/AHPs (30.0 %) that included mainly SLPs, and finally by family members (9.0%). See Figure 1.

Distribution of referral sources.
Analysis of the percentage of referral concerns revealed that more than half the children (55.2%) were referred for literacy, speech, language, and academic concerns, and there were similar frequencies of referral for the categories hearing, listening, and processing difficulties (23.3%) and emotional-behavioral issues (21.4%; see Figure 2).
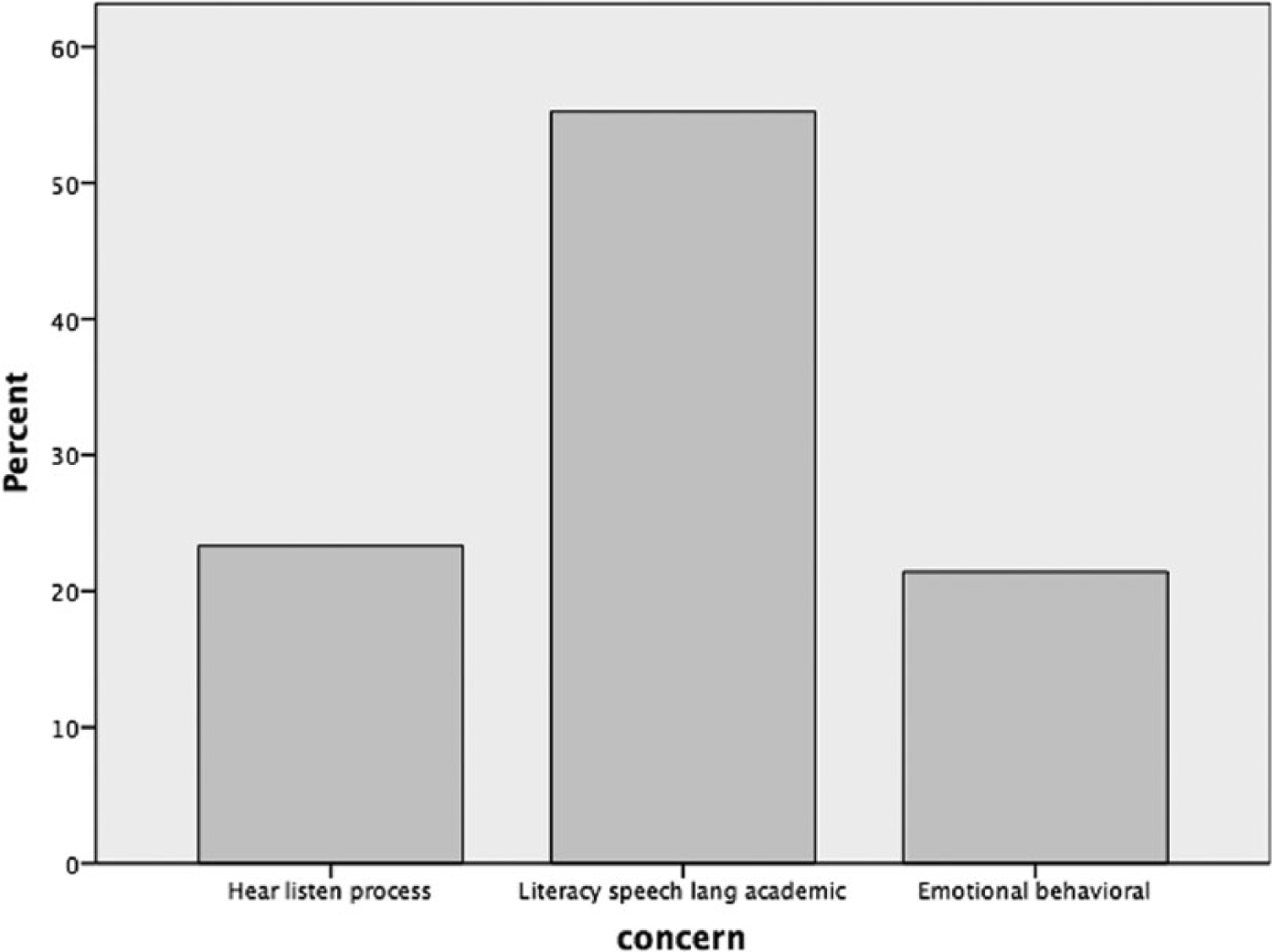
Distribution of referral concerns.
Statistical Analyses
To examine the relationship between the categorical variables (referral sources and referral concerns), between-group comparisons were conducted using χ2 tests at the p = .05 level of significance. The overall χ2 Fisher’s Exact test assessing the relation between the referral sources and the referral concerns was significant, χ2(4) = 11.068, p = .023. The analysis for proportion of referral source (school, M/AHP, and family) by referral concern (hearing, listening, and processing difficulties; literacy, speech, language, and academic underperformance; and emotional-behavioral issues) is presented in Table 2.
Relationship Between Referral Concerns and Referral Sources.
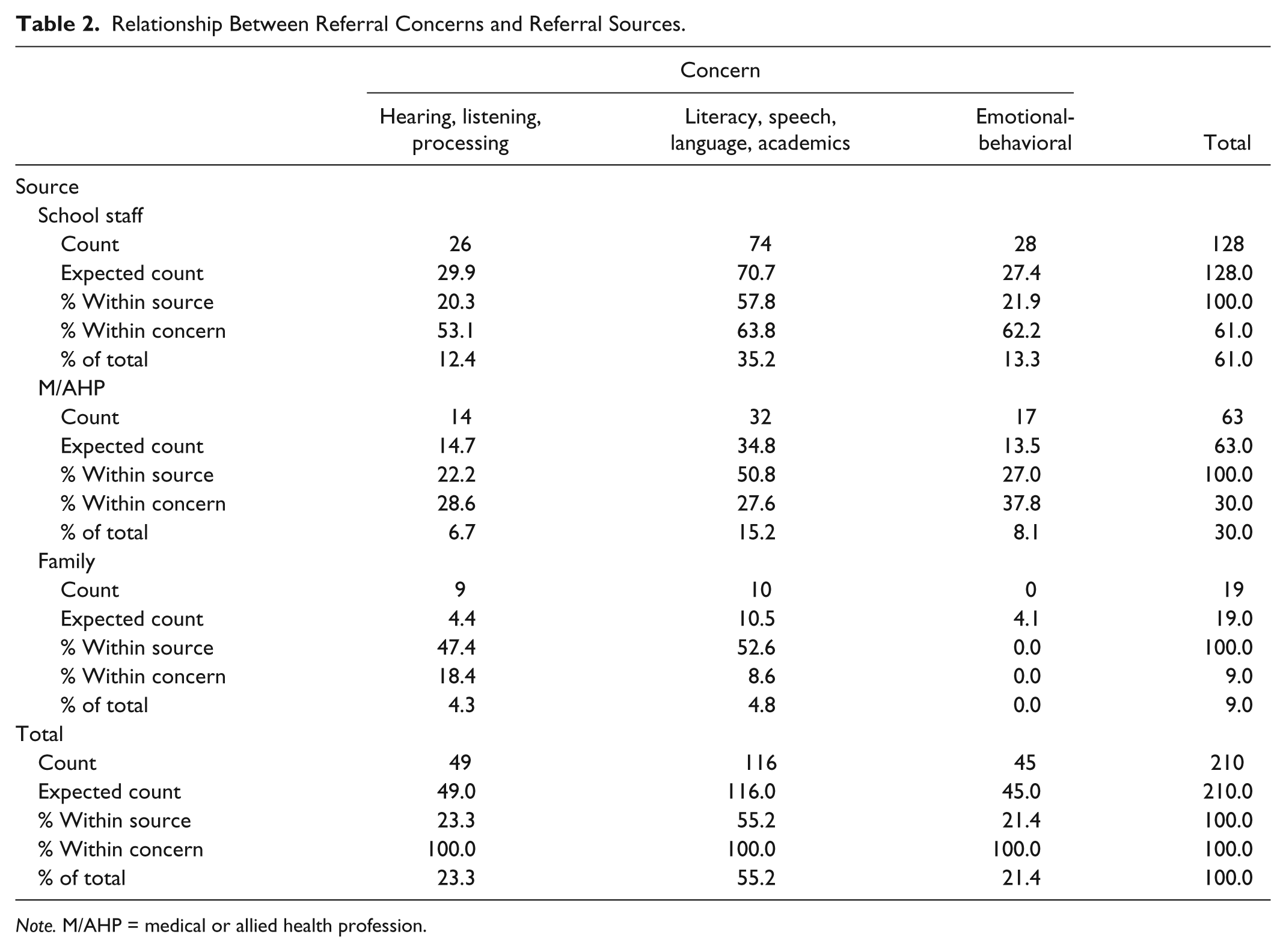
Note. M/AHP = medical or allied health profession.
Results of the χ2 test showed that both referral sources of school and M/AHPs referred clients for a CAP assessment primarily on the basis of literacy, speech, language, and academic underperformance (35.2% for school staff and 15.2% for M/AHP) and similarly for hearing, listening, and processing difficulties (12.4% for school staff and 6.7% for M/AHP) and emotional-behavioral issues (13.3% for school staff and 8.1% for M/AHP). However, in the category of family, referrals were equally made on the basis of the hearing, listening, and processing difficulties (18.4%), followed by literacy, speech, language, and academic underperformance (4.3% and 4.8%). There were no referrals made by family on the basis of emotional-behavioral issues.
To determine which categories of variables were major contributors to the statistically significant χ2 values, χ2 pair comparisons were examined. The result of χ2 indicated that there was a significant relationship between the referral sources of M/AHP and family for emotional-behavioral issues and hearing, listening and processing difficulties (χ2 = 8.583, p < .005). A significant relationship was also found between school staff and family for emotional-behavioral issues and hearing, listening, and processing difficulties (χ2 = 8.4, p < .005). Finally, a significant relationship was found between the M/AHP and family for emotional-behavioral issues and literacy, speech, language, and academic difficulties (χ2 = 4.874, p < .05).
Discussion
Findings of the descriptive statistics showed that the category of literacy, speech, language, and academic problems was the most salient area prompting referral for a CAP evaluation by all sources. Literature is available describing the close association between CAPD and literacy and academic problems and CAPD and speech and language disorders (Bamiou, Musiek, & Luxon, 2001; Banai & Kraus, 2007; Dawes & Bishop, 2009; Dawes et al., 2009; Domitz & Schow, 2000). Numerous theories have been hypothesized (although not yet proven) to explain the link between CAP, language and learning difficulties. Tallal and Piercy (1973) used an auditory repetition task (ART) to investigate the temporal processing of children with SLI compared with normal developing children. These authors concluded that children with SLI had more difficulty on this task than their normal developing counterparts when the interstimulus interval was short. In a follow-up study, Tallal, Miller, Jenkins, and Merzenich (1997) attributed oral and written childhood language disorders to a nonverbal processing deficit which occurs when auditory information is presented rapidly. Tallal (1980) found similar findings in a study with reading-impaired children. In contrast, however, Nittrouer (1999) found that good and poor readers did not differ in their ART performance or ability to identify brief formant transitions. Language, learning, and SLI are common deficits associated with literacy and academic underperformance. Diagnosis of language and learning difficulties may in fact overshadow the referral for CAPD evaluation as CAP deficits are less known as a clinical entity.
The second most frequent category of concerns on which referral was based, was hearing, listening, and processing problems. Referral to an audiologist on this basis would be highly insightful as the audiologist is the professional competent in evaluating the audiological system using audiometric instruments, and thus should have been the most obvious place to refer a child for these specific concerns. However, overall, these referral criteria were used by only 23.3% of cases. School staff and M/AHPs underutilized this criterion as a prompt for referral. A possible reason for lack of recognition of deficits in the auditory system as an underlying explanation for the child’s functional deficits could be that referral sources are not familiar with the audiological evaluation of CAPD. Potential referral sources are possibly also unable to distinguish auditory processing deficits from general academic, literacy, speech, and language disorders and may in their professional view believe that CAPD is a language or learning disorder. It is also possible that they refer children with these problems to other professionals such as the SLP or psychologist even if there are only listening, hearing, or processing symptomatologies (e.g., difficulty experienced only in complex listening situations such as when there is excessive background noise). The referral to other allied health professionals (other than the audiologist) may also be explained on the basis of comorbidity or the possibility that hearing, listening, or processing symptomatology may also be associated with other deficits (e.g., , a child with a language disorder may display hearing, listening or processing difficulties).
A large proportion of families also used these criteria appropriately as a stimulus for referral to an audiologist. A tentative explanation accounting for the prevalence of this referral category among family referrers is their ability to detect the child’s difficulty in attending to auditory information in an everyday home environment. Families may thus be in the best position to identify the child’s auditory discrimination difficulties, misidentification of auditory-presented instructions, confusion of sounds and words, inability to follow instructions, or communication, particularly in compromised listening environments. Because these difficulties occur in routine home environments, parents may not be confused with listening and processing difficulties as opposed to difficulties in other academic areas such as literacy or academic underperformance.
The third category of presenting problems was emotional-behavioral problems that prompted referral in only 21.4% of cases. It is most probable that the audiologist is not the primary person associated with this referral concern and the possibility of an audiological associated problem is entertained only after exhausting other alternative diagnoses.
School staff and M/AHPs used emotional-behavioral problems as a basis of referral. In contrast, the family did not use this concern at all as a referral criterion possibly as this symptomatology is more obscure and is probably attributed by them to psychological disorder.
School staff play a central role in referring children for CAP evaluation. They have broad knowledge and training in a variety of educational and associated content and issues, thereby positioning them to identify CAPD as a possible etiology for children’s listening difficulties. They also have access to large populations of children and carry the responsibility for delivering the curriculum to children, as well as for evaluating and monitoring children’s performance and referring children to a specialist when appropriate. This highlights the importance of continued appraisal of school staff in relation to CAPD, its symptomatology and audiological diagnosis to assist with identifying appropriate children for referral. A recent review of the literature evaluated whether reexamining the current CAPD protocols for school-age children is required, and concluded that the focus should rather be redirected to evaluating overall listening needs (DeBonis, 2015). Thus, for school staff, describing and differentiating children’s listening performance in a variety of listening contexts would be useful to inform the referral for CAP evaluation. These include differentiating performance in quiet environments as opposed to environments with excessive background noise or high reverberation, one-on-one situations as opposed to group situations where dichotic listening (multi-task listening) is required, and single-task auditory contexts as opposed to multiple task auditory contexts where the ability to divert auditory attention to various simultaneously presented auditory stimuli is required. It is important to note, however, that although these observations may be useful for educators to consider the necessity for CAP referral, these listening behaviors are not implicitly suggestive of CAPD.
Similarly M/AHPs encounter broad populations of children who potentially require CAPD assessment, yet the referral rate was lower than school staff. The relatively lower referral rate by M/AHPs for CAP assessment may be due to several reasons. It is possible that many personnel in this category conceptualize CAPD in a different way to the audiologist; they are not fully knowledgeable of strongly indicative referral criteria, the complexity of this diagnostic category, types of audiological assessments that can inform a diagnosis, and knowledge of the audiologist’s expertise in CAP evaluation.
In this study, the family did not make as many referrals for CAP evaluation compared to school staff and M/AHPs. It is likely that families (and possibly many other nonhealth professionals) are unaware of this diagnostic category and of symptoms that would prompt referral for CAP assessment, particularly as CAPD is a complex disorder that frequently defies specificity. In addition, families often become immersed in their child’s difficulties thereby limiting their objectivity when considering the source of problems. Families did not make any referrals for CAP evaluation based on emotional-behavioral symptoms, suggesting that they are unaware of this association, or this concern is not apparent in a home environment, or they consult specialists other than the audiologist in this regard. Notwithstanding the importance of parental referrals for CAP assessment, it would be a difficult task to apprise parents with the appropriate knowledge on a widespread basis. This fortifies the relevance of school staff and M/AHPs in detecting criteria for audiological CAPD referral.
Limitations
This sample was conducted on clients attending a private audiological clinic, and the origin of the sample may possibly be limited in generalizability, although no state-funded services for CAP testing are available in this state. In addition, participants in this study were collapsed into one sample from the age range 7 to 11 years. It would be interesting to increase the sample size and examine possible developmental differences that might alter the referral source and concerns.
Conclusion
The findings of this study suggested that school staff were the primary referral sources, while literacy, speech, language, and academic underperformance were the primary concern necessitating referral for an audiological CAP assessment. This suggests that for educators, CAPD is connected to general concerns about children’s underperformance at school. School staff are at the forefront of contact with children’s listening and learning difficulties and are therefore in one of the best positions to identify children that require an audiological CAP assessment. In addition, their training in education positions them to be alert to behaviors and symptoms that could suggest the need for referral. Dialogue between school staff and audiologists should be cultivated to further define the referral criteria for CAPD evaluation.
Human Subjects Approval Statement
At the time of the assessment, all parents/guardians signed and dated an informed consent form for their case records to be used in any current or future research projects. They were provided with a copy of the informed consent form which also assured them that they could withdraw their participation and inclusion in research studies conducted by this clinic at any time, which none did.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.