
Abstract
The population of older adults with chronic disease is increasing, yet little is known about their perception of chronic disease and self-management. To develop successful and sustainable chronic disease self-management interventions in the older adult population, health care providers must first understand older adults’ attitudes toward health status and behavior change. This pilot study was conducted to determine the feasibility of the study design. The purpose of this pilot study was to assess the appropriateness of using a mixed-methods research design to investigate Appalachian older adult’s attitude toward the chronic disease experience and health behavior change. A convergent, parallel mixed-method design included a quantitative questionnaire and qualitative focus groups in churches in northeast Tennessee. The aim of the study was met, and the methodology of the study was found to be feasible for larger studies. Divergence of data was found when evaluating qualitative and quantitative data. The study instrument was found to be reliable for future use. The implications of the results suggest that the study design is appropriate for the purpose of the study.
Keywords
Introduction
Over the last decade, advances in health care have increased life expectancy. Because Americans are living longer, more are experiencing chronic diseases than ever before. In fact, an epidemiological evolution has occurred in which infectious disease is no longer the primary cause of morbidity. Chronic disease has become a global phenomenon of pandemic proportions, becoming the leading cause of death (World Health Organization [WHO], 2012). The WHO has declared chronic illness to be a global crisis and a leading cause of mortality in older adults (WHO, 2005). Significant growth in the older adult population, those 65 years and older, is projected as the “Baby Boomer” population continues aging. Growth in this section of the population is expected to increase 20% by the year 2030 (Federal Interagency Forum on Aging-Related Statistics, 2012).
As the older adult population increases in size and age, research is focusing on ways to enhance individuals’ abilities to self-manage chronic disease. To help individuals better self-manage, health care providers must understand clients’ attitudes toward chronic disease, health behavior change, barriers to change, and the role social support plays in the self-management process. Few research studies have been completed that address chronic disease in older adults. The purpose of this pilot study was to assess the feasibility and appropriateness of using a mixed-methods research design to investigate Appalachian older adult’s attitude toward the chronic disease experience and health behavior change.
Self-Management
Although self-management serves increasingly as a method of chronic disease management, it has not been sufficiently explored specifically in the older adult population (Sell, Amella, Andrews, Mueller, & Wachs, 2016). Self-management is a process in which the client learns to incorporate skills and knowledge required to provide self-care (Whittemore & Dixon, 2008). This process empowers (Whittemore & Dixon, 2008) the client as the client is educated about symptom management and risk-factor reduction (Coster & Norman, 2009). The client moves into the role of team member and is encouraged to actively communicate with the health care team as the team works to improve health outcomes (Walker, Swerissen, & Belfrage, 2003). For the older adult, self-management may be a valuable tool, yet little attention has been paid to the goals of older adults in this process. This gap raises questions about how older adults perceive behavior change and what method of support during health behavior change. Although self-management may be a viable option for older adults, more conclusive research from the perspective of the older adult is needed.
Variables related to self-management
In a review of 22 published studies (Sell et al., 2016), a predominance (n = 16) of the samples’ mean ages was below 65 years. For individuals to change behaviors, their willingness to change (Glanz, Rimer, & Viswanath, 2008) and attitudes toward approaching change must be assessed. Individuals’ attitudes toward change such as their intention and willingness to participate in the steps needed to accomplish the change can foreshadow the outcome of initiating a health behavior change.
Self-efficacy has been recognized in studies as a moderating variable of successful behavior change (Garrod, Marshall, & Jones, 2008). The stronger the level of self-efficacy, the more likely the change will be successful (Bandura, 1997). In chronic disease self-management, clients’ beliefs in their abilities to competently self-manage the disease process are essential components of the change process.
Moral disengagement is a component of social cognitive theory (SCT) (Bandura, 2004) in which individuals are motivated to or hindered from making changes based on the significance of the risk behavior to the individual. In a form of moral disengagement, the individual may also misrepresent or negate the injury that one’s actions can cause (Bandura, Barbaraneli, & Pastorelli, 1996); this reasoning may negatively affect the impetus for change. The resulting discord between moral standards (values; Bandura et al., 1996; Glanz et al., 2008) and disengagement beliefs are manifested by a lack of motivation to improve health behaviors and/or to participate in self-management (Bandura et al., 1996). An example can be seen in alcoholics who continue to drink because it is not hurting themselves or others.
Social determinants of health are recognized as affecting the risk of chronic disease, disability, and mortality (Marmot & Wilkinson, 2006). Social determinants of health include age, social support, income level, level of education, health literacy, and environment obstacles such as housing and have been recognized to affect both the development and effects of chronic disease (Marmot & Bell, 2009). In older adults, a lower education level was noted to be related to higher levels of disability (Marmot & Wilkinson, 2006).
Health literacy is the ability of the patient to understand and use health information in health decisions (Berkman, Sheridan, Donahue, Halpern, & Crotty, 2011). In the United States, an estimated 80 million adults have a health literacy level that negatively affects their ability to manage health conditions (Berkman et al., 2011) and in individuals with chronic disease, studies have shown that low health literacy can affect patient outcomes, ability to access care, and illness and injury (Berkman et al., 2011).
Depression is an established barrier to behavior change that negatively affects chronic disease (Greenberg, 2012). The Centers for Disease Control and Prevention (CDC) estimates 6.2% of individuals above the age of 65 years who experience depression (CDC, 2013). The rate of depression is significantly higher in those with chronic diseases, increasing 10% to 20% (Janevic, Rosland, Wiitala, Connell, & Piette, 2012). Depression can affect attitude, motivation, and focus on health behavior change. Thus, depression is considered a potential intervening variable that can influence self-management behaviors and should be evaluated.
Research Design and Method
Study Design
A convergent, parallel mixed-method study design was used to explore the chronic disease phenomenon using both quantitative and qualitative methods. The sequential collection of data (Creswell & Plano Clark, 2011) through both questionnaire completion and focus group participation was used to explore participants’ attitudes and perceptions concerning the impact of chronic disease, self-management, and health behavior change. This methodology included data obtained from two different perspectives (Creswell & Plano Clark, 2011) and aided in substantiation of findings when merging data results.
Setting and Sample
Stratified purposive sampling was used in faith-based organizations in the Appalachian region of northeast Tennessee to recruit older adults diagnosed with diseases reflective of the regional population where chronic diseases rank in the top six for mortality (Tennessee Department of Health, 2008). The use of stratified purposive sampling ensured that specific demographic characteristics were included in the mixed-method study (Sandelowski, 2000). The size of each focus group was limited to five to eight individuals to facilitate qualitative data collection as larger groups could hinder communication and data collection (Krueger, 2009). The small sample size of the pilot study allowed for exploration of the feasibility of the recruiting process.
Inclusion Criteria
Older adults were eligible if they were English speaking, age 65 or older, and diagnosed with chronic obstructive pulmonary disease (COPD), hypertension, or type 2 diabetes mellitus for more than 1 year. Individuals who had limited or no reading proficiency but met the above criteria were also eligible. Individuals hospitalized within the past 30 days were excluded because their perceptions may have been altered by the recent exacerbations of symptoms. Because of the limited number of non-English speaking older adults in the region and lack of translations of existing questionnaire instruments, non-English-speaking individuals were not included in this study.
Data Collection Instruments
Quantitative data were collected via a questionnaire that included demographic and clinical information as well as several instruments that addressed social support, moral disengagement, self-efficacy, and self-regulation. Specifically, the questionnaire included demographic and social determinants of health data, and the nine-item Patient Health Questionnaire for Depression (Kroenke, Spitzer, & Williams, 2001) that evaluated symptoms of depression using a scale ranging from 0 (not at all) to 3 (nearly every day). A score of 5 indicated a risk for mild depression and a score of 20 indicated a risk for severe depression. The questionnaire further included an adapted Disengagement Beliefs Scale (Dijkstra, 2009) that uses a 5-point Likert-type scale from 1 (completely disagree) to 5 (completely agree). The higher the individual score, the more likely disengagement beliefs were present. The six-item Self-Efficacy for Managing Chronic Disease Scale (Lorig et al., 1996) used a Likert-type format with scales ranging from 1 (not at all confident) to 10 (totally confident). A higher number scored by an individual indicated a higher level of self-efficacy. To evaluate literacy, the Single-Item Literacy Screener (SILS; Morris, MacLean, Chew, & Littenberg, 2006) was used. Literacy was rated using a Likert-type scale with 1 (never) through 5 (always). A score greater than 2 indicates a possible deficiency in reading literacy. To address change behaviors, the Contemplation Ladder (Biener & Abrams, 1991) for considering behavior change asked the participants to rate their level of interest in change on a scale of 1 (not thinking about change) to 10 (ready to make a change). The participants were also asked to rate self-reported level of daily self-management behaviors (Lorig et al., 1996) and self-reported health status, each using a 5-point Likert-type scale from 1 (excellent) to 5 (poor).
The questionnaire also included items regarding the role of spiritual beliefs in health and the significance of spirituality in participants’ lives. A single question solicited preferred methods of learning and self-management participation such as using health coaching, computerized system, group activities, or family participation in the process. Physiologic parameters such as blood pressure, weight, height, abdominal girth, body mass index, shortness of breath, and oxygen saturation were collected as indicators of self-management. For those participants who reported a diagnosis of diabetes, glycosylated hemoglobin (Hgb A1c) was measured using the Bayer© A1C Now home test kit. The value was used to indicate mean blood glucose levels over a 6-week period.
The quantitative questionnaire combined demographics, biometrics, and the standardized instruments; prior to the pilot study, the questionnaire was administered to three individuals’ representative of the study population. These individuals provided feedback on question content and clarity (Waltz, Strickland, & Lenz, 2010). Content experts were used to review questionnaire content both before and after the study for ambiguity and content problems (Waltz et al., 2010).
Data Collection Procedures
The study was approved by the institutional review board (IRB) at the Medical University of South Carolina (MUSC) and the IRB from East Tennessee State University. Parish nurse programs established in the Appalachian region of northeast Tennessee were contacted and asked to serve as study hosts because the nurses had established relationships with potential participants. A study goal of five focus groups with five to eight participants per group was set.
The research study was advertised through church newsletters, bulletins, and flyers. Individuals who met criteria were sent a follow-up letter containing information about the study purpose, date of the focus group, data collection procedures, and informed consent. The parish nurse made reminder calls the night before the scheduled meeting. On the specified date, participants were directed to a private location to provide informed consent. After consenting, blood pressure, heart rate, oxygen saturation, weight, and height were collected. If the participant was diabetic, an Hgb A1c was also measured. These measures were collected by the principal investigator in a private location. All participants received their results in a sealed envelope after assessments were completed. For depression screening, those who scored positive for depressive symptoms were notified and encouraged to seek care from a primary provider; all participants were given a brochure on recognizing the symptoms of depression.
To collect questionnaire data, participants were given a numbered envelope containing the questionnaire and directed to a private location. The packet also contained a US$10.00 gift card for all who participated. Once completed, the questionnaires were collected and placed in a locked box kept with the researcher during the focus groups. A light lunch was provided to all participants; after lunch, information on the purpose of the focus group and the possibility to withdraw from the study at any time were reviewed; assurance of confidentiality of the information collected during the study was given. The note taker was introduced, and the purpose of having a member of the research team taking notes and recording the conversation was explained.
The focus group discussion used 13 prepared questions in a semi-structured format that allowed for evolution of the conversation as themes emerged (appendix). The structure of the focus groups was based on the Krueger method (Krueger, 2009) with the principal investigator acting as the facilitator. Each question was asked and, when necessary, verbal probes were used to further elicit information from the study participants. The focus groups ended when no new themes emerged. All participants from whom feedback was solicited were debriefed regarding the research format, questionnaire, and qualitative questions to determine if the methodology was clear and understandable to the participants.
Data Analysis
Questionnaire data were stored in Research Electronic Data Capture (REDCap), a system developed by Vanderbilt University with data management features enabling secure storage and imported to SPSS (Statistical Package for Social Sciences); all data were stored on the MUSC secure server. For analysis, questionnaire results were imported into SPSS 18; data were cleaned and evaluated for missing values and outliers. Missing data were evaluated for randomness or patterns and imputed by using the mean or median method (Munro, 2005). Descriptive statistics were calculated demographic and clinical variables. Frequency distributions and 95% confidence intervals (CIs) were used for categorical data, means, medians, and standard deviations and 95% CIs for continuous variables. Cronbach’s alpha, a coefficient of internal consistency commonly used as an estimate of instrument reliability, was used to measure reliability of instrument scales. Due to the relatively small sample size (n = 29), relationships among variables were investigated using nonparametric correlations (Spearman’s ρ).
The qualitative data were recorded and then transcribed verbatim. Substantive coding was used to identify and analyze the data. In addition, coding was accomplished through the use of QRS NVivo 10 software (QRS International, 2012) and the six-phase method of thematic analysis as proposed by Braun and Clark (2006).
In this mixed-method study, triangulation was achieved by exploring the same phenomenon of self-management through two different methods (Plano Clark & Creswell, 2008). The use of more than one method increases the validity of and confidence in results and can provide a greater understanding of the phenomenon under study. After separate analyses of qualitative and quantitative data, the data were merged in a side-by-side comparison to evaluate convergence or divergence between the two data sets (Creswell & Plano Clark, 2011).
Results
Feasibility of Design
For this study, a total of 40 potential participants were approached for participation. The pilot study began with a total of 29 participants recruited from the 33 who expressed interest. Of the 33, three did not meet eligibility criteria, and one person did not attend the study visit. The goal of enrollment was between five and eight participants per focus group, and that goal was met. The process for contacting and reminding the potential participants worked well; the parish nurse was extremely helpful facilitating enrollment. Mailing information prior to the meeting also encouraged participant review of the project description and consent form. Most participants were prepared with specific questions that could be addressed before written informed consent was obtained.
The demographic characteristics of the sample are reported in Table 1. Eighty-three percent (24 / 29) of the participants had a self-reported diagnosis of hypertension, 31% (9 / 29) reported diabetes, and 15.4% (4/29) had COPD. The average length of time since diagnosis was 10 to 20 years indicating a sample with long-term experience with chronic disease.
Means and Standard Deviations for Demographic Variables.
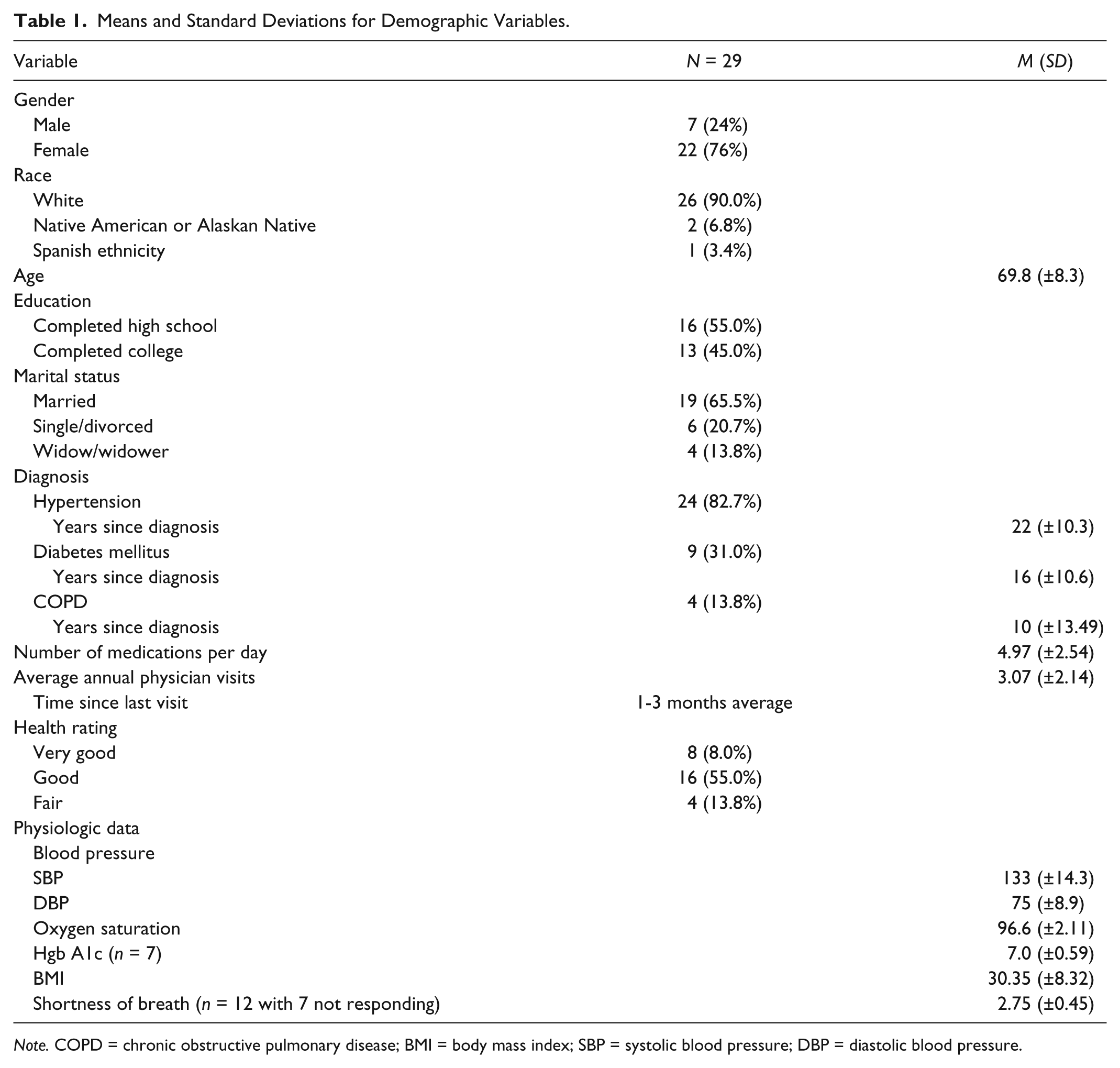
Note. COPD = chronic obstructive pulmonary disease; BMI = body mass index; SBP = systolic blood pressure; DBP = diastolic blood pressure.
During the pilot, the completion of informed consent required approximately 5 min with the obtainment of physiologic parameters requiring 10 min per participant. Capturing all physiologic parameters provided a snapshot of the self-management status through assessment of disease-specific outcome measures such as diabetes self-management assessed through Hgb A1c (Table 2).
Means (SD) and Frequency Distributions for Self-Management Outcome Measures.

Quantitative Analysis/Variability in Outcome Measures
Cronbach’s alpha suggested excellent reliability for the Self-Efficacy Scale (α = .928), acceptable reliability for the Moral Disengagement Scale (α = .732), and very good reliability for the patient health questionnaire 9 (PHQ-9) Scale (α = .808). The SILS had a mean score of 4.50 with an SD of ±1.10. The mean contemplation score was 8.00 with a standard deviation of ±2.27.
To examine the potential for relationships among depression, self-efficacy, self-management, daily self-management, depression, health literacy, and self-rated health variables, Spearman’s ρ correlation coefficient with a 95% CI were calculated for each pair of variables. A statistically significant moderate correlation was found between depression and self-rated health (r = .436, p < .023, 95% CI = [0.08, 0.69]). Specifically, the data revealed that a higher depression scores are related to a lower self-efficacy scores. Overall, the sample mean depression score was 3.68 (low risk for depression). A moderate positive correlation between health literacy and self-efficacy (r = .385, p < .039, 95% CI = [0.02, 0.66]) indicated that higher levels of health literacy are statistically significantly associated with increased levels of self-efficacy. Individual’s level of self-rated health had a moderate relation to the inability to manage the disease daily (r = .391, p < .040, 95% CI = [0.03, 0.66]). Finally, there was a moderate correlation between self-efficacy and self-rated health (r = .416, p < .028, 95% CI = [0.06, 0.68]), indicating that as self-efficacy increased, a person’s self-rated health also increased.
In addition, participant scores on self-rated health, daily disease management, self-efficacy, and moral disengagement were evaluated by diagnosis (Table 3). To evaluate ability to self-manage, physiologic parameters relevant to each diagnosis were compared (Table 3).
Self-Rated Health, Daily Disease Management, Self-Efficacy, Moral Disengagement by Chronic Disease Diagnosis.

Note. COPD = chronic obstructive pulmonary disease.
Triangulation of Qualitative and Quantitative Data
The process of merging data was used to compare and contrast data in an effort to support the findings (Creswell & Plano Clark, 2011). In this convergent, parallel mixed-method design, qualitative and quantitative data were compared side by side (Table 4; Creswell & Plano Clark, 2011). Data were merged to address research questions related to implementation of health behavior change using SCT, using quantitative data to support qualitative data. The results of merging the data revealed individual differences in perception of chronic disease and attitude toward change. Self-rated health and self-efficacy were found to differ among disease diagnoses. Motivators for change were consistent in each group, and barriers were related to individuality and disease impact. The mechanism of social support to support behavior change indicated an overall preference for family involvement, and most indicated the desire to be treated as an individual who participates as a member of the health care team.
Results of Merged Qualitative and Quantitative Data.

Note. COPD = chronic obstructive pulmonary disease; HTN = hypertension; DM = diabetes mellitus.
Discussion
In older adults, few studies have been completed evaluating self-management in those with chronic disease. And of those studies, only a limited number have been completed in the United States and none with Appalachian adults in northeast Tennessee. This study is important in that it provides a study framework to complete additional and larger studies in this population. In this convergent, parallel mixed-method feasibility study, the purpose was to evaluate whether the design would capture data relevant to Appalachian older adults with chronic disease. The study was to determine whether the protocol, instrumentation, and data analysis procedures were appropriate for use in this older adult population. This study is important in that it provides a study framework to complete additional larger studies in this population. In this convergent, parallel mixed-method design feasibility study, three aims were addressed to determine whether the protocol, instrumentation, and data analysis procedures were appropriate for use in this older adult population. Review of the data collection process revealed the need for additional staff to decrease participants’ wait time. The proposed sample size and focus group number were both met. The recruiting procedure for the study provided an adequate sample and was considered appropriate for the study purpose.
The principal investigator determined instruments were reliable as indicated by moderate to high Cronbach’s alpha coefficient. In the review of missing data, a systematic pattern was discovered with the question rating shortness of breath: 41.0% (n = 17) of the 29 participants did not answer the question. The pattern of missing data was not related to the format of the instrumentation but to a diagnosis of hypertension. The principal investigator posited that individuals with hypertension did not answer the question on the basis that they did not believe it related to their condition even though it could be a sign of heart failure. The principal investigator also asked three individuals, who were not part of the study but met inclusion criteria to review the instrument for face validity to provide feedback regarding format and question clarity. Feedback from the debriefing of the participants was also used to determine whether changes to the questionnaire were indicated before future studies are undertaken.
As noted previously, the sample was not large enough to meet the criteria necessary to use parametric correlational techniques such as Pearson’s correlation coefficient. As such, nonparametric Spearman’s ρ correlation was used to evaluate for relationships among variables. Results suggest that a relationship may exist among self-efficacy, self-rated health, health literacy, and daily self-management variables. Conclusions about the relationships cannot be definitively established; these findings should be confirmed in future, larger studies in which regression analysis can be used.
Findings from triangulation of quantitative and qualitative data indicated that extrapolation of themes relevant to the research questions was possible. In analyzing data, looking for convergence and divergence, a divergence of data was found relevant to risk factors and communication. Overall, the assessment of the feasibility study instrument revealed the need to alter the instrument to reflect global social support systems such as providers and health care systems. Additional support will be included in future studies, and it was determined that overall study purpose is feasible for the purpose of the study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the South Carolina Clinical and Translational Research Institute through grants NIH/NCRR Grant UL1 RR029882 and UL1 TR000062 as well as East Tennessee State University Center for Nursing Research.