
Abstract
To investigate different social support dimensions and their association with mortality among older adults in Finland. This study is part of the longitudinal population-based Cardiovascular Risk Factors, Aging and Dementia (CAIDE) study (N = 1,295), with an age range of 65 to 80 years and a follow-up of 21 years. Cox proportional hazard models were used. In the unadjusted analyses, older adults without general social support and health-related social support from nonrelatives had higher mortality risk than those with social support in the overall population, respectively (hazard ratio [HR], 1.23; 95% confidence interval [CI] [1.02, 1.48]), (HR 1.23; [1.04, 1.44]). After stratifying into age groups and adjusting for covariates, heterogeneous trajectories emerged for associations between social support dimensions and mortality. Lack of social support predicts mortality even after 21 years of follow-up. The findings highlight the diversity of social support patterns and the importance of preventive measures when aiming to support health and well-being in later life. Future research should harness age variations to understand the different needs and explore nonrelatives’ roles in social support.
Introduction
Social support is a social-emotional need known to have a beneficial effect on physical and emotional well-being in old age. Several studies have revealed an association between social support and survival among older people (Hill et al., 2016; Lyyra & Heikkinen, 2006; see also Kröger, 2022). Moreover, absence of social support has been linked to mortality and loneliness (De Brito et al., 2017; Penninx et al., 1997; Roth & Peng, 2022; Ten Bruggencate et al., 2018; Williams et al., 2019). While social support is beneficial throughout life, it is especially crucial in later life, which is marked by health losses and increased desire for emotionally fulfilling social ties (Bengtson & Settersten, 2016).
Definitions of social support vary notably across disciplines; whereas some definitions embody the structural elements of social support, like network size, other definitions focus on the functional elements, such as the precise support received (Avlund et al., 1998, 2004; Hakulinen et al., 2016; Lyyra & Heikkinen, 2006; Penninx et al., 1997). Sarason et al. (1983) have defined social support as the existence or availability of people who can be relied on and from whom individuals can receive care, love and a sense of being valued. Further, Barrera (1986) proposed three types of social support: social embeddedness (evaluates frequency of contacts), received support (quantifies actual support received) and perceived support (estimates subjective exchanges in support and subsequent satisfaction).
To date, longitudinal research examining the outcomes of social support in later life has been scarce despite increased research interest in the negative consequences of loneliness and social isolation (e.g., Fakoya et al., 2020). This study aims to fill this research gap by examining different dimensions of social support and their predictive association with mortality among older adults living in Finland during a 21-year follow-up. The different social support dimensions were divided into (i) general social support, (ii) health-related social support from relatives and (iii) health-related social support from nonrelatives. Hence, this study contributes to existing research on social support and its health outcomes in later life, while introducing and exploring different forms and sources of social support.
Social Support, Health and Mortality in Later Life
Previous research has shown that social support in later life has many sources and is exchanged across several types of relationships, including spouses, children, friends, neighbours and other relatives (Roth & Peng, 2022). Studies among older adults have often focused on the existence of spousal support, indicating its role as a key contributor to health, well-being and quality of life in older age (Leung et al., 2014; Williams et al., 2019). In addition, studies examining social support provided by other family members, such as adult children, have suggested that social support received from relatives enhances mental health and may for some older adults be the most important source of social support (Chen et al., 2014; Okabayashi et al., 2004).
Moreover, studies have found that also friends play an important role in providing social support for older adults (Gallardo-Peralta et al., 2018) and that the existence of at least one close friend yields positive mental and health benefits in later life (Taylor, 2011). Similarly, secondary networks such as neighbours and neighbourhoods, and different types of social groups (both formally and informally organised) are known to provide social support and increase social participation and well-being in older age (Gallardo-Peralta et al., 2018; Hand et al., 2012; Nocon & Pearson, 2000). Social support provided by peer-support groups have been found to be especially beneficial for older adults experiencing challenging life situations (Geffen et al., 2019; Joo et al., 2025).
Some studies have found that having a close relationship with family, children and friends increases access to information about health services and consequently contributes to better health outcomes in later life (Gyasi et al., 2020). Existing research has also suggested that social support buffers the harmful physical and mental impacts caused by stress and builds resilience (Zhu & Chou, 2022), and that social support is directly associated with a better health-related quality of life among older adults with severe illnesses (Leung et al., 2014). Previous research on the association between social support and mortality has indicated that low levels of social support increase risk of death, but that the association varies depending on age and gender (Fuhrer & Stanfield, 2002; Lyyra & Heikkinen, 2006) indicating different patterns of social support and its outcomes.
Despite existing evidence on the impact of social support on mortality in later life, little is still known about how the different dimensions of social support are associated with the mortality of older adults after long follow-up periods. Conflicting knowledge exists mainly because of the diverse operationalisation of social support in various studies. Most research has focused on the functional roles of social support and their association with mortality rather than the degree to which the different sources of social support interact with and act to influence the mortality of older adults. Moreover, only a limited number of studies, especially longitudinal ones, have focused on the sources of social support and their association with mortality (Roth & Peng, 2022).
Methods
This study used a longitudinal research design with a 21-year follow up. In the analysis, Cox proportional hazards models (Cox, 1972) and Kaplan-Meier graphs (Jager et al., 2008) were used to examine the association between social support dimensions and mortality among older adults.
Data and Sample
Our data was derived from the Cardiovascular Risk Factors, Aging and Dementia study (CAIDE). The CAIDE study is a population-based longitudinal study that was initiated to explore modifiable risk and protective factors for dementia among older adults in the regions of Kuopio and Joensuu in Finland (Barbera et al., 2020). Participants in the CAIDE study were identified from Finnish population-based surveys within the North Karelia project in 1972 and 1977 and the FINMONICA study in 1982 and 1987 when the study population was middle-aged (mean age 50.4 ± 6 years) (Barbera et al., 2020). In 1998, a total of 2,000 individuals living in the Kuopio and Joensuu regions in Eastern Finland were invited to participate in the CAIDE study, and 1,449 agreed to participate with an age range of 65 to 79 and mean age of 71 years. The final sample of 1,295 participants consisted of individuals who had responded to the social support questions in a questionnaire in the 1998 study. The study was approved by the Research Ethics Committee of the Research Ethics Committee of Northern Savo Hospital District (Finland). All participants gave their informed consent (Figure 1).

Flow chart showing the selection of study participants.
Measurements
Social Support
Social support was measured using six items from the social support questionnaire (SSQ) (Sarason et al., 1983). Here, participants were asked to list people who provided them support under the circumstances of each item. The six items included: (ss1) Who can you trust when you want to forget your worries when feeling burdened? (ss2) Whose help can you truly trust when you need to relax due to great pressure? (ss3) Who truly accepts you as you are with all your good and bad sides? (ss4) Who can you truly trust that they care for you no matter what happens? (ss5) Who can you truly trust that makes you feel better when you are feeling down? (ss6) Who can you trust that comforts you when you are upset (confused, shocked)? Response categories for these items were coded as (i) spouse, (ii) some other next of kin, (iii) close friend, (iv) some other relative or friend from work and (v) nobody. Sarason’s social support questionnaire has been validated as a reliable instrument for measuring social support in several settings, including European countries (Rascle et al., 2005; Sarason et al., 1983).
Social Support Dimensions
General Social Support
For this dimension of social support, we assessed the SSQ responses to identify responses indicating that support was received as well as those indicating nobody/no support. Thus, a binary variable was created with 0 representing those with social support and 1 those without social support.
Health-Related Social Support from Relatives and Nonrelatives
These two dimensions of social support were created through another question that was not part of the SSQ items but part of the overall questionnaire administered to participants in the CAIDE follow-ups: If you have problems regarding health for which you need advice or other support, can you get help from the following people? Responses included: (i) Spouse/life partner, (ii) Your own or your spouse’s parents, (iii) Your own children, (iv) Other relatives, (v) Neighbours, (vi) Colleagues at work or school, (vii) Friends, (viii) Someone else. Responses were aggregated into two categories: (i) relatives (including spouse/life partner, your own or your spouse’s parents, your own children, other relatives) and (ii) nonrelatives (including neighbours, colleagues at work or school, friends, someone else) (Table 1).
Formation of the Social Support Dimensions.

Baseline Characteristics
Social demographic characteristics such as age, sex, income, education, civil status and self-rated health were included. The age variable (years) was based on participants’ dates of birth. Age was used as a continuous variable and also as a dichotomous variable in the stratified analyses where it was aggregated into two groups: (i) below 70 and (ii) 70 and above. Sex was men, women. Civil status was defined as (i) married, (ii) single, (iii) separated or divorced and (iv) widowed. Education in years was used as a continuous variable. Annual household income in Finnish marks (mk) was aggregated into three categories: low (≤80,000 mk), average (80,001–160,000 mk) and high (>160,001 mk). Self-rated health was indicated by self-report responses of participants on a scale of (i) very good, (ii) quite good, (iii) average, (iv) quite poor and (v) very poor. Self-rated health was then categorised by combining (very good and quite good), (average) and (quite poor and very poor) to form (i) good, (ii) average and (iii) poor.
Baseline characteristics of the study population are shown in Table 2. Altogether, 45.6% of participants were below 70 years of age and 54.4% were age 70 or above. In all, 38.6% were men and 61.4% were women. Household income range was 41.2% low, 42.4% average and 16.3% high. Mean years of education was 8.4 years, with a standard deviation of 3.5. In all, 81.2% of participants were married, 7.1% single, 4.2% separated/divorced and 7.5% were widowed. Over half of the study population (52.8%) reported having average self-rated health, while 34.1% had good health and 13.1% had reported poor health status.
Baseline Characteristics of Study Participants.

Statistical Analysis
Cox proportional hazards models were used to analyse the associations between the social support dimensions with all-cause mortality over a follow-up period of 21 years (Cox, 1972). Analyses were done to reveal the associations between the social support dimensions and mortality for all participants in four models. Model 1 was a univariate model of the social support dimensions and mortality. Model 2 comprised social support dimensions separately adjusted for sex and age as a continuous variable. Model 3 included the social support dimensions each separately adjusted for covariates including sex, education, income, civil status and age as continuous. Lastly, Model 4 included sex, education, income, civil status, self-rated health and age as a continuous variable. We specifically used these four models because, for the univariate model, we wanted to understand the independent effect of each social support dimension on mortality. Model 2 consisted of age and sex as confounders, which are often considered important predictors of mortality (Carey et al., 2007; Reilev et al., 2020) with a direct impact on mortality. Since the mortality of older people can be predicted by several other factors that are usually intertwined with real-life experiences (Benyamini et al., 2003; Stålbrand et al., 2007) we incorporated these in the models. Models 3 and 4 differ in that model 3 excludes the subjective health of the older adults, whereas model 4 is the fully adjusted model comprising all covariates (age, sex, income, education, civil status and self-rated health).
The mortality risk of older people is known to differ in different age groups (Benyamini et al., 2003). Furthermore, healthcare needs increase with age, so the age factor was considered. Thus, we examined the effect of social support dimensions on mortality in two different age subgroups: below 70 and 70 years or above for all models (see Table 4). Potential impacts of age and sex on the association between different dimensions of social support and mortality (Carey et al., 2007; Reilev et al., 2020; Schoevers et al., 2000) were investigated. This was done by separately by adding an interaction term between age (<70 years and ≥70 years) and social support, and sex and social support to the model, respectively. The interaction terms between sex and different social support dimensions were not statistically significant. Still, the interaction analyses between age and some social support dimensions, such as health-related social support from nonrelatives, showed statistically significant findings with a p-value of .01. Thus, Cox proportional hazards models regarding all social support dimensions were performed separately for those below 70 years and those equal to or above 70 years.
After stratifying by age, additional analysis was done to investigate the associations of the three social support dimensions with mortality within the two age groups of below 70 and equal to or above 70 years. These associations of the three social support dimensions with mortality were analysed in four models. Model 1 was an unadjusted univariate model of the social support dimensions stratified by age; Model 2 included the social support dimensions each separately adjusted for sex and age as a continuous variable. Model 3 included the social support dimensions with each separately adjusted for covariates including sex, education, income, civil status and age as a continuous variable. Model 4 was a fully adjusted model that included sex, education, income, civil status, self-rated health and age as a continuous variable. Within the social support dimensions (general social support, health-related social support from relatives, and health-related social support from nonrelatives) the group with social support was used as the reference group. Statistical analyses were also performed using a Kaplan-Meier graph to plot the survival rate of participants for the 21-year follow-up period. The validity of the proportional hazards assumption for the social support elements was verified using Schoenfeld residuals.
Mortality Risk
We assessed the mortality risk over a period of 21 years. Death dates extracted from the Finnish National Population Register were used to confirm death. The follow-up period started at the measurement date in 1998. Mortality was followed-up until May 23rd, 2019.
Results
The results in Table 3 show that in Model 1 two dimensions of lack of social support were associated with mortality in all participants: general social support (hazard ratio [HR], 1.23; 95% confidence interval [CI] [1.02, 1.48]) and health-related social support from nonrelatives (HR, 1.23; [1.04, 1.44]), contrary to the other dimension, health-related social support from relatives, which was not statistically significant. Other models in Table 3 were not statistically significant for all participants.
Associations of Social Support Dimensions with Mortality in All Participants: Cox Proportional Hazards Model with 95% CI.

Note. HR = hazard ratio; CI = confidence interval. The observations are for all participants. In the table, Model 1 univariate analysis; Model 2 adjusted for sex and age as continuous; Model 3 adjusted for sex, education, income, civil status and age as continuous; Model 4 adjusted for sex, education, income, civil status, self-rated health and age as continuous.
Statistically significant values in bold (p < .05).
As Table 4 shows, in the below 70 age subgroup there was a significant association between one social support dimension and mortality in the univariate: not receiving health-related social support from nonrelatives (HR, 1.44, 95% CI [1.10, 1.89]), but not in the above 70 age subgroup. Furthermore, in the same below 70 age group, in the univariate model the general social support dimension exhibited marginal significance with mortality despite not meeting the standard threshold of significance (HR, 1.38, [0.98, 1.94]) with a p-value of .06.
Associations of Social Support Dimensions with Mortality by Age Subgroup: Cox Proportional Hazards Model with 95% CI.

Note. HR = hazard ratio; CI = confidence interval. In the table, Model 1 univariate analysis; Model 2 adjusted for sex and age as continuous; Model 3 adjusted for sex, education, income, civil status and age as continuous; Model 4 adjusted for sex, education, income, civil status, self-rated health and age as continuous.
Statistically significant values in bold (p < .05).
In model 2 (Table 4), after adjusting for sex and age as a continuous variable, not receiving health-related social support from nonrelatives had an almost significant association with lower mortality in those above 70 (HR 0.83, 95% CI [0.67, 1.02]). Although this did not yield statistical significance, it is worth reporting that it was marginally significant with a p-value of .07.
Model 3 was quite revealing in several ways; first, after adjusting for confounders (sex, education, income, civil status and age as continuous), older adults below 70 years who did not receive general social support had a significantly higher mortality risk (HR 1.47, 95% CI [1.03, 2.10]) compared to those who received social support in the same dimension. Further statistical tests within the same Model 3 revealed that older adults of 70 and above years had a lower mortality risk without health-related social support from nonrelatives (HR 0.74, [0.59, 0.92]) compared to those who received this support. Although not receiving health-related social support from nonrelatives had an almost significant association with increased mortality in those below 70 years in Model 3, it did not reach the conventional significance level (HR 1.30, [0.98, 1.73]) with a p-value of .06.
After adjusting for sex, education, income, civil status, self-rated health and age as continuous variables in the fully adjusted Model 4, older adults of 70 and above years who did not receive health-related social support from nonrelatives had a lower mortality risk than those that received social support within the same subgroups (HR 0.79, 95% CI [0.63, 0.98]). While the association between health-related social support from nonrelatives and mortality was almost significant for older adults below 70 years in Model 4, it fell short of the expected significance threshold. In the age below 70 and 70 and above subgroup analysis, one social support dimension did not have any associations with mortality in models 1 to 4: health-related social support from relatives.
Figure 2 plots the survival estimations of older people within the general social support dimension. There were differences in the estimated survival times for respondents with general social support and those without this over the follow-up period. Older adults who received general social support had a median survival time of 16.8 years, and those without 14.2 years. The median difference between the two groups was 2.7 years.

Kaplan-Meier survival estimates within the general social support dimension.
Figure 3 shows the Kaplan-Meier survival curves for receiving health-related social support from relatives (a) and nonrelatives (b). The median survival time for those with health-related social support from relatives was 16.7 years and for those without, 15.4. Similarly, those with health-related social support from nonrelatives had a median survival time of 17.2 years, while those without had 15.7 years.
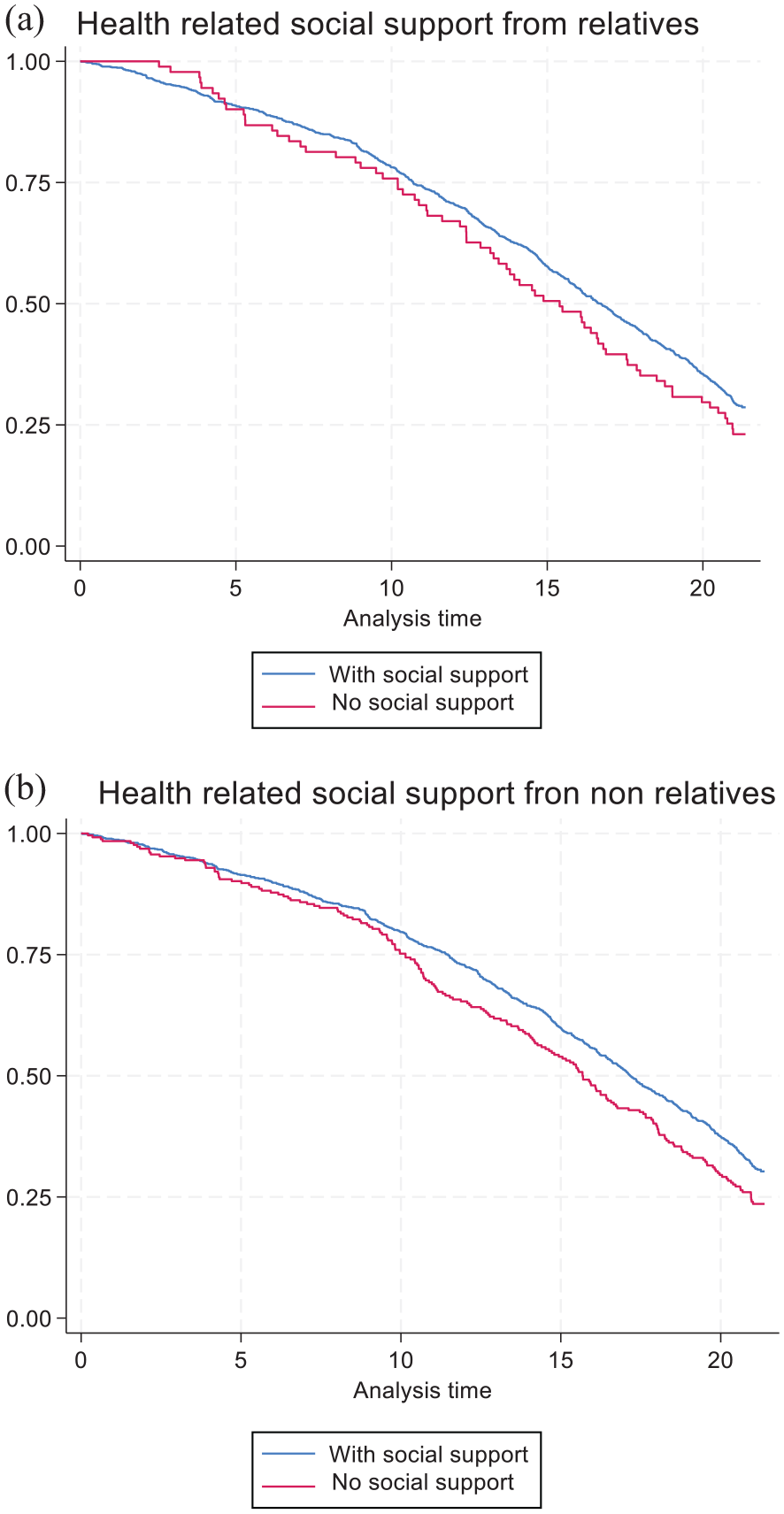
Survival estimates for health-related support from relatives (a) and nonrelatives (b).
Discussion
Our findings show that older adults without general social support and health-related social support from nonrelatives had a higher mortality risk than those with this social support. Upon classification into age groups and adjusting for covariates, heterogeneous trajectories emerged for the associations between social support dimensions and mortality. Our findings imply that older adults aged below 70 years were at higher risk of death without general and health-related social support from nonrelatives than those who received this social support, yet the same effect was not evident in those 70 years and above. These results were surprising given that no differences were found in the effect of social support dimensions and mortality in the 70 and above age group in the same model.
The counterintuitive results associating social support dimensions with mortality within only the younger age group (those below 70 years) of older adults may be explained, in part, by the fact that this category of older people below 70 years could be the main providers of social support without reciprocity of this support from older people above 70 years. The lack of reciprocity in social support relationships has been associated with feelings of stress, inferiority, indebtedness and the risk of death (Chandola et al., 2007; De Brito et al., 2017; Siegrist, 2005).
A trend that stands out from the results is that having health-related social support from nonrelatives such as neighbours, colleagues and friends increased the survival of older adults. This finding diverges from most previous literature that suggests that family members and relatives play the biggest, or only, role in supporting older people (Chen et al., 2014; Roth & Peng, 2022). An alternative explanation for the strong role of nonrelatives in providing support could be connected to societal and cultural factors related to the study population.
Finland traditionally represents a Nordic welfare state with a strong public sector providing care for all its citizens (e.g., Rostgaard et al., 2022) and, unlike many familiastic countries, adult children or families are not obligated to support their older parents by law (Anttonen et al., 2003). Moreover, due to long geographical distances, older adults do not always have adult children or family member close by (Åkerman et al., 2021). For these reasons, Finnish older adults may invest and expect more day-to-day social support from other types of social relations outside the family, such as friends and neighbours. However, it is important to note that Finnish society is also constantly changing and the perceptions of social support and its sources are likely to evolve over time. In future research it would be interesting to capture possible changes in social support dimensions by considering also the effects of period and cohort (e.g., Glenn, 2003).
The results of our study demonstrate the advantages of a long follow-up period as it was possible to capture the latent and gradual changes and effects of the lack of social support among the different age groups of older adults that may have been impossible to observe over a shorter period. Moreover, by having 21 years of follow-up, our study shows the linkage between lack of social support and older adult mortality and allows a more accurate assessment of the trajectories of mortality risks among older adults. Further heterogeneity was evident within the health-related social support from nonrelatives dimension. In contrast to previous findings, not receiving health-related social support from nonrelatives acted as a protective factor for those above 70 years in models 3 and 4.
The latter finding aligns with the attributes of selective survival, where a reversal of mortality tends to occur where disadvantaged populations enjoy better health outcomes, good quality of life, and higher survival rates than anticipated (Markides & Machalek, 1984). As the variables used were likely to have an influential bearing on the results, we utilised the social support dimensions, self-rated health, income, education and civil status together with age as a continuous to this effect. The selective survival effect and variations in results underscore the necessity to tailor the care and services of older adults to their specific needs (Nguyen et al., 2021) as well as the role of different dimensions and sources of social support in health promotion throughout the life course.
Overall, the results of this study are consistent with and build on previous literature demonstrating the protective effect of the presence of social support on mortality among older adults (De Brito et al., 2017; Hill et al., 2016; Roth & Peng, 2022; Santini et al., 2015; Wang et al., 2024).
However, the existing literature examines the impact of lack of social support in the short term, ten years or less (Lyyra & Heikkinen, 2006; De Brito et al., 2017; Penninx et al., 1997; Roth & Peng, 2022; Ten Bruggencate et al., 2018; Williams et al., 2019). Hence, this study’s 21-year follow-up period adds to the novelty of these findings and provides more evidence on the life-course influences on health and well-being in older age.
Policy Implications
The findings of this study provide greater understanding of the impact of lack of social support on mortality and lay a foundation for sustainable, informed solutions towards averting mortality risks in old age. As the number of older adults is projected to rise to 149.2 million within the European union by 2050 (European Union, 2019), our findings offer a point of reference for examining how different dimensions and sources of social support could be used as means to promote longer, healthier lives. From a policy perspective, our findings indicate that actions aimed to promote health and well-being of older adults should not focus only on old age, but invest in preventive measures throughout the different stages of life. Moreover, our findings indicate that policies should acknowledge diverse sources of social support and aim to provide arenas for social support also beyond family relations. In practice, this could mean investing in programmes that enhance people’s ability to maintain social relationships in their communities. Moreover, interventions are needed to provide opportunities also to create new social connections in situations where meaningful and supportive social networks do not exist.
Limitations and Strengths
One of this study’s notable limitations is potential sample selection bias, as it is likely that the study population represents a healthier group of older adults who have had the ability to participate in a long follow-up study. Moreover, due to the long 21-year follow-up period our analysis has been limited to measurements used at the beginning of data collection in 1998. Since then, there has been an increase in research on social well-being of older adults and new measurements related to social support have been developed. To our knowledge, the Sarason Social Support Questionnaire is currently less used than during the first wave of data collection and may not detect social support as comprehensively as other validated scales. Moreover, the SSQ has not been expansively used in the Finnish context.
The Cox proportional hazards models also have some limitations, for instance, the models assume that the hazards remain constant during the follow-up. To overcome this limitation, we tested the Schoenfeld residuals with the Stata estat phtest command and this showed that the proportional hazards assumption was met in all the basic models. It should also be noted that the level of social support may vary during the follow-up period. Thus, it is important to keep in mind that the findings of this study reflect social support at the start of the follow-up.
Despite the above limitations, the long follow-up period of 21 years, the high participation rate, the use of validated items of social support at the baseline, and using more than one statistical method may be seen as key strengths of this study. The unique data also offer many opportunities for future research on the topic. The CAIDE study had its third follow-up (CAIDE 85+) in 2019 to 2020 and has the option for updating the administrative data, which provides future opportunities for follow up on the long-term influences of social support among the oldest old.
Conclusions
The present study demonstrated the link between lack of social support for older adults and mortality. While lack of social support predicts mortality among older adults even after 21 years of follow-up, the heterogenous pathways of the ageing process highlighted by this study cannot be overlooked. The selective survival effect and variations in results present within the age groups in our study draw attention to the need for personalised care and services for older adults beyond age group classifications, as individuals may have different needs to those ascribed to their age groups. Although the results showed a significant association between mortality within only two of the three dimensions examined, that is, general social support and health-related social support from nonrelatives, the findings are a beneficial addition to the existing knowledge in furthering our understanding of the pathways and dimensions of social support in increasing the survival rates of older people. This study also showed the importance of social support for the long life expectancy of older adults. Besides its theoretical connotations, this study could serve as a benchmark for developing practical solutions for averting mortality risks among older people.
Footnotes
Abbreviations
CAIDE: Cardiovascular Risk Factors, Aging and Dementia
FINMONICA: Finnish Multinational Monitoring of Trends and Determinants in Cardiovascular Disease study
Ethical Considerations
The study was approved by the Research Ethics Committee of the Northern Savo Hospital District (Finland). All participants gave their informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was financially supported by the European Union’s Horizon 2020 research and Innovation programme under the Marie Sklodowska-Curie (CK, grant number 101034307); Research Council of Finland (IL, grant number 334419); Juho Vainio Foundation; the Finnish Cultural Foundation; The Ministry of Education and Culture, Finland (JK); Yrjö Jahnsson Foundation; Alzheimerfonden (Sweden); Region Stockholm (ALF grant); European Research Council (ERC, 804371); NordForsk NJ-FINGERS grant; Swedish Research Council; Center for Innovative Medicine (CIMED) at Region Stockholm (Sweden); Stiftelsen Stockholms sjukhem (Sweden); Swedish Research Council for Health, Working Life and Welfare (FORTE); Hjärnfonden (Sweden); Alzheimer’s Research and Prevention Foundation (US); Research Council of Finland (Grant number 355265).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
Data will not be made publicly available due to Ethical requirements. External collaborators can apply to the CAIDE study steering group for pseudonymised datasets and/or samples. Application must be submitted to Prof. Alina Solomon (