
Abstract
With rapid aging and the spread of chronic diseases, public eHealth services are helpful tools to monitor their physiological situations and develop healthy behaviors. However, the studies on older adults adopting public eHealth services have been relatively limited. We propose a modified United Theory of Acceptance and Use of Technology (UTAUT) model, considering the unique adoption patterns of older people. Our study shows that older adults adopting patterns are influenced first by social influence (SI) and facilitating conditions (FC), then influenced by performance expectancy (PE) and effort expectancy (EE). This model includes two moderating effects of performance expectancy (PE) and effort expectancy (EE) between two external constructs of social influence (SI), facilitating conditions (FC), and older adults’ behavioral intention (BI) to adopt public eHealth services. A dataset of 510 questionnaires was collected on the use of a self-monitoring telecare device (Babybot) in Hsinchu City, Taiwan. The results demonstrate that SI and FC positively influence older adults’ adoption of public eHealth services. Furthermore, PE positively moderates the relationship between FC and BI, while EE positively moderates the relationships between FC and BI, and between SI and BI. The findings reveal that PE and EE moderate SI and FC in affecting older adults’ adoption of public eHealth services. This modified UTAUT model provides insights into the unique factors that drive older adults’ adoption behavior. This study offers valuable policy and managerial implications for promoting older adults’ adoption of public eHealth services.
Plain Language Summary
The study focuses on the adoption of public eHealth services by older adults, considering the challenges posed by rapid aging and the prevalence of chronic diseases. The modified United Theory of Acceptance and Use of Technology (UTAUT) model is proposed to account for the unique adoption patterns of older people. Social influence (SI) and facilitating conditions (FC) are found to have the greatest influence on older adults’ adoption patterns, followed by performance expectancy (PE) and effort expectancy (EE). The model also includes two moderating effects of PE and EE between SI, FC, and older adults’ behavioral intention (BI) to adopt public eHealth services. Data from 510 questionnaires on the use of a self-monitoring telecare device in Hsinchu City, Taiwan, show that SI and FC positively influence older adults’ adoption of public eHealth services. Additionally, PE and EE are found to moderate the relationships between SI, FC, and BI. These findings provide valuable insights into the factors driving older adults’ adoption behavior and offer important implications for promoting their adoption of public eHealth services.
Keywords
Introduction
Cardiovascular disease, kidney disease, and even the risk of death in older adults with triple-high status (high blood pressure, high total cholesterol, and high blood glucose) are relatively higher than in the general population (Health Promotion Administration, 2016). These health issues have placed significant pressure on the public sector to become more cost-efficient and effective due to the increasing burden of long-term health care and older person health management (Health Promotion Administration, 2016; Park & Kim, 2012). Self-management has effectively reduced the occurrence of triple-high status, slowed its deterioration, and even lowered healthcare spending (Carter et al., 2012; Park & Kim, 2012; Shahbazi et al., 2021). eHealth is an innovative information and healthcare delivery system that, with the help of the internet and citizen-centered public healthcare services, allows people to monitor their physiological situations and develop healthy behaviors more efficiently and effectively (Arfi et al., 2021; Shahbazi et al., 2021; J. Zhou et al., 2020).
Despite the potential benefits of eHealth, its adoption among older adults remains limited (Levine et al., 2016; Peek et al., 2014). Levine et al. (2016) found that the use of eHealth by older people in the USA showed only slight increases from 2011 to 2014. This indicates that eHealth is not popular among older adults, thus hindering its potential to increase access to healthcare services (Levine et al., 2016; Peek et al., 2014). People over 65 are typically less familiar with technology than younger adults, and most older people show degradation in perceptual, motor, and cognitive functions that might hinder their ability to accept technologies (Hou & Hu, 2021; Moore et al., 2021).
Comprehending the factors that influence older individuals’ acceptance of new eHealth services is critical for allocating government resources, particularly budgets, to provide a self-monitoring health environment in an aging society. With appropriate implementation, remote and distant healthcare technology can help older adults effectually cope with their healthcare by encouraging behavior adjustment and facilitating support (Arfi et al., 2021; Hirvonen et al., 2020; Osifeko et al., 2018; Peek et al., 2014). Understanding why older people accept new eHealth services is essential when allocating government resources, mainly budgets, to provide a self-monitoring health environment in an aging society (Cajamarca et al., 2020; Carpenter et al., 2022).
This study aims to modify the UAUAT model to develop the model of older individuals’ eHealth service adoption and an effective eHealth program strategy to facilitate adoption. The study will modify the United Theory of Acceptance and Use of Technology (UTAUT) to examine the impact of government support (GS), social influence (SI), performance expectancy (PE), and effort expectancy (EE) on the adoption of public eHealth services by older adults (Venkatesh et al., 2003).
The continuous rise in the adoption of eHealth services represents an opportunity to improve and manage older adults’ health. However, while the adoption of ICT has been reviewed from many perspectives, research on older adults’ readiness for eHealth services is relatively rare. The united theory of acceptance and use of technology (UTAUT) has been used in numerous studies (Venkatesh et al., 2003). However, while the adoption of ICT has been reviewed from many perspectives, research on older adults’ readiness for eHealth services is relatively rare. Several researchers have extended and examined the UTAUT model in different contexts and contributed to the theory regarding older adults’ eHealth adoption (Arfi et al., 2021; Shahbazi et al., 2021). Meanwhile, based on the observation of older adults’ use of public eHealth services at community care centers, the constructs categorized as external environmental (social influence [SI] and facilitating conditions [FC]) appear relatively more influential to behavioral intention (BI) compared with internal technological (performance expectancy (PE) and effort expectancy (EE).
This research contributes to the understanding of older adults’ eHealth adoption by refining two constructs of social influence (SI) and facilitating conditions (FC) and examining the moderating effects of performance expectancy (PE) and effort expectancy (EE) on behavioral intention (BI) to adopt public eHealth services. Few studies have focused on building a theoretical foundation for older adults’ engagement in eHealth or the impact of government support on eHealth adoption.
Effective eHealth design strategies might emphasize how to provide older people with adequate support for health activities by removing or lessening inconvenience, technology anxiety, and resistance to change with innovation (Arfi et al., 2021; Chen & Chan, 2014; Chu et al., 2011; Hirvonen et al., 2020; Mitzner et al., 2010). However, little attention has been paid to why and how older adults engage in eHealth, and very few studies have focused on building a theoretical foundation and understanding the impact of government support (GS), social influence (SI), performance expectancy (PE), and effort expectancy (EE) on the adoption of a public eHealth service by older people. Therefore, there is a need to develop a theory of older adults’ eHealth service adoption and a strategy for effective eHealth programs that can facilitate their adoption.
The paper is structured as follows: Section 2 constructs a theoretical model for elucidating and predicting the adoption intention of public health services by older people by modifying the UTAUT. Section 3 presents the research methodology. This includes the research design, questionnaire development, data collection, and analysis techniques. Section 4 describes the results and hypothesis development, and the final section presents the conclusions.
Background and Theory
EHealth and Older Adults’ Technology Adoption
The World Health Organization (WHO, 2017) stated that the world population is aging due to a growing proportion of older adults, coinciding with a sharp increase in non-communicable diseases (e.g., heart disease, diabetes, and cancer) and a 77% co-occurrence of multiple chronic conditions. This situation will affect the healthcare system in the future and calls for further preparation (Bähler et al., 2015). Thus, the World Health Organization (WHO, 2016) identifies the promotion of eHealth, an innovative information system and health care delivery system, as a priority. Leveraging the internet and citizen-centered public healthcare services, individuals can more efficiently and effectively monitor their physiological conditions and cultivate healthier behaviors (Arfi et al., 2021; Shahbazi et al., 2021; J. Zhou et al., 2020).
Nazir et al. (2019) argued that the development of the Internet of Things (IoT) and connected devices have contributed to advances in the eHealth service field, allowing older people with chronic diseases to regularly measure body temperature, diet, sleep, blood pressure, glucose, and electrocardiogram, then immediately upload the data to be shared medical facilities. Moreover, improving these technologies can relieve the social burden of aging and accelerate the transition to personalized digital healthcare (Kańtoch & Kańtoch, 2020).
eHealth is becoming a crucial solution. It is expected to improve the quality of life and empower individuals to control and manage their health by providing low-cost and high-quality healthcare (Kańtoch & Kańtoch, 2020). Current solutions involving smart telephones, web-based management, social media eHealth technologies, and low-cost and high-quality healthcare eHealth services have been studied regarding their ability to assist healthcare professionals and personnel in communicating with patients to improve disease management. They are expected to enhance the quality of life, achieve excellent and equitable health and welfare, empower individuals to control their health, and develop and strengthen individuals’ resources to increase independence and participation in society (WHO, 2017).
A variety of studies have highlighted the importance of online-based information systems (IS), information technology (IT), and innovative information and communication technologies (ICT) in the medical industry (Gee et al., 2015; Watkin & Xie, 2014). Also, many studies have consistently demonstrated that teams of pharmacists or nurses who employ eHealth services in patient management can significantly improve the control of chronic diseases (Earle et al., 2010; Park & Kim, 2012; Seto et al., 2012). However, adapting to eHealth technologies is not for older people, and several studies have sought to investigate the determinants of their adoption. Charness et al. (2010) found that older adults’ needs for health concerns and healthcare are higher than those of any other age group and confirmed that more older people are adopting eHealth and are willing to use it. Xie (2011) found that older adults’ adoption and use of technology have lagged behind those of younger people. Older adults may have low eHealth literacy or ability to access, evaluate, and use health information to make medical decisions.
De Veer et al. (2015) also found that 63% of older people would definitely or probably intend to use eHealth services if offered. However, older people who did not believe in eHealth’s advantages and ease of adoption were less prone to use eHealth. Freund et al. (2017) showed that t older adults appeared willing to look for medical information online while being open-minded about using eHealth. Maswadi et al. (2020) indicated that continuous monitoring of older people could reduce sudden accidents and promote immediate response to emergencies.
For older people to successfully use eHealth services, the technical and environmental infrastructures provided by governments and eHealth services and their personal and technology-use factors must be considered. Heinsch et al. (2021) articulated that theoretical perspectives of eHealth interventions currently focus on explaining or predicting acceptance. However, the inherent complexity of eHealth implementation is less well represented in the eHealth and technological adoption literature. Yu et al. (2022) proposed that an integrated acceptance framework (IAF) is useful for identifying factors of eHealth acceptance by older adults to highlight the potential main barriers and facilitators when planning a new adoption scenario. They note that the characteristics of older adults influence the adoption factors of eHealth services by older people, their perceptions of technology, the service content, and social influences from the external environment.
The continuous rise in the adoption of eHealth services represents an opportunity to improve and manage older adults’ health. Thus, questions regarding the determinants and effectiveness of adopting eHealth services for older people remain unanswered. This study elaborates on the relevant determinants of older adults’ adoption of public eHealth services to support and improve their quality of life.
The United Theory of Acceptance and Use of Technology (UTAUT)
Venkatesh et al. (2003) indicate that technology acceptance is a relatively mature research regime with a significant amount of literature. Several models have evolved, mainly based on social psychology, seeking to elaborate on individuals’ acceptance and use of new technologies. More widely accepted theories are the technology acceptance model (TAM), theory of planned behavior (TPB), theory of reasoned action (TRA), motivational model (MM), combined TAM and TPB (C-TAM-TPB), model of personal computer use, theory of innovation diffusion, and social cognitive theory (SCT) (Bandura, 1986; Davis, 1989; Davis et al., 1992; Fishbein, 1967; Fishbein & Ajzen, 1975; Rogers, 2003; Taylor & Todd, 1995).
Later, Venkatesh et al. (2003) created the most representative and integrated theory and model of a more complex framework, synthesizing the eight major technology acceptance models mentioned above: the unified theory of acceptance and use of technology (UTAUT). This model was developed to combine the contributions of the mature yet fragmented studies on technology acceptance and to propose a unified theory to explain individuals’ acceptance and use of technology.
UTAUT has been applied and verified in multiple contexts to motivate individuals to adopt innovative technology and is regarded as a promising theory. Venkatesh et al. (2003) develop UTAUT as a comprehensive synthesis of former technology acceptance research, including four core determinants of behavior intention (BI) and use performance expectancy (PE), effort expectancy (EE), social influence (SI), and facilitating conditions (FC). In the UTAUT model, perceived usefulness (PU), perceived ease of use (PEOU), and subjective norm (SN) of the TAM model are incorporated into PE, EE, and SI; FC is defined as one determinant of BI, and experience, age, gender, and voluntariness of use are added as moderating factors. More specifically, PE, EE, SI, and FC are direct predictors of the intention to use innovative technology, and FC and BI are direct determinants of actual use. Four constructs of PE, EE, SI, and FC explain more than 70% of the variance in BI and around 50% in actual use.
Recent research has employed the UTAUT regarding older adults’ acceptance and use of eHealth services by proposing additional factors affecting their intention to use them (Quaosar et al., 2018; J. Zhou et al., 2020). For example, Quaosar et al. (2018) extend the UTAUT model by adding perceived credibility to older adults’ use of m-health services and assert that the extended UTAUT is an excellent predictive model. J. Zhou et al. (2020) conducted a quantitative meta-analysis synthesizing 25 empirical TAM and UTAUT studies published from 2010 to 2020, categorized into three influencing variables (user individual, product and technology, and environmental characteristics). They validated the factors of PE and EE’s significant positive correlation with BI of older people and SI and FC’s positive correlation.
Among these studies on older adults’ acceptance and use of eHealth, researchers have adopted the extended, transformed, or combined UTAUT model mentioned above to identify acceptance factors and examine the effects of the model on the intentions and use in different contexts (Alsswey & Al-Samarraie, 2019; Cimperman et al., 2016; Hoque & Sorwar, 2017; van Houwelingen et al., 2018; Venkatesh et al., 2003; M. Zhou et al., 2019). However, finding evidence for an appropriate acceptance model or constructing an optimal one is tricky. For developing and testing the models to identify and reflect the multidimensional, dynamic nature and factors of eHealth adoption by older people, this paper elaborates on older adults’ acceptance needs. It more clearly predicts determinants of primary barriers and facilitators.
The Modified Older Adults’ UTAUT
Following the previous studies, this study aims to modify the UTAUT model by elaborating on technological and environmental factors in the model of older adults’ adoption of public eHealth services. Two environmental determinants categorize social influence (SI) into two factors of relationship (RL) and reference (RF) and categorize facilitating conditions (FC) into two factors of government support (GS) and health benefit (HB). Moreover, two technological factors explore performance expectancy (PE) and effort expectancy (EE) as moderators of older adults’ intentions to use local eHealth services. Referring to Venkatesh et al. (2003), this study defines BI, SI, FC, PE, and EE, and proposes hypotheses as follows.
Social Influence (SI) and Behavioral Intention (BI.)
Behavioral intention (BI) is a measure of the strength of older adults’ intention to perform a specific behavior. It reflects the acceptance of the use of eHealth services. Social influence (SI) is the degree to which older people perceive that significant others who influence them believe they should use eHealth services. It reflects relevant determinants of social factors, subjective norms, and impressions from the technology acceptance literature. Relationship (RL) is the degree to which older adults perceive that close others (e.g., family or friends) believe they should use eHealth services. Reference (RF) reflects the degree to which older people perceive that others with reference values think they should use eHealth services.
M. Zhou et al. (2019) investigated older adults’ adoption of telehealth services with the TAM model and indicated that prior studies have been more concerned with the user’s attitude toward technology than social factors. However, their results show that, for older people, social factors are more likely to influence their intention to adopt telehealth services and even improve their health. Osifeko et al. (2018) surveyed 210 respondents in Nigeria on the adoption of eHealth services and suggested that social influence is a vital factor in influencing potential users, as others who are important to potential users can convince them to become users. J. Zhou et al. (2020) employed a quantitative meta-analysis synthesizing 25 empirical TAM and UTAUT studies that validate SI’s significant positive correlation with BI of older people.
Accordingly, recent studies have suggested that positive and negative SI from their families, peers, and friends affect older adults’ technology adoption. Also, the determinant of SI should be re-elaborated into more specific constructs to achieve unique variance (Syed-Abdul et al., 2019; Wang et al., 2021; Xu et al., 2021). Considering the abovementioned rationale, the following hypotheses are proposed:
Hypothesis 1: Social influence (SI) is positively related to older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 1a: Relationship (RL) of social influence (SI) is positively related to older adults’ behavioral intention (BI)to use eHealth services.
Hypothesis 1b: Reference (RF) of social influence (SI) is positively related to older adults’ behavioral intention (BI) to use eHealth services.
Facilitating Conditions (FC) and Behavioral Intention (BI.)
Facilitating conditions (FC) refer to the degree to which older adults believe that an organizational and technical infrastructure exists to support their use of eHealth services (i.e., perceived behavioral control and compatibility). Government support (GS) reflects the degree to which older people believe that government and technical infrastructure exist to support eHealth services. Health benefit (HB) is defined as the degree to which older adults feel that the government’s and technical infrastructure’s benefits exist to support their use of eHealth services.
Vichitvanichphong et al. (2018) showed that with substantial support and resources (e.g., facilitating support) when learning how to use gerontechnology, older people are more willing to adopt due to the advantages of the applications provided for their lives. The more benefits exist to meet older adults’ functional requirements, and the fewer barriers they perceive, the higher their intentions to use (J. Zhou et al., 2020). Schreiweis et al. (2019) conducted a systematic literature analysis on the barriers and success factors of adopting eHealth services. The external environmental barriers include a lack of support, functionality, and information provision about the benefits of eHealth. Key facilitators are the design, delivery, and integration of e-health programs and support for privacy and self-efficacy enhancement in eHealth use. M. Zhou et al. (2019) found through a meta-analysis that FC positively correlates with the BI of older people when the government provides support and promotes the benefits of trustworthy, user-friendly, health-beneficial eHealth services. In promoting eHealth services, the government is regarded as a facilitator and should provide environmental and technological FC for promoting older adults’ adoption. Thus, the following hypotheses are formulated:
Hypothesis 2: Facilitating conditions (FC) are positively related to older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 2a: Government support (GS) of facilitating conditions (FC) is positively related to older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 2b: Health benefit (HB) of facilitating conditions (FC) is positively related to older adults’ behavioral intention (BI) to use eHealth services.
Moderating Effects of Performance Expectancy (PE) and Effort Expectancy (EE.)
Performance expectancy (PE) is reflected in the degree to which older people believe that using eHealth services will help them obtain physical health enhancements and facilitate achieving some goals (i.e., technology will enhance their quality of life). It involves related determinants such as perceived usefulness, extrinsic motivation, and outcome expectations from technology acceptance.
Quaosar et al. (2018) and Zhao et al. (2018) found that PE positively affected older adults’ intention to use gerontechnology, similar to the results of J. Zhou et al.’s (2020) study, which validated the significant positive correlation between PE and EE with BI of older people. However, previous papers have shown that PE may also be a moderator in the relationships between external factors and older adults’ technology adoption.
Arfi et al. (2021) employed the UTAUT model to examine the adoption of eHealth devices and found that PE and EE positively influence BI, but SI and FC have no effect, inconsistent with prior studies. Furthermore, considering the age group of users, they found that older people showed significant changes in the effects of SI and FC and a decrease in the effects of PE and EE. This means that older users may have higher cognitive and physical limitations as well as affiliation needs and rely more than younger people on SI and FC to adopt innovation due to social modeling and influence. Having little experience with eHealth devices and communication skills, they are easily influenced by their family, friends, and other environmental factors. Hoo et al. (2021) found that age significantly moderates speed and security, but not SI or convenience, in adopting e-wallet technology among Malaysians. Older adults, believing that the system is not secure or safe, are less willing to take higher security risks than the young, leading to low adoption by older people. In short, the study found that older adults expect using an e-Wallet to be complex and inconvenient. Moreover, Philippi et al. (2021) verified that internet anxiety moderates the relationship between SI and BI, meaning that SI is especially important for more anxious people. When sufficient information, trust, and support are provided, users can experience relief from their anxiety related to low self-efficacy, perceived ability, and performance of eHealth (Gunasinghe et al., 2019; Petersen et al., 2020).
Accordingly, these studies show that a lower personal perceived value to new technology may strengthen external factors to the intention of adoption. Khazaei and Tareq (2021) examined the adoption of battery electric vehicles (BEVs) and found that users with a higher perceived value toward new technology neglect the influence of social norms on their intention. However, most older adults are regarded as laggard users because the barriers to adopting new technology strongly influence their perceived benefits. In other words, with increasing cognitive and physical limitations and low self-efficacy, older people are easily affected by SI and FC and moderated by PE between SI, FC, and BI. Thus, we formulate the following hypotheses:
Hypothesis 3-1: Performance expectancy (PE) moderates the relationship between social influence (SI) and older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 3-1a: Performance expectancy (PE) moderates the relationship between the relationship (RL) of social influence (SI) and older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 3-1b: Performance expectancy (PE) moderates the relationship between reference (RF) of social influence (SI) and older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 3-2: Performance expectancy (PE) moderates the relationship between facilitating conditions (FC) and older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 3-2a: Performance expectancy (PE) moderates the relationship between government support (GS) of facilitating conditions (FC) and older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 3-2b: Performance expectancy (PE) moderates the relationship between health benefit (HB) of facilitating conditions (FC) and older adults’ behavioral intention (BI) to use eHealth services.
Effort expectancy (EE) refers to the degree of ease associated with using eHealth services, such as ease of use and the determinants and complexity. Some prior researchers have examined the effects of EE on older adults’ BI. Quaosar et al. (2018) and J. Zhou et al. (2020) found that EE positively affected older adults’ intention to use gerontechnology. Moudud-Ul-Huq et al. (2021) verified that EE significantly influences older adults’ intention to use m-health services, in line with Semiz and Semiz (2021) and Wang et al. (2021). However, some previous papers indicated that EE might moderate the relationship between external factors and behavior intention when interacting with older users.
Francisco et al. (2014) confirmed that age significantly moderates the relationship between behavioral intention with external influences, ease of use, and trust due to older adults’ lower technological propensity and greater need for external force by third-party mouth marketing. Ibrahim (2018) found that age significantly regulates SI and moderates the effect of EE on SME employees’ adoption of technology innovations. Moreover, older employees had low expectations of the ease of technology, and SI substantially influenced them. The author suggested that firms should provide facilitating conditions to promote their use intention. Nunes et al. (2019) found that user age moderates between EE, SI, FC, and BI to use mobile health applications, and those older users have a strong linkage between EE and intentions, while SI and FC have differing influences on intention between young and older users. Combining the above results, it can be reasonably inferred that the lower EE of older adults may affect the effect of SI and FC on intention.
These studies revealed that older users have a lower EE for new technologies than younger users. Moreover, SI and FC have a more significant effect on the intention of older users to adopt the technology. In other words, older users have more barriers to using new technologies and are less likely to recognize the ease of use of new technologies, which may lead to a strengthening of the influence of external factors on behavioral intention. Thus, the final hypotheses are postulated:
Hypothesis 4-1: Effort expectancy (EE) moderates the relationship between social influence (SI) and older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 4-1a: Effort expectancy (EE) moderates the relationship between the relationship (RL) of social influence (SI) and older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 4-1b: Effort expectancy (EE) moderates the relationship between reference (RF) of social influence (SI) and older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 4-2: Effort expectancy (EE) moderates the relationship between facilitating conditions (FC) and older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 4-2a: Effort expectancy (EE) moderates the relationship between government support (GS) of facilitating conditions (FC) and older adults’ behavioral intention (BI) to use eHealth services.
Hypothesis 4-2b: Effort expectancy (EE) moderates the relationship between health benefit (HB) of facilitating conditions (FC) and older adults’ behavioral intention (BI) to use eHealth services.
Research Framework
In this study, we focus on the adoption behavior of older adults toward eHealth services, particularly a government-initiated public service. We further assume that there may be an interaction between external environmental factors and the perceptions of new technologies since the attitude of older people toward new technologies influences their intention to use them. Therefore, we propose a modified UTAUT model (Figure 1) to illustrate the potential behavioral patterns of technology adoption among older adults.
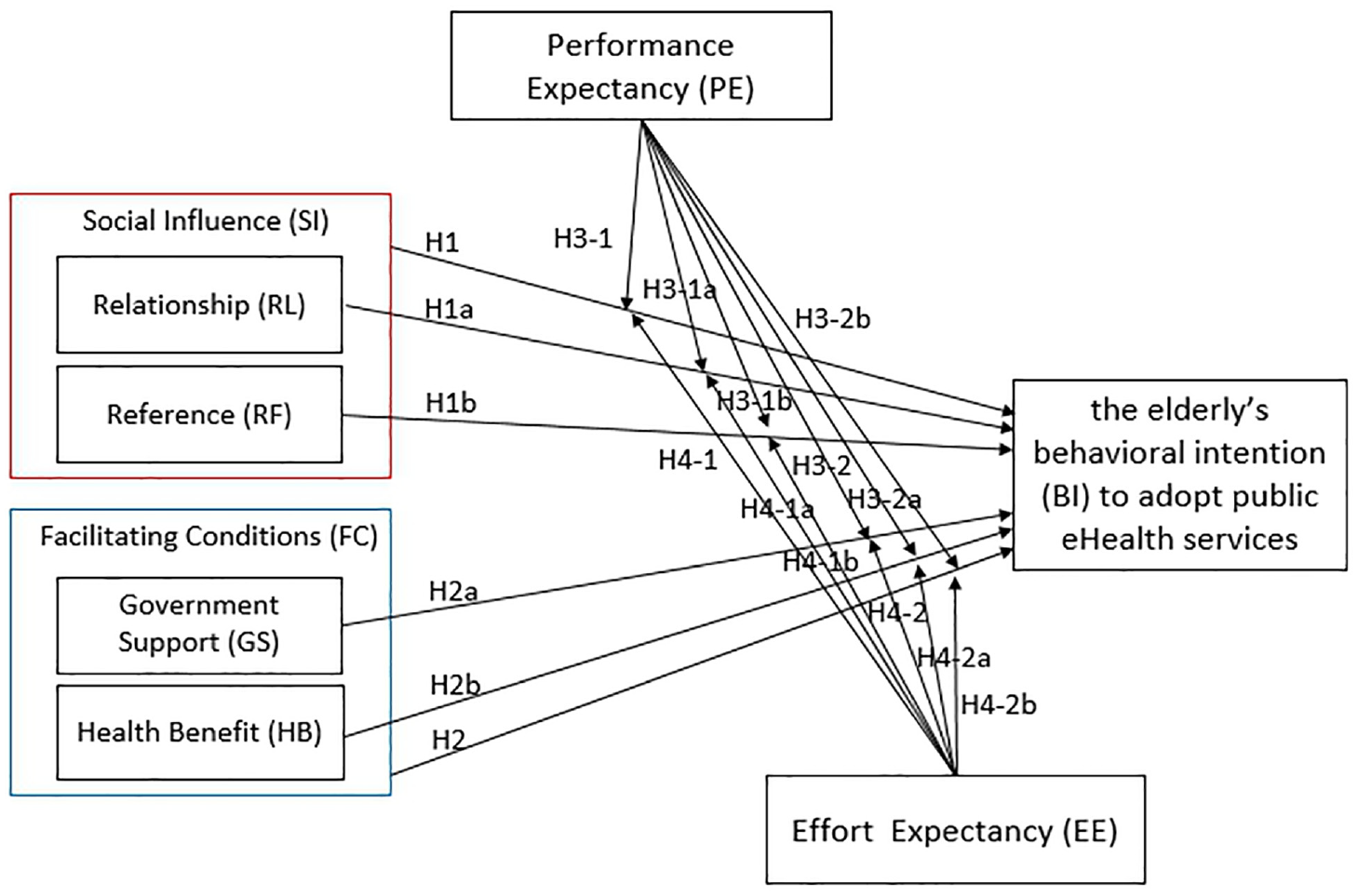
Modified UTAUT Model: moderation and behavioral intention.
Methodology
Taiwan’s Public eHealth Service
Taiwan’s public eHealth service is still in its infancy, mostly focused on developing and deploying the systems or devices and system quality assessment. Many agencies have invested in relevant industries and actively developed the market, and public eHealth service platform platforms have gradually matured. The government has also invested substantial resources and effort to promote and support the market to encourage more users to adopt public eHealth services; these efforts include funding, system architecture, choice of location, and personnel training programs.
The Hsinchu city government is the first to promote a smart city by launching the “Hsinchu Citycard” (citizen card) project in Taiwan (Figure 2) and providing older adults with the public telecare equipment “Babybot” and convenient, smart eHealth services. In 2014, the government established an eHealth management system in the public health bureau, with a self-monitoring tool in 28 community care centers (Figure 3).

Hsinchu Citycard for older adults.
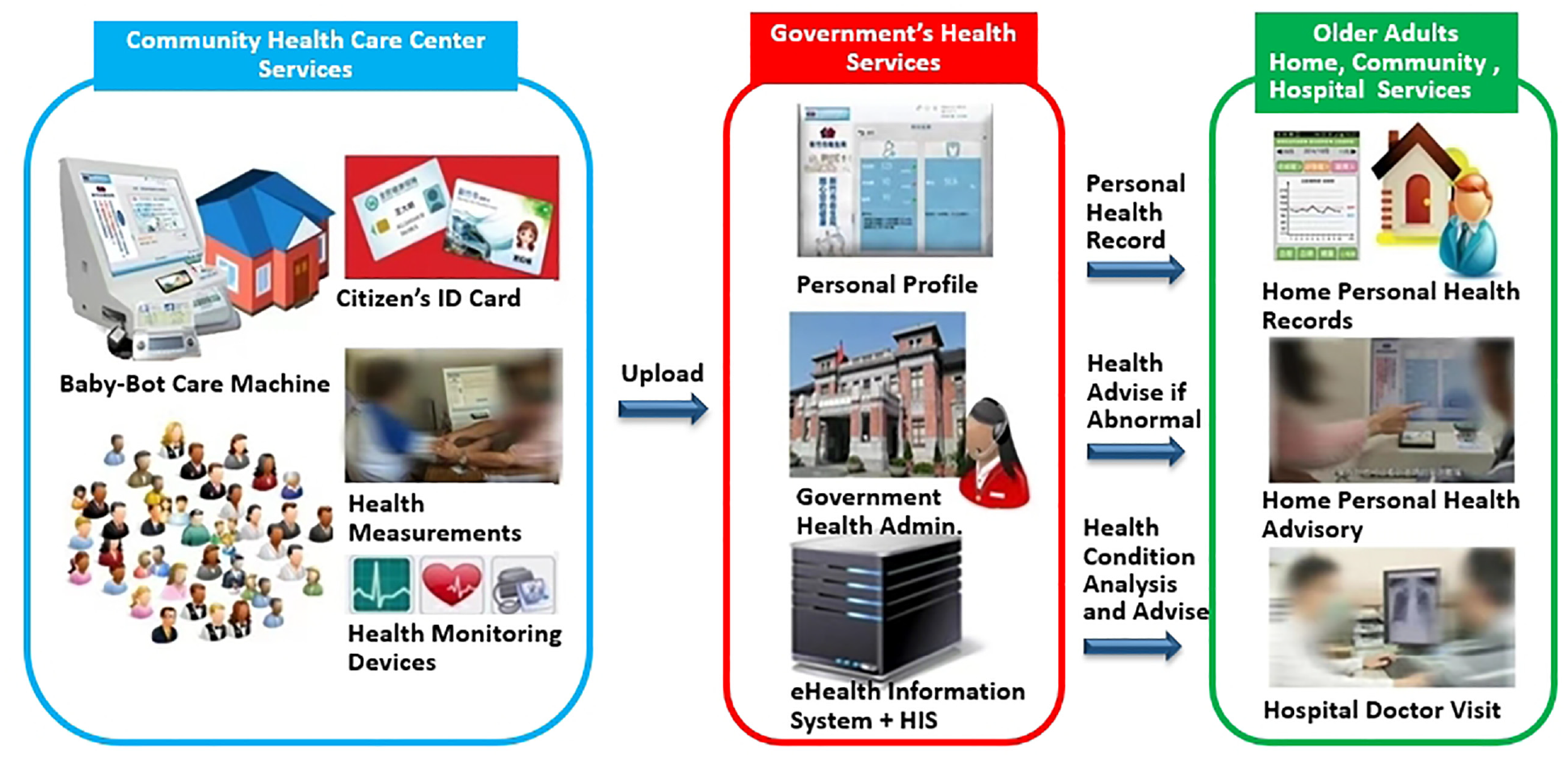
The eHealth management system of Hsinchu City.
Older adults can measure blood pressure, weight, and other vital signs free of charge using a citizen card or insurance card along with health information using the cloud platform, thereby reducing the complexity of personal identity information when undergoing a health examination. Afterward, health promotion staff within the health department can target high-risk cases through tracking and follow-up care to help each patient rebuild a healthy life.
In addition, anyone can go to public health institutes to check their health information, as this card is integrated into the hospital information management system (Hospital Information System, HIS). The ability to track one’s blood pressure and other vital health indicators will positively affect older adults’ health and help enhance personal health awareness and management.
Research Design
To explore the factors influencing the adoption of eHealth services among older adults, this study uses the Babybot and eHealth services introduced by the Hsinchu City Government as a case study. The research employs a questionnaire to assess the attitudes and intentions of older participants toward the adoption of this public service.
Regarding the questionnaire, all measures for each factor have been validated through previous research. Nineteen items of the five variables are adapted from the widely accepted UTAUT model developed by Venkatesh et al. (2003), including 4 items of behavioral intention (BI), 4 items of social influence (SI)— relationship (RL), 4 items of facilitating conditions (FC)—government support (GS), 4 items of performance expectancy (PE), and 3 items of effort expectancy (EE). Four items of SI—reference (RF) are also derived from Venkatesh et al. (2003). Three items of FC—health benefit (HB) are derived from Rogers (1983). Moreover, this study contains five demographic information items of gender, age, education, living status, and working status.
While generating the list, the researchers conducted personal interviews with domain experts (two from each community care center, a volunteer manager, and an administrator) until further questionnaire adjustments were necessary. The completed questionnaire consisted of two parts. One part recorded the subject’s demographic information, while the other part contained 26 measurement items detailing the subject’s perception of the seven factors in the model. The items are measured using a 5-point Likert-type scale (1 = strongly disagree, 5 = strongly agree).
Data Collection
The questionnaire was pretested with 40 older adults in Hsinchu City, Taiwan, and minor changes were made to the items and wording of several questions. Ethical approval for this study was granted in accordance with the tenets of the Declaration of Helsinki.
The data collection used were snowball and convenience sampling, and face-to-face interviews were used for the questionnaire surveys instead of the more typical postal or telephone survey. Currently, the application of eHealth services in Taiwan is only at an early stage. Only medical centers and a few regional communities have fully implemented or partly applied the eHealth services for older adults. A convenience sample of 560 older adults from 28 community care stations in Hsinchu City in northern Taiwan was invited to participate in the study in 2015.
This research endeavored to find specific volunteer managers of community care stations to invite older adults with actual local eHealth service experiences in the community (not at home) to raise the response rate and assist in conducting the self-administered questionnaires. In this study, we also provided explanations using a neutral language (Taiwanese/Hakka) when necessary to address potential concerns related to survey response strategies, cultural comprehension, and response issues. This approach aimed to minimize potential errors that could arise from social desirability and interviewer bias, ensuring that respondents could understand the questions and respond more accurately (Nymberg et al., 2019; Schwarz et al., 2010).
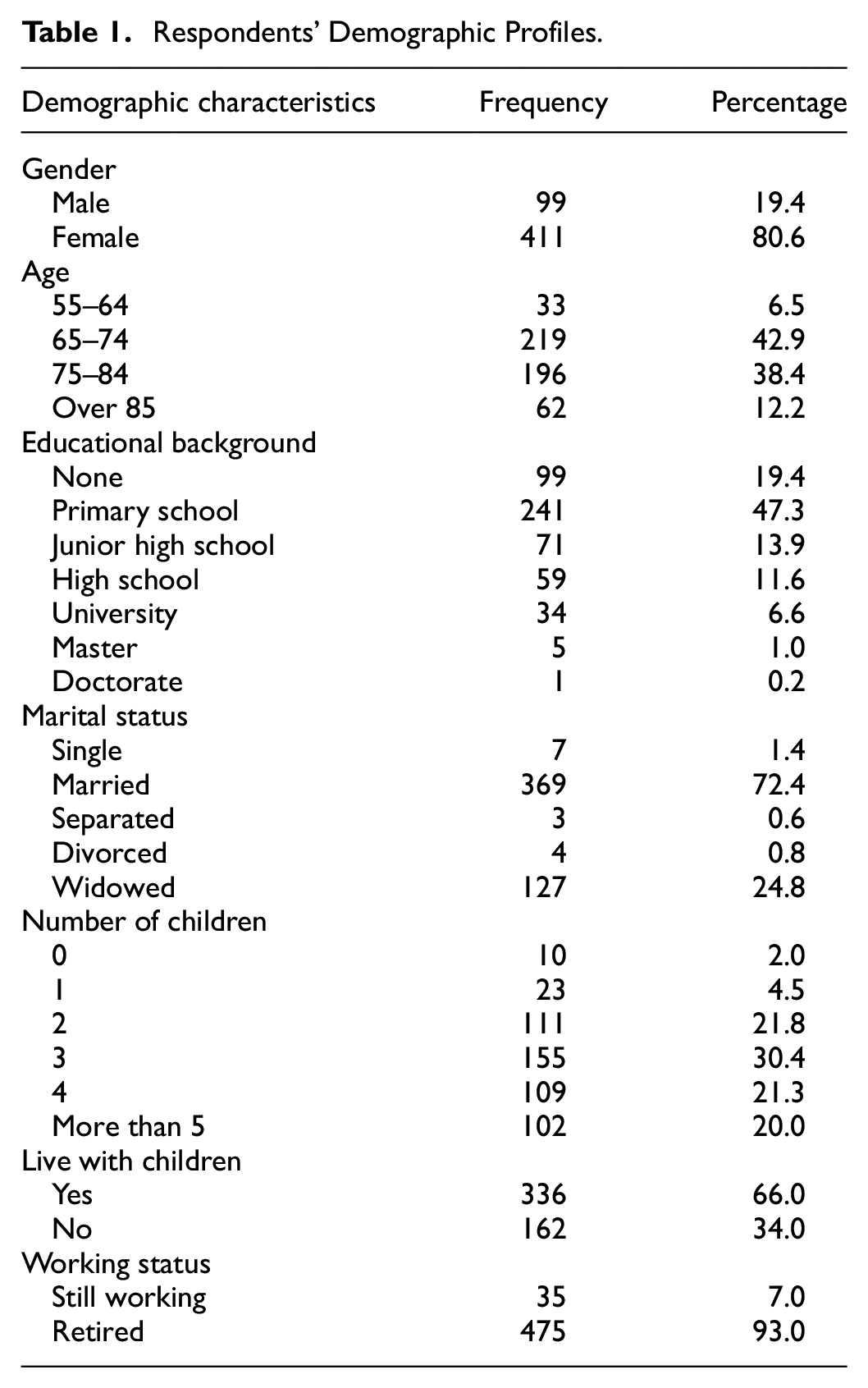
Five hundred and sixty questionnaires were collected. Fifty respondents gave unfinished answers, and their responses were removed from the study, leaving 510 valid questionnaires for further statistical analysis. Table 1 shows the respondents’ profiles. The majority of the respondents were female (80.6%) and married (72.4%), nearly half (49.4%) were aged from 55 to 74 and had a primary school education (47.3%), and most had 2 to 4 children (73.6%). These respondents are likely to represent the older adult population of Taiwan generally. To account for the impact of respondent characteristics on the intention of older people to use eHealth services, these characteristics were transformed into corresponding control variables. For instance, “gender” was denoted as a dummy variable with “male” being represented as 1; “age” was measured on a 4-point Likert scale replacing the original four intervals; “education level” was scaled on a 7-point Likert scale; “living with children” was denoted as a dummy variable with “yes” being marked as 1; and “working status” was also coded as a dummy variable with “still working” assigned a value of 1.
Respondents’ Demographic Profiles.
Estimation Techniques
The statistical analyses were performed using SPSS 26.0, with a significance level set at 0.05, except for the confirmatory factor analysis conducted using AMOS 26.0. Pearson’s correlation was used to assess the relationship between variables. Stepwise hierarchical linear regression models with ordinary least squares (OLS) estimation were employed for hypothesis testing. The approach outlined by Baron and Kenny (1986) was followed to examine moderation effects.
Validity Checks
As indicated in Appendix 1, a six-factor scale is used to measure behavioral intention (BI) in terms of (1) relationship (RL) of social influence (SI); (2) reference (RF) of social influence (SI); (3) government support (GS) of facilitating conditions (FC); (4) health benefit (HB) of facilitating conditions (FC); (5) performance expectancy (PE); and (6) effort expectancy (EE). These seven items were loaded on a single factor (Cronbach α = .91, eigenvalue = 1.82), with factor loadings ranging from 0.61 to 0.91, above the cutoff value of 0.5. This research controls for gender, age, education, living with children, and working status.
Separate exploratory factor analyses were conducted to test whether the observed multi-item measures are related to their corresponding factors. Convergent validity is established by the reliability scores of the factors from 0.82 to 0.95, above the critical value of Cronbach’s α = .7. The average variance extracted (AVE) for every factor from 0.60 to 0.84 is higher than 0.5. Together, these outcomes establish the construct validity of our measures.
Discriminant validity is established through exploratory and confirmatory factor analysis to verify our constructs using all items from the scales. To test the hypotheses, the exploratory factor analysis replicates the determinants of older adults adopting eHealth services. The items loaded onto the intended factors have eigenvalues greater than one (Appendix 1). Moreover, the analysis does not reveal a single or general factor suggesting the presence of a common method (Brewer et al., 1970) or social desirability bias (Thomas & Kilmann, 1975).
This paper conducted a confirmatory factor analysis to validate the proposed determinants of adopting eHealth services by older adults to a seven-factor structure (i.e., RL of SI, RF of SI, GS of FC, HB of FC, PE, EE, and BI). The model shows adequate model fit, χ2 = 519.10, df = 278, p < .001; Goodness-of-Fit Index (GFI) = 0.92, Non-Normed Fit Index (NNFI) = 0.95, Comparative Fit Index (CFI) = 0.92, Root Mean Square Error of Approximation (RMSEA) = 0.044, and Standardized Root Mean Square Residual (SRMR) = 0.03.
Results
Descriptive Statistics
Descriptive statistics for all the variables are presented in Table 2. Among 510 older adults, most are no longer working (93.0%) and live with children (66.0%). The mean of performance expectancy (PE) (μ = 4.015) is higher than the mean of all variables of EE (μ = 2.068), RL of SI (μ = 3.841), RF of SI (μ = 3.861), GS of FC (μ = 3.867), HB of FC (μ = 3.793), and BI (μ = 3.827), showing that older person has a higher PE than any other variables. This indicates that older people feel that using Babybot would help improve the quality of their health.
Means, Standard Deviations, and Correlations.

p < .05. **p < .01. ***p < .001; two-tailed test.
Moreover, the mean of EE (μ = 2.068) indicates that older adults disagree with EE to some extent. This means older people do not think operating Babybot is or will be easy for them. Among the remaining variables of RL, RF, GS, HB, and BI, all μ values are near 4, indicating that older adults intend to use Babybot to some extent due to their family, friends, and others’ influence as well as GS and HB.
The correlation between male and education (γ = .166) is positively significant, implying that older males have a higher level of education. The correlation between age and education (γ = −.326) is negatively significant, suggesting that older individuals tend to have lower levels of education. The correlation between PE and age (γ = −.127) is negatively significant, indicating that older adults are less likely to expect that Babybot will contribute to improving their health.
The correlation between EE and age (γ = −.236) is negatively significant, indicating that older individuals tend not to perceive using Babybot as easily. The correlation between EE and education (γ = .279**) is positively significant, suggesting that those with higher levels of education among older adults find using Babybot easier. The correlations between RF (γ = .099), HB (γ = .110), BI (γ = .110), and education are all positively significant, suggesting that as education levels increase among older people, they are more likely to develop a positive impression of Babybot when observing others using it, perceive its benefits more readily, and be more willing to adopt Babybot.
Tests of Hypotheses
This study tests the four hypotheses using ordinary least squares (OLS) regression, and the results are as follows (Table 3). H1, which postulates a positive relationship between SI and BI, is supported (β = .709, p < .001). H1a, which postulates a positive relationship between RL of SI and BI, is also supported (β = .282, p < .001). H1b, which postulates a positive relationship between RF of SI and BI, is also supported (β = .504, p < .001).
The Estimations of SI and FC On Older Adults’ Adoption Intention.

Note. Computed by OLS regression.
p < .10. *p < .05. **p < .01. ***p < .001.
H2, which postulates a positive relationship between FC and BI. (Table 3), is supported (β = .723, p < .001). H2a, which postulates a positive relationship between GS of FC and BI, is also supported (β = .252, p < .001). H2b, which postulates a positive relationship between HB of FC and BI, is also supported (β = .597, p < .01).
H3-1 (Table 4) postulates that PE moderates the relationship between SI and BI, and PE positively but partially moderates (β = −.519, p < .10, Figure 4). H3-1a postulates that PE moderates the relationship between RL and BI, and PE also positively but partially moderates (β = −.592, p < .10, Figure 5). H3-1b, which postulates that PE moderates the relationship between RF and BI, is not supported (β = .113).
The Moderating Effects of PE and EE on the Influence of SI.

Note. Computed by OLS regression.
p < .10. *p < .05. **p < .01. ***p < .001.

Moderating effects of PE slack on the relationship between SI and BI.

Moderating effects of PE slack on the relationship between RL and BI.
H3-2 (Table 5), which postulates that PE moderates the relationship between FC and BI, is not supported (β = −.359). However, H3-2a, which postulates that PE moderates the relationship between GS and BI, is supported (β = −.783, p < .01, Figure 6). H3-2b, which postulates that PE moderates the relationship between HB and BI, is not supported (β = .159).
The Moderating Effect of PE and EE on the Influence of FC.

Note. Computed by OLS regression.
p < .10. *p < .05. **p < .01. ***p < .001.
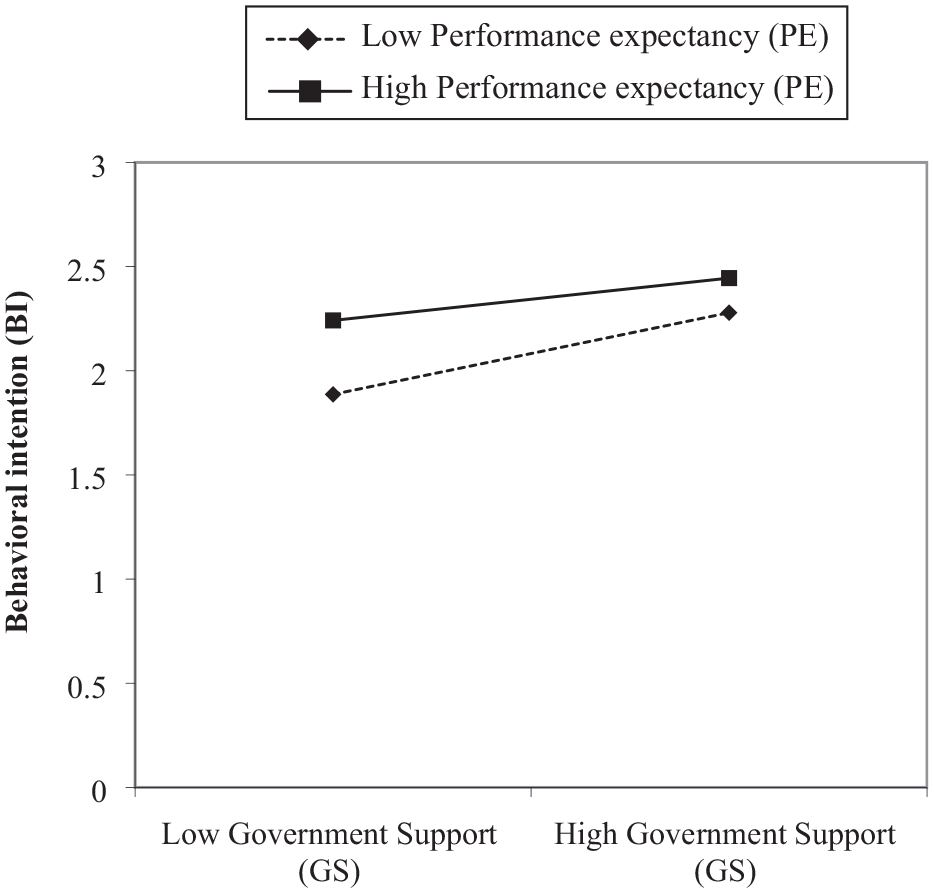
Moderating effects of PE slack on the relationship between GS and BI.
H4-1 (Table 4), which postulates that EE moderates the relationship between SI and BI, is not supported (β = .016). In contrast, H4-1a, which postulates that EE moderates the relationship between RL and BI, is supported (β = −.689, p < .01, Figure 7). H4-1b postulates that EE moderates the relationship between RF and BI, and EE positively but partially moderates (β = .490, p < .10, Figure 8).

Moderating effects of EE slack on the relationship between RL and BI.

Moderating effects of EE slack on the relationship between RF and BI.
H4-2 (Table 5), which postulates that EE moderates the relationship between FC and BI, is not supported (β = −.311). However, H4-2a, which postulates that EE moderates the relationship between GS and BI, is supported (β = −.475, p < .05, Figure 9). H4-2b, which postulates that EE moderates the relationship between HB and BI, is not supported (β = −.015).

Moderating effects of EE slack on the relationship between GS and BI.
Discussions
The results indicate that SI, RL, RF, FC, GS, and HB positively and significantly affect older adults’ BI to adopt eHealth services, and FC has a more significant effect than SI on BI. This implies that FC is the most significant factor for system success. These results are in line with the findings of most previous studies on this subject (Osifeko et al., 2018; Quaosar et al., 2018; Syed-Abdul et al., 2019; Wang et al., 2021; Xu et al., 2021).
Regarding SI, including RL and RF, the results show that with family members, peers’, friends’, and others’ encouragement, recommendation, and advice, older adults will feel more self-confident in using eHealth services. Older people seem to care about the opinions of close others, which enhances their confidence in adopting eHealth services. Thus, they will probably utilize to use eHealth services frequently. This research echoes previous studies, which confirmed that family, peers, friends, and socially and culturally important or influential people play vital roles, as described above (Hoque & Sorwar, 2017; Wang et al., 2021).
Moreover, the results show that FC, including GS and HB, positively correlates to older adults’ BI to use eHealth services. FC is a critical factor in the success of eHealth services and also acts as a crucial and significant determinant in promoting and implementing eHealth services. Therefore, the government’s efforts in promoting and offering training programs for a trustworthy, user-friendly, health-beneficial provider of eHealth services will encourage and assist older people in accepting the new technology. Since the public eHealth service is provided by the government and guided by government policy, older adults will feel more secure and comfortable in delivering their sensitive personal health information online and more confident in adopting eHealth services. Our study also supports past research findings that with better privacy policies, eHealth use will increase (Vassli & Farshchian, 2018; Zhang et al., 2019).
In addition, regarding the moderating effects of PE and EE, the primary result shows that PE positively moderates the relationship between GS and BI, while EE positively moderates the relationships between BI on the one hand and GS and RL on the other. PE partially moderates the relationship between SI, RL, and BI, and EE partially moderates the relationship between RF and BI. These indicate that an older adult with low (vs. high) PE/EE who receives high GS, RL, and SI will show a greater increase in BI. However, when receiving high RF, an older adult with high (vs. low) EE will show a greater increase in BI. With trustworthy, user-friendly eHealth services provided by the government and with family members’ and friends’ encouragement, recommendation, and advice, older adults will feel more secure and confident in using eHealth services, especially those who originally showed low (vs. high) PE/EE. Older people care about the opinions of others close to them, and adequate government support can boost their confidence to adopt eHealth services. However, others’ encouragement, recommendation, and advice will increase the use intention more among older adults with high (vs. low) EE. That is, older people who expect eHealth services to be easy to adopt are more likely to use eHealth services due to others’ encouragement (Kim & Chung, 2017). Consequently, the constructs categorized as external environmental of SI and FC interacted with the constructs categorized as internal perceived technology value of PE and EE to enhance older adults’ behavioral intention to use public eHealth service.
Conclusions
eHealth services are designed to enhance people’s quality of life. However, the efficacy of public eHealth services in achieving this objective remains uncertain, as their adoption has not yet become widespread in Taiwan. In order to improve the quantity and quality of eHealth services, it is crucial for eHealth researchers to seriously consider the willingness of older users to adopt such services. This paper advocates for a more comprehensive focus in future research on the factors influencing older individuals’ willingness to embrace eHealth services, whether in terms of product or service design or their role in health promotion.
Utilizing a developed model as a theoretical foundation, our study on older adults’ adoption of eHealth services reveals that the influence of various factors still differs based on users’ attitudes toward adopting innovative technologies. The older population faces more barriers to using new technologies, leading to lower awareness of effort expectancy (EE) and performance expectancy (PE), which are internal technological factors. Consequently, their intentions to adopt eHealth services are more likely to be swayed by social influence (SI) and facilitating conditions (FC), both external environmental factors.
We propose a modified Unified Theory of Acceptance and Use of Technology (UTAUT) model, with the results demonstrating an interplay between external environmental factors and internal technological factors in shaping older adults’ intention to use eHealth services. This study suggests that the primary focus for predicting older adults’ intention to use public eHealth services should be on government support and recommendations from close acquaintances. Such support should encompass government policy interventions highlighting the benefits of using e-health services, promotion strategies, volunteer assistance, and the effectiveness and convenience of utilizing these services.
Our proposed modified UTAUT model for older adults’ eHealth service adoption serves as a bridge between technology engineering and health promotion research, paving the way for future research directions that can enrich the work of eHealth specialists.
Findings
Our research findings underscore the pivotal role of Facilitating Conditions (FC) in the success of eHealth services, contributing significantly to the Behavioral Intentions (BI) of older adults to adopt these services. Government interventions were found to be crucial for the successful implementation and promotion of eHealth services. This suggests a need for carefully crafted eHealth policy and promotion programs before the system is made publicly accessible. Further, our research underlines the necessity for eHealth services to be perceived as beneficial, popular, and socially and culturally accepted within the older adults’ community. The role of the government in providing user-friendly service interfaces and guiding the design flow to assist older users is emphasized.
Additionally, we found that the trustworthiness of government-provided eHealth services, combined with the encouragement, recommendation, and advice from family members and friends, considerably increased older adults’ sense of security and confidence in using these services. This was particularly true for those individuals who initially exhibited low performance expectancy (PE) and effort expectancy (EE) toward eHealth services. These findings show that social influence (SI), such as the opinions of close acquaintances and adequate government support can significantly boost older adults’ confidence to adopt eHealth services.
Interestingly, our findings suggest that encouragement, recommendations, and advice from others could increase the usage intention more among older people with high (vs. low) EE. In other words, older individuals who expect eHealth services to be easy to adopt are more likely to use such services due to encouragement from others (Kim & Chung, 2017). Consequently, these constructs categorized as external environmental factors, such as SI and FC, interacted with those categorized as internal perceived technology value factors, such as PE and EE, to enhance older adults’ behavioral intention to use public eHealth services.
Implications for Research
This research contributes significantly to our understanding of factors driving the success of eHealth services, particularly for older users. Our findings underscore the critical role of Facilitating Conditions (FC) in influencing the behavioral intentions of older adults to adopt such services. Therefore, the considerable impact of government interventions highlights a need for strategic policymaking in implementing and promoting eHealth services.
This research brings forward the idea of eHealth services not merely as a technical tool but as a socially and culturally embedded activity in the community of older adults. The study illuminates how the perceived utility, popularity, and cultural acceptability of eHealth services can significantly enhance older people’s intention to use them. These findings may guide future research to explore further the social and cultural dimensions of technology acceptance among older adults.
Additionally, our research sheds light on the role of age-friendly service design in facilitating the adoption of eHealth services. This implies that future studies should pay greater attention to user experience and interface design, particularly for older users with different needs and limitations than younger demographics.
Another key contribution of our research is highlighting the role of volunteers in adopting and using eHealth services. We propose that future research should examine more deeply the role of volunteers, their training needs, and the impact of their engagement on the overall success of eHealth services.
Finally, our findings suggest that public acknowledgment of the use of eHealth services by policymakers can foster a positive attitude toward these services in the older adult community. Future research should delve into the role of public acknowledgment and other similar societal interventions in promoting the adoption of eHealth services. These findings collectively provide new directions for future research to enrich our understanding of the factors influencing older people’s adoption of eHealth services.
Managerial Implications
These findings hold significant implications for policy development. The government should focus on providing user-friendly and trustworthy eHealth services, which are of paramount importance for fostering older adults’ adoption. Our research also emphasizes the role of social influence in older adults’ intention to use eHealth services. Policymakers should consider strategies to increase social influence, such as encouraging family and friends to recommend eHealth services.
The findings of our study emphasize the need for an effective governmental strategy when it comes to implementing eHealth services for the older population. Government bodies should prioritize developing accessible and user-friendly interfaces tailored to the unique needs of older users. Ease of use and comprehension are vital considerations and could make the difference between adopting or rejecting such services.
The trustworthiness of government-provided eHealth services is another critical factor. The government must ensure the highest level of data security and privacy protection and the reliability and accuracy of the provided health information. This will go a long way in building user confidence and fostering adoption among older adults.
In addition to these, our research has also highlighted the significant role of social influence in driving the adoption of eHealth services. Hence, government initiatives should create a supportive social environment, where friends, family members, and healthcare providers actively encourage older people to use these services. These encouragements should be paired with education about the benefits of eHealth services and potentially even demonstrations on how to use them effectively.
Moreover, the government should consider implementing a comprehensive volunteer program for eHealth services. Volunteers can offer additional support to older users, helping them navigate the system and troubleshoot any issues they might encounter. This could significantly reduce the effort expectancy for older adults and promote usage.
Finally, the government should acknowledge and praise the public use of eHealth services. For example, the government, by declaring initiative to activate older adults’ eHealth services, deploying volunteers for assistance, establishing an extensive network of eHealth service centers, conducting enticing lottery promotions, and recognizing older individuals who use eHealth services, has taken significant measures to promote and support eHealth adoption. Such public acknowledgment could reinforce positive attitudes toward these services and signal their importance and relevance in today’s society. This strategy could contribute to making eHealth services a socially accepted and culturally endorsed activity within the community of older adults.
Limitations
This research adopted a series of processes of model design, measure development, sampling, and statistical analysis. As a result, it achieved excellent internal validity. Nevertheless, this research has some limitations, which provide opportunities for future exploration. First, while the conclusions of this research applied to the public eHealth service setting and this model was validated in community care stations, care should be taken in generalizing the findings to eHealth services used in homes or communities.
Second, the study only examines the effect of local government policy; thus, more studies are needed to explore whether the central government can effectively affect the user’s intention through policy design. Another factor not evaluated is the eHealth services’ dependence on the participants’ intrinsic motivation. The design of the service system itself is based on the user’s needs and motivation for health care. With government policy support and reinforcement, such as an age-friendly system design, volunteers’ support in helping older adults use the system, and positive rewards for using it, the eHealth service system can function more effectively. However, even the most positive, supportive environment may not be able to overcome the limitations caused by some intrinsic factors. Undoubtedly, for non-users, it will be more or less a complicated minimum level that needs to be evaluated in future studies.
Footnotes
Appendix 1
Items and Factor Analysis.

| Factor loading | |
|---|---|
| Relationship (RL) of Social influence (SI) (eigenvalues = 11.168, α = .947) | |
| 1. My family members who influence my health behaviors think I should use Babybot. | 0.776 |
| 2. My family members who are very important to me think I should use Babybot. | 0.827 |
| 3. My friends who influence my health behaviors think I should use Babybot. | 0.837 |
| 4. My friends who are very important to me think I should use Babybot. | 0.783 |
| Reference (RF) of Social influence (SI) (eigenvalues = 1.075, α = .900) | |
| 1. Other people think I should use Babybot. | 0.748 |
| 2. Watching others use it can increase my positive perception of Babybot. 3. I think it’s very important for most people to adopt Babybot. |
0.717 0.742 |
| 4. I can see the benefit of others using Babybot. | 0.608 |
| Government support (GS) of Facilitating conditions (FC) (eigenvalues = 1.328, α = .823) | |
| 1. The Health Bureau helps me to use Babybot. | 0.616 |
| 2. The Health Bureau has assigned volunteers to assist me in using Babybot. 3. The Health Bureau helps me to use Babybot by establishing many Babybot stations. 4. The Health Bureau helps me to use Babybot by designing lucky-draw promotions. |
0.824 0.699 0.683 |
| Health benefit (HB) of Facilitating conditions (FC) (eigenvalues = 1.050, α = .906) | |
| 1. Using Babybot can help me reduce the number of visits to the hospital or clinic. | 0.681 |
| 2. Using Babybot can help me reduce the cost of health management. | 0.645 |
| 3. Using Babybot can increase the convenience of my health management. | 0.790 |
| Performance expectancy (PE) (eigenvalues = 2.477, α = .901) | |
| 1. Using Babybot can help to manage personal health easily. | 0.807 |
| 2. Using Babybot can help to improve the quality of personal health status control. | 0.793 |
| 3. Using Babybot can help to control personal health status. 4. Using Babybot can help to improve personal health status control. |
0.741 0.736 |
| Effort expectancy (EE) (eigenvalues = 1.290, α = .899) | |
| 1. Learning how to operate Babybot is easy for me. | 0.843 |
| 2. Babybot is easy to use, and I can operate it independently. | 0.914 |
| 3. Operating Babybot is easy for me. | 0.871 |
| Behavioral intention (BI) (eigenvalues = 1.817, α = .912) | |
| 1. If possible, I’m going to use Babybot for self-health management. | 0.740 |
| 2. In the future, I would be willing to use Babybot to manage my health conditions. 3. In the future, I would be willing to recommend that others use Babybot. |
0.774 0.746 |
| 4. Overall, my willingness to use Babybot is high. | 0.690 |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.