
Abstract
Police safety and use of force decisions during critical incidents are an ongoing source of concern for both police practitioners and the public. Prior research in the area of police performance reveals that psychological and physiological stress responses during critical incidents can shape the outcome of the incident, either positively or negatively. The goal of this study was to test a training method to improve use of force decision making among police. This randomized controlled pilot study consisted of training officers to apply techniques to enhance psychological and physiological control during stressful critical incidents. Of a pool of 80 police officers, potential participants were invited based on equivalent age, years of experience, physiological characteristics (i.e., body mass index [BMI] and cardiovascular reactivity), and expertise. Results revealed that the intervention group displayed significantly better physiological control, situational awareness, and overall performance, and made a greater number of correct use of force decisions than officers in the control group (all ps < .01). The relevant improvements in use of force decision-making found in this pilot study indicate that this training method warrants further investigation. Improved use of force decision making directly translates into potential lifesaving decisions for police and the civilians they are working with.
Keywords
There is no other job like a police officer’s, that requires someone to deliberately go out and actively search for dangerous situations where their life or someone else’s life may be threatened.
Police safety and use of force decisions during critical incidents are an ongoing source of concern for both police practitioners and the public. This concern is evidenced by extensive media coverage of this issue. A recent news article in the Wall Street Journal (WSJ) highlights both the sky rocketing cost of police-misconduct cases and the growing public distrust of the use of force decisions made by police officers. The authors of the WSJ article used data gathered from public records and report that among the U.S. cities with the 10 largest police forces, there has been a 48% increase in costs of police-misconduct cases since 2010 (Elinson & Frosch, 2015). The authors further reported, “Those cities collectively, paid out $1.02 billion over those 5 years (2010-2015) in such cases, which include alleged beatings, shootings and wrongful imprisonment” (Elinson & Frosch, 2015). A significant portion of the billions of dollars spent on policing in North America include arming police officers and training them to make appropriate use of force decisions (Statistics Canada, 2013; U.S. Department of Justice Fiscal Year, 2014). It remains to be examined why questionable use of force decisions continue to be made despite significant resources directed toward police training.
Foundational research in the area of police performance reveals that psychological and physiological stress responses during critical incidents shape the outcome of the incident, either for good or for bad (Arnetz, Arble, Backman, Lynch, & Lublin, 2013; Arnetz, Nevedal, Lumley, Backman, & Lublin, 2009). Maladaptive stress responses during a critical incident put the officer and members of the public at risk of injury or death. Furthermore, maladaptive stress responses can negatively affect an officer’s health and performance over time (Covey, Shucard, Violanti, Lee, & Shucard, 2013; Violanti, 2010). The objective of the current study was to design and test a training method to improve police officers’ stress responses and use of force decision making during critical incidents. The training method was designed to be brief and integrated into existing use of force training programs at police organizations.
How Stress Affects Critical Incident Outcomes
When an individual encounters a potential threat, the body engages in a series of automatic physiological processes in response to the threat. During a physiological stress response, the sympathetic nervous system (SNS) is activated, and the parasympathetic nervous system (PNS), responsible for calming and stabilizing the body, is withdrawn. The degree of a SNS response is determined by one’s cognitive perception of how threatening the stimulus is (Kalisch, Müller, & Tüscher, 2015). Furthermore, the physiological responses during stress can be enhanced or diminished by psychological factors, such as perceived control over the situation. A moderate amount of SNS arousal is beneficial for performing optimally during critical incidents. The benefits of moderate arousal include alertness, focused attention, and improved cognitive performance (Jameson, Mendes, Blackstock, & Schmader, 2010). Moderate arousal facilitates memory formation and memory retrieval (Cahill & Alkire, 2013). During moderate SNS arousal, sensory perceptions including visual, auditory, and olfactory senses are enhanced. Improved sensory awareness increases an individual’s ability to successfully address a threat (Kalisch et al., 2015).
Police work, however, is an inherently a high-risk occupation. Officers routinely face unpredictable, unexpected, and uncontrollable events, all of which are factors that increase the threatening nature of an encounter (Sapolsky, 2004). Furthermore, officers are often required to face these threats under the least ideal conditions, including darkness, unfamiliar territory, and other distractions such as unexpected noise or erratic bystanders. When a stimulus is perceived as very threatening, such as in the case of potential injury or death, an individual experiences a greater degree of SNS arousal. A severe SNS response is colloquially known as the fight or flight response (Lovallo, 2016). Fight or flight is an instinctual survival response comprised of significant neurological, behavioral, and neuroendocrine changes, and is accompanied by negative emotions such as anxiety, fear, and anger (Lipton, 2008; Lovallo, 2016). During a fight or flight response, rapid release of epinephrine from the adrenal gland stimulates an increase in respiration, heart rate, and blood pressure (BP). A heart rate of 100 or above is an indication that the stress response has been activated (Johnson, 2008). Oxygen-rich blood is directed to the major muscle groups in the legs, torso, and arms to support necessary fighting or fleeing action (Lundberg, 2011). Epinephrine signals the liver to release glucose to power the fight or flight response. All non-essential bodily functions, such as digestion and muscle repair, are stopped (Everly & Lating, 2013). The Hypothalamic–Pituitary–Adrenal (HPA) axis is also activated during fight or flight. The HPA axis produces a cascade of hormones that act to maintain the fight or flight response, and importantly, to shut it off when the threat has been resolved. A key regulating hormone in the HPA cascade is cortisol, which is responsible for suppressing immune function and shutting down the fight or flight response (Johnson, 2008). It is important to note that while fight or flight is a purely physiological process, psychological processes, such as threat perception, anxiety, and anticipation stress, can stimulate, maintain, or inhibit the shut off of the fight or flight response. Cortisol is excreted in a dose-response manner to the level of threat the individual perceives (Lovallo, 2016). Aspects of the fight or flight response, including perceptual distortions, reduced motor dexterity, and impaired cognitive function, can be detrimental to use of force decision making during critical incidents (Johnson, 2008).
Perceptual Distortions
During fight or flight, perceptual distortions in sensory information can occur. Sensory distortions include changes in vision, sense of time (i.e., slowing down or speeding up), and a narrowing of auditory information (Klinger, 2006; Klinger & Brunson, 2009). Vision is compromised in three ways: reduced peripheral vision, distance-only eyesight, and forced binocular vision (Olson, 1998). Reduced peripheral vision, also known as “tunnel vision,” is caused by restricted blood flow to the eyes and eye muscle contractions. The eye lens tends to flatten, thus reducing depth perception. The eyes focus on the source of a threat, with heightened attention to visual detail, while ignoring near objects (Olson, 1998). Officers may focus on one single threat, missing other potentially life-threatening cues around them.
Even trained officers are at risk of having a fight or flight response and experiencing the associated perceptual distortions. For example, Westmoreland and Haddock (1989) conducted a study that entailed putting officers through 98 shooting scenarios involving both non-stressful and stressful situations. Findings from this study showed overwhelmingly that even trained officers focused on the immediate threat when confronted with life-threatening situations, at the expense of peripheral awareness. Studies show that during a fight or flight response, an officer’s vision may be compromised by up to 70%, resulting in the failure to detect subtle movements due to loss of peripheral vision (tunnel vision). Olson (1998) reported that it can take up to 440% longer to react when peripheral vision is decreased by 70%. The pupil dilation caused by SNS arousal impairs vision for close objects (4-feet range). SNS arousal disrupts monocular vision and results in the loss of control of the dominant eye (used for precision shooting, that is, monocular vision) inhibiting the ability to focus on a gun sight (Klinger & Brunson, 2009; Siddle & Breedlove, 1995). Visual distortions have implications for using weapons accurately when targets are at close range (Johnson, 2008). The perceptual distortions that occur during fight or flight affect an officer’s ability to see and hear potential threats within their immediate environment. These perceptual distortions combined with a slowed reaction time may directly affect the safety of the officer and the public.
Motor Deficits
During fight or flight, heart-rate and respiration increase, and an individual is more likely to hyperventilate or hold one’s breath, impairing the brain areas affecting fine motor skills (Johnson, 2008). The rapid increase in BP and blood flow to the large muscle groups enhances strength and gross motor skills such as punching, kicking, and running, the very actions needed to fight or flee (Everly & Lating, 2013). However, in regard to fine motor skills, the vasoconstriction of minor blood vessels in the extremities results in the loss of dexterity, cold hands, and muscle tremors (Johnson, 2008). The loss of fine motor skills may compromise an officer’s hand/eye coordination and precision movements necessary to operate weapons optimally.
Cognitive Deficits
A fight or flight response is an instinctual response and happens automatically, without a person deciding whether or not to have one. Vascular processes directed by adrenal hormones (e.g., epinephrine and cortisol) stimulate automatic reactions in the area of the brain called the hindbrain. Automatic instinctual processes are significantly faster than information processed in the pre-frontal cortex, an area of the brain required for memory, decision making, and logical thought (Arnsten & Goldman-Rakic, 1998; Goldstein, Rasmusson, Bunney, & Roth, 1996; Takamatsu et al., 2003). During a fight or flight response, adrenal stress hormones constrict blood vessels, reducing oxygen levels in the pre-frontal cortex, further decreasing an individual’s ability to access stored memories and learned information (Lipton, 2008; Westmoreland & Haddock, 1989). The ramifications of experiencing a severe fight or flight response include difficulty remembering stored information and implementing learned behaviors, all of which may translate into an officer making less than ideal tactical maneuvers and use of force decisions during critical incidents.
Excessive respiration during a fight or flight response may also lead to cognitive deficits. Rapid breathing and hyperventilation lead to dizziness, and even a mental state called “depersonalization” in which the individual feels that they are disconnected from their body (Brown & Gerbarg, 2009). When a person inhales, his or her SNS is dominant. When a person exhales, the parasympathetic nervous system is dominant (Cacioppo & Tassinary, 1998). What this means is that when a person is inhaling rapidly, they are increasing SNS arousal without allowing for the calming effect of the parasympathetic system, which can act as a “brake” to regulate SNS arousal.
In summary, there are both psychological and physiological aspects of the stress response. Psychological aspects include the degree to which a person evaluates a situation or stimulus as a threat. Based on the degree of the threat perceived, the body automatically activates SNS arousal, a physiological response, to meet the level of the perceived threat. Understanding the psychological and physiological mechanisms that underlie stress responses can inform the creation of an intervention to improve police performance during critical incidents. For example, although the fight or flight response is an automatic instinctual reaction to a perceived threat, police officers know that they will routinely be exposed to threatening situations. Therefore, controlling one’s respiration before, during, and after a critical incident is a way to avoid excessive SNS arousal and the associated cognitive, sensory, and motor deficits. Controlled respiration can be learned and practiced as one of a number of psychophysiological techniques to improve use of force decision making during critical incidents (Johnson, 2008).
Improving Police Performance and Safety
Prior research in the area of police stress has not focused specifically on improving use of force decision making. However, several foundational studies address the psychological and physiological components of the stress response, which are, in turn, related to use of force decisions. McCraty and colleagues (McCraty, Atkinson, Tomasino, & Bradley, 2009; McCraty & Atkinson, 2012) designed and tested a stress reduction program for police and correction officers. The program is based on premise that improving self-regulation skills (i.e., emotion regulation and energy levels) and reducing physiological reactivity to stress (i.e., cardiovascular and respiratory activation) would improve officer health and performance outcomes (McCraty & Atkinson, 2012; McCraty et al., 2009). The authors conducted a 16-week study in which they taught officers to practice self-regulation skills and controlled respiration (5-second inhale and a 5-second exhale). McCraty and Atkinson (2012) reported that officers in the training group self-reported improvements in their communication skills at work, and with family, increased positive emotion, vitality, reduced negative emotion and depressive symptoms, and improved self-regulation in response to stress. The authors did not find any significant differences between the trained and non-trained officers on use of force and decision-making skills during critical incident scenarios (McCraty & Atkinson, 2012). Backman, Arnetz, Levin, and Lublin (1997), and Arnetz and colleagues (2009; Arnetz et al., 2013) developed a program to improve police resilience and tested this program via a randomized controlled trial. Their 10-session program (90 min per session) was based on the premise that giving officers the opportunity to practice stress reduction techniques (i.e., relaxation) while listening, via audiotape, to repeated critical incident scenarios and visualizing optimal performance would enhance the perception of predictability and control when facing such events in the real world. The authors reported clinically significant improvements in officer performance and reduced psychological distress when tested on a critical incident scenario 1 year following their training. Andersen and colleagues (2015) conducted the Arnetz et al. (2009) program with special forces police officers. The authors reported that officers displayed reduced SNS arousal while listening to the critical incident scenarios over 1 week of training. However, officers requested more intensive, scenario-based resilience training, better tailored to the high-stress use of force decision making in their real-world encounters (Andersen et al., 2015).
Based on prior research, the current training method was developed specifically to improve police use of force decision making during critical incidents. This training method is called the “international performance resilience and efficiency program” (iPREP). The iPREP method is based on empirical research detailing the psychological and physiological factors that are theorized to most strongly influence use of force outcomes. Specifically, the psychological perception and anticipation of threat, and the associated physiological SNS arousal that, if left unchecked, would result in sensory, motor, and cognitive deficits during critical incidents (Johnson, 2008; Kalisch et al., 2015). Of equal importance is the way in which the iPREP training method is administered. Driskell and Johnston (1998) conducted seminal research comparing methods of training police and military personnel to perform during life-threatening situations. The authors outline the necessary components for training delivery that maximize skill acquisition, retention, and application (Driskell & Johnston, 1998). The authors report that optimal training must include dynamic processes beginning with exposure to the knowledge to be learned in a non-stress environment; training the necessary skills in an increasingly stressful and realistic environment; and providing opportunities for increasing one’s confidence in his or her ability to perform during stress (Driskell & Johnston, 1998).
Dynamic police training is not a new concept (Olson, 1998). However, to our knowledge, no one to date has combined dynamic police training with empirically based methods to reduce psychological threat perception and improve physiological control, as we have done with the iPREP method. Advances in neurobiology and learning theory support the iPREP methodology (Cahill & Alkire, 2013; Driskell & Johnston, 1998). Namely that reducing threat perceptions while systematically increasing situational and cognitive challenges will enable an individual to capitalize on the benefits of epinephrine, for memory formation and retrieval during moderate SNS arousal, without experiencing the sensory, motor, and cognitive deficits associated with fight or flight (Cahill & Alkire, 2013; Johnson, 2008; Lovallo, 2016). Furthermore, the iPREP methodology utilizes techniques frequently implemented by elite athletes used to reduce threat and enhance knowledge acquisition and skill retention. Techniques include visualization, mental rehearsal, focused attention, and controlled respiration. Ryan and Simons (1982) found that, although mental rehearsal and visualization alone did not substitute for actual physical practice to enhance motor skills among police, these techniques help solidify the learning process in regard to situational awareness and sensory perception during police critical incidents. These techniques have been successfully applied among police officers and associated with better performance (Arnetz et al., 2009). Unique to iPREP is the addition of a mental coaching technique to enhance sensory perception. Heightened sensory perceptions, including visual, auditory, tactile, and olfactory senses, are critical components of police situational awareness. Biofeedback is used to train the officer how to rapidly attain the optimal state of sensory awareness and physiological control. Situational awareness is defined as the ability to perceive and process all potential threats in the environment. This is accomplished by using the full array of sensory input (i.e., visual, auditory, olfactory, tactile) to recognize and prioritize the order in which threats should be addressed. Situational awareness is just as important as knowledge of weapons and tactical maneuvers. It forms the basic foundational skills necessary for a police officer to keep the public and themselves safe and make the most appropriate use of force decisions.
The Current Study
A randomized controlled trial was conducted to test the iPREP methodology. A baseline skills test (i.e., pre-test) was administered, after which officers were randomized into intervention and control conditions. Following the training week, a final test (post-test) was held to determine if the intervention group displayed enhanced performance in comparison with the control group. We hypothesized the following:
Method
Of a pool of approximately 80 officers serving on the Finnish Federal Special Response Police Teams (SRTs), select officers (n = 16) were invited to participate in the study. The selected group (n = 16) was chosen because they had comparable years of service on the special unit (~2 years). The majority of officers invited agreed to participate (n = 12).
Sample Size Considerations
Despite the randomized controlled design of this study, empirical studies with few participants are at risk of “small sample failure of random assignment” (Strube, 1991). This occurs when, by chance, individuals with qualities that are confounded with outcome variables happen to be randomized to one group, thus inflating or deflating intervention effects incorrectly. While in the case of larger sample sizes, randomization is the process that solves the problem of individual differences accounting for treatment effects. As recommended by clinical researchers and statisticians specializing in intervention research with random assignment, this study applied the recommended steps to reduce the likelihood that “small sample failure of random assignment” accounts for study findings (Hsu, 1989; Strube, 1991). First, participants were matched on gender, years of service as a police officer on the SRT, prior training exposure (i.e., all received training from the same organization), and close in age. Importantly, all participants were tested on skills and abilities immediately prior to the randomization. A pre-test ensures that potential individual-difference confounds (i.e., police tactical skills and decision-making abilities) were equal across both groups. In addition to controlling for tactical skills and abilities, physical variables potentially related to SNS arousal were assessed. Specifically, body mass index (BMI) and baseline cardiovascular function were assessed and determined to be equal at baseline.
This study was approved by the University of Toronto Research Ethics Board as well as the Research Ethics Committee of the Police University College of Finland. All participants signed the ethics-approved consent form before participating.
Procedure
Two weeks before the study began, officers were mailed a consent form and demographic surveys to their home in a confidential envelope. Prior to initiating the intervention, a pre-test assessing officer skills and abilities was conducted. Following the pre-test, officers were randomized into the intervention and control groups. The intervention group accompanied the researchers to the Police University College of Finland campus for 3 days of iPREP training. The control group engaged in training-as-usual activities (e.g., shooting targets, active physical training, undercover pursuit of criminals, etc.) at their base in Helsinki, Finland. Five days following the pre-test and training, a post-test assessing officer performance during stressful scenarios was conducted on the 6th day. During all assessment and training scenarios, officers wore full police gear. All scenarios were conducted in realistic field settings (e.g., abandoned school, apartments, abandoned warehouse, etc.), using real weapons with simunition (i.e., chalk bullets that leave a colored mark, which can be used to assess shooting accuracy). In addition, trained actors, low light exposures, and loud noises were used for the purpose of enhancing the stress level and realism of the scenarios. See below for further explanation:
Pre-test
At the beginning of the pre-test, officers were fitted with chest bands which recorded their SNS arousal (i.e., heart rate, respiration, movement). Critical incident scenarios for assessing tactical skills and decision making were designed by senior training officers of the Finnish National Police. Training officers were independent of the research study and were not involved in study design or implementation to avoid bias. Trained actors (experienced police officers) conducted the scenarios so as to enhance the reality of the incidents. Officers waited together but were called independently to engage in each pre-test scenario as follows: (a) Car robbery in progress: Officer is called to the scene of a robbery. A man holding a knife was searching an empty car. As the officer approaches, the man runs behind the car, drops the knife, and then runs toward the officer, ignoring any commands to stop. (b) Potential hostage situation: Officer is called to the scene of an abandoned building with a potential hostage situation in progress. Officer enters an empty room, hears movement in a second room. In the second room, a criminal holds a gun to the head of another individual. (c) Domestic dispute: Officer is given information that loud noises are coming from an apartment, potentially a domestic dispute in progress. When the officer approaches the residence, screaming can be heard coming from the back of the apartment. Upon entry of the apartment, the officer encounters two men, one angry and yelling, the other standing stationary in the corner. Upon entering the room where the screaming is coming from, the officer encounters a man and woman struggling; the man is holding a knife. (d) School shooting in progress: Officer enters an empty hallway leading to a classroom where the hostage situation is happening. A hysterical person runs out of the classroom and passes the officer. Upon entering the classroom, the officer encounters a gunman facing them and a gunman holding two individuals hostage in classroom seats on the other side of the room.
Randomization
At the end of the pre-test day, the trainer’s scores revealed that there were no differences in tactical abilities among officers. Officers were then randomized via a coin flip into the intervention and control groups. Following a 24-hr break, officers in the intervention group began the iPREP training at the Police University College of Finland, while the control group returned to their base in Helsinki, Finland to engage in training-as-usual activities.
Training Intervention (iPREP)
Core components of the training included (a) education about the physiology of the stress response system, energy management, and fueling for peak performance; (b) group instruction on how to use mental focus and visualization to enhance sensory perception and situational awareness in performance and non-performance settings; (c) instruction and use of biofeedback to practice engaging in controlled breathing exercises that have been shown to enhance SNS control during stress (McCraty et al., 2012). Controlled breathing is not a relaxation exercise; rather, it balances the activity of the sympathetic and parasympathetic nervous system during stress, facilitating states of moderate arousal and blocking panic reactions and hyperventilation responses that lead to maladaptive sensory responses such as tunnel vision and auditory exclusion (Johnson, 2008); (d) dynamic police training during realistic critical incident scenarios. Following the principles of dynamic training, instruction begins with three to four consecutive, brief, slow-motion critical incident scenarios. An important component of this stage of training is helping the officer to recognize their SNS arousal in order to enhance situational awareness and decision making. Once an officer was aware of their physiological arousal state, they were instructed to apply the psychological and physiological control techniques during subsequent scenarios. A central benefit of dynamic training is that the use of force trainer has objective evidence to determine if the officer has indeed learned the skills based on their performance in the scenarios and does not need to rely on the officer’s self-reports. Officers are often required to make split-second UOF decisions. During fight or flight, an individual reverts to the automatic actions they have been trained to perform. The slow- motion scenarios are purposly low-stress exercises in order to provide the officer with the opportunity to aquire optimal motor movements that will be automatically performed during high stress encounters. Training continues in blocks of moderate and then high speed action, with increasing levels of stress during the scenarios. Use of force instructors provide positive feedback to the officers whenever possible to enhance their confidence and mastery of skills. Importantly, in between each use of force learning block, officers review their performance through visualizing both what happened and mentally rehearsing the optimal performance, as instructed by the use of force trainer according to the “best practices” of the organization. By the end of the use of force instructional period, officers were able to transition to an optimal mental and physiological state within seconds.
Post-test
Participants were fitted with the chest bands at the beginning of the post-test day. To avoid bias, federal SRT senior trainers, who were blinded to study conditions, prepared the post-test scenarios without consulting with the researchers. Scenarios were designed to test the officer’s situational awareness, decision making, and action skills (i.e., shoot/no shoot), as well as overall performance. Analogous to the pre-test, trained police actors carried out the two post-test scenarios to enhance the reality of the scenarios. Participants completed a brief survey before and after each critical incident, assessing their confidence in their skill to manage the critical incident and the stressfulness of the incident. To reduce the chance that officers would warn others about the upcoming scenarios, officers waited alone in isolated rooms and were called out at random to complete the post-test scenarios independently as follows: (a) Officers were informed that a potentially armed suspect was seen entering a known drug house where a loud noise was reported. Upon entering the abandoned building that had been transitioned into a drug house, officers witnessed an armed man kill another man and run into a room down a hallway. In the room where the suspect ran, five men were in various positions around the room (two men were standing in corners with their hands in their pockets, one man was sitting on a seat holding a gun pointed at the floor, and the armed suspect was holding another man hostage at knifepoint). (b) Officers were informed that a disturbance was reported from a known gang club in an old warehouse. Prior to entering the building, officers were required to perform 20 squats in full gear to stimulate physiological arousal that would normally be elevated due to the effort to arrive at the call out. The warehouse scenario consisted of four separate incidents in which the officer had to make shoot/no shoot decisions. The first was two men fist fighting at the end of a darkened hallway, the second entailed the officer opening a door to encounter a man holding a tool (wrench) facing the officer, the third was a hostage situation with one man holding a gun to another man’s head in a darkened locker room, and finally, immediately following the hostage situation, a man approached the officer from the side with a radio in his hand, asking “What happened here?”
Measures
Relevant demographic information was assessed prior to the onset of the study (i.e., age, height, weight, marital status, years as a police officer, and years as a special forces police officer).
Heart rate
The chest-band monitors (i.e., Zephyr Bioharness) were non-invasive devices fitted next to the skin of the participant under their uniform. Monitors recorded the participant’s physiological reactivity (moment by moment) in real time. In this study, two components of cardiovascular physiology were recorded: (a) Heart Rate Max (HR_Max), the highest heart rate attained during the critical incident scenario and (b) Heart-Rate Recovery Time (HR_Recovery) which indicates the time, in seconds, for the officer’s heart rate to return to their average baseline resting HR measured over the course of 5 min at the beginning of the post-test day while sitting.
Blood Pressure
Omnisense ambulatory BP wrist cuffs were used to measure the participant’s systolic and diastolic BP before and after exposure to the critical incident scenarios.
Performance ratings
The senior SRT trainers, blinded to study conditions, rated the officers on situational awareness, decision making (shoot/no shoot), and overall performance. In the drug house scenario, there were six different potential threats in the environment. Officers were rated on how many threats they recognized and managed. Overall performance in the drug house was rated on a 10-point scale, including the appropriateness of decision making and actions relevant to the threats at hand. In the warehouse scenario, there were five potential threats in the environment and four shoot/no shoot decisions to be made. Identical to the drug house scenario, officers were rated on how many threats they were aware of and managed and their decision-making skills and actions.
Self-reported stress, skills, and ability to manage the scenarios
Self-reported surveys were administered directly before and after each scenario. All questions were rated on a 10-point Likert-type scale (1 = lowest and 10 = highest score). The pre-incident survey included ratings of anticipation stress (“How stressful do you anticipate the upcoming scenario to be?”), self-confidence in decision making (“How confident do you feel that you will be able to make the appropriate decisions during the scenario?”), self-confidence in situational awareness (“How confident are you that you will be able to maintain situational awareness during the scenario?”), self-confidence in carrying out correct actions (“How confident are you that you will be able to carry out the correct actions during the scenario?”). Similarly, the post-incident self-report survey queried the stress level of the scenario (“How stressful was this scenario?”), decision making (“Were you able to make the appropriate decisions during the scenario?”), situational awareness (“Were you able to maintain situational awareness during the scenario?”), self-confidence in having carried out the correct actions (“Were you able to carry out the correct actions during the scenario?”), overall performance (“Rate your overall performance during the scenario”), ability to de-stress (“Ability to return to a non-stressed state in your body after the scenario finished?”), time to de-stress (“How long did it take you to return to a non-stressed state in your body after the scenario finished?”).
Analytic Methods
The Shapiro–Wilk test was used to assess normality of the following continuous variables: Heart Rate Max (HR_Max), Heart-Rate Recovery Time (HR_Recovery), BP (systolic and diastolic), situational awareness, trainer’s rating, participants’ subjective self-report, shoot/no shoot decision making. Independent samples t tests were used to compare mean differences between the intervention and control groups on continuous variables with a normal distribution. If the assumption of normality was not met, Mann–Whitney U tests were used to compare mean differences between the intervention and control groups (Whitney, 1997). Fisher’s Exact chi-square tests were used to examine categorical variables (participant perceived accuracy of shoot/no shoot actions). Cohen’s d (using absolute values) was calculated to examine if results comprised of meaningful differences. According to Cohen (1992), a small effect is .2, a medium effect is .5, and a large effect is .8 or above. All analyses were conducted using PASW Statistics version 20.
Results
Sample and Descriptive Statistics
All participants (n = 12) were White male police officers (M_age = 31.50; Range_age = 7). All officers had completed a similar number of years of police service prior to entering the SRT (M_police service = 4.68). All participants were within their second year of SRT service (M_SRT = 2.08; Range_SRT = 2.75; SD_SRT = 0.76). An independent samples t test did not reveal any difference in BMI between the intervention (M = 25.21, SD = 0.669) and control groups (M = 24.98, SD = 1.078), t(10) = 0.451, p = .662. Independent samples t tests did not reveal any significant differences in pre-test baseline skills, including the SRT trainer’s ratings of situational awareness, decision making (shoot/no shoot), and overall performance (Figure 1), or participant’s self-reported stress levels, confidence and perceived skills (ps > .05).

Pre- and post-training: Daily overall performance.
Similarly, no significant differences in physiology, including, HR_Max, HR_Recovery, and BP (both systolic and diastolic), were noted (ps > .05). As a manipulation check to test if the post-test scenarios were realistically stressful, changes in HR and self-reported stress levels were examined (Table 1). Paired samples t tests revealed a significant increase in heart-rate response from resting to scenario performance (ps < .05). Although self-reported stress levels did not change significantly from pre- to post-scenario, all scenarios were rated above the median on a 10-point scale, indicating moderate to high stress.
Manipulation Check: Stress Responses to the Critical Incident Simulations (N = 12, Unless Otherwise Noted).

Note. BPM = beats per minute.
Due to an equipment malfunction, HR_Max during the scenario was not measured for 10 participants instead of 12.
Mann–Whitney U tests were performed to examine differences in situational awareness and overall performance between groups. Results revealed significant differences in SRT_Trainer’s ratings of the intervention and control groups at post-test. Specifically, officers in the intervention group were significantly more situationally aware than officers in the control group (Figure 2). For Scenario 1 (drug house), officers in the intervention group noticed more of the six threats in the environment (M = 5.67, SD = 0.5164) than the control group (M = 2.5, SD = 1.0488; U = .000, p < .01), Cohen’s d = 3.83. Similarly, a Mann–Whitney U test revealed significant differences between groups for Scenario 2 (warehouse). Specifically, officers in the intervention group noticed more of the five threats in the environment (M = 4.5, SD = 0.8367) than the control group (M = 2.17, SD = 1.1691; U = 2.000, p < .000), Cohen’s d = 2.29.

Post-training scenarios: Scenario-based situational awareness.
Independent samples t tests conducted to assess overall performance revealed significant differences between groups. Specifically, for Scenario 1 (drug house), officers in the intervention group were rated as performing significantly better on a scale of 1 to 10 (M = 7.5, SD = 1.0488) than officers in the control group (M = 3.67, SD = 1.6330), t(10) = 4.838, p = .001; Cohen’s d = 2.79. Similarly, in Scenario 2 (warehouse) officers in the intervention group were rated as performing significantly better (M = 8.17, SD = 1.4720) than officers in the control group (M = 3.17, SD = 1.7224), t(10) = 5.406, p < .000; Cohen’s d = 3.12 (Figure 3).

Post-training scenarios: Scenario-based overall performance.
An independent samples t test revealed that, out of four use of force decisions embedded within Scenario 2 (warehouse), officers in the intervention group made significantly more correct shoot/no shoot decisions (M = 3.83, SD = 0.4083) compared with officers in the control group (M = 2.33, SD = 0.8165), t(10) = 4.025, p < .01; Cohen’s d = 2.32 (Figure 4).

Warehouse shoot/no shoot decisions.
At post-test, an independent samples t test revealed that there were significant differences in HR_Max and change in HR from baseline on Scenario 1 (drug house) between the intervention group and the control group (ps < .05; Table 2). Although the intervention group displayed lower HR_Max for Scenario 2 (warehouse), the differences between the intervention group and control group did not reach statistical significance (Table 2).
Comparing Physiological Arousal Between Groups at Post-Test.

An independent samples t test revealed that, although the intervention group did recover in a shorter time than the control group, the differences in HR_Recovery for both Scenario 1 (drug house) and Scenario 2 (warehouse) were not statistically significant (Table 2).
Independent t tests revealed that systolic and diastolic BP values, both before and after each critical incident scenario during the post-test, were not significantly different between groups (ps > .05; Table 2).
At post-test, independent samples t tests and Mann–Whitney U tests revealed no significant differences between groups on self-reported ratings before the scenarios on the following variables: How stressful the scenario was anticipated to be, the ability to make appropriate decisions in the upcoming scenario, and situational awareness (Table 3). All ratings were above average, with means ranging from 5.33 to 8.83 on a 10-point scale (ps > .05). However, Mann–Whitney U tests revealed significant differences between the intervention and control group’s pre-scenario ratings of their confidence to carry out the correct actions during the upcoming scenario. Specifically, in Scenario 1 (drug house) the control group reported higher levels of confidence than the intervention group (p < .05). Similarly, in Scenario 2 (warehouse) the control group reported higher levels of confidence than the intervention group (p < .05; Table 3). Independent samples t tests did not reveal any significant differences between the intervention and control group on the following self-reported questions rated after each of the scenarios at post-test: How stressful was the scenario, ability to maintain situational awareness, overall performance, and ability to return to a non-stressed physical state, and time, in minutes, to return to a non-stressed physical state. All ratings were above average with means ranging from 5.50 to 8.20 on a 10-point scale (ps > .05). Fisher’s Exact chi-square tests revealed no differences between groups in perceived ability to carry out the correct shoot/no shoot actions during both Scenario 1 (drug house) and Scenario 2 (warehouse; Table 3).
Comparing Self-Reported Stress and Performance Between Groups at Post-Test.
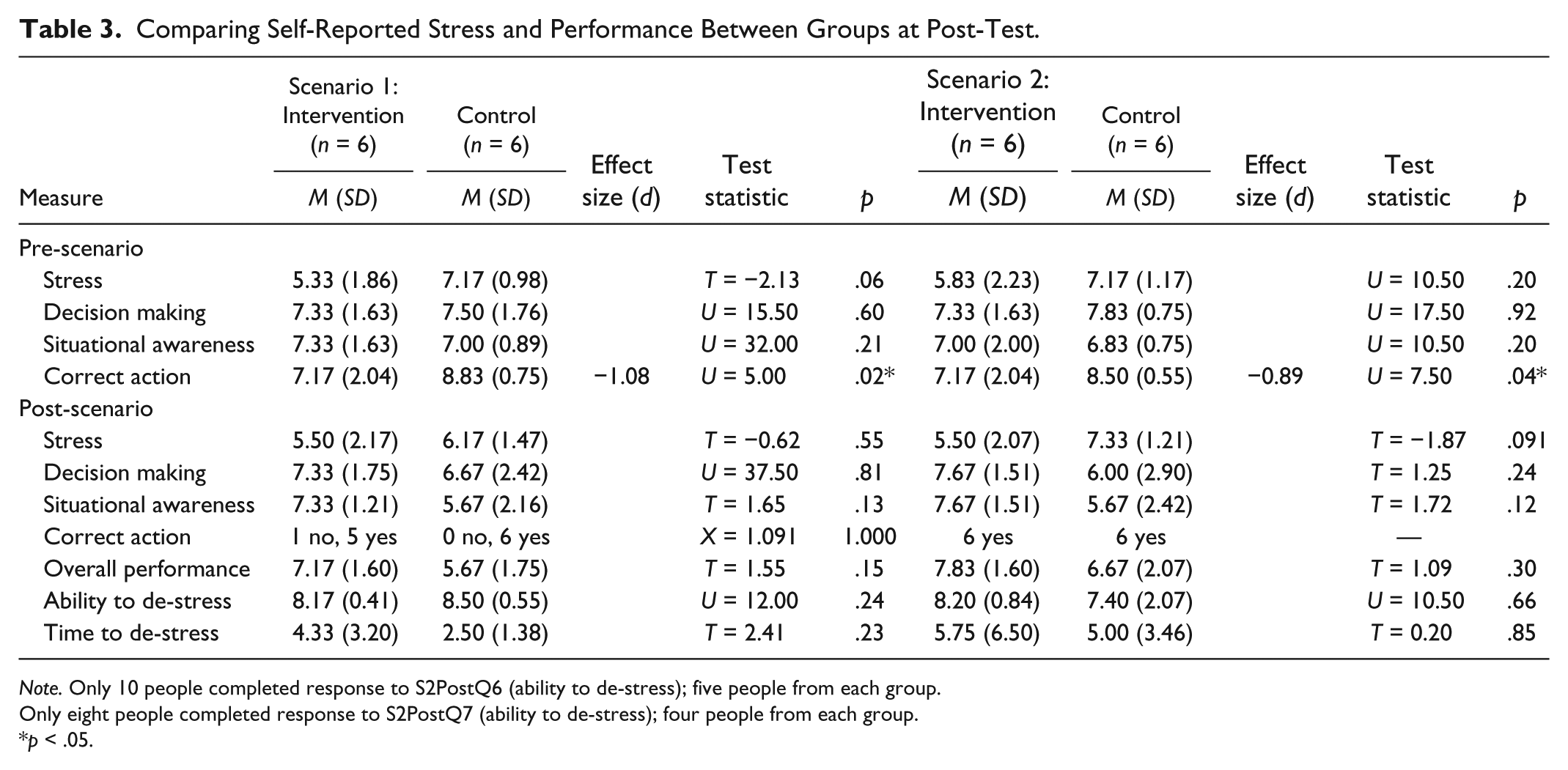
Note. Only 10 people completed response to S2PostQ6 (ability to de-stress); five people from each group.
Only eight people completed response to S2PostQ7 (ability to de-stress); four people from each group.
p < .05.
Discussion
In this experiment, we tested if a novel resilience program, integrated directly into use of force training, would improve police performance and safety during highly realistic critical incident scenarios. In support of our hypotheses, officers in the intervention group displayed significantly enhanced situational awareness, overall performance, and made a greater number of correct use of force decisions (shoot/no shoot) than officers in the control group. Specifically, officers in the intervention group saw more of the potential threats in the environment, allowing them to more accurately decide what was actually happening in the situation and perform actions in line with police “best practice” policies for use of force. Improved performance directly translates into potential lifesaving decisions for police and the civilians they are working with.
As Olson (1998) reviewed, inappropriate use of force decisions during critical incidents are frequently associated with poor situational awareness arising from extreme physiological arousal; an officer may even look in the direction of the threat but not actually see or encode what is going on or “may repeatedly pull the trigger of an empty weapon, misidentify innocuous items as weapons, or not see or hear innocent bystanders in the line of fire” (Olson, 1998). It follows then that the core component of improving use of force decision making is to improve an officer’s ability to maintain an optimal state of sensory awareness (e.g., visual, auditory, tactile, olfactory) associated with moderate arousal during critical incidents (Kalisch et al., 2015). Controlling ones’ heart rate within a moderate range is of key importance in maintaining physiological control, cognitive acuity, and the ability to perform under pressure (McCraty & Atkinson, 2012; McCraty et al., 2009). To examine if that goal was achieved by our intervention, the first step was to make sure that the testing scenarios induced significant physiological stress arousal. As demonstrated by the manipulation check (Table 1), large effects indicate that officers did experience the scenarios as highly realistic and stressful, as shown by both self-reports and a significant increase in heart rate from baseline to scenario performance. In line with our hypotheses, the data showed that the intervention group displayed lower heart rate max during the scenarios and a quicker time to recovery following the scenarios than individuals in the control group. Based on observational data gathered at specialized law enforcement trainings, Siddle (1995) provided general heart-rate ranges, in beats per minute (BPM), that indicate moderate, potentially maladaptive, and extreme arousal states, and their associated implications for situational awareness. On average, a range between 115 and 145/150 BPM indicates an optimal state of arousal and sensory awareness, after which there is a potential decline in abilities and skills. When the heart rate reaches 170 and above BPM, perceptual distortions, freezing, and possible irrational behavior can occur. An officer with a heart rate of 200 or more is at risk of freezing or complete lack of awareness. Officers in our intervention group were more likely to remain in or near the optimal heart-rate range in both scenarios compared with the control group. It is also important to note that officers in the intervention group recovered approximately 2 minutes faster following Scenario 1 and over 6 minutes faster following Scenario 2 than officers in the control group. Although this finding did not reach statistical significance, it is relevant given that officers may routinely encounter instances in which they need to face multiple threats in a short period of time, in which rapid recovery is advantageous for both safety and subsequent performance. Although we did not find significant differences in BP, this may be associated with the data collection method. Although BP was measured before and after each scenario, there was a several minute delay in placing the wrist cuff BP monitor on the officer to attain the reading, during which time BP likely returned to normal.
Ratings of officers’ self-perceptions of stress, situational awareness, and the ability to make the best decisions and perform the correct actions during the scenarios were gathered from participants both before and after each scenario. There were no significant differences between groups on any of the pre- or post-ratings, except on their rating of confidence in taking the correct action (shoot/no shoot) during the situation. The control group perceived greater confidence before the scenario in their ability to take correct actions in the upcoming event, and all participants in the control group were confident that they had completed the correct actions after the scenario had ended. This finding is of particular interest given that the self-reports of control group officers were in stark contrast with the objective ratings of performance and actions given by expert raters blind to study condition. This finding highlights an important issue—officers may be inaccurately confident in their tactical skills to correctly manage a life or death situation, and rightly so; all participants in this study were shown to have high levels of equivalent tactical skills at baseline in low stress scenarios. However, when faced with a highly threatening realistic scenario, an individual may not account for the perceptual deterioration associated with high stress arousal, which negatively affects their ability to perform tactical maneuvers. These findings highlight the benefit of advancing police tactical training by incorporating principles of psychological and physiological control during stress.
A limitation of this study is the small sample size. However, a number of factors enhance confidence in the study findings. First, our results are aligned with findings from prior randomized controlled trials in this field and extend the applicability by integrating our training into the existing use of force programming (Arnetz et al., 2009). Second, we successfully reduced the potential for small sample failure of random assignment, as discussed in the Method section (Coalition for Evidence-Based Policy, 2014; Hsu, 1989; Strube, 1991). Third, the results are based on multiple objective outcomes, including both biological data and expert raters. Of note, there were two expert raters coding participant behavior and actions from various angles to further enhance coding accuracy. Although we included self-report measures, the key study variables were measured without the risk of biases that are inherent to self-reported information, such as social desirability (Podsakoff & Organ, 1986). Fourth, key outcome variables were measured during multiple scenarios, using realistic, ecologically valid critical incident simulations. The latter method further enhances the reliability and generalizability of the data.
Implications and Applications
Enhancing resilience among officers is an increasingly popular idea among scholars and police organizations looking to support the well-being of their officers. To this end, large-scale resilience building programs originally developed for military personnel are now being applied in police organizations across North America, via classroom instruction. Programs such as the Road to Mental Readiness in Canada (Pedersen, 2013) and Comprehensive Soldier Fitness (Cornum, Matthews, & Seligman, 2011) in the United States aim to improve the health and performance of first responders through general resilience building techniques. Randomized controlled trials testing the efficacy of these programs to improve use of force outcomes are not available. It may be misleading to assume that resilience programs delivered in classroom environments will generalize to use of force and behavioral performance outcomes in the real world. Patterson, Chung, and Swan (2012) conducted a meta-analysis on exactly this topic. These authors assessed the impact of police-specific stress management interventions that aimed to improve psychological, physiological, and behavioral outcomes among police. The meta-analysis revealed overwhelmingly non-significant physiological or behavioral outcomes in the programs they reviewed (Patterson et al., 2012). Researchers have the highest confidence that a program is effective when the following standards are met: (a) the intervention must be designed to address the specific outcomes it claims to change and (b) the intervention must be tested using a randomized controlled trial, the scientific gold standard for determining program effectiveness (Patterson et al., 2012).
The iPREP intervention was developed to address identified outcomes that are known to enhance use of force decisions (e.g., situational awareness). Officers were then trained on these specific targets by directly addressing the mechanisms hypothesized to improve performance, namely psychophysiological control. Importantly, the iPREP intervention was integrated directly into realistic use of force training rather than delivered in the classroom setting. Further research is needed to determine the most efficacious manner of reducing use of force mistakes and enhancing police safety and well-being in real-world settings. However, taken together, the findings from the current study provide preliminary evidence that the iPREP intervention warrants future investigation into whether it can improve situational awareness and use of force decisions among larger, more varied samples (e.g., recruits, patrol officers) and in real-world settings.
Former assistant U.S. attorney, Kami Chavis Simmons, who now directs the criminal-justice program at Wake Forest University School of Law, is quoted in the WSJ stating, “The [use of force litigation] numbers are staggering, and they have huge consequences for taxpayers.” Professor Simmons urges politicians and police organizations to address use of force litigation from a different perspective: “Municipalities should take a hard look at the culture of police organizations and any structural reforms that might help alleviate the possibility of some of these huge civil suits” (Elinson & Frosch, 2015). We posit that many police organizations are looking for solutions to growing concerns about use of force decision making but are facing shrinking training budgets. Given these realities, organizations may benefit from investing in resilience programming, such as iPREP, which is integrated directly into the existing use of force training. Integrated training is not only cost-effective but it also enhances the ecological validity of the method and potential generalizability to real-world settings.
Footnotes
Acknowledgements
A special thank you to the following individuals: Mr. Kimmo Himberg, the director of the Police University College of Finland for the opportunity to conduct this research in collaboration with the University; and Konstantinos Papazoglou, MA, a graduate student at the University of Toronto; Marian Pitel, BSc, and Markku Nyman, MA, for their assistance with the study’s implementation. A special thank you to all the members of the Karhu Special Response Team who participated in this research study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.