
Abstract
We examined how (a) health insurance coverage, and (b) familiarity with the Patient Protection and Affordable Care Act (ACA)’s or ObamaCare mandate of cost-free access to preventive health services, affect the use of preventive services by residents of a minority community. It was based on primary data collected from a survey conducted during March to April 2012 among a sample of self-identified African American adults in Tallahassee-Leon County area of northwest Florida. The Statistical Package for the Social Sciences (SPSS) Version 22 was used for running frequency analysis on the data set and multivariable regression modeling. The results showed that of 524 respondents, 382 (73%) had health insurance while 142 (27%) lacked insurance. Majority of insured respondents, 332 (87%), used preventive health services. However, the remaining 13% of respondents did not use preventive services because they were unfamiliar with the ACA provision of free access to preventive services for insured people. Regression analysis showed a high (91.04%) probability that, among the insured, the use of preventive health services depended on the person’s age, income, and education. For uninsured residents, the lack of health insurance was the key reason for non-use of preventive health services, while among the insured, lack of knowledge about the ACA benefit of free access contributed to non-use of preventive services. Expansion of Medicaid eligibility can increase insurance coverage rates among African Americans and other minority populations. Health promotion and awareness campaigns about the law’s benefits by local and state health departments can enhance the use of preventive services.
Keywords
Introduction
The Patient Protection and Affordable Care Act (Public Law. 111-148, 124 Stat. 119), hereinafter rendered as Affordable Care Act (ACA), was signed into law by President Barack Obama in March 2010. The ACA, which is otherwise popularly known as ObamaCare, extends coverage for preventive health services without need for a co-payment, co-insurance, or deductible for persons who purchased a new health insurance policy on or after September 23, 2010 (U.S. Department of Health and Human Services, 2010). The law specifies a range of 15 covered preventive services for adults; 22 for women, including pregnant women; and 26 for children.
Preventive health services include screening and counseling services such as blood pressure, depression, cholesterol, colorectal cancer screenings, and diet counseling. The specific covered services for women include screenings for urinary tract or other infections, gestational diabetes for pregnant women as well as breast cancer mammography and cervical cancer screenings, and so on (Loosier et al., 2014). The covered services for children include behavioral assessments, developmental screening, immunizations for children from birth to age 18, lead screening for children at risk of exposure, obesity screening, counseling, and oral health risk assessment (Ghitza & Tai, 2014).
The starting point for accessing preventive health services under the law is a visit to one’s primary care physician. The use of preventive services have been proven to be beneficial in enhancing both individual and population health. Ayanian, Weissman, Chasan-Taber, and Epstein (1999) have suggested that utilization of preventive health services can increase the quality of life for people and decrease health care costs. As well, Partnership for Prevention (2007) has determined that use of preventive services can minimize hospitalization and reduce costs on the health care system.
But without health insurance, a patient cannot visit a doctor’s office to obtain preventive health services. The policy intent of the law was to expand health insurance coverage which would provide increased access to preventive health services for eligible Americans. This intent was expressed in the standards related to essential health benefits. The ACA listed preventive services as essential health benefits (Olchanski, Cohen, & Neumann, 2013).
Despite the ACA provision of free access to preventive health services, there is a huge gap in the use of those services by ethnic minorities including African Americans. It is not clear whether that gap is due to lack of health insurance or lack of knowledge about the ACA provision. Our sense, consistent with existing literature, is that African Americans appear to have been left behind in terms of access and utilization of health care, including preventive health services, compared with the majority population group (Benjamin & Lee, 2012; Robinson & Finegold, 2012). Mayberry, Mili, and Ofili (2000) found that racial and ethnic groups continued to have poorer access to quality health care services and different patterns of utilization relative to white Americans, including a lower use of preventive services, a greater likelihood of not having a usual source of care, a greater likelihood of being uninsured. (p. 109)
Several studies (Chou, Tulolo, Raver, Hsu, & Young, 2013; Fiscella, Franks, Doescher, & Saver, 2002; Gaskin & Hoffman 2000; Jacobs & Skocpol, 2012; LaVeist, 2005; Mochari-Greenberger, Liao, & Mosca, 2014; Tarver & Menachemi, 2014) have investigated racial and ethnic disparities in access to and use of health care services. Findings from some of these studies indicate that the inability to access preventive health services is due to lack of health insurance coverage. In particular, the study by Fiscella et al. (2002) examined disparities in health care use by race, ethnicity, and language among insured Hispanic, non-Hispanic White, and African American patients. They analyzed differences in the use of preventive health care services, such as physician visit, mental health visit, mammography, and influenza vaccination, and found that African Americans, for instance, were less likely than non-Hispanic White patients to receive an influenza vaccination due to lack of health insurance coverage. This finding is supported by other studies (Brown, Ojeda, Wyn, & Levan, 2000; Doubeni et al., 2010; Himmelstein et al., 2007), which demonstrated that lack of health insurance restricted access to health services, including preventive screening and diagnostic services, and treatment and management of health conditions.
In a study on racial and ethnic differences in preventable hospitalization, Gaskin and Hoffman (2000) found that African Americans and Hispanics were more likely to be hospitalized for preventable health conditions. The resort to hospitalization is due to limited access to a primary care physician. Patients without health insurance are unable to see primary care physicians to obtain preventive help before their conditions worsen. In another study, Gaskin, Dinwiddie, Chan, and McCleary (2012) found that disparities in health care utilization are related to both individuals’ racial and ethnic identity as well as the racial and ethnic composition of their communities. For this reason, efforts to improve access to health care services and eliminate health care disparities for African Americans and other minority groups should not only focus on individual-level factors but also on community-level factors such as residence (i.e., zip codes). This is because the conditions that persist in certain residential areas might limit health insurance coverage and access to health services.
The relative impacts of insurance status and race/ethnicity on disparities in health service utilization have been investigated extensively (Boss, Smith, & Ishman, 2011; Shelley, Russell, Parikh, & Fahs, 2011; Shi, Lebrun, & Tsai, 2010). Most of these studies indicate that although insurance status and race/ethnicity are each independently associated with health care service utilization, race/ethnicity had the stronger association. This finding is corroborated in Chou et al. (2013) which showed that race is more significant than insurance status in accounting for disparities in access to health services. This indicates that disparities in utilization of health services persisted in the presence of health insurance coverage. As initiatives to reduce such disparities have often focused on expanding health insurance coverage for vulnerable populations, it is not clear whether the ACA alone would have significant impact on reducing racial and ethnic disparities in utilization of preventive health services.
Different aspects of health disparities have persisted for a long time. Robinson and Finegold (2012) indicate that African Americans are less likely to receive preventive care and are more likely to have chronic diseases such as diabetes and certain cancers. In general, heart disease and stroke account for the largest proportion of disparities in life expectancy between African Americans and non-Latino Whites, despite the existence of prevention strategies (Freeman, Zonszein, Islam, Blank, & Strelnick, 2011; Tarver & Menachemi, 2014). African American women are more likely to be diagnosed with breast cancer (Rugo et al., 2013; Sturtz, Melley, Mamula, Shriver, & Ellsworth, 2014; Vadaparampil et al., 2012). All of this is due to an increase in the number of individuals without insurance, unequal access to improvements in cancer treatments, and barriers to early detection and screening among African American women. Given the promise and opportunities that the ACA holds to address these gaps, it is important to review the extent to which African Americans have taken advantage of the provisions of the Act to access and use preventive health services.
The present study is focused on the problems related to access and use of preventive health services among African Americans in the Tallahassee-Leon County area of northwest Florida. It contributes to the existing literature by examining the effects of health insurance coverage, and knowledge about free access to preventive health services under ObamaCare, on the use of preventive health services. The survey instrument measured, among others, two indicators of use of preventive health services. It asked (a) whether a respondent had health insurance coverage and (b) whether a respondent had knowledge or was familiar with ObamaCare’s provision that insured people can obtain preventive health services without co-pay or deductibles. Data were analyzed to determine the extent of insurance coverage among the target population as well as the differences in use and non-use of preventive services among the insured.
Method
Study Area and Population
Tallahassee serves the dual role of state capital of Florida and the jurisdiction of Leon County. It has three colleges and a well-educated population made up of professionals in academia, science, technology, business, arts, and so on. For this reason, the expectation is that most of the residents would have employer-based, or some other forms of, health insurance. Official county-level data (Holland, Emerick, & Howard, 2012) of the distribution of health insurance coverage by race/ethnicity and other categories (see Table 1) indicate that majority of residents have health insurance.
Health Insurance Coverage in Leon County, 2011, by Race/Ethnicity and Other Categories.

Note. GED = General Education Diploma.
Source. Florida County-Level BRFSS Survey, Florida Department of Health, Bureau of Epidemiology, cited in Holland, Emerick, and Howard (2012).
Although majority of residents are covered, there is a coverage gap of almost 16% between African Americans and Whites: the non-Hispanic White population has 93.4% coverage while the non-Hispanic Black (or African American) population has 77.6% coverage. This warrants examination of the extent of lack of insurance among African Americans and how that limits their use of preventive health services.
Based on the 2010 Census, Leon County’s total population was 275,487 of which 173,480 (63%) were White and 83,520 (about 30%) were African American. Asians, American Indians, Alaska Natives, Hispanics, and Others belonging to more than one racial/ethnic group made up the remaining 7% of the population (U.S. Census Bureau, 2010). (The 2013 estimate of Leon County population was “White”—179,396; “Black”—88,694; “Other”—10,287; “Hispanic origin”—15,694; Total—278,377. By race and ethnicity, Leon County’s population includes 64.4% White, 31.9% Black, and 3.7% Other races. Also, 5.7% of Leon County residents are of Hispanic origin; Tallahassee-Leon County Planning Department, 2014). African Americans constitute the largest minority population of the county.
Sampling Method and Data Collection
The survey area included the subdivisions of Southside, Frenchtown, and other areas in the city that have large concentrations of African Americans. Simple random sampling was the sampling method used in selecting respondents to whom the survey instruments were administered. Eight hundred ten printed surveys were administered in the designated areas during March to April 2012. The survey was developed from insights gained from the literature related to problems of health insurance coverage and the low level of access to and use of preventive health care among minority populations.
The instrument contained questions that were specifically worded to find out whether a respondent had health insurance. At least two questions in the second section of the questionnaire gauged the extent to which respondents used preventive health care, and whether a respondent’s knowledge or familiarity with ObamaCare’s provision of free access to preventive services had affected their decision to use the services. For example, the third question in Section 2, “I can’t obtain preventive services because I’m unaware of ACA free access to services,” was based on the assumption that respondents do not typically use preventive health services. The question gauged the extent to which use or non-use of preventive services might be related to the respondent’s degree of knowledge or awareness of the benefit offered by the health care reform law, namely, removal of the impediment of co-pay.
In the survey, use of preventive health services is denoted by doctor’s office visit. The underlying logic is that a patient (or respondent) must first have health insurance coverage before she or he can visit a physician’s office. Some questions in Section 1 including whether a respondent had health insurance, whether they had a doctor, and how often they visited doctors’ offices validly measured the indicator of use of preventive services. Furthermore, the rationale for considering physician office visit as an active measure or indicator of use of preventive services is that physician visit provides opportunity not only to obtain general health and wellness checkup but also a chance to ask questions regarding one’s health.
During a patient’s visit, the doctor has opportunity to order tests and referrals, prescribe medications, and even recommend hospitalization, if needed. Whether it is to obtain screening for blood pressure, diabetes, cholesterol, depression, and for early detection of cancers, or to obtain flu shots and information on treatment and management of chronic conditions, a visit to the primary care physician is the starting point for obtaining preventive health care. Without health insurance, a patient cannot visit a doctor’s office to take advantage of preventive health services. However, even with health insurance, the need to provide co-pay is often an impediment that discourages some people from visiting doctor’s offices. Therefore, familiarity with ObamaCare’s provision of cost-free access to preventive health care is expected to increase the rate of use of preventive care among this target population.
In terms of characteristics, it was a low-cost survey which had a high degree of sample-population congruence, meaning the sample subjects represented the population from which the sample was drawn. In other words, as explained below, majority of the respondents were self-identified adult African Americans who resided in the designated survey area. The instrument was in a written form and was administered face-to-face to individuals who were able to read and write their own responses on the survey. It was explained to respondents that ACA referred to the new health care legislation signed into law by President Obama, and that it also meant the same thing as ObamaCare.
As indicated above, simple random sampling was the sampling process adopted for selecting respondents. In simple random sampling, each element and combination of elements (of the population) has an equal chance of being selected into the sample frame. For this to be possible, a list of all the elements in the population must be available and a method is used that ensures that each element has an equal chance of being selected (Johnson & Reynolds, 2012). Because there is no existing list of all the elements in the target population (African Americans in Leon County in the 18-64 age bracket), an estimate was made by disaggregating the African American population in the county into age groups based on the 2013 estimate of race and ethnicity categorization of the county population. From this disaggregation, 20,620 African Americans are in the 18 to 24 age group; 32,776 are in the 25 to 54 age group; and 7,097 are in the 55 to 64 age bracket, thus amounting to a potential sampling frame of 60,493. Out of the total target population of 60,493, a sample size was selected at a significant level of 95%. The formula offered by Miller and Brewer (2003) was used to determine the sample size:

where n is the sample size (i.e., number of respondents surveyed), N is the sampling frame (the total target population, that is, African Americans in the 18-64 age bracket), and α is the error margin (0.05). The calculation for the sample size based on this formula is shown below:

Based on this formula, only 397 persons can be sampled from a target population of 60,493 people. To mitigate a low sample size, it was decided to increase the sample size to more than double the number of people that could be sampled using the Miller and Brewer formula. In this regard, it was decided to administer 810 surveys. It should be noted that this was an arbitrary number which met the expressed need of having a reasonable sample size. Survey administration entailed traveling in the defined area and politely canvasing individuals who, through oral questioning, self-identified themselves as African Americans in the 18 to 64 age range.
The survey contained open-ended as well as close-ended questions. The open-ended questions required respondents to select from a 5-point Likert-type scale response menu of options: strongly agree, agree, undecided/do not know, disagree, and strongly disagree (see Appendix A). The Statistical Package for the Social Sciences (SPSS) Version 22 was used for running the frequency analysis on the data set as well as multivariable regression modeling.
Results
Of the 810 surveys distributed, 798 were retrieved and analyzed. The distribution of respondents in terms of race showed that 524 were African Americans, representing 66% of the respondents. The other 274 respondents were Whites, Hispanics, and so on, representing 24% of the sample. Of the 524 African American respondents, 382 (73%) had health insurance while 142 (27%) had no health insurance. A majority of the uninsured respondents, 87 (61%), indicated that they use emergency rooms whenever they become ill. Of the 382 respondents who had insurance, 332 (87%) indicated that they used preventive health services, meaning they checked “disagree” and “strongly disagree” to the question: “I’m for the most part unable to visit doctor’s office for regular checkup because I don’t have health insurance.” Use of preventive health services is measured by ability to visit doctor’s office; in other words, physician visit is the proxy for “use of preventive health services.”
Because it was explained to respondents that, in the context of this study, doctor’s office visits were specifically for the purpose of asking for and receiving health and wellness screenings and counseling services, the responses they offered represented indication of actual use of preventive services and not just ability to access those services. Of the 50 insured respondents who do not use preventive health services, 30 (60%) claim they did not use preventive services because they were unaware that they could obtain those services without cost as mandated by the ACA. This result suggests that a person might have health insurance and yet not use preventive health services because they are unaware of the free access to those services under the ACA. Although this is a small fraction of the insured, it is important to target them with outreaches and educational campaigns so that they can take full advantage of the benefits of preventive health care.
In addition to the percentage distribution of the responses, there is also graphical representation of the results in the form of bar charts. The charts display the relationship between age, education, and income, and the use of preventive health care. As well, regression analysis is deployed as additional tool for analyzing these relationships. It should be noted that although other variables such as the social determinants of health, historical, and cultural issues are significant for explaining access to and use of preventive health care among minority population, this study is focused on the role of health insurance coverage and knowledge about the policy innovation of ObamaCare in explaining the potential use of preventive services among this population.
Discussion
With regard to how demographic characteristics of age, education, and income determine the use of preventive health services among African Americans, Figure 1 presents the age distribution of the insured respondents who do not use preventive health services.

Age distribution of insured respondents who do not use preventive care.
It shows that 75% of insured respondents who do not use preventive care are in the 18 to 24 years age group. Most of the respondents were neither aware of the availability of preventive services nor the ACA mandate that they could obtain the services without a co-pay. The implication of non-use of preventive health services by a large percentage of insured young people is that they would add to the pressure experienced by hospital emergency rooms. This is because they would seek urgent treatment when they become ill from an avoidable health condition, which would have been detected and prevented had they visited their doctor’s office. Informing young African Americans about availability of cost-free preventive health services and the benefits of those services can avoid illnesses which can be costly in the long term. For instance, if 19-year-old young adults get the flu vaccine in time, they are reducing the risk of getting infected with the flu virus. They could also avoid treatment which is more expensive than getting a flu shot.
With regard to the relationship between educational attainment and use of preventive health services, Figure 2 presents the educational level of insured respondents who do not use preventive services.

Educational level of insured respondents who do not use preventive services.
The bar chart shows that about 55% of insured respondents who do not use preventive services indicate their educational attainment as “some college.” It indicates that less educated respondents tend not to use preventive care as much as the more educated respondents. It suggests that there might be a link between a respondent’s level of education and their willingness and ability to seek and utilize information about preventive care. This is a subject examined in Richardson, Allen, and Xiao (2012). Disseminating information about ObamaCare preventive (or essential) health benefits to the less educated members of the African American community in the Tallahassee-Leon county area can potentially result in increased rate of utilization of preventive services.
As shown in Figure 3, about 49% of insured respondents who do not use preventive services are in the US$0 to US$15,999 income bracket.
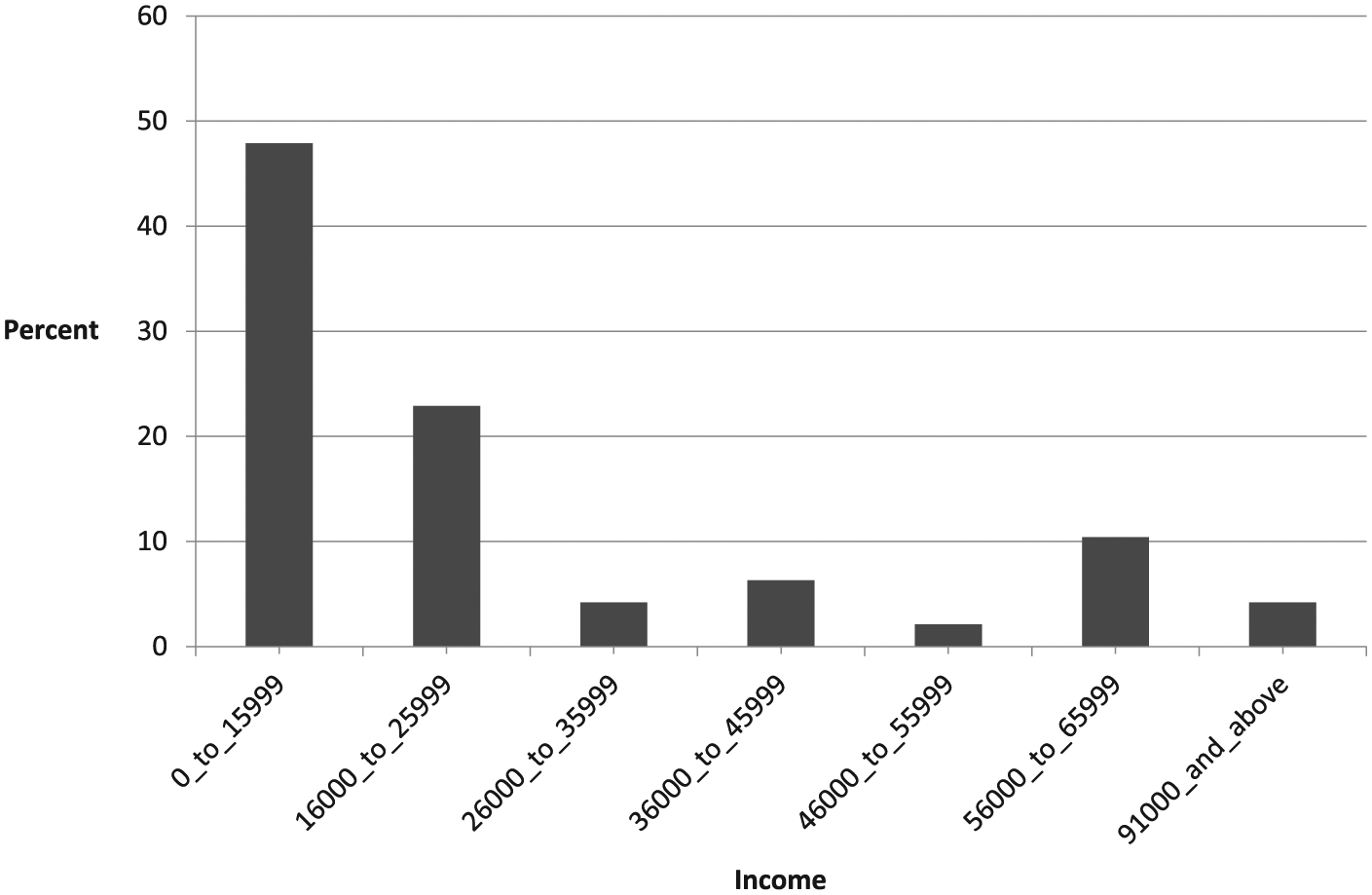
Income distribution of insured respondents who do not use preventive care.
The bar chart indicates that low-income respondents do not use preventive health services as frequently as higher income respondents, even though they are insured. This could possibly be attributed to their inability, or unwillingness, to access information and use preventive health services. There is an urgent need to inform low-income people of the availability and benefits of free access to preventive health services under the ACA.
While the survey data show that a large number of African American respondents have health insurance, a small fraction of those respondents did not use preventive health services. This indicates that lack of health insurance was not the only reason for non-use of preventive health services. An important limiting factor was lack of knowledge or awareness that preventive health services are free for the insured under the ACA. Other limiting factors were the age, education, and income of insured people. Regression analysis was deployed to further amplify the evidence in the bar charts and the accompanying discussion. For the purpose of regression analysis, “age,” “education,” and “income” are regarded as independent variables while the dependent variable is “use of preventive health services.”
Regression models are useful for understanding the relationship between a dependent variable, Y, and one or more independent variables, X1, X2, to Xn. Specifically, binary logistic regression is used here because the dependent variable “use of preventive health services” is a dichotomous variable (those with health insurance who use preventive services, and those with health insurance who do not use preventive care services). The model as shown in Appendix B predicts the effect of age, education, and income on use of preventive services. The regression analysis showed that the p value is .9104, where p is the probability of using preventive care services for the values of age, income, and education. This suggests a high probability (91.04%) that age, income, and education are determinants of the use of preventive health services among the insured: the younger, less educated insured respondents tend not to use preventive services compared with the older, more educated, and higher income respondents.
However, it is clear that there is a significant overlap among the age, education, and income variables regarding the use of preventive services. As the figures show, a large proportion of the young people in the 18 to 24 age bracket, who do not use preventive services, are also college educated, meaning that getting higher education may not translate into awareness about ObamaCare’s cost-free access to preventive services and actual use of the services. It is possible that the rate of use of preventive services among these age and education categories has not improved because young college students typically feel that they are healthy and do not care much about health insurance and preventive health care. Even with health insurance and familiarity with the ObamaCare provision, they do not care about visiting doctors’ offices to obtain preventive services because they consider such a waste of their time.
Conclusion and Recommendations
Taken together, lack of health insurance is the main reason that a significant number of uninsured respondents could not visit doctors’ offices and, therefore, could not obtain preventive health services. Although a majority of insured respondents used preventive health services, a small number did not because they were not aware of the ACA mandate that the services can be obtained without cost. Survey data also showed that the majority of uninsured respondents resorted to hospital emergency rooms to obtain both emergency and non-emergency care: 61% of respondents without health insurance used hospital emergency rooms whenever they are ill. This finding suggests that hospitals bear the burden of providing uncompensated care that not only poses financial difficulties for them but also increases health care costs for the insured. This is possible because the insured subsidize the cost of providing care for the uninsured by paying higher health insurance premiums (Pagan & Pauly, 2006).
To address the problem of uncompensated care, the ACA intended for large numbers of uninsured people to be covered so that they can visit their primary care doctors to receive preventive care instead of depending on hospital emergency rooms. The law sought to achieve expanded health insurance coverage by mandating U.S. states to expand Medicaid eligibility, which would potentially cut in half the uninsurance rates (Garfield, Damico, Stephens, & Rouhani, 2014). However, the mandate was struck down by the Supreme Court. The Supreme Court decision in National Federation of Independent Business, et al., v. Sebelius, 2012 (132 US 2566 [2012]) made the mandate optional, rather than required, meaning that states can choose whether to expand their Medicaid programs.
The fact that states have adopted different strategies in their effort to extend health insurance coverage to the uninsured indicates that uninsurance remains an urgent public policy concern. It is in this context that a consensus of scholars (Ghitza & Tai, 2014; Loosier et al., 2014) have suggested that governmental jurisdictions need to be more proactive in finding ways to provide some form of coverage for vulnerable individuals regardless of their ability to pay. But it is common knowledge that states are confronted with multiple budgetary and political constraints, which limit their capacity to provide health insurance coverage for all needy individuals.
In sum, the continuing controversies and constraints related to expanding health insurance coverage to uninsured Americans, including vulnerable minority populations, do not offer any easy or conclusive answers. However, this study shows that the ACA is a veritable policy tool that can increase health insurance coverage. With expanded health insurance coverage, a large number of uninsured people can visit primary care physicians’ offices to receive preventive health services. There is also a need for outreach to enlighten citizens on the law’s provision of free access to preventive health services so that they can utilize the services and improve their health outcomes.
Policy Implications and Recommendations
Our results have some implications for policy and future research. To address the problems associated with uninsurance, it is necessary to implement the ACA or ObamaCare in all its essence to ensure that no eligible American is denied coverage. One outcome of uninsurance is the burden of uncompensated care on hospitals which results from having to treat and care for people who otherwise would have avoided illness if they had access to and used preventive health services. In addition to expansion of Medicaid rolls in states, the ACA also provided for the establishment of state and federal insurance exchanges (or insurance marketplaces). Establishing exchanges and expanding Medicaid in more states have already resulted in increased coverage in some states as indicated in a recent study (Witters, 2014).
However, Florida has refused to expand Medicaid, and a significant number of residents remain uninsured. It is estimated that if Florida expands Medicaid eligibility, upward of 80,000 uninsured people, majority of whom are African Americans would become insured (Mitchell, 2014). The issue of Medicaid expansion is so divisive in Florida along party lines. However, there is somewhat of an acknowledgment on both sides of the aisle in the Florida Legislature that the state needs to address the problem of uninsurance as Florida is one of the states with the highest uninsurance rates. The problem is lack of agreement on the modalities to achieve the goal of expanded health insurance coverage of the poor and some in the middle class who are caught up in the coverage gap (Clemans-Cope, Kenney, Buettgens, Carroll, & Blavin, 2012; Garfield et al., 2014). It is hoped that Florida political leaders at the Cabinet and Legislature levels would resolve their political and policy differences and agree on implementation of Medicaid expansion.
Other interventions such as health promotion and educational campaigns can increase awareness within underserved communities about the availability and benefits of preventive health services. Health promotion and educational outreaches can be implemented at the community level. State and local health authorities such as the Leon County Health Department and the Florida Department of Health can consider using social media strategies. These strategies can be deployed to enlighten the African American community in the Tallahassee-Leon County area about the ACA’s provision of free access to preventive health services. Similar communities in other parts of the state can benefit from such outreaches.
Agenda for Future Research
The present study was limited to a small part of the state of Florida, and the survey data were drawn from a sample made up mostly of African American residents in the Tallahassee-Leon County area. However, the analysis can be extrapolated to explain how other African American communities in other areas that have characteristics similar to Tallahassee-Leon County might fare regarding health insurance and use of preventive health services.
Future research can target an expanded area such as a number of counties in the Big Bend or other regions in Florida. Some inter-county or inter-regional comparisons can also be done to gain a broader perspective on how the typical minority population in a given region might perform in terms of health insurance coverage and use of preventive care. This can yield different insights on the issues of lack of insurance and use of preventive health services.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.