
Abstract
Although there is no paucity of theoretical frameworks for explaining people’s health service utilization (HSU), theoretical frameworks designed to account for variations in immigrants’ HSU remain underdeveloped. Building on influential theories or models for explaining HSU and especially Andersen’s widely used health behavior model, this article proposes a theoretical framework for explaining disparities in immigrant HSU. The proposed framework explains disparities in immigrant HSU by the health care need, resources, and predisposing factors of immigrants, and macrostructural/contextual conditions at both the general and immigrant-specific levels, as well as the mediating relationships among some of these factors. It is believed that this new framework can offer a fuller understanding of the determination process of immigrant HSU.
Understanding health service utilization (HSU) is important for tailoring services to public needs. Knowledge about determinants of HSU can help disease treatment and prevention, inform health care institutions of target customers for medical contact, and prepare health care organizations for the projected growth of diverse and aging populations. As reviewed in this article, there is no paucity of theoretical frameworks for explaining people’s HSU. However, theoretical frameworks designed to account for immigrants’ HSU remain underdeveloped. There are special factors that influence the HSU of immigrants such as degree of assimilation, immigration status, context of emigration, HSU in the homeland, context of reception in the host country, transnational health access, and cultural factors pertinent to HSU (Bergmark, Barr, & Garcia, 2010; Bustamante et al., 2012; Kao, 2009; LeClere, Jensen, & Biddlecom, 1994; Portes, Kyle, & Eaton, 1992; Ransford, Carrillo, & Rivera, 2010). Albeit touched upon in various studies, many of these factors have not been theorized and incorporated into a single cohesive analytical framework for understanding immigrant HSU. Much research has evolved since the latest model proposed by Andersen (1995) in the 1990s, and therefore, there is a need to integrate new knowledge into theoretical models of immigrant HSU.
The foreign-born population in the United States was at the highest level totaling 42.2 million and accounting for 13.2% of the total U.S. population (the highest percentage since 1930) in 2014 according to the latest PEW Research Center report based on data from the American Community Surveys conducted by the Bureau of the Census (Brown & Stepler, 2015). However, immigrants are a vulnerable population at high risk of poor physical and mental health outcomes and inadequate health care (Aday, 1993; Derose, Escarce, & Lurie, 2007; Dey & Lucas, 2006). Immigrants are less likely to have a health insurance, to have a regular place of care or doctor, and to use health services than the native-born (Derose, Bahney, Lurie, & Escarce, 2009; Lucas, Barr-Anderson, & Kington, 2003; Pandey & Kagotho, 2010; Thamer, Richard, Casebeer, & Ray, 1997; Xu & Borders, 2008). Still, 21.4% (or 9 million) of the foreign-born were uninsured in contrast with 8.7% of the U.S.-born in 2014 when the Patient Protection and Affordable Care Act of 2010 (the Affordable Care Act) took full effect (Smith & Medalia, 2015, Table 5). About 76% of the foreign-born had a regular place for medical care compared with 87.7% of the U.S.-born; 29% of the foreign-born never visited a doctor’s office in the last 12 months as opposed to only 17.6% of the U.S.-born, and the percentage was somewhat lower for foreign-born Asians (26%) but much higher for foreign-born Hispanics (34.9%; Dey & Lucas, 2006, Table 2). Underutilization of health care services is directly associated with poorer health conditions, such as longer stays in hospital, more serious health problems, and heightened mortality rates (Chavez, 2012). Another important consequence of the underutilization of health care services by immigrants is a higher cost to the health care system, especially in countries where access to emergency services is free to everyone. For example, a study in Spain found that substitution of primary and secondary care by emergency room visits by immigrants led to much higher health care costs (Cots et al., 2007). In addition, underutilization of health services and health problems of immigrants may have external effects (e.g., contagious effect) on the native population. As the U.S. immigrant population continues to grow, the health outcomes of immigrants have the potential to impact the overall health status of the U.S. population and the U.S. health care system (Chou, Johnson, & Blewett, 2010). It is very important to fully grasp and direct attention to the special factors that determine immigrant HSU. Thus, the formulation of a theoretical framework especially for understanding the HSU of immigrants is in order.
The purpose of this article is to develop a theoretical framework for explaining immigrants’ HSU. In the remainder of this article, we first review existent theoretical frameworks for understanding HSU and highlight the gaps in the literature. Building on the existing frameworks and latest research, we then propose a modified theoretical framework for explaining immigrants’ HSU.
Existing Theoretical Models
Many theoretical frameworks or models have been proposed to explain the HSU of people in general. We group these models in the existing literature into two broad categories: earlier or non-Andersen models and Andersen’s health behavior model. We briefly review the earlier models because these models identify some essential determinants of HSU and lay some foundations for the emergence of the more comprehensive Andersen model. It is hoped through the review that one can see the development of a better framework as well as its limitations. We then provide a more detailed assessment of Andersen’s health behavior model because this is the most widely used model of HSU in general and for immigrants. This assessment will help reveal the strengths and limitations of the Andersen model as it relates to immigrant HSU and pave the way for the development of our modified framework for immigrant HSU.
Earlier Models
Before the Andersen model established its dominance in the 1990s, at least four categories of earlier influential models can be identified in the existing literature. Sociological models utilize the notion of sick role to explain people’s HSU. For example, Talcott Parsons’s (1951) sick role theory views illness as a dysfunction or deviance from normal function and health-seeking behavior as a way to return to normal roles. This theory is a pioneer in conceptualizing the role of sickness and health service-seeking behavior. However, it fails to explain variation in sick people’s behavior in seeking health services, among other criticisms. Edward Suchman’s (1965) model of stages of illness behavior and medical care identifies five stages in people’s decision about whether to seek health care: symptom experience, assumption of a sick role, medical care contact, dependent patient role, and recovery. This model elaborates the entire process about making decisions on HSU. Nonetheless, like Parsons’s sick role theory, it does not address resources needed to access health care services, and it ignores the role of the health care delivery system.
Socio-psychological models use psychological factors or processes to explain behavior for seeking health care. For instance, Stoeckle, Zola, and Davidson (1963) suggested three categories of psychological determinants of HSU: patients’ beliefs, attitudes, and knowledge about their symptoms; their attitudes and expectations about doctors and health services; and their understanding of illness and necessity to seek medical care. Mechanic’s (1968, 1978) help-seeking model emphasizes individuals’ perceptions of symptom severity and their response to the symptoms as crucial factors in determining their health care-seeking behavior. Although socio-psychological models offer some direct explanations for differences in HSU behavior, psychological factors alone have limited power in predicting HSU. In particular, the socio-psychological approach neglects the societal and institutional context in which health and illness behavior takes place (Gibson, 1972) and the important role of the health service delivery system (J. Anderson, 1973).
Although the sociological and socio-psychological models underscore the role of individual factors in HSU, institutional models stress the impact of health care delivery systems on HSU. Institutional models view HSU behavior primarily as an outcome of the structure of the health care system (Gibson, 1972). Variations in the supply of medical personnel and facilities, the payment system for health insurance, and distribution of health services largely determine differences in HSU behaviors. A more recent public health model proposed by Derose, Gresenz, and Ringel (2011) to understand disparities in health care access by emphasizing the role of public health can be pigeonholed into this category as well. There is certainly no denial that the health care institution and organizations are indispensable and must be incorporated into any explanation of individual differences in HSU. However, individual differences in HSU cannot be totally accounted for by structural characteristics, although the structure of the health care system no doubt plays an important role in influencing HSU behavior.
Albeit useful, the sociological, socio-psychological, and institutional models reviewed above mostly rely on a particular set of predictors to explain disparities in HSU. Nevertheless, health belief model proposed by Irwin Rosenstock and his associates in the 1950s and 1960s (Rosenstock, 1966; Rosenstock, Derryberry, & Carriger, 1959) represents an approach to developing a more comprehensive model that takes into account multifarious determinants of HSU. Rosenstock (1966) suggested four groups of interrelated factors that explain preventative health services: (a) perceived susceptibility to disease, (b) perceived severity of illness, (c) perceived benefits of taking action, and (d) perceived barriers to take action. In addition, cues to action must be present to prompt health-seeking action. This initial health belief model captures some essential psychological determinants of preventive care utilization, but it was limited to predicting preventive HSU and ignored socioeconomic, demographic, and structural factors. In response to critique, in the 1970s Rosenstock (1974) added demographic (e.g., sex, age, race/ethnicity, education), socio-psychological (e.g., personality, social class, and peer pressure), and structural (e.g., knowledge of a disease and previous contact with a disease) factors as exogenous factors. Nevertheless, he acknowledges no direct effect of these foregoing factors on health care use. In the 1980s, Rosenstock and his associates further expanded the health belief model to the domain of treatment of health problem (Rosenstock, Strecher, & Becker, 1988). With the modifications over time, the health belief model boosts its predictive power and popularity. Nevertheless, inattention to the role of the health care institution and policy remains a major drawback of this model.
Andersen’s Health Behavior Model
The Andersen health behavior model (Andersen, 1968, 1995) is the most common framework used in the study of health service access and utilization (Akresh, 2009; Cabassa, Zayas, & Hansen, 2006; Derose et al., 2011). The Andersen model was first proposed in 1968 and has undergone several phases of revision over time. In his initial formulation, Andersen (1968) explained people’s HSU by three clusters of factors: (a) predisposition to use health service, including demographics, social structure, and health beliefs; (b) enabling factors, including personal or family resources (e.g., income, health insurance, and regular source of care) and community resources (e.g., availability of health personnel and facilities); and (c) need for care, including perceived needs and clinically evaluated needs. Andersen treats the relationships among these three clusters of factors as a sequential order. Although these factors are highly pertinent to HSU, this model has several limitations. First, mediating relationships may not occur in a systematic fashion, albeit existent between certain variables of the above three clusters of factors. Not every variable has an indirect relationship with other variables. For instance, health beliefs (part of the predisposing factors) may not necessarily affect personal or family resources (part of the enabling factors), and need for health care may not depend on enabling factors and social structure. Second, certain enabling resources (e.g., community resources) are necessary but not sufficient conditions for HSU (Andersen, 1995). Third, because larger social structural factors beyond individual control are part of social structure, they should be singled out rather than treated as part of individual predisposition. Finally, there are also other determinants of HSU that have not been incorporated.
In the 1970s, Andersen’s Phase 2 model was developed with contributions of his collaborators (Aday & Andersen, 1974; Andersen, Kravits, & Anderson, 1975; Andersen & Newman, 1973; Andersen, Smedby, & Anderson, 1970) at the Center for Health Administration Studies, the University of Chicago. This revised model juxtaposes the three categories of determinants in the initial model and adds a new category of determinants called health care system, which comprises health policy, resources, and organization. In addition, the model specifies the type, site, purpose, and time interval of HSU, which can impact health care use. It also adds consumer satisfaction as the outcome of HSU. This addition turns HSU into a mediating variable and makes this model more complicated.
Andersen’s Phase 3 model revised in the 1980s and 1990s adds another category of HSU determinants—external environment, which includes physical, political, and economic factors (see Andersen, 1995). It broadens the concept of HSU to “health behavior,” which contains HSU and “personal health practices” such as diet, exercise, and self-care. Although this model seems to apply to broader outcomes, the determinants of HSU may be quite different from those of personal health practices. For example, the health care system such as health care policy and availability of health personnel and facilities may have little bearing on diet, exercise, and self-care. The broader the outcome variable, the less precise the predictors will be. Furthermore, this model reverses the causal relationship between HSU and need factors measured by perceived and evaluated health status in the initial model.
Finally, Andersen’s (1995) Phase 4 model is a more complex path model that predicts health status and consumer satisfaction as the ultimate endogenous variables rather than HSU. This model reflects all the strengths and weaknesses of the models in the previous three phases. It includes more outcome variables in the model. It treats the health care system and external environment as exogenous variables separated from population characteristics in the Phase 2 and Phase 3 models. It returns the three categories of population characteristics to sequential causal order in the initial model. It includes the broader health behavior concept rather than just HSU. It treats health behavior (including HSU) as an intervening variable rather than an outcome variable. It includes feedback effects from health outcome and health behavior to population characteristics and health behavior. For the purpose of predicting HSU, this more complex model may be less precise than the previous models. Overall, Andersen’s initial model with the addition of some predictors in his later models (e.g., health care system, environmental factors) may be most effective in predicting HSU.
Andersen’s health behavior model has been extended to some vulnerable populations, such as the elderly (Evashwick, Rowe, Diehr, & Branch, 1984), homeless people (Gelberg, Andersen, & Leake, 2000; Stein, Andersen, & Gelberg, 2007), African American women (Copeland & Butler, 2007), rural residents (Slifkin, 2002), and immigrants (e.g., Akresh, 2009; Bustamante et al., 2012; J. Y. Choi, 2009; Kao, 2009; LeClere et al., 1994). However, studies that apply the Andersen model to immigrants are most often limited to a simple application of his Phase 1 model with little or no modification of the framework (e.g., Akresh, 2009; S. Choi, 2006; S. Lee, Choi, & Jung, 2014). A few of them (Bustamante et al., 2012; Kao, 2009; LeClere et al., 1994) add or use a few predictors germane to immigrants such as duration of residence, host language proficiency, generational status, age at immigration, and legal status but fall short of proposing a theoretical framework especially for accounting for immigrant HSU. Portes et al. (1992) and J. Y. Choi (2009) recognized the importance of some contextual factors but did not systematically theorize and mold them into a comprehensive and cohesive framework. To gain a better understanding of immigrant HSU, to guide empirical analysis of immigrant HSU, and to provide better health services for immigrants, developing a comprehensive theoretical framework for explaining immigrant HSU is a desideratum to which we now turn.
A Conceptual Framework for Understanding Immigrant HSU
To explain disparities in immigrant HSU, we propose a modified theoretical framework that retains the useful ideas of Andersen’s health behavioral model and other models but takes into account factors especially pertinent to immigrants. Our main ideas are presented in Figure 1. We believe that Andersen’s ideas of need, enabling, and predisposing factors are cogent but need to be specified for immigrants. We also believe that macrostructural or contextual factors should be emphasized and singled out. Furthermore, the direct and indirect effects of need, enabling, predisposing, and macrostructural/contextual factors on HSU should be elucidated. We argue that disparities in the HSU of immigrants can be explained by the health care needs, resources, and predisposing factors of immigrants, and macrostructural/contextual conditions as well as the mediating relationships among some of these factors at both the general and immigrant-specific levels. It is important to note that unlike Andersen’s Phase 3 and Phase 4 models and Gelberg et al.’s (2000) model that cover personal health practices and health behaviors in general, our outcome variable is limited to the use of health services provided by health professionals and does not include “personal health practices” and other care. In the balance of this section, we elaborate these determinants and specify mechanisms through which these factors influence immigrant HSU.
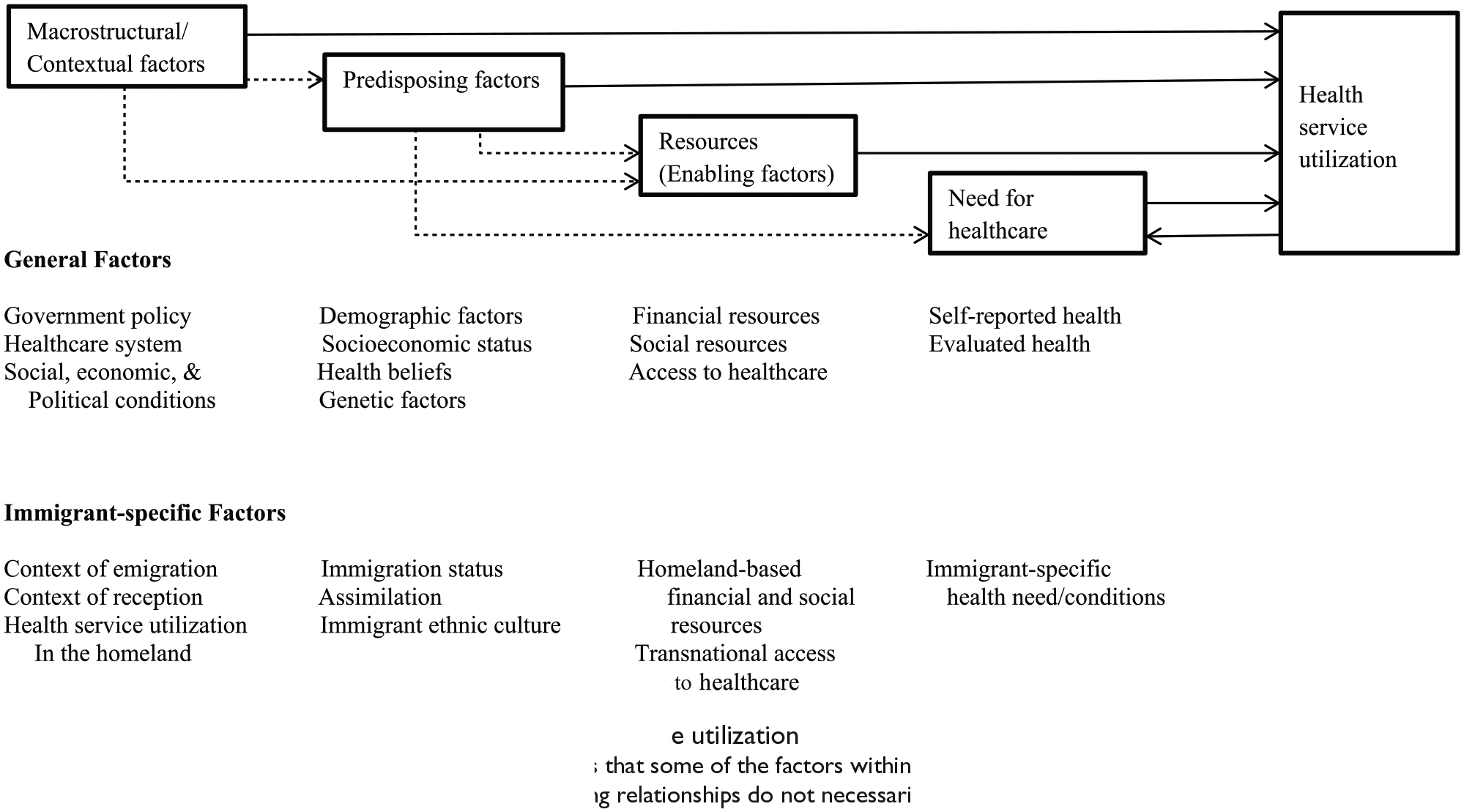
An analytical framework for immigrant health service utilization
Need for Health Care
The concept of need for health care is self-explanatory. Without doubt, HSU depends most directly on needs for such services or health conditions. For immigrants, the need factors may be divided into general needs and immigrant-specific needs.
General needs
Obviously, a healthy immigrant has much less need than a sick one to see a health professional for services other than regular physical checkup and preventive care (Morris, Sutton, & Gravelle, 2005). The need factors are clearly identified by Andersen (1968, 1995) and are measured by health status. In agreement with Andersen, we believe that health conditions have two dimensions: self-rated health status and professionally evaluated health status. Self-rated health condition has been recognized as a valid indicator of health (Y. Lee, 2000). In general, self-rated health reflects the self-assessment of an individual’s own health in terms of feelings, symptoms, and informal evaluation and is a consistent and strong predictor for health care-seeking activities, medication use, and HSU (Giltay, Vollaard, & Kromhout, 2012; Y. Lee, 2000; Mellner & Lundberg, 2003). Professionally evaluated health can verify or invalidate self-assessment of health status, but it is limited to registered patients and may not well predict HSU for patients with chronic diseases. Self-reported health and professionally evaluated health may not always be in concordance and may vary in predictive values (see, for example, DeSalvo & Muntner, 2011; Giltay et al., 2012; Mellner & Lundberg, 2003). In reality, data on self-rated health can be obtained easily and are often available in most health surveys; however, data on professionally evaluated health are much more difficult to come by. Nonetheless, whenever possible, data on professionally evaluated health should be used in conjunction with self-rated health. We expect that a better health status is inversely associated with the use of health services. That is, immigrants who have a better health status, either self-assessed or professionally evaluated, are less likely to use health services than those who have a worse health status, simply because they have a lower level of need to. Several available studies attest to this relationship (e.g., Afilalo et al., 2004; Blackwell, Martinez, Gentleman, Sanmartin, & Berthelot, 2009; Broyles, McAuley, & Baird-Holmes, 1999; Dhingra, Zack, Strine, Pearson, & Balluz, 2010). Need for health care has been found to be the strongest predictor of HSU (see, for example, de Boer, Wijker, & de Haes, 1997; Hernández-Quevedo & Jiménez-Rubio, 2009).
It is also important to note that although need for health care is universal regardless of ethnicity, gender, age, and socioeconomic status (SES), need in the form of self-reported or professionally evaluated health status may be expressed and perceived differently across gender and ethnic lines. Women are more likely to self-report poorer health conditions, and therefore, have greater need for services than men because they are more likely than men to express pain and distress and to factor in less serious ailments in their reports (e.g., Khazan, 2012; Shin, Shin, & Rhee, 2012). As a result of social learning, men learn to tolerate pain and discomfort whereas for women expressing pain and distress is considered normal. Ethnic variations in reaction to pain are often observed, despite no significant ethnic differences in physiological pain threshold (Lipton & Marbach, 1984). For example, Jews and Italians tended to have emotional responses to pain whereas the Irish tended to show denial of pain (Zborowski, 1952; Zola, 1966); African Americans are more likely than non-Hispanic Whites to report pain and suffering and have greater needs for health services (Campbell & Edwards, 2012; Green et al., 2003).
Immigrant-specific needs
Immigrants have some special needs for certain types of health problems because of disease prevalence and health environment in the country of origin. For example, tuberculosis rate is much higher among immigrants than among the native-born population (e.g., in 2010, 18.1% for the foreign-born vs. 1.8% for the U.S.-born, especially among foreign-born Asians and Pacific Islanders, 33.2%, and foreign-born Blacks, 26.2%; Centers for Disease Control and Prevention [CDC], 2013). Asthma rate is also higher among the foreign-born than among the U.S.-born (CDC, 2013). Asian immigrants are more susceptible to such health problems as hepatitis, parasitoses, and liver and lung cancers due to the prevalence of these diseases in the homelands (Chen & Hawks, 1995; Dhooper, 2003; Flaskerud & Kim, 1999). Foreign-born children have a lower rate of immunization, especially against haemophilus influenzae type b and hepatitis B than U.S.-born children (Strine et al., 2002). Their immunization record is less likely to be up to date compared with that of U.S.-born children (Kandula, 2008). These special health care needs vary across immigrant groups. The greater the special needs, the greater the HSU.
In addition, immigrants differ from natives in need for health care over time. Immigrants are typically healthier than natives at the time of immigration because of the selection of healthier persons for migration known as the “healthy migrant effect” (Antecol & Bedard, 2006; McDonald & Kennedy, 2004, 2005). However, the longer they stay in the host country, the more likely their health condition resembles native-born individuals as found in the United States and abroad (e.g., Antecol & Bedard, 2006; Hernández-Quevedo & Jiménez-Rubio, 2009; McDonald & Kennedy, 2004, 2005; Stephen, Foote, Hendershot, & Schoenborn, 1994). Thus, over time, immigrants’ need for care is likely to increase, so is their HSU.
If we take the time dimension into account, we can expect a reciprocal relationship between need for health care and HSU as shown in Figure 1. A poorer heath condition, either self-rated or professionally evaluated and either general or immigrant specific, will increase the rate of HSU. As a result of professional health services, health status or condition will improve or the need for health care will decrease. Testing such a relationship will require longitudinal data and such statistical technique as structural equation modeling.
Resources
In the context of HSU, resources refer to the means that enable individuals to receive, and/or access to, health services. We group resources into three types: financial resources, social resources, and access to health care. Financial resources are monetary means for obtaining health services. Social resources are relationships through kin, friendship, and communities that grant or increase one’s access to health services. Social resources can be conceptualized as social capital that enables access to health care. Access to health services means that there must be availability of health professionals and facilities in the community to provide needed services; it also means that individuals can choose a regular doctor or facility for medical care. There are also general resources and immigrant-specific resources.
General resources
Immigrants must have financial resources to receive health care. Income and ability to purchase health insurance are common measures of financial resources. Health insurance has been found to be a consistent predictor of immigrant HSU, whereas the effect of income is mixed (see, for example, Akresh, 2009; Bustamante et al., 2012; LeClere et al., 1994; Wells, Golding, Hough, Burman, & Karno, 1989). In particular, low income appears to be a barrier to the use of secondary care (Morris et al., 2005).
The important role of social resources or social capital in HSU has increasingly been recognized (see J. Y. Choi, 2009; Macintyre, Ellaway, & Cummins, 2002; Pescosolido, Gardner, & Lubell, 1998; Veenstra et al., 2005). Social networks or relationships through family members, relatives, friends, and peers can help diffuse health information, encourage the adoption of health behavioral norms, and control deviant health-related behaviors (Kawachi & Berkman, 2000; Nandi et al., 2008). Social networks can also connect immigrants with right health service personnel and facilities and increase their access to health care services. In particular, the family plays a crucial role in how and when individuals seek health services (Doherty & Campbell, 1988; LeClere et al., 1994; Litman & Venters, 1979). Family/kinship networks have protective effects for recent immigrants in access to health services. Note that the effect of social networks on immigrants’ HSU may not always be positive (J. Y. Choi, 2009; Chung & Lin, 1994). The networks may encourage cultural alternatives to formal health care and may have limited health care information. Pescosolido et al. (1998) reported that in the case of mental health services among Puerto Ricans, small social networks increased the probability of service, but large social networks may buffer or delay such services during the time of medical needs. It is also worth mentioning that the measurement of social capital in the literature of HSU and health studies in general is less than perfect (see, for example, McDonald & Kennedy, 2005), and remains a task for improvement in the future.
Resources also include access to health services. Evidence suggests that having access to doctors and medical facilities is associated with a higher rate of HSU (e.g., Lebrun & Dubay, 2010; Ye, Mack, Fry-Johnson, & Parker, 2012). The availability of trained interpreters is also part of resources critical for immigrant HSU (Barone, 2010; Hauck, Corr, Lewis, & Oliver, 2012). It is important to note that access to health services for immigrants varies by type of care such as primary, secondary, and tertiary care. For instance, in Spain, immigrants tend to lack access to secondary care but have a higher probability of hospital emergency service than Spaniards (Hernández-Quevedo & Jiménez-Rubio, 2009). Immigrants’ heavy reliance on emergency services has been reported in Denmark (Nielsen, Hempler, Waldorff, Kreiner, & Krasnik, 2012) and in the United States, especially among undocumented Latino immigrants (Chan, Krishel, Bramwell, & Clark, 1996; Coffman, Shobe, Dmochowski, & Fox, 2007).
Immigrant-specific resources
Unlike natives whose resources are normally constrained within their country, some wealthy immigrants bring in financial resources from their country of origin to the host country (Yan, 2014). The foreign source of money can increase their chance of HSU. The effect of financial resources on HSU is generally greater for immigrants than for the natives because immigrants, especially new immigrants, tend to land in unskilled and low-paying jobs (e.g., Aguilera & Massey, 2003; Piore, 1979). Differing from the natives’, immigrants’ social resources often go beyond the host country. Quite a few immigrants use their social connections such as kin and friends in the home country to get free or cheaper medicine and/or cheaper and better health services in the homeland, which reduce their HSU in the host country (Bergmark et al., 2010). Their access to health services is more transnational and flexible; they can choose between the home country and the host country for services, contingent upon the price and quality of health services (Bergmark et al., 2010). They can also use traditional medicine. Under some circumstances, immigrants may decide to stay in the home country for an extended period of time to treat certain types of diseases such as cancer (Feet in 2 Worlds, 2009).
Predisposing Factors
In the context of HSU, predisposing factors may be defined as conditions that indicate a propensity for HSU. In this category, we include only individual-level variables pertinent to the predisposition or propensity for HSU. Macro conditions such as the health care system and external environment will be treated separately later. Predisposing factors can be general and immigrant specific.
General predisposing factors
General predisposing factors include, but are not limited to, demographic factors, socioeconomic factors, health beliefs, and genetic factors. Demographic factors typically include gender, age, race or ethnicity, and marital status (Andersen, 1968, 1995). Women may be more likely to seek medical care partly because of their need and partly because of socialization. Empirical evidence suggests that women have a greater likelihood of HSU than men (Broyles et al., 1999; Dhingra et al., 2010; Hulka & Wheat, 1985). All else being equal, older people are more likely to seek medical care than younger ones because of their biological needs as a result of aging (Andersen, 1968, 1995; Graham, 1957). There are racial and ethnic differences in HSU partly because of genetic predisposition and partly because of culture (Broyles et al., 1999; Dhingra et al., 2010). Currently married people tend to be healthier and less likely to need medical care than their non-married counterparts, but married people may be more likely to seek preventive care than the unmarried (Hammond, Matthews, & Corbie-Smith, 2010; Peifer, Hu, & Vega, 2000).
SES certainly has an impact on individual propensity for HSU. Education is an indicator of social status. People with a higher level of education may be more likely to seek health service (Hernández-Quevedo & Jiménez-Rubio, 2009), especially preventive health services, than those with a lower level of education because their knowledge of health and their resources enable them to treat health problems in a timely fashion and to prevent health problems from happening. Available evidence appears to generally coincide with this positive association between education and HSU (see Alegría et al., 1991; Blackwell et al., 2009; Parslow, Christensen, & Jacomb, 2002; Szwarcwald, Souza-Junior, & Damacena, 2010). In the same vein, people with a higher occupational status may be more likely to seek medical care than those with a lower occupational status for similar reasons (Alegría et al., 1991).
Health beliefs such as attitudes, knowledge, and values concerning health and health services may affect how people perceive the need to seek health care and their HSU behavior (Andersen, 1995; Rosenstock, 1966). In general, the greater the perceived susceptibility to disease, the higher the likelihood of HSU; the greater the perceived severity of illness, the higher the likelihood of HSU; the greater the perceived benefits of taking action, the higher the likelihood of HSU; and, the greater the perceived barriers of taking action, the lower the likelihood of HSU.
With the recent advancements in genome research and mapping and gene therapy, genetic factors have increasingly been recognized as factors contributing to some diseases, which can influence the need for health services and HSU (Health & Martin, 1993; True et al., 1997). Individuals who have a significantly higher probability of contracting certain diseases may be informed and urged to take preventative action for self-protection. If genetic data become available, they should be included in the category of predisposing factors.
Immigrant-specific predisposing factors
Because immigrants are a special population and a vulnerable population, certain special predisposing conditions also operate to impact their HSU. These conditions comprise at least immigration status, assimilation, and immigrant ethnic culture. This section specifies each of these conditions.
Immigration status
Immigration status is associated with rights, benefits, resources, psychological status, and therefore, HSU. Legal status is probably the most important status that affects the likelihood of immigrant HSU. An undocumented immigrant status itself is a critical barrier to health care services (Chavez, 2012). The status of undocumented immigrants can preclude or decrease their incorporation to the host society and can deter them from using health services. Undocumented immigrants are less likely than legal immigrants to seek medical care because of the fear of deportation, shame, language barriers, and expensive medical bills (Berk & Schur, 2001; Bustamante et al., 2012; Raymond-Flesch, Siemons, Pourat, Jacobs, & Brindis, 2014; Schoevers, Loeffen, Muijsenbergh, & Largro-Janssen, 2010). Undocumented immigrants are treated differently across countries. For instance, according to the Affordable Care Act, undocumented immigrants in the United States do not have access to primary and preventive care and are ineligible for Medicare, nonemergency Medicaid, and Children’s Health Insurance Program but remain eligible for emergency care and emergency Medicaid if low on income. In Spain, immigrants, regardless of legal status, are entitled to health care services as Spaniards as long as they register in the local population census; non-registered immigrants are covered only by emergency services (Hernández-Quevedo & Jiménez-Rubio, 2009). In France, illegal immigrants are allowed to receive care in emergency room with extremely serious diseases and can stay for the follow-up exam (Duguet & Beviere, 2011). In the Netherlands, illegal immigrants do not have right to get health insurance, but are able to receive only medically necessary care (Schoevers et al., 2010). A report by Médecins du Monde European (2009) revealed that access and rights to health care of undocumented immigrants varied across 11 European countries but were overall very restrictive. Furthermore, although in theory, undocumented immigrants in many of these European countries may have rights to health coverage, in reality only a small to moderate percentage of them have effective health coverage. In Israel, undocumented immigrants also do not have access to primary and preventive care (Filc, 2010). These differences notwithstanding, undocumented immigrants are universally vulnerable for insufficient HSU.
There is also a new versus old immigrant divide. Under the Personal Responsibility and Work Opportunity Reconciliatory Act (PRWORA) of 1996, newer legal immigrants are less likely to use health services than earlier legal immigrants because they are no longer eligible for publicly funded services such as Medicaid for the first 5 years of residency. New immigrants need time and resources to adapt to the host country. They often experience hardships and barriers in HSU, such as lack of financial resources, limited English proficiency, unfamiliarity with the host health care system, distrust in Western medical care, and experience of disrespect or discrimination. These hardships and barriers reduce their chance to seek health care services (e.g., Jang, Kim, & Chiriboga, 2005; Ku & Matani, 2001; Lai & Surood, 2010; Lebrun, 2012).
Assimilation
Compared with the native-born, a significantly higher proportion of immigrants have no health insurance, have no regular place of care, and do not seek professional medical care (Derose et al., 2009; Dey & Lucas, 2006; Frisbie, Cho, & Hummer, 2001; Ku & Matani, 2001). Even if they do seek medical care, the likelihood of using secondary care is much lower than that for the native-born (McDonald & Kennedy, 2005). Unlike the native-born, immigrants have to adapt to the culture and society of the host country. For new immigrants in the United States, they are introduced to a health care system that can be quite different from that in their home country (Bustamante et al., 2012). How well immigrants adapt to host culture and social systems including the health care system has an important impact on their HSU. The degree of their adaptation partly accounts for variations in their HSU.
There are different types of adaptation. One is cultural assimilation or acculturation, which is defined as change of cultural patterns to those of the host society (Gordon, 1964). Acculturation to host culture may increase HSU because an increase in acceptance of host norms and values (including those for HSU) can lead to health-seeking behaviors similar to those of the native-born. Evidence of positive effects of acculturation on HSU is abundant (e.g., Cabassa et al., 2006; Fassaert, Hesselink, & Verhoeff, 2009; Lara, Gamboa, Kahramanian, Morales, & Bautista, 2005; Wells et al., 1989). Acculturation is often measured by English proficiency and length of host residency. A higher level of English proficiency and a longer host residency are indicative of a higher degree of assimilation to the host culture. A higher level of English proficiency enables immigrants to have better access to the health care system (Akresh, 2009; Lara et al., 2005; Lebrun, 2012; LeClere et al., 1994; Solis, Marks, Garcia, & Shelton, 1990). A longer host residency significantly increases the likelihood of immigrant HSU (Lebrun, 2012; LeClere et al., 1994). Another type of adaptation is structural assimilation or assimilation to groups and institutions of the host (Gordon, 1964), which can be measured by residential integration and joining of host organizations or institutions, but measurements of structural assimilation are often lacking. Still another type is identificational assimilation or change in the sense of peoplehood (Gordon, 1964). Acquisition of host citizenship can be a good indicator of it (Kao, 2009). It can be hypothesized that the higher the degree of assimilation, the higher the likelihood of HSU, all else being equal.
Immigrant ethnic culture
Culture is the way of life. Immigrant ethnic culture refers to norms, values, beliefs, traditions, behaviors, and other cultural patterns brought by immigrants from the homeland to the host society. Immigrant ethnic culture influences HSU because certain immigrant groups’ beliefs about health and illness and their treatments of diseases may be quite different from those of the host society. For example, many Latino immigrants see illness as God’s will or divine penalty caused by prior or current sinful behaviors. Instead of seeking professional health services, some Latino immigrants use folk healers such as curanderos and naturalistas for treating some illnesses (León, 2002; Menjívar, 2002; Padilla & Villalobos, 2007; Ransford et al., 2010). The curandero typically utilizes prayer, religious counseling, and limpias (spiritual cleaning ceremonies) in combination with herbal medications. As part of the alternative healing system, some Latino immigrants also employ personal prayer and faith as a coping mechanism for distress and traumatic adjustments to the host country (Ransford et al., 2010). These “cultural alternatives” fall under the rubric of complementary and alternative medicine and are considered affordable and well-revered elements of culture (DeStefano, 2001; Gómez-Beloz & Chávez, 2001; Pagán & Pauly, 2005). Significant proportions of Latino immigrants also report using alternative medicine such as herbs, dietary supplements, massage, chiropractic, and other home remedies to treat many health problems. These practices are especially common as a first treatment, for minor illnesses, and among recent arrivals and immigrants with limited financial resources, English proficiency, or access to health care (Garcés, Scarinci, & Harrison, 2006; Mikhail, Wali, & Ziment, 2004; Ransford et al., 2010). Mikhail et al. (2004) found that about 80% of the participants did not inform their doctors about their use of alternative medicine.
Asian immigrant groups also have their own health beliefs, health behaviors, and illness treatments. For example, Chinese immigrants tend to believe that illness results from the imbalance of yin and yang, the two opposite yet complementary forces, in the body; health will return as a result of harmony between yin and yang. Korean and Vietnamese immigrants also have similar kinds of health beliefs. Asian Indian immigrants also view illness as an outcome of body imbalance, and some believe that illness stems from past actions or actions in past lives.
Many Asian immigrants use ethnic-specific traditional medicine to treat health problems. They believe that the traditional medicine can remove the cause of illness rather than just the symptoms. Recent research has demonstrated that many Chinese immigrants use traditional Chinese medicine (TCM) including herbs, acupuncture, massage (tuina), therapeutic exercise (qigong), diet, and other forms of healing on a regular basis (Ahn et al., 2006; Wu, Burke, & LeBaron, 2007). For example, Wu et al. (2007) reported that almost all Chinese immigrant patients used some forms of TCM in the previous year, that the majority did not share information about the usage with their physicians, and that they tended to use TCM for chronic diseases but used Western medicine for infectious diseases and surgeries. The use of traditional medicine is also observed among other Asian immigrant groups such as Koreans, Vietnamese, and Asian Indians (e.g., Ahn et al., 2006; Hsiao et al., 2006; Kim, Han, Kim, & Duong, 2002; Mehta & McCarthy, 2008; Satow, Kumar, Burke, & Inciardi, 2008).
Trust in doctors is another issue of concern for immigrants in HSU. Immigrants from different countries may have different degrees of trust in health care providers because of their experiences with doctors prior to emigration, their different degrees of familiarity with host culture, and their varying levels of English competence, and therefore, communication skills. The level of immigrant trust in health care providers in the host country can affect their propensity and behaviors to use health services. For example, a study by Ransford et al. (2010) found that some Latino immigrants crossed the border to Mexico to seek health care because they considered Mexican doctors better as the doctors spent more time with them, provided more detailed explanations, and used a generally more holistic approach in addition to easier access, cost savings, and higher doses for medications. Mistrust of doctors and avoidance of medical care were also reported by Latino immigrants who were concerned that doctors were only motivated by money and lacked an understanding and sensitivity about their immigration status (Raymond-Flesch et al., 2014; Rhodes et al., 2015). Distrust of health information and alienation from the health system due to experience in the former Soviet Union and lack of communication between doctors and patients in the United States were also underlying reasons why some Russian immigrants did not seek out health information and services (Benisovich & King, 2001). Russian immigrants tend to have degrees of distrust of U.S. health care as they were used to an authoritarian relationship with health practitioners and may see free exchange of information and open discussion between doctors and patients as a lack of competence on the doctor’s side. Trust in doctors also influences the provision of accurate medical history and conditions, compliance with doctor’s advice, participation in preventive screenings, use of harmful remedies, and satisfaction with care (Lai & Surood, 2010; Topal, Eser, Sanberk, Bayliss, & Saatci, 2012).
Cultural differences between immigrant groups and the native-born in body images can have impact on the health and HSU of immigrants. The impact could stem from two directions. On one hand, some immigrant groups such as many south Asians believe that a larger body size symbolizes good health, and such belief lowers their motivation to develop or maintain healthy lifestyle behaviors and seek health services (Patel, Philips-Caesar, & Boutin-Foster, 2012; Simeon et al., 2003). On the other hand, a much greater proportion of immigrants, especially those from Asia, Africa, and Latin America, find discrepancies between their own body sizes or cultural norms about body images and the ideal body images of tallness and slimness prevalent in the United States and other Western societies for women (Fallon, 1990; Wiseman, Gray, Mosimann, & Ahrens, 1992). These immigrant women are vulnerable to body image distortions and eating disorders as they may feel the heavy burdens to correct their own negative body images through unnecessary dieting, cosmetic surgeries, and tanning (Evans & McConnell, 2003; Hall, 1995; Kawamura, 2002).
Macrostructural/Contextual Factors
While individual health care needs, resources, and predisposition reflect individual life choices, social structure signifies life chances constrained by the larger society. Although most empirical analyses continue to focus on individual-level determinants of HSU (Derose et al., 2011), the role of macrostructural conditions in determining HSU must be recognized because these macro conditions do exert significant influence on the behaviors and likelihood of individual HSU. Macrosturctural or contextual factors may be defined as conditions at the societal or community level that are beyond individual control. There are general macrostructural conditions and also immigrant-specific contextual variables.
General macrostructural conditions
General macrostructural conditions include at least government policy, the health care system, and other larger social, economic, and political conditions. Government policy can significantly increase or decrease immigrant HSU. Unlike Andersen (1995) who only recognizes the importance of national health policy, we argue that government policy, not necessarily just health policy, can influence immigrant HSU. Some policies may not be designed to influence health behaviors but can significantly impact HSU. For example, the PRWORA enacted by Congress on August 22, 1996, is not a government health policy according to its intent. However, this law made most legal immigrants ineligible for publicly funded services such as Medicaid for the first 5 years of residence and Supplemental Security Income and Food Stamps until acquisition of U.S. citizenship and established other restrictions (Derose et al., 2007). As a result, immigrants’ access to health care was restricted and their HSU declined significantly (see, for example, Ellwood & Ku, 1998; Hagan, Rodriguez, Capps, & Kabiri, 2003; Kandula, Grogan, Rathouz, & Lauderdale, 2004). It should be noted that state or local government policies can have impact on HSU as well. A case in point is the policy of the Hawaii state government that granted Marshallese immigrants the unique legal right to apply for a state health insurance program (Hawaii Section 1115 Medicaid Waiver program) and other state-funded public benefits while disallowing Filipino, Korean, and other immigrant groups the same right, leading to big differences in health insurance and utilization rates among these immigrant groups (J. Y. Choi, 2009).
Intertwined with government policy, the health care system could have dramatic effects on the HSU of immigrants. For instance, the new Obama care system under The Affordable Care Act can boost the HSU of legal immigrants because like U.S. citizens, they are mandated to acquire health insurance, are eligible to buy insurance through the health insurance exchanges, and are qualified to receive the premium and cost-sharing subsidies. However, undocumented immigrants are not covered by the mandate for obtaining health insurance coverage and are ineligible for the health insurance exchanges and the subsidies (Bustamante et al., 2012).
Other macro conditions may also impact immigrant HSU. For example, a severe economic recession can increase unemployment, lower average income, increase individual cost-sharing of health insurance premium, and therefore, reduce the HSU of immigrants. Civil war, domestic unrest, and social disorder may negatively impact immigrant HSU.
Immigrant-specific contextual variables
Whereas the role of general macrostructural conditions in HSU has been recognized, the role of immigrant-specific contextual variables has received insufficient attention. In fact, immigrant-specific contextual factors have great impact on immigrant HSU. Context of emigration is an essential predictor of immigrant HSU. Immigrants leave their country of origin under different conditions. How they exit affects how they use health services in the host country. For instance, Portes et al. (1992) showed that the Cuban government-sponsored exodus of Mariel refugees (including some elderly, criminal, and mentally ill Cubans) in 1980 positively impacted the mental HSU of these refugees because of the available mental health services to them in Cuba prior to departure, whereas self-selected migration of male and younger Haitian refugees in the early 1980s reduced their need for mental health services. Because of immigrant selectivity, economic immigrants may have a lower level of need and propensity for HSU than refugees.
Experience of HSU in the homeland prior to emigration can have a lingering effect on immigrant HSU in the host country. For instance, as shown by Portes et al. (1992), Cuban refugees had prior exposure to mental health facilities under the Communist system in Cuba and were more likely to use mental health services in Florida, but Haitian refugees leaving remote rural areas in their impoverished homeland had little knowledge of mental health facilities and exposure to such service and were less likely to use mental health services in Florida. Immigrants from countries with a universal health care system (e.g., Germany, Belgium, Canada, Spain) are more likely to carry health insurance and use health services in the United States, but immigrants from many African, Asian, and Latin American countries without a universal health care system tend to have a lower rate of HSU (Sanz et al., 2011).
Context of reception by the host country also plays an important role in immigrant HSU. Context of reception comprises governmental, societal, and communal levels (Portes & Rumbaut, 2001). Government policies toward new immigrants include exclusion, passive acceptance, and active encouragement. Attitudes of the host society toward newcomers vary in terms of newcomers’ race, class, religion, language, and so on. The most immediate context of reception is immigrants’ ethnic community, which can vary from non-existence to existence and from working-class and peasant community to middle-class, professional, and entrepreneurial community. The existence of ethnic community or networks is crucial for immigrant HSU because the ethnic networks help socialize new immigrants to normative health-seeking behaviors, and offer information on health services, assistance in translation and transportation, and advice for health care decision making (Doherty & Campbell, 1988; LeClere et al., 1994). Variations and combinations at these three levels of context of reception can produce differential effects on immigrant adaptation in general and immigrant HSU in particular. For example, the hostile stance of the U.S. government and society toward both Mariel refugees and Haitian refugees in the early 1980s placed both groups at a disadvantageous position in incorporation and health services. However, the Cuban ethnic enclave with a professional and entrepreneurial component in Miami offered a more favorable environment for Cuban refugees in mental health services, whereas an absence of the preexisting Haitian ethnic community in Miami put Haitian refugees in an unfavorable milieu for receiving mental health service (Portes et al., 1992). Apparently, ties to the ethnic community in the host country are crucial for immigrant HSU as they can provide economic, social, and medical resources and support for newcomers. J. Y. Choi (2009) also demonstrated how the differential health policy treatments of Filipino, Korean, and Marshallese immigrants by the Hawaii state government and the differences in ethnic community and individual networks led to different rates of health insurance and health services among these three immigrant groups.
Mediating Effects
In addition to the direct effects of the foregoing determinants, some of the predisposing and macrostructural/contextual factors may affect immigrant HSU indirectly through other variables. This is also known as mediating or intervening effects. These mediating effects are specified in Figure 1. A solid line denotes a direct effect; a broken line indicates that some of the factors within the category have an indirect effect on HSU via one or more mediating variables, but the mediating relationships do not necessarily occur in a total fashion. For instance, age, one of the general predisposing factors, definitely has an effect on HSU via need factors. As one ages, the need for health care generally rises, and so will HSU. Put differently, need factors mediate the relationship between age and HSU. In the same vein, genetic factors, another general predisposing factor, can impact the need for health care, which in turn affects HSU. SES, also part of the general predisposing factors, can influence HSU through enabling factors because people with a higher SES tend to have more resources than those with a lower SES. Immigration status, an immigrant-specific predisposing factor, has an indirect effect on HSU through enabling factors. This is so because, for example, undocumented immigrants have much less resources for health care and, therefore, are less likely to use health services. Nevertheless, health beliefs, part of the predisposing factors, may not necessarily affect HSU through resources.
Macrostructural/contextual factors can influence HSU through resources and predisposing factors. For example, the Obama care system has an immediate impact on immigrant HSU through enabling factors by increasing the access of legal immigrants to health care while decreasing the access of undocumented immigrants. The PRWORA impacts immigrant HSU primarily through enabling factors by restricting immigrant access to health care. Immigrant-specific contextual variables indirectly affect immigrant HSU by impacting their resources, especially access to health care. Government policy can also have an impact on HSU by allowing immigrants to change their immigration status (e.g., legalization of undocumented immigrants) and by facilitating their assimilation to the host society.
Conclusion
There are plenty of theories of people’s HSU in general, but systematic theorization that explains the HSU of immigrants, a special and vulnerable population, is still lacking. In particular, greater endeavors must be made to incorporate more recent research into a theory of immigrant HSU. This article aims at developing a theoretical framework that can account for immigrant HSU. Toward this end, the article briefly reviews existing theories of HSU, including earlier non-Andersen models and the most influential Andersen health behavior model.
Modifying Andersen’s framework, we propose a theoretical framework that explains disparities in immigrant HSU by four categories of determinants at the general and immigrant-specific levels: (a) need for health care, indicating motivations for health services; (b) resources, representing ability to receive, and/or access to, health services; (c) predisposing factors, signifying propensity for HSU in terms of demographic, socioeconomic, and genetic factors, and health beliefs; and (d) macro social structural or contextual conditions, representing general sociostructural factors in the larger society beyond individual control. In addition to the determinants at the general level, we identify and specify immigrant-specific determinants that distinguish immigrants and the native-born in HSU. These factors include four categories: (a) immigrant-specific health needs or conditions; (b) homeland-based financial and social resources and transnational access to health care; (c) immigrant-specific predisposing factors including immigration status, signifying vulnerability or invulnerability to receive health care; assimilation, indicating immigrants’ adaption to the host society that leads them to behave similarly to natives in HSU, and immigrant ethnic culture, betokening the cultural tradition of immigrant groups that offers alternatives to standard professional health care; and (d) context of emigration, context of reception, and HSU in the homeland. We also consider the mediating effects of some of these factors.
As can be seen, we retain the need factors, enabling factors, and predisposing factors in Andersen’s framework. However, our model differs from the Andersen model in several important aspects. First and foremost, we systematically theorize and categorize the conditions that specifically influence the HSU of immigrants and distinguish immigrants and non-immigrants in HSU. Our model will help researchers, health care professionals, and policymakers focus attention to conditions particularly germane to immigrant HSU, collect data especially pertinent to it, and make decisions that improve immigrant HSU. Second, we carefully consider the mediating effects of some determinants and specify which variable influences immigrant HSU through which mediating variable. Third, we divide resources into three types, including financial resources, social resources or social capital, and access to health care, and we stress the important role of social resources. Fourth, we single out macro social structural conditions and call attention to the role of these conditions in immigrant HSU. Finally, differing from the Andersen model, we consider both health policy and non-health policy that directly and indirectly influence immigrant HSU. A case in point is the PRWORA of 1996, a non-health policy that has impacted immigrants’ HSU by excluding most legal immigrants from publicly funded services including Medicaid. We believe that our framework makes significant improvements over the Andersen framework and can offer a fuller understanding of the determination process of immigrant HSU. This theoretical framework is subject to empirical validation and rejection. It should also be noted that for empirical testing, this general framework may need some modifications contingent upon specific type of HSU, location, and time.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.