
Abstract
Animal-assisted activities (AAAs) are mainly carried out in institutions. The aim of this prospective pilot study was to assess the willingness of patients with cardiac implanted electronic devices (IEDs) to participate in AAA. The sample included 75 ambulatory patients (18 females, M age = 69 years), who attended an outpatient clinic for control of antibradycardic pacemakers (n = 15) or implanted cardioverter defibrillators (n = 60). Twenty-three percent were current and 48% were previous pet-owners. Current pet-owners were younger than non-pet-owners (63.5 vs. 72.0 years, p = .0003). Twelve patients (16%) showed interest in AAA visits. However, only two patients agreed to an AAA visit. Both patients were visited once, but declined further visits. Hence, AAA sessions at home were poorly accepted, mainly because the patients considered themselves too busy or healthy, or due to a general disinterest in AAA. Potential health benefits associated with AAA may not be feasible to investigate during home visits of AAA-teams in patients with IEDs who are healthy enough to leave their homes. For further studies concerning AAA in patients with cardiovascular diseases, we suggest focusing on institutions like rehabilitation centers or day care centers and on more severely sick, homebound patients.
Introduction
Animal-assisted activities (AAAs) have been applied for more than 40 years in patients with different psychological and physical disorders. In AAA, the bond between humans and animals is used as an integral part of a patient’s treatment. AAA in health care involves a variety of species like dogs, cats, horses, and domesticated birds. Despite their increasing application in a wide range of therapeutic services, the empirical evidence base of AAAs is limited (Beetz, Uvnas-Moberg, Julius, & Kotrschal, 2012; Munoz Lasa et al., 2015). There are only few randomized studies which have investigated the effect of AAA, as listed in Table 1 (Borgi et al., 2016; Calcaterra et al., 2015; Cole, Gawlinski, Steers, & Kotlerman, 2007; Friedmann et al., 2015; Harper et al., 2015; Ko, Youn, Kim, & Kim, 2015; Majic, Gutzmann, Heinz, Lang, & Rapp, 2013; Menna, Santaniello, Gerardi, Di Maggio, & Milan, 2015; Nurenberg et al., 2015; Vagnoli et al., 2015; Wohlfarth, Mutschler, Beetz, Kreuser, & Korsten-Reck, 2013). Most of these studies were carried out in patients with psychiatric disorders.
Overview of Randomized Studies Investigating Animal-Assisted Activities.

However, patients with cardiovascular disorders may also benefit from AAA. AAA use in cardiovascular disease has been previously reported only from hospitalized patients. In one study of patients with advanced heart failure, a 12-min hospital visit with a therapy dog improved hemodynamic parameters, neurohormone levels, and anxiety (Cole et al., 2007). In a further study of 69 patients, canine-assisted ambulation was a safe and effective adjunct to an early ambulation program for hospitalized heart failure patients (Abate, Zucconi, & Boxer, 2011). It is unknown, however, whether these beneficial effects persist during a long-term follow-up period after hospital discharge.
It has been observed that physiological variables such as cardiac autonomic activity change during short-term interactions with animals and are positively influenced by pet-ownership (Abate et al., 2011; Aiba et al., 2012). Registration of parameters of cardiac autonomic activity requires monitoring devices which have to be carried by the patient and, thus, might induce stress and inconvenience (Lobodzinski & Laks, 2012). Parameters of cardiac autonomic activity are also registered by modern implanted electronic devices (IED) like pacemakers or cardiac defibrillators and can be measured by device interrogation. Potential benefits of AAA on cardiac autonomic activity could be ideally studied in patients with IED.
So far, AAA has been carried out mainly in institutions, such as nursing homes; rehabilitation units; psychiatric, surgical, or orthopedic departments of hospitals; or prisons (Abate et al., 2011; Aiba et al., 2012; Beetz et al., 2012; Borgi et al., 2016; Calcaterra et al., 2015; Cole et al., 2007; Friedmann et al., 2015; Harper et al., 2015; Harris, Rinehart, & Gerstman, 1993; Ko et al., 2015; Majic et al., 2013; Menna et al., 2015; Munoz Lasa et al., 2015; Nurenberg et al., 2015; Vagnoli et al., 2015; Wohlfarth et al., 2013). Home visits for AAA are unusual in Europe; however, they are an offered service in the United States for homebound patients and are appreciated by patients who are too sick to leave their homes by themselves (Harris et al., 1993). It is unknown if ambulatory outpatients with cardiovascular disorders would be interested to be visited by AAA-teams in their homes. The aim of this prospective pilot study was to assess the willingness of patients with IEDs to participate in AAA home sessions.
Method
The study is a prospective, single arm, observational study. Subjects included were consecutive outpatients with IEDs who were scheduled for an appointment in the outpatient clinic for control of their IED between November 2012 and March 2013 in a cardiological outpatient clinic of a 900-bed community hospital in the center of a large city.
Step 1: In the waiting area of the outpatient clinic, pamphlets were displayed about AAA aimed to inform the patients.
Step 2: The study physician (P.J. or D.G.) approached the patient in the waiting area, introduced himself as study physician and informed the patient about AAA referring to the pamphlet.
Step 3: If the patient showed interest, the patient was interviewed by the study physician about current and previous pet-ownership according to a preset questionnaire. The subjects were offered AAA free of any charge. They could choose being visited at home or to meet with the therapy team in the outpatient clinic and between a dog and a cat as therapy animals. The potential health benefits of regular AAA-visits over the course of the study were identified. Finally, patients were asked whether they were interested in visits of AAA-teams, and those who were not interested were asked to explain precisely why.
Step 4: In case they were interested, physicians explained to them the study procedures, the opportunities, aims, and potential benefits. The patients had to fill in a questionnaire about their former experiences with animals. In addition, the following demographic and clinical data were documented: age, gender, type of IED, and current and previous pet-ownership. All these recruitments were done in the waiting room. The cardiologist responsible for the clinical examination and check-up of each patient’s IED was not involved in the study. This person was informed of the activity of the study physician in the waiting area, but did not interfere with or influence patients’ decisions regarding their possible participation in AAA.
Step 5: After initial contact, the patients were approached by telephone within 1 week by a certified AAA-team to arrange an appointment. Informal records, without the use of a specific pro forma, were made of patients’ reactions to the telephone call.
The AAA-teams considered the following activities which they typically carry out according to the preferences of the patients: encouraging patients to pet the dog, brush the coat, throw a ball, give treats, let the dog perform some feats, or talk about the patient’s experience with pets. As the purpose of the pilot study was to determine feasibility of the AAA home visits, the activities during the AAA-visits were not specifically planned in advance, and no preset protocol forms for documentation of the activities was developed. The agreed procedure included writing an informal report about each visit. If a current pet-owner expressed an interest in an AAA visit, the procedure included the plan of an individual approach by the AAA-team to avoid conflicts between the visiting therapy animal and the resident pet.
The AAA-teams consisted of specially trained and certified therapy dogs and their handlers, being members of the organization “Tiere als Therapie” (Animals for Therapy), an ESAAT (European Society for Animal-Assisted Therapy) member association with high quality standards and long experience in AAA (http://www.en.esaat.org/). The requirements for the therapy animals of this organization are as follows: excellent health status with a health certificate renewed every year by a veterinarian, free of any pain, good-tempered character, free of any parasites and precautions against parasites, and completely vaccinated. Furthermore, therapy animals are trained using positive reinforcement techniques to be stress-resistant and relaxed with regard to contact with new situations, children, and other animals and stress-resistant with regard to unknown sounds, movements, and optical stimuli. An annual evaluation of the therapy animal’s behavior and the AAA-team performance is carried out to ensure best working practice.
For statistical analysis, differences among categories were tested by applying Fisher’s test for categorical variables and by t test for continuous variables. The analysis was conducted by the statistical software R (R Core Team, 2014).
The study was ethically approved by the institutional review board of the Wiener Krankenanstaltenverbund in Vienna, and oral informed consent was obtained from all included patients for the interview in the waiting area.
Results
Step 1: Overall, 120 patients were asked to participate in the interview in the waiting area.
Step 2: Twenty of these 120 patients declined the interview because of the following reasons: no interest in the interview (n = 8), language barriers (n = 7), and hardness of hearing (n = 5).
Step 3: The remaining 100 patients were interviewed; however, 25 of them were excluded because they had no IED. Thus, 75 patients, 57 males and 18 females, with a mean age of 69 years (range = 42-91) were included in the analysis. Fifteen patients had antibradycardic pacemakers (PM), 44 had implanted cardioverter defibrillators (ICD), 14 had an ICD combined with a cardiac resynchronization device (CRT-D), and two patients had a PM combined with an ICD. All 75 patients were ambulatory, none of them were wheelchair-bond or in need for assistance to attend the outpatient clinic.
Six of the 75 patients did not provide information about previous or current pet-ownership. From the remaining 69 patients, the following information about pet-ownership was provided: Sixteen of the patients (23%) were current pet-owners (dog: n = 6, cat: n = 4, dog and cat: n = 4, hamster: n = 1, bees: n = 1). The mean age of the 16 current pet-owners was lower than that of the 53 current non-pet-owners (63.5 vs. 72.0 years, p = .003). Of the 53 current non-pet-owners, 33 patients reported previous pet-ownership (dog: n = 19, cat: n = 7, dog and cat: n = 5, hamster: n = 2). The clinical characteristics of the 49 former and current pet-owners did not differ from the 20 patients who were never pet-owners, as listed in Table 2.
Step 4: Twelve of the included 75 patients (16%) were initially interested in receiving AAA during home visits. None of the patients were interested in meeting with the AAA-team in the outpatient clinic. Ten of these 12 were previous pet-owners and only two had never had a pet (p = .0553). Their clinical characteristics were not different from those of the 63 patients who were not interested in AAA. The following reasons were given by the 63 patients who were not interested in AAA: no interest at all (n = 19), too busy (n = 13), current pet-ownership (n = 11), living outside of Vienna (n = 6), aversion to animals (n = 3), no trust in AAA (n = 4), language problems (n = 3), refusal to speak (n = 2), scheduled surgery (n = 1), and mental illness (n = 1).
Step 5: Of the 12 patients who were initially interested, only two agreed to a visit of an AAA-team in their homes. The AAA-teams reported that during the visits, both patients were engaged. One patient was not interested in AAA but was happy to have someone to talk to. He did not show any interest in the dog and considered himself inappropriate for AAA. Therefore, no further visits were carried out. The second patient, a previous dog owner, was interested in the dog, enjoyed, and was engaged in the visit but still did not want a continuation of the visits because he did not expect any benefit for his situation.
Comparison of Clinical Characteristics Between Ever and Never Pet-Owners.
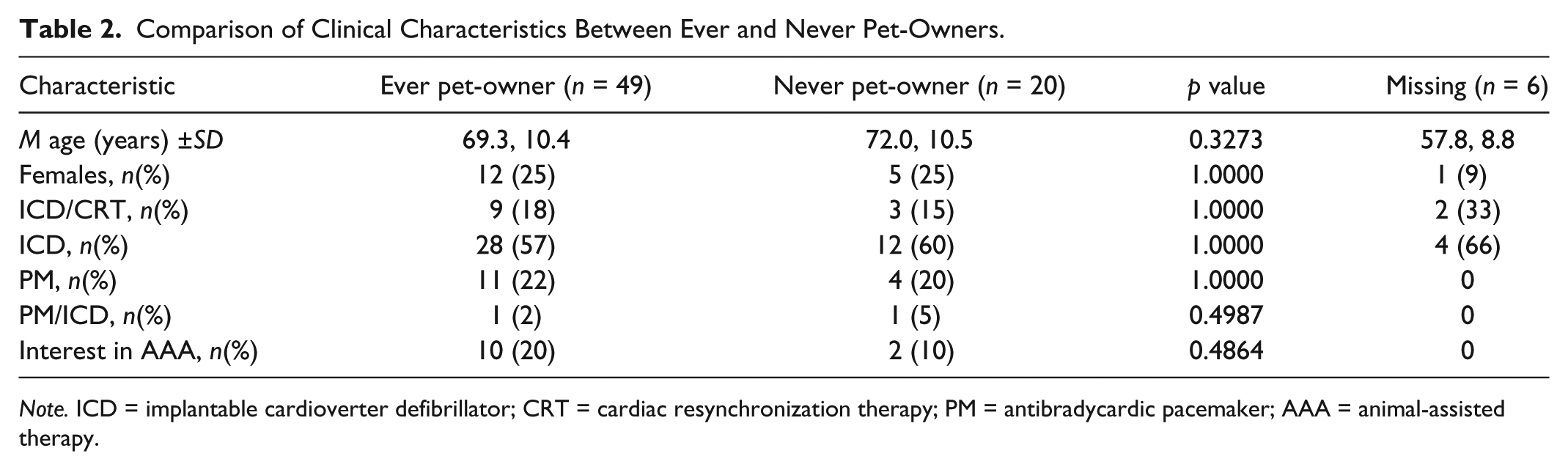
Note. ICD = implantable cardioverter defibrillator; CRT = cardiac resynchronization therapy; PM = antibradycardic pacemaker; AAA = animal-assisted therapy.
The remaining 10 patients, who were initially interested, refused a visit due to the following reasons: one patient’s wife was hospitalized, therefore, AAA would have been too much stress for him. Another had too many appointments and no time for AAA, while a further patient was afraid that the dog could harm her dialysis shunt. One patient from the group felt too healthy for any therapy, two had lost interest in AAA, and one was hospitalized and subsequently died. Two patients could not be contacted by telephone, and one could not remember that he had claimed interest in AAA.
Overall, the results of this pilot study showed that 23% of patients with IEDs were current pet-owners, 48% previous pet-owners, and 29% have never owned a pet. Pet-owners with IEDs were younger than non-pet-owners. Only 16% of patients with IEDs expressed an interest in visits of AAA-teams in homes, while only two patients agreed to a visit. While only two patients (2.6%) were visited, both patients declined continuation of AAA. Thus, it seems that AAA-visits in their homes were not valued by patients with IEDs, although a high proportion of them were previous or current pet-owners.
Discussion
The low rate of interest for AAA may be due to the fact that the included patients considered themselves as relatively healthy, thus avoiding any additional contact with the hospital. This assumption is substantiated by the finding that none of the patients wanted AAA-team visits in the outpatient clinic.
Surprisingly, although 12 patients were interested in and consented to home visits, in only two cases were visits actually completed. It is possible that patients were fearful of jeopardizing their care by saying no, even if the physician was not objectively coercive in any way and the physician, who explained the study, was not the care provider. A further factor may be the lack of a specific protocol or script for the telephone call making the visit appointment. It is therefore not possible to be sure that each patient received exactly the same information over the phone.
It remains unclear if outpatients with cardiovascular disorders are willing to accept visits of AAA-teams in their homes. The results of our pilot study suggest a low rate of acceptance due to various reasons, mainly because the patients consider themselves as too busy or healthy, or are not interested in AAA. As home settings differ from institutions in patients’ degree of control, privacy, and how time is spent, patients’ estimation of AAA might differ between these settings (Harris et al., 1993). Patients may prefer not to have “guest pets” in their homes.
Based on these experiences with this subset of outpatients with IEDs, it has to be investigated whether AAA in another setting, outside the patients’ homes, would be more accepted or whether AAA-team visits in patients’ homes with advanced stages of heart failure would be an option. For further studies concerning AAA in patients with cardiovascular diseases, we suggest focusing on institutions like rehabilitation centers or day care centers. Furthermore, the monitoring function of IEDs could be used to assess the influence of animal–human interaction on parameters of cardiac autonomic activity in interested patients, pet-owners as well as non-pet-owners, with IEDs. Care has to be taken to define a protocol for information transmitted by phone between AAA-teams and patients to avoid misunderstandings.
Limitations of the study are the low number of patients and the absence of any assessment of psychiatric comorbidities like depression or anxiety, which could have had an impact on the very low interest in AAA. Furthermore, degrees of sickness and functional disability were not assessed. Information on the ethnic and religious background of the patients was not gathered, meaning that any possible relationships between these factors and interest in AAA could not be assessed.
Our findings suggest that the previously reported benefits of AAA in ambulatory outpatients with cardiovascular disorders may not be feasible to investigate during home visits of outpatients with IEDs by AAA-teams. More studies with patients across the range of cardiac illness severity are needed.
Footnotes
Acknowledgements
The authors thank Andrea Beetz, PhD, and Erika Jensen-Jarolim, MD, for fruitful discussions; members of the association “Tiere als Therapie” and their dogs for helpful support and visits to the patients’ homes; and Amelia Wein, for help with the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The study was supported by Comparative Medicine, Messerli Research Institute, Vienna, Austria.