
Abstract
Keywords
There is some evidence of increases in alcohol-related harm in Australia, despite relatively stable rates of alcohol consumption for the total population (Byrnes, Shakeshaft, Petrie, & Doran, 2013; Livingston, Matthews, Barratt, Lloyd, & Room, 2010). Early adulthood, generally defined as the period from age 18 to age 26, is the peak age for harmful levels of not only alcohol but also other drug use (Stone, Becker, Huber, & Catalano, 2012). One possibility, which remains untested, is whether the use of amphetamine-type stimulants (ATS; that is, ecstasy [3,4-methylenedioxymethamphetamine or MDMA] and methamphetamine) is associated with hazardous alcohol consumption among young adults. Heavier patterns of alcohol consumption have been observed among young adult ATS users compared with non-users (Degenhardt, Barker, & Topp, 2004; Furr, Delva, & Anthony, 2000). This combined use of alcohol and stimulants is an emerging concern, as a growing body of research suggests that combined use may result in greater harms than the separate use of these substances (Fisk, Murphy, Montgomery, & Hadjiefthyvoulou, 2011; Hedden et al., 2010). However, factors that may lead to hazardous alcohol consumption among ATS users have not been systematically examined.
It is plausible that the recurrent use of stimulants, including ecstasy and methamphetamine, could lead to increases in alcohol consumption. A number of preclinical studies provide evidence suggesting that repeated exposure to stimulants may be associated with increased sensitivity to the stimulant effects of alcohol due to alterations in endogenous reward processes, especially those involving the dopaminergic system (see Ferreira, Abrahao, & Souza-Formigoni, 2013; Lessov & Phillips, 2003). Lessov and Phillips’ (2003) study of adult female mice found that repeated administration of cocaine resulted in significant behavioral sensitization to ethanol. Increased sensitivity to the stimulant effects of alcohol may, in turn, increase the risk of subsequent binge drinking and alcohol use disorders. In a multidose laboratory study of 104 high-risk heavy social drinkers and 84 light drinker controls, King, de Wit, McNamara, and Cao (2011) observed greater stimulant and rewarding effects from alcohol among heavy drinkers in comparison with light drinkers. In addition, experiencing greater positive effects from alcohol was associated with increased frequency of binge drinking during the study’s 2-year follow-up (King et al., 2011). Furthermore, it is possible that regular ecstasy or methamphetamine users may need to drink larger quantities of alcohol to experience its rewarding stimulant effects, as a consequence of lasting damage to dopaminergic receptors arising from neurotoxic levels of ecstasy or methamphetamine use (see Cole, Sumnall, O’Shea, & Marsden, 2003; Izco et al., 2007). Alternatively, regular ATS use may have an indirect effect on long-term drinking patterns. Recurrent episodes of alcohol and ATS use, involving greater-than-usual levels of alcohol consumption, could increase the likelihood of future alcohol use disorders simply as a consequence of increased alcohol consumption over a period of time (Magura & Rosenblum, 2000). However, our current understanding of these issues is limited by the fact that there is a lack of longitudinal research to assess the potential mechanisms underlying the association between ATS use and hazardous alcohol use. Previous observational studies are predominantly cross-sectional in design. The available prospective research suggests that sustained stimulant use is associated with greater alcohol consumption than other patterns of illicit drug use but does not establish whether prior stimulant use contributes to these drinking patterns (Borders & Booth, 2012; Gossop, Browne, Stewart, & Marsden, 2003). Consequently, the actual impact of ATS use on young adults’ subsequent alcohol consumption is not well understood.
Hazardous levels of alcohol consumption among ATS users could also be indicative of a concurrent, rather than longitudinal, relationship between ATS and alcohol use. The combined use of ATS and alcohol may serve an instrumental function in young adults’ drug use episodes. First, ATS use may facilitate binge alcohol consumption. Individuals under the influence of ATS are potentially able to consume alcohol without experiencing the usual sedative effects (Hernández-López et al., 2002), thus facilitating longer wakefulness and longer periods of drinking. Second, ATS users may drink greater quantities of alcohol to mitigate unwanted effects of ATS. It has been noted that users sometimes “pre-load” with alcohol during the onset phase of the stimulant use episode, and “post-load” during the come-down phase, to mitigate effects, such as anxiety, agitation, and restlessness (Fisk et al., 2011). In addition, young adults may combine ATS and alcohol to maximize the desired subjective effects of either substance. In particular, simultaneous ATS and alcohol use may produce a longer lasting euphoria than the separate use of these substances (Hernández-López et al., 2002).
There are also a number of individual factors that may predispose young adults to both alcohol and ATS consumption, and thus provide an alternative explanation for alcohol consumption levels among ATS users. Early and regular alcohol use in adolescence is associated with hazardous alcohol use in early adulthood (Bonomo, Bowes, Coffey, Carlin, & Patton, 2004; Toumbourou et al., 2014) and increased risk of subsequent ATS use (Hayatbakhsh, Najman, Bor, & Williams, 2009; Wu, Liu, & Fan, 2010). In a longitudinal study of 2,042 Australian young adults, Hayatbakhsh and colleagues (2009) found that drinking alcohol at age 14 significantly predicted both amphetamine use and amphetamine-use disorders. Similarly, a number of other adolescent factors (e.g., school performance, peer networks, and psychological distress) can contribute to hazardous alcohol use in early adulthood (Kuntsche, Rehm, & Gmel, 2004), and may also contribute to ATS use in this age group (Degenhardt, Coffey, Carlin, Moran, & Patton, 2007; Hayatbakhsh et al., 2009). Consequently, it is important to control for these potential confounding factors.
The role of the social environmental context of ATS and alcohol use must also be considered. Stimulant use is inextricably linked to young adults’ social environmental settings (Van Havere, Vanderplasschen, Lammertyn, Broekaert, & Bellis, 2011), and the settings in which ATS are used may contribute to hazardous levels of alcohol consumption (Jacinto, Duterte, Sales, & Murphy, 2008; Singer & Schensul, 2011). Licensed venues, particularly nightclubs, are characterized by both alcohol and other drug use (Calafat, Fernández, Juan, & Becoña, 2008; Van Havere et al., 2011) and, consequently, may encourage simultaneous use. Ecstasy was linked to the rave scene from the mid-1980s (Engels & ter Bogt, 2004). In earlier periods, alcohol consumption appeared to be relatively infrequent within this scene and possibly even viewed as undesirable (Duff, Johnston, Moore, & Goren, 2007). However, Australian evidence suggests a possible departure from these “traditional” patterns of ecstasy use (Breen et al., 2006; Kinner, George, Johnston, Dunn, & Degenhardt, 2012). In addition, the social settings in which ecstasy is used appear to have diversified to encompass venues such as nightclubs, pubs, and music festivals (Agar & Reisinger, 2004; Horowitz, Galanter, Dermatis, & Franklin, 2008). However, the possible relationship between and influence of social settings of consumption on ATS and alcohol use, beyond raves and electronic dance music events, has not been examined.
To explore why ATS users also frequently use alcohol, this study examines ATS and alcohol use patterns and engagement with licensed venues as predictors of hazardous patterns of alcohol use after 30 months of follow-up among a population-based sample of Australian young adult ATS users (aged 19-23 years). Because there may be common predictors of ATS and alcohol use, the study adjusts for a number of potential confounding factors, including age, sex, early alcohol use, baseline alcohol use, ATS-using social contacts, school suspension, income, and psychological distress.
Method
Participants
The Natural History Study of Drug Use (NHSDU) is a prospective longitudinal study of drug use in a population-based sample of young adults in South-East Queensland, Australia, which commenced in 2009. Drug-use screening questionnaires were mailed to 12,079 young adults (aged 19-23 years) randomly selected from the Brisbane and Gold Coast electoral roll (response rate = 49.9%). From the screening data, we developed a sampling frame from which an ATS-user group (used ecstasy or methamphetamine ≥ 3 times within the last 12 months) was recruited. The threshold of ≥3 occasions of ecstasy use or ≥3 occasions of methamphetamine use in the last 12 months was used to recruit recurrent, rather than experimental, users of these substances. These groups were not mutually exclusive; participants could be recruited on the basis of their use of either or both substances. Of the young adults screened (N = 6,029), 522 (8.7%) were eligible to participate on the basis of their ATS use, and 352 of these eligible ATS users participated in the baseline interview. This method is described in detail elsewhere (Smirnov, Kemp, Wells, Legosz, & Najman, 2014).
Data for this study are drawn from the baseline face-to-face interview, and 6- and 30-month follow-up online surveys. In the current study, 60 cases (17.0%) were excluded due to missing data, including 33 participants who did not complete the 6- or 30-month surveys. These 60 participants did not differ significantly from other ATS users in terms of alcohol or ATS use, with 90.0% consuming alcohol in the last month at baseline compared with 95.9% of the current ATS-user sample (χ2 = 0.46, ns). On average, the excluded participants consumed alcohol on 11.4 days in the last month compared with 9.6 drinking days among the current sample (z = −1.00, ns). In addition, 38.8% and 28.6% of the excluded participants had used ecstasy and methamphetamine in the last month, respectively, compared with 42.1% and 22.6% of the current ATS-user sample (ecstasy: χ2 = 0.19, ns; methamphetamine: χ2 = 0.83, ns). The final sample for this study is 292 ATS users.
Measures
30-month alcohol use (outcome)
Alcohol consumption at 30 months was assessed by a quantity–frequency measure of last month alcohol consumption (i.e., days of consumption × number of standard drinks on a typical day in the last month). A standard drink was defined as any drink containing 10 g of alcohol (National Health and Medical Research Council, 2009). Participants were provided with a chart showing the number of standard drinks in a range of different sizes and types of beverages (beer, wine, and spirits). We focused on last month consumption patterns as this involved better recall than a longer reference period (Stockwell et al., 2004).
We created a categorical variable for alcohol use at 30 months based on recognized thresholds for hazardous drinking (i.e., ≥ 5 standard drinks on a drinking occasion; Naimi et al., 2003) and the distribution of quantity–frequency levels in our sample. ATS users in this study tended not to be daily drinkers (last month drinking days: M = 9.65, 95% Confidence Interval [CI] = [8.78, 10.53]). This equates to drinking on about 2 days a week, which is suggestive of weekend drinking patterns. However, ATS users consumed a mean of 9.61 standard drinks per day of drinking in the last month (95% CI = [7.52, 11.70]), which is well beyond the threshold for hazardous drinking. To capture this range of consumption, four alcohol use categories were specified: low (0-14 standard drinks in the last month), moderate (15-50 standard drinks), high (51-99 standard drinks), and very high (≥100 standard drinks). The cutoff of 51 drinks for the “high use” category corresponds to ≥ 5 drinks per day of drinking for those who consumed alcohol on approximately 10 days per month (the average number of drinking days for the sample). Thus, the “very high use” category approximates ≥10 drinks per day of drinking.
Amphetamine-type stimulant use
Two elements of ATS use were measured: frequency and recency.
Frequency of ATS use
At baseline, participants were asked about the frequency of their ecstasy and methamphetamine use in the last 12 months. Dichotomous variables were created for frequency of ecstasy and methamphetamine use (<monthly use vs. ≥monthly use in the last 12 months).
Recency of ATS use
At 30 months, participants reported how recently they had used ecstasy and methamphetamine. The “recency” variables were included to capture the timing (i.e., concurrent patterns) of alcohol and ATS use and comprised three categories: (a) use in the last month, (b) use in the last 12 months (but not the last month), and (c) no use in the last 12 months. Because we wanted to capture all recent ATS use at 30 months, we did not limit the recency variables to ATS use that occurred concurrently with alcohol use.
Engagement with licensed venues
Two variables from the 6-month survey measured engagement with licensed venues: frequent (≥monthly) nightclub and pub/bar attendance in the last 12 months. Given the 12-month time frame, these variables address a period comparable with the baseline measures. Frequent venue attendance could also be a proxy for a more general propensity for recreational social activity. Therefore, a variable measuring weekly attendance at parties, measured at the 6-month survey, was included.
Background factors
To assess the independent relationship between ATS use and alcohol use, we adjusted for a number of individual and contextual factors. Patterns of alcohol use at 30 months are likely to reflect pre-existing alcohol consumption levels. Thus, we included a baseline alcohol use measure, adopting the same categories as the 30-month alcohol variable (low: 0-14 standard drinks in the last month; moderate: 15-50 standard drinks; high: 51-99 standard drinks; and very high: ≥100 standard drinks). As with the 30-month alcohol use variable, participants were classified into these categories based on a quantity–frequency measure of last month alcohol use at baseline (i.e., days of consumption × number of standard drinks on a typical day in the last month).
We also adjusted for age, gender, early alcohol use (before age 13), number of ecstasy- and methamphetamine-using social contacts at baseline (defined as how many ecstasy/methamphetamine users participants knew by face or name), school suspension, income at baseline, and psychological distress (evaluated at baseline using the Hospital Anxiety and Depression Scale [HADS]). The combined HADS subscales provide a valid and reliable measure of psychological distress, with a Cronbach’s alpha of .88 to .89 (Bjelland, Dahl, Haug, & Neckelmann, 2002; Cosco, Doyle, Ward, & McGee, 2012). A HADS score of ≥16 is used to indicate high levels of psychological distress (Bjelland et al., 2002).
Analysis
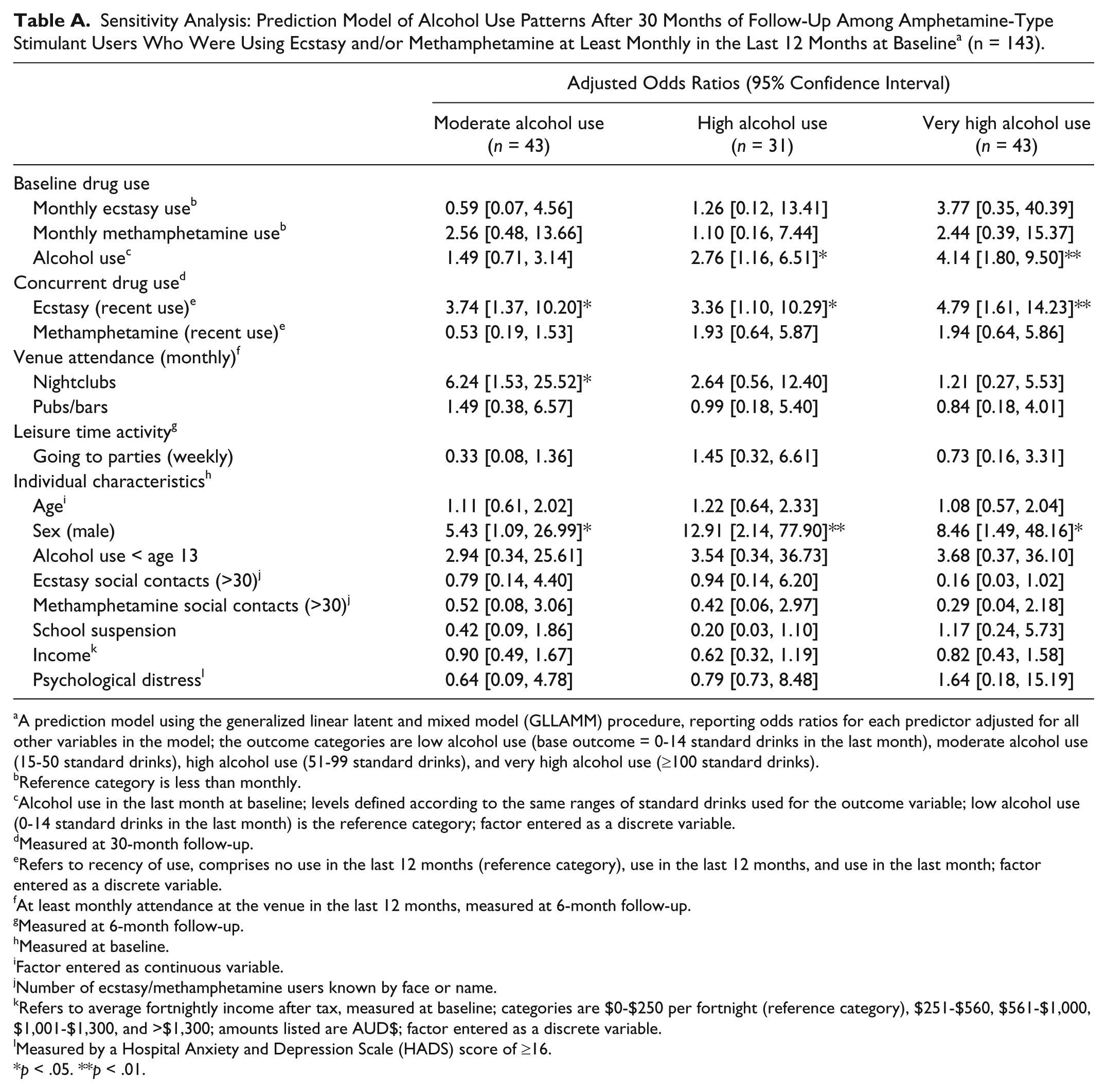
This study comprises longitudinal analysis of NHSDU data. Multinomial logistic regression reporting estimated odds ratios was conducted to examine unadjusted associations between patterns of alcohol use at 30 months and predictor variables. We developed a prediction model of 30-month alcohol use using mixed-effects multinomial logistic regression, conducted using Version 2.3.20 of the generalized linear latent and mixed model (GLLAMM) procedure for Stata (Rabe-Hesketh, Skrondal, & Pickles, 2005; Skrondal & Rabe-Hesketh, 2003). A two-level model was implemented, accommodating the repeated drug use measures for each individual. A sensitivity analysis was conducted with a subgroup of ATS users who were engaged in monthly or more frequent use of ecstasy and/or methamphetamine at baseline (see the appendix). The pattern of association was broadly similar to the results reported for the full sample in this study with no significant difference found in the magnitude of estimates (Altman & Bland, 2003). Data were analyzed using Stata/SE Version 11.2.
Results
Recent Ecstasy and Methamphetamine Use at Baseline and 30 Months
Use of both ecstasy and methamphetamine was common among ATS users in this study. At baseline, more than half (55.8%) of ATS users had used both ecstasy and methamphetamine in the last 12 months, while 39.7% and 4.1% had only used ecstasy or methamphetamine, respectively. One ATS user (0.3%) had not used either ecstasy or methamphetamine in the last 12 months. In contrast, more than a third of ATS users (36.3%) had not used ecstasy or methamphetamine in the last 12 months at the 30-month follow-up. Among recent users at 30 months, 29.5% had used both ecstasy and methamphetamine in the last 12 months, while 28.4% and 5.8% had only used ecstasy or methamphetamine, respectively.
Percentage With Characteristic For Predictor and Control Variables by 30-Month Alcohol Use Categories
Table 1 presents the percentage of ATS users in the “low,” “moderate,” “high,” and “very high” 30-month alcohol use categories with the characteristic for all predictor and control variables. Of those ATS users who were engaged in very high alcohol use at baseline, 41.1% were still drinking at very high levels after 30 months of follow-up. Furthermore, approximately one third (32.9%) and one quarter (24.4%) of ATS users who were drinking at high and moderate levels at baseline were drinking at very high levels after 30 months, respectively. Just under half (47.2%) of ATS users who were engaged in low levels of alcohol use at baseline were drinking at low levels at 30 months, while 41.5% had increased to moderate use. At 30 months, a higher proportion of male ATS users were drinking at very high (36.4% vs. 18.4%) and high (20.7% vs. 13.2%) levels, compared with female users.
Percentage (%) of Amphetamine-Type Stimulant Users in the “Low,” “Moderate,” “High,” and “Very High” 30-Month Alcohol Use Categories With Characteristic (n = 292).
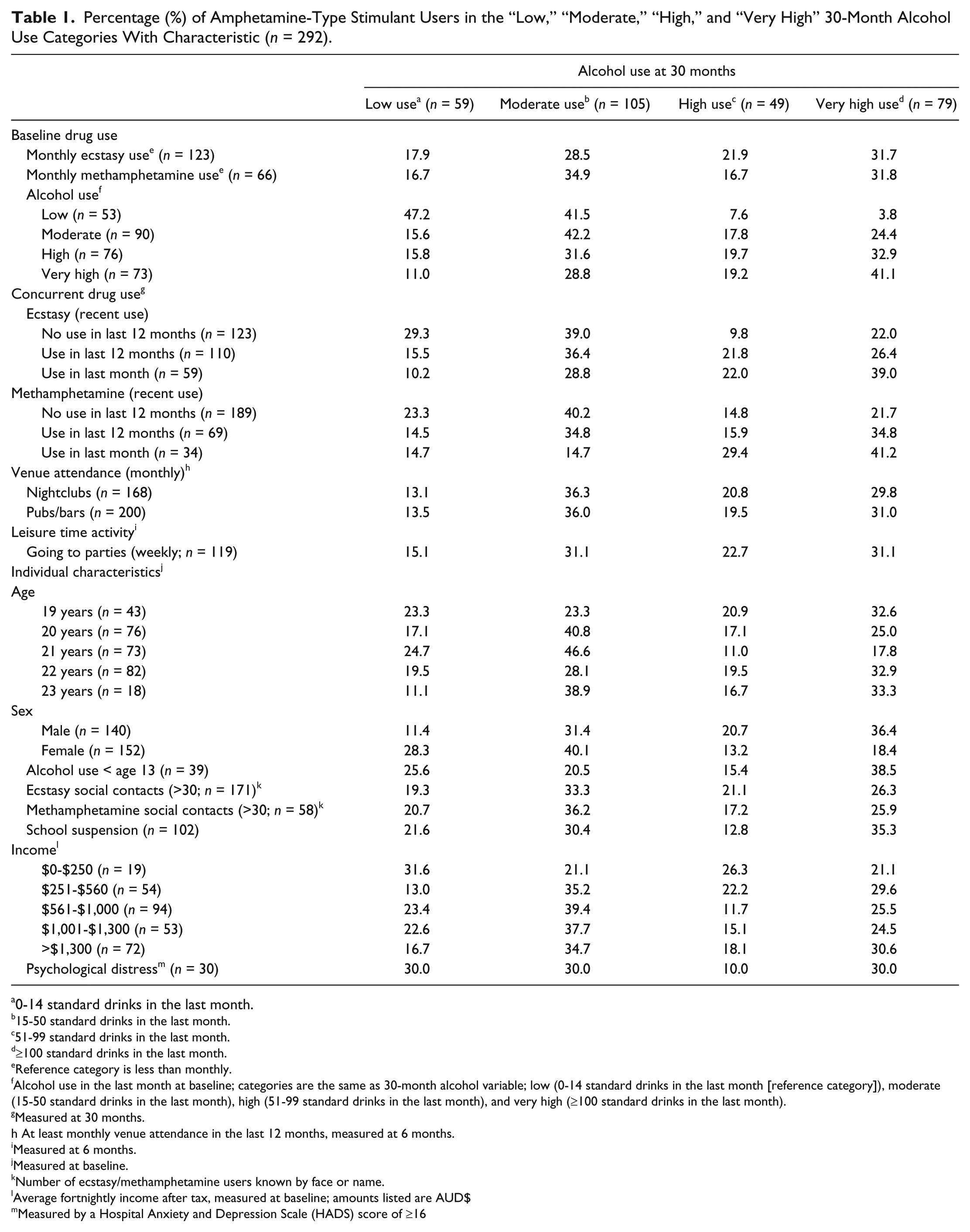
0-14 standard drinks in the last month.
15-50 standard drinks in the last month.
51-99 standard drinks in the last month.
≥100 standard drinks in the last month.
Reference category is less than monthly.
Alcohol use in the last month at baseline; categories are the same as 30-month alcohol variable; low (0-14 standard drinks in the last month [reference category]), moderate (15-50 standard drinks in the last month), high (51-99 standard drinks in the last month), and very high (≥100 standard drinks in the last month).
Measured at 30 months.
At least monthly venue attendance in the last 12 months, measured at 6 months.
Measured at 6 months.
Measured at baseline.
Number of ecstasy/methamphetamine users known by face or name.
Average fortnightly income after tax, measured at baseline; amounts listed are AUD$
Measured by a Hospital Anxiety and Depression Scale (HADS) score of ≥16
Predictors of Patterns of Alcohol Use Among ATS Users
Table 2 presents results of multinomial logistic regression reporting unadjusted odds ratios of high alcohol use at 30 months. Alcohol use patterns at 30 months were associated with baseline alcohol use, recency of ecstasy and methamphetamine use, frequent (≥monthly) nightclub and pub/bar attendance, going to parties on a weekly basis, and sex.
Predictors of Alcohol Use Patterns Among Amphetamine-Type Stimulant Users After 30 Months of Follow-Up—Unadjusted a Associations (n = 292).

Multinomial logistic regression reporting unadjusted odds ratios; the outcome categories are low alcohol use (base outcome = 0-14 standard drinks in the last month), moderate alcohol use (15-50 standard drinks), high alcohol use (51-99 standard drinks), and very high alcohol use (≥100 standard drinks).
Reference category is less than monthly.
Alcohol use in the last month at baseline; categories are low alcohol use (reference category: 0-14 standard drinks in the last month), moderate alcohol use (15-50 standard drinks), high alcohol use (51-99 standard drinks), and very high alcohol use (≥100 standard drinks); factor entered as a discrete variable.
Measured at 30-month follow-up.
Refers to recency of use, comprises no use in the last 12 months (reference category), use in the last 12 months, and use in the last month; factor entered as discrete variable.
At least monthly attendance at the venue in the last 12 months, measured at 6-month follow-up.
Measured at 6-month follow-up.
Measured at baseline.
Factor entered as continuous variable.
Number of ecstasy/methamphetamine users known by face or name.
Refers to average fortnightly income after tax, measured at baseline; categories are $0-$250 per fortnight (reference category), $251-$560, $561-$1,000, $1,001-$1,300, and >$1,300; amounts listed are AUD$; factor entered as discrete variable.
Measured by a Hospital Anxiety and Depression Scale (HADS) score of ≥16.
p < .05. **p < .01. ***p < .001.
Table 3 presents a prediction model of patterns of alcohol use among ATS users after 30 months, reporting adjusted odds ratios. High baseline patterns of alcohol use predicted very high alcohol use at 30 months. Moreover, recency of ecstasy use at 30 months predicted moderate, high, and very high alcohol use. It is important to note that 30-month alcohol use was predicted by concurrent ecstasy use, independent of baseline alcohol use. There was no association between methamphetamine use and 30-month alcohol use patterns. Monthly nightclub attendance predicted very high alcohol use, while pub/bar attendance predicted moderate alcohol use. Of the other potential confounding variables, only sex was significant, with male ATS users having greater odds of being involved in high and very high patterns of alcohol use at 30 months.
Prediction Model of Alcohol Use Patterns Among Amphetamine-Type Stimulant Users After 30 Months of Follow-Up a (n = 292).

A prediction model using the generalized linear latent and mixed model (GLLAMM) procedure, reporting odds ratios for each predictor adjusted for all other variables in the model; the outcome categories are low alcohol use (base outcome = 0-14 standard drinks in the last month), moderate alcohol use (15-50 standard drinks), high alcohol use (51-99 standard drinks), and very high alcohol use (≥100 standard drinks).
Reference category is less than monthly.
Alcohol use in the last month at baseline; levels defined according to the same ranges of standard drinks used for the outcome variable; low alcohol use (0-14 standard drinks in the last month) is the reference category; factor entered as a discrete variable.
Measured at 30-month follow-up.
Refers to recency of use, comprises no use in the last 12 months (reference category), use in the last 12 months, and use in the last month; factor entered as a discrete variable.
At least monthly attendance at the venue in the last 12 months, measured at 6-month follow-up.
Measured at 6-month follow-up.
Measured at baseline.
Factor entered as continuous variable.
Number of ecstasy/methamphetamine users known by face or name.
Refers to average fortnightly income after tax, measured at baseline; categories are $0-$250 per fortnight (reference category), $251-$560, $561-$1,000, $1,001-$1,300, and >$1,300; amounts listed are AUD$; factor entered as a discrete variable.
Measured by a Hospital Anxiety and Depression Scale (HADS) score of ≥16.
p < .05. **p < .01.
Discussion
Our study did not find a longitudinal association between ATS and subsequent alcohol use after 30 months of follow-up, suggesting that ATS use does not lead to hazardous patterns of alcohol use in this Australian young adult population. However, hazardous patterns of alcohol consumption among ATS users at 30 months were associated with recent (last month) concurrent ecstasy use and frequent attendance at nightclubs, independent of baseline alcohol use and other potential confounding factors. Concurrent ecstasy use and frequent attendance at nightclubs both more than doubled the relative odds of hazardous patterns of alcohol consumption among ATS users at 30 months.
Our findings provide evidence of a concurrent association between ecstasy use and hazardous patterns of alcohol consumption, rather than a longitudinal association, controlling for potential confounding factors. The link between high-level alcohol consumption and concurrent ecstasy use suggests that the combined use of these substances may result in greater biological or subjective rewards than those derived from separate use. Combined ecstasy and alcohol use could reinforce the use of both drugs by enhancing the positive effects of either drug (e.g., prolonged feelings of euphoria) and by ameliorating unwanted/negative effects (e.g., sedative effect of alcohol; Boeri, Sterk, Bahora, & Elifson, 2008; Hernández-López et al., 2002). However, as there was no evidence of a longitudinal relationship between ecstasy and alcohol use, this suggests that long-term changes in users’ intrinsic reward processes are not necessarily responsible for the drug use patterns observed. Alternatively, ecstasy users may deliberately choose to use ecstasy in combination with alcohol to achieve a desired effect, such as an increased physical capacity to drink when using ecstasy. Previous research has emphasized the importance of acknowledging the active role that drug users may play in combining substances during drug-use episodes to enhance pleasure, extend or prolong the effects of a substance, and mitigate the negative effects of a substance (Hunt, Evans, Moloney, & Bailey, 2009).
In contrast, there was no association with concurrent methamphetamine use. However, concurrent and simultaneous patterns of methamphetamine and alcohol use have been observed in a number of other studies (see Bujarski et al., 2014; McKetin, Lubman, et al., 2014). The population prevalence of ecstasy use was higher than methamphetamine use at the time of recruitment for the NHSDU, resulting in a lower number of methamphetamine users in the study. Consequently, the lack of association between concurrent methamphetamine use and alcohol use could simply reflect low statistical power.
Young adults’ drug use behavior may also be influenced by their social environment. ATS users who frequently attended nightclubs (at least monthly) during the early study phases had increased odds of very high levels of alcohol use at 30 months, independent of baseline alcohol use and propensity for attending parties. It is already understood that attendance at licensed venues, especially pubs and bars, is linked with increased alcohol consumption among young adults (see Kypri, Paschall, Langley, Baxter, & Bourdeau, 2010). The strength of this association may be dependent not only on the availability of alcohol but also on aspects of the design and management of licensed venues (Miller, Holder, & Voas, 2009; Van Havere et al., 2011). This study aligns with recent Australian research, providing evidence that this dynamic is applicable to young adult ATS users in contemporary nightclub settings. McKetin, Chalmers, Sunderland, and Bright (2014) found that young adult ecstasy users who consumed stimulants on their last Saturday night out were 3 times more likely to binge drink compared with ecstasy-using peers who were not using stimulants that night. In addition, these stimulant-intoxicated young adults reported drinking excessively, consuming a median of 20 standard drinks during their night out (McKetin, Chalmers, et al., 2014). The independent association we have observed between nightclub attendance and hazardous alcohol use is longitudinal in nature, suggesting that regular attendance at these venues may promote long-term changes in behavior.
Some research suggests there are decreasing gender differences in young people’s alcohol and other drug use patterns (see Nolen-Hoeksema, 2004; Roche & Deehan, 2002). Our study provides mixed evidence on this question. Although our results showed that both female and male ATS users were engaging in hazardous patterns of alcohol use, there was evidence of substantially greater short- and long-term risk among males.
Implications
The association between hazardous levels of alcohol consumption and concurrent ecstasy use suggests that young adult ecstasy users may be an important target group for alcohol interventions, especially in light of the relatively high population prevalence of ecstasy use in this age group. In 2010, 9.9% and 6.8% of young adults aged 20 to 29 years had used ecstasy and methamphetamine in the last 12 months, respectively (Australian Institute of Health and Welfare [AIHW], 2011). In particular, the integration of ecstasy and alcohol harm reduction messages for this target group is a feasible objective. Furthermore, the association between nightclub attendance and hazardous alcohol use suggests that interventions should prioritize nightclub patrons rather than those attending other types of venues.
Our findings also raise the question of whether the seemingly synergistic use of alcohol and stimulants, particularly ecstasy, may cause greater short- and long-term harm than their separate use. Research suggests an association between combined ATS and alcohol use and risky behaviors, such as extreme levels of binge drinking (McKetin, Chalmers, et al., 2014), engaging in unsafe sex (Breen et al., 2006), and driving under the influence of alcohol or other drugs (Duff & Rowland, 2006; Matthews et al., 2009). However, further research is required to examine the nature and extent, at a population level, of adverse health and social outcomes associated with combined alcohol and ecstasy use.
Limitations
Some limitations should be noted. Our results could potentially be explained by confounding factors not examined in this study, particularly individual characteristics such as sensation seeking and aggression. Such predisposing factors may conceivably lead to both ecstasy and alcohol use. However, it is unclear whether they could explain the concurrent patterns of use we observed. Further research including these potential confounding factors is needed. In addition, for most of these young adults, their frequency of ecstasy use will likely decline or stabilize at low levels within a reasonably short time frame (Smirnov et al., 2013). The present findings suggest there will, to some extent, be a decrease in alcohol consumption alongside these changes in ecstasy use. A longer follow-up period is required to confirm whether this is the case. Furthermore, our findings suggest that drug use expectancies may play a role in the relationship between ecstasy use and hazardous patterns of alcohol use; however, our study does not directly measure this phenomenon. An assessment of alcohol and ATS use expectancies may help to elucidate our findings. In addition, while the screening response rate of the NHSDU (49.9%) was reasonable in comparison with response rates routinely obtained by mail-out surveys and drug use surveys (AIHW, 2011; Breen, Shakeshaft, Doran, Sanson-Fisher, & Mattick, 2010; Ryu, Couper, & Marans, 2006), bias may have resulted from non-response. Finally, not all ecstasy used in Australia comprises MDMA, and consequently, our findings are not necessarily specific to this drug.
Conclusion
Neither earlier life course ecstasy nor methamphetamine use predicted subsequent involvement in hazardous alcohol consumption, after 30 months of follow-up, in this sample of Australian young adults. However, there is evidence of a link between hazardous alcohol consumption and concurrent ecstasy use in this population. It is likely that some young adults may be using ecstasy and alcohol together to achieve certain subjective or behavioral outcomes. In addition, the association between very high levels of alcohol use and frequent nightclub attendance suggests that ecstasy users’ cultural activities may have become increasingly assimilated within a culture of binge alcohol use. Consequently, there may be a need for integrated harm reduction approaches addressing both alcohol and ATS use, as well as the context of this use.
Footnotes
Appendix
Sensitivity Analysis: Prediction Model of Alcohol Use Patterns After 30 Months of Follow-Up Among Amphetamine-Type Stimulant Users Who Were Using Ecstasy and/or Methamphetamine at Least Monthly in the Last 12 Months at Baseline a (n = 143).
| Adjusted Odds Ratios (95% Confidence Interval) |
|||
|---|---|---|---|
| Moderate alcohol use (n = 43) | High alcohol use (n = 31) | Very high alcohol use (n = 43) | |
| Baseline drug use | |||
| Monthly ecstasy use b | 0.59 [0.07, 4.56] | 1.26 [0.12, 13.41] | 3.77 [0.35, 40.39] |
| Monthly methamphetamine use b | 2.56 [0.48, 13.66] | 1.10 [0.16, 7.44] | 2.44 [0.39, 15.37] |
| Alcohol use c | 1.49 [0.71, 3.14] | 2.76 [1.16, 6.51]* | 4.14 [1.80, 9.50]** |
| Concurrent drug use d | |||
| Ecstasy (recent use) e | 3.74 [1.37, 10.20]* | 3.36 [1.10, 10.29]* | 4.79 [1.61, 14.23]** |
| Methamphetamine (recent use) e | 0.53 [0.19, 1.53] | 1.93 [0.64, 5.87] | 1.94 [0.64, 5.86] |
| Venue attendance (monthly) f | |||
| Nightclubs | 6.24 [1.53, 25.52]* | 2.64 [0.56, 12.40] | 1.21 [0.27, 5.53] |
| Pubs/bars | 1.49 [0.38, 6.57] | 0.99 [0.18, 5.40] | 0.84 [0.18, 4.01] |
| Leisure time activity g | |||
| Going to parties (weekly) | 0.33 [0.08, 1.36] | 1.45 [0.32, 6.61] | 0.73 [0.16, 3.31] |
| Individual characteristics h | |||
| Age i | 1.11 [0.61, 2.02] | 1.22 [0.64, 2.33] | 1.08 [0.57, 2.04] |
| Sex (male) | 5.43 [1.09, 26.99]* | 12.91 [2.14, 77.90]** | 8.46 [1.49, 48.16]* |
| Alcohol use < age 13 | 2.94 [0.34, 25.61] | 3.54 [0.34, 36.73] | 3.68 [0.37, 36.10] |
| Ecstasy social contacts (>30) j | 0.79 [0.14, 4.40] | 0.94 [0.14, 6.20] | 0.16 [0.03, 1.02] |
| Methamphetamine social contacts (>30) j | 0.52 [0.08, 3.06] | 0.42 [0.06, 2.97] | 0.29 [0.04, 2.18] |
| School suspension | 0.42 [0.09, 1.86] | 0.20 [0.03, 1.10] | 1.17 [0.24, 5.73] |
| Income k | 0.90 [0.49, 1.67] | 0.62 [0.32, 1.19] | 0.82 [0.43, 1.58] |
| Psychological distress l | 0.64 [0.09, 4.78] | 0.79 [0.73, 8.48] | 1.64 [0.18, 15.19] |
A prediction model using the generalized linear latent and mixed model (GLLAMM) procedure, reporting odds ratios for each predictor adjusted for all other variables in the model; the outcome categories are low alcohol use (base outcome = 0-14 standard drinks in the last month), moderate alcohol use (15-50 standard drinks), high alcohol use (51-99 standard drinks), and very high alcohol use (≥100 standard drinks).
Reference category is less than monthly.
Alcohol use in the last month at baseline; levels defined according to the same ranges of standard drinks used for the outcome variable; low alcohol use (0-14 standard drinks in the last month) is the reference category; factor entered as a discrete variable.
Measured at 30-month follow-up.
Refers to recency of use, comprises no use in the last 12 months (reference category), use in the last 12 months, and use in the last month; factor entered as a discrete variable.
At least monthly attendance at the venue in the last 12 months, measured at 6-month follow-up.
Measured at 6-month follow-up.
Measured at baseline.
Factor entered as continuous variable.
Number of ecstasy/methamphetamine users known by face or name.
Refers to average fortnightly income after tax, measured at baseline; categories are $0-$250 per fortnight (reference category), $251-$560, $561-$1,000, $1,001-$1,300, and >$1,300; amounts listed are AUD$; factor entered as a discrete variable.
Measured by a Hospital Anxiety and Depression Scale (HADS) score of ≥16.
p < .05. **p < .01.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported under the Australian Research Council’s Linkage Projects funding scheme [Project LP0776879].