
Abstract
The measurement of religiosity in current health-related literature is mostly based on the traditional Christian belief system. It has been argued that such a measurement approach may misrepresent the true degree of religiosity in Taiwanese people. In this study, religiosity was measured in two ways: self-reported religion type and a qualitatively derived index of religious piety based on principles as suggested by Gries, Su, and Schak to be used in the Taiwanese context. Their effects on dissociation, paranormal belief, and quality of life were juxtaposed for comparison. In addition, the beneficial effect of religious piety was examined in the framework of McClenon’s ritual healing theory. A total of 266 healthy older adults across Taiwan were interviewed by four trained assistants over a 4-month period. Factor scores were used to represent the dissociative tendencies (depersonalization/derealization, forgetfulness, amnesia, and psychological absorption) and paranormal belief facets (precognition, psi power, other forms of life, traditional religious belief, superstition, and telepathy). The results showed that older people of high religious piety display better quality of life profiles than their counterparts in the low religious piety group. The effects of self-reported religion type were mainly seen with paranormal beliefs compatible with their religious beliefs, whereas the effects of religious piety were more pronounced in relation to quality of life than dissociation and paranormal belief. The beneficial advantage of dissociation hypothesized by ritual healing theory did not receive empirical support in the nonclinical sample of this study.
Introduction
Psychologists have long been interested in the effects of religion on a wide range of health-related psychosocial variables. William James (1842-1910) is regarded by most psychologists as the first pioneer of the scientific study of religion. He distinguished between institutionalized religion and personal religion as two distinctly different constructs of religiosity. The former refers to the doctrines and beliefs of a religious organization, whereas the latter refers to the mystical experiences one has as a result of accepting the doctrines or beliefs (James, 1987). He took a pragmatic attitude toward the efficacy of religiosity: If an individual believes in and performs religious activities, and those actions happen to work, then that practice appears the proper choice for the individual. However, if the processes of religion have little efficacy, then there is no rationality for continuing the practice. James’s view of religiosity was later echoed by Gordon Allport (1897-1967), who was largely credited for the creation of the terms intrinsic religion and extrinsic religion (Allport & Ross, 1967). Intrinsic religion refers to a genuine, heartfelt devout faith, whereas extrinsic religion refers to a more utilitarian use of religion as a means to an end, such as church attendance to gain social status. Later on, social psychologist Daniel Batson (1943-) added a third orientation to religion which he called quest, an open-ended search for meaning. Batson, Schoenrade, and Ventis (1993) created an instrument called Religious Life Inventory in which intrinsic religion, extrinsic religion, and quest formed the three dimensions about religion. It has since provided a popular conceptual framework for the scientific study of religion in the Western world.
In the current health-related literature, the roles of religiosity in relation to mental health have often been shown as positive in both clinical and nonclinical literature. However, studies do not always agree on its positive role (see Pargament, 2002, for an excellent summary). In particular, religiosity was found to be associated with some negative psychological traits such as authoritarianism, suggestibility, dependence, dogmatism and rigidity (see Gartner, 1996, for a review), and other types of undesirable phenomenon such as child abuse and neglect, intergroup conflict and violence, and false perceptions of control (see Paloutzian & Kirkpatrick, 1995, for a review of earlier studies). However, by and large, studies published in health-related disciplines generally show positive association between religiosity and overall health. Among the important findings for those who are actively involved in religious activities are lower rates in mortality, coronary disease, emphysema, cirrhosis, suicide, and high blood pressure (Hilton, Fellingham, & Lyon, 2002; Seeman, Dubin, & Seeman, 2003); better positive health habits (McCullough & Willoughby, 2009); fewer depressive symptoms and better cognitive function (Koenig, George, & Titus, 2004); reduced level of pain in cancer patients (Holt et al., 2009); and slower disease progression in people with HIV (Ironson, Stuetzle, & Fletcher, 2006).
Myriad measures for measuring religiosity have been constructed and used extensively by health researchers using scientific methods of inquiry (see Hill & Pargament, 2008, for a review). In a literature review of medical research from 1990 to 2010 using PubMed alone, by limiting the search to articles published in the top quarter of the journals according to the Thomson Reuters Web of Science (formerly ISI Web of Knowledge) journals citation index 2010, Bonelli and Koenig (2013) found that 72.1% associated less mental disorder with higher religious involvement. Most of the studies in the scientific study of religion use self-reported type of instruments for the measurement of religiosity. However, there is evidence that its real effect on certain behaviors may be misrepresented because survey respondents may interpret the meaning of survey items tapping religiosity differently, give socially desirable answers, or be affected by dispositional factors such as conscientiousness or embarrassment (Hout & Greeley, 1998). This phenomenon should warrant even more concern in the Taiwanese context because there are significant differences in ways Taiwanese and Westerners express their religious beliefs as commonly observed in election campaigns: Americans in particular are more likely to participate in routine religious activities taking place outside their homes and more outspoken about their religious beliefs. In contrast, most Taiwanese people carry out their routine religious activities at home, which are often perceived not as religious but as an unremarkable component of their culture. They also tend to be more reserved in the expression of their religious views. Moreover, a recent study by Gries, Su, and Schak (2012) also revealed that the traditional zero-sum approach (religious activities classified exclusively into one specific religion type) to measuring religiosity as found in literature to date has many problems when applied in a polytheistic society like Taiwan.
As Taiwan has arguably joined the ranks of developed nations in terms of technology and people’s general well-being, it has also begun to experience problems associated with these countries. In particular, Taiwan is seeing an ever-increasing proportion of elderly people in its population fabric. Defining those who are 65 years of age and above as the elderly, local English media China Post, citing data from Taiwan’s Bureau of Health Promotion, reported that Taiwan officially became an aging society in 1993 when the proportion of the elderly reached 7% of the entire population. Moreover, based on the current trend of growth, the Council for Economic Planning and Development predicted that the country will become an “aged population” by 2017 when the proportion reaches 14%, and further develop into a “super-aged population” by 2025 when more than 20% of the population will be elderly (http://www.chinapost.com.tw/taiwan/national/national-news/2011/07/12/309550/Taiwans-future.htm). As Taiwan’s population rapidly ages, concern about quality of life in older people heightens because the majority can now expect to live a long life. Public concern over quality of life increases with the improvement of medical technologies and therapeutic approaches just for the sake of prolonging life. However, no one wishes to live long if he or she is no longer able to enjoy life. Toward this end, an increasing number of health researchers are calling for religion to be integrated into clinical practices, especially in older populations (Bush et al., 2012; Weaver, Flannelly, Strock, Krause, & Flannelly, 2005). Therefore, this study intends to examine the effect of religion on the quality of life in Taiwanese older people by using a construct called religious piety applicable to the local settings based on a positive-sum approach (allowing religious activities to be cross-referenced among different religion types) for measuring religiosity as recommended by Gries et al. (2012). More importantly, the construct of religiosity will be related to the quality of life through cognitive dissociation and paranormal belief as two potential mediators under the framework of the “ritual healing theory” proposed by McClenon (2005). Cognitive dissociation, paranormal belief, and ritual healing theory are briefly reviewed in the following section before four hypotheses of investigation are presented.
Dissociation
The term dissociation is commonly used to cover a range of psychological processes in clinical studies. It is broadly described as a failure to integrate memories and perceptions that are normally associated together simultaneously. The most salient characteristic of all dissociative symptoms is a detachment from reality through activation of altered states of consciousness in reaction to overwhelming internal or external stimulation. While dissociation is usually considered as a transient state by clinical practitioners (Kruger & Mace, 2002), it may also be treated as a long-lasting trait (Nardo et al., 2013). The latter would imply that some people may be dissociative over a prolonged period of time as reported in people displaying eating disorders (Hallings-Pott, Waller, Watson, & Scragg, 2005).
Dissociation as a trait has largely been reported in studies of trauma victims. However, not all dissociative traits are the result of trauma (Butler, 2006). Conceptualizing dissociation as a trait means to display this construct on a continuum. The major characteristic of all dissociative phenomena involves a detachment from reality. At the pathological end of the continuum, dissociation severely limits perceptions and impairs ability to connect with others to such a degree that they are unable to care for themselves. At the nonpathological end of the continuum, dissociation simply refers to the nonpathological altered states of consciousness seen in common events such as daydreaming while driving a car. In fact, some researchers even suggest that nonpathological dissociation can be thought of as a normally distributed trait in the general population that is approximately 50% heritable (Jang, Paris, Zweig-Frank, & Livesley, 1998). In a comprehensive review, some researchers found that nonpathological dissociation is characterized by proneness to fantasy, suggestibility, and cognitive failures (Giesbrecht, Lynn, Lilienfeld, & Merckelbach, 2008). When viewed from a nonpathological perspective, a dissociative moment is a state of both sleep and waking simultaneously. Most people would have dissociated without recognizing it, such as one may have walked a number of streets and cannot recall seeing anything he or she walks past. It is also viewed as a coping strategy in the sense of defense mechanism in seeking to minimize conflict or tolerate stress (Weiten & Lloyd, 2008).
Paranormal Belief
It is reasonable to view a religious conviction from the perspective of a more encompassing construct called paranormal belief. Paranormal, by definition, conveys beliefs that are beyond analytical thinking of human capacity and thus transcending the laws of nature, such as a belief in reincarnation or the existence of God, gods, or soul. Contrary to common belief, paranormal belief and analytical thinking ability are not necessarily incompatible. In fact, scientific and paranormal thinking have been observed to coexist simultaneously both in children (Nemeroff & Rozin, 2000) and in adults (McClenon, 1993). A relatively recent theory proposed by Sun, Slusarz, and Terry (2005) may be able to explain this phenomenon: People have two independent modes of processing information—intuitive and analytical reasoning. These two modes of thinking rely on different databases and have different rules of operation. The idea of two coexisting cognitive systems in the human brain is consistent with the observation that believers of religion and magic often believe in two realities, a natural reality and a mystical reality. Under this theory, Epstein, Pacini, Denes-Raj, and Heier (1996) reported that people with high intuitive thinking disposition tend to display higher paranormal belief (positive correlation), whereas people with higher analytical thinking disposition tend to display lower paranormal belief (negative correlation). It is worth pointing out that the positive correlation was observed to be much stronger than the negative correlation.
Albeit the psychological functions of paranormal belief have been extensively documented with respect to cognitive tendency of developing schizophrenia (Genovese, 2005; Goulding, 2005; Hergovich, Schott, & Arendasy, 2008; Williams & Irwin, 1991), reality testing (Irwin, 2004), control over life (Irwin, 2000; Watt, Watson, & Wilson, 2007), and false sense of causation (Wiseman & Watt, 2006), there has not been as much empirical research aimed at uncovering the underlying relationships between paranormal belief and cognitive dissociation. In attempts to account for the positive effects of religion on human survival, McClenon (2005) recently postulated in his ritual healing theory that the mental processes of dissociation provided the missing link for explaining how the beneficial effects of paranormal beliefs came about. This study intends to contribute to the current literature by applying the ritual healing theory to the formulation of hypotheses concerning the relationships among dissociation, paranormal belief, religious piety, and quality of life for older people.
Ritual Healing Theory
Based on research findings in areas of social psychology, human genetics, and evolutionary psychology, McClenon (2005) proposed a theory which he called “ritual healing theory.” It postulates that the capacity for paranormal perceptions through dissociative abilities has a physiological basis. When people encounter an anomalous experience, the ability to dissociate themselves from the unpleasant side of this experience is beneficial for one’s continued survival. The individuals who successfully overcome cognitive difficulties by using dissociative tendencies may pass on dissociation genotypes to their offspring. Over time, dissociation develops into a unique human ability to psychologically manipulate reality through connecting or disconnecting mental imageries. Commonly encountered experiences linked to dissociation may include episodes of seeing ghosts/spirits/gods, conversing with the dead, objects moving without reason, or out of body experiences. These experiences, when accumulated, generate religious/paranormal beliefs in spiritual forces, souls, and life after death. According to McClenon, people with dissociative capacities have survival advantages because they are better able to cope with trauma or unpleasant experiences. In retrospect, the view of a genetic component to religiosity was supported by twins-study research which claimed that about 50% of the observed variation in measures of religious interests, attitudes, and values is genetically determined (Waller, Kojetin, Bouchard, Lykken, & Tellegen, 1990).
Within a religious context, dissociation is often facilitated by religious rituals. The ritualistic behavior in religious activities allows participants to enter either an overt or covert dissociative mental state. In fact, Price and Snow (1998) believed that all religious services are characterized by dissociation in one form or another. Schumaker (1995) suggested that psychologically manipulating reality to fit existing personal and cultural backgrounds is essential for one’s continued mental health. When viewed from this perspective, paranormal beliefs can be considered as imagery instruments for facilitating the process of dissociation. It should be noted that the dissociation as conceptualized in ritual healing theory does not in any way refute the authenticity of the religious or paranormal claims. Instead, it argues from an evolutional perspective that paranormal beliefs have some universal features that provide greater benefits for survival to those with greater dissociative capacities (McClenon, 2005), and may thus lead to better quality of life.
Hypotheses
This study was designed to assess the effect of religious piety on quality of life in the population of older people in association with its role as a potential mediator in the relationships among cognitive dissociation, paranormal belief, and older people’s quality of life. Specifically, four research hypotheses examined in this study are stated as follows:
Method
Recruitment of Respondents
Respondents were recruited from community leisure places where older people congregate as well as sites where routine religious activities are held across Taiwan. The snowball sampling scheme was used in which help from acquaintances was solicited through networking in the early phase. To be eligible to participate in this study, three conditions were required: older than 65 years of age, capable of making unaided physical movements and free from recognizable psychiatric symptoms, and must identify with one of the four religion types (Folk religion, Buddhism, Christianity, and Atheism). These conditions were set so that the potential confounding of the effects under investigation might be minimal. The target for the number of participants was initially set to be 160. At a Type I Error rate of 0.05, according to the statistical power table provided by Cohen (1988), such a sample size would yield sufficient statistical power (97%) for detecting a significant correlation under medium or greater effect size (r > .3). However, to make provisions for potential bias associated with snowball sampling, the target sample size was increased to 250 in the sampling plan. Several randomly recruited participants recommended their friends fitting our criterion for inclusion. The participation was completely voluntary.
Data were obtained in one-on-one personal interview settings. The interview format was chosen over the more convenient alternative of self-report questionnaire because the nature of religious piety, dissociation, and paranormal belief would require a two-way interaction process in which the interviewer and the interviewee might need to exchange questions for clarifying doubts. The interview consisted of four parts: background information (age, gender, religion type, education level, disposable monthly income, and assessment of religious piety), quality of life, dissociation, and paranormal belief. The entire interview process took approximately 90 min. A total of 350 older people were approached who met our requirements for inclusion into this study, of whom 266 completed the whole interview process during a 3-month span, roughly 5% of whom did not complete the interview on the first occasion and had to come back to complete. There were 129 females and 137 males. The average age was 72.41 with a standard deviation of 7.53. One hundred thirty (48.87%) of the sampled respondents had primary school education or less and 37 (13.91%) completed education above college level. The respondents’ self-identified religious affiliations were as follows: Buddhism (n = 45), Taoism/Folk religion (n = 173), Christianity/Catholics (n = 38), and Atheism (n = 10).
Instrumentation
Religious piety
Instead of commonly seen self-report types of methods for assessing the degree of religiousness that yield subscale scores for different dimensions of religiosity, a qualitatively derived three-level index of religious piety was used based on the contents revealed in the first part of the interview with respondents. The question “Do you identify yourself as a follower of any of the following four religion types: Buddhism, Christianity/Catholics, Folk religion, Atheism?” was asked first. The respondents were then presented with a set of visual prompts depicting religious beliefs and rituals in the context of their self-declared religion type and asked what they think of these beliefs and whether they participated in these activities. Following the priming stage, the respondents were directed to rate five statements on 1- to 5-point Likert-type scale: “Importance of your religious faith in your life,” “Observance of the religious rituals demanded of you by your religion to the best you can,” “Your religion influences your daily life,” “You seek to share your religious belief with other people,” and “Your religious belief influences you in times of making important decisions.” The responses were averaged to provide an indicator for the degree of their religious piety. Those with an average greater than four (n = 64) were qualitatively identified as the high religious piety group, whereas those with an average lower than three were classified into low religious piety group (n = 44). The rest were classified into the medium religious piety group. It should be noted that adjusting the visual prompts depicting prayer, meditation, worship, financial donation, and other common religious practices in relation to the religious context of the participant’s self-claimed religion type complies in principle with the “positive-sum” approach Gries et al. (2012) suggested for use in Taiwan in differentiation from the more commonly used “zero-sum” approaches.
Dissociation
The method of measuring dissociative tendencies in this study was Bernstein and Putnam’s Dissociative Experiences Scale (DES-II; Carlson & Putnam, 1993). The DES-II is a clinically developed scale consisting of 28 items developed from interviews with clinicians working in the treatment of dissociative disorders related to memory, identity, awareness, and cognition. The dissociative experiences covered in DES-II are labeled as amnesia, depersonalization, derealization, absorption, and imaginative involvement. Despite its clinical nature, DES-II may be relatively easy to administer by one familiar with basic psychological testing knowledge after some training. The participants’ responses were recorded with reference to the frequency of dissociative experiences that might have occurred to them in terms of percentages of time (0%-100% by 10 s) in which they experienced a certain dissociative phenomenon.
When the principal component factor analysis was applied to the 28 DES-II items, four major factors were identified by the scree plot of the eigenvalues, which accounted for more than 59.90% of the total variance. Both orthogonal and nonorthogonal factor structures after rotation were examined. The factor structure after orthogonal rotation yielded readily meaningful interpretation of the resulting factors, which were thus retained for analysis in this study. The first factor had high loadings on items (r > .70 on Items 11, 12, 13) addressing depersonalization (not recognizing oneself in the mirror, feeling that other people and objects are not real, feeling that their body does not belong to them) and moderately high loadings (r = .65 on Item 28) addressing derealization (seeing the world through a fog). This factor was identified as the “depersonalization/derealization” aspect of the dissociation construct. The second factor had high loadings on items addressing general forgetfulness (r > .50 on Items 1-9) that may be observed in most people, such as not remembering what happened during a trip or what clothes they put on. This factor was identified as “forgetfulness.” The first two factors accounted for roughly equal amount of variance (17.58% and 16.93%, respectively). The third factor had moderately high positive loadings on items addressing the important events of their life (r > .60 on Items 24-26) and moderately high loadings (r > .50 on Items 9 and 10), which are commonly associated with serious memory loss. This factor accounted for 13.32% of the total variance and was labeled as amnesia. The last factor had high loadings (r > .65 on Items 14 and 19) addressing daydreaming (reliving past events vividly as if they are occurring now) and selective unconsciousness (ignoring pain), and moderately high loadings (r > .50 on Items 20, 22, 23) addressing cognitive blanking (staring off into space and thinking of nothing) and disengagement from true self (acting as two different people in different situations and do things with ease with things they may find difficult other times). The last factor is reminiscent of the construct suggested by Tellegen and Atkinson (1974) known as “psychological absorption.” This factor accounted for 11.79% of the total variance in the current sample. Despite the nonclinical nature of our data, the pattern of the four factors as discovered in this study was amazingly similar to those reported by Carlson, Putnam, Ross, and Anderson (1991) and Schwart and Frischholz (1991). Factor scores were thus used to represent the four aspects of the dissociation construct: depersonalization/derealization, general forgetfulness, amnesia, and psychological absorption.
Quality of life
The quality of life of older people was assessed by a health-related questionnaire developed by World Health Organization (WHO) with the aim of providing cross-culturally acceptable measures for assessing quality of life in the general population (WHO, 1995). This measure is commonly known as the World Health Organization Quality of Life (WHOQOL) Questionnaire. The original WHOQOL comprised 96 items measuring 24 facets organized into six domains. Each facet contained four items, plus four Facet-G items measuring overall quality of life and general health. Therefore, the WHOQOL questionnaire was also commonly referred to as WHOQOL-100. The six domains were as follows: physical, psychological, level of independence, social relationships, environment, and spiritual/religion/personal beliefs. One item from each of the 24 facets, one overall quality of life item, and one general health item were chosen to form a short version commonly known as WHOQOL-BREF for easy administration and practical uses. Four of the original six domains were confirmed in the short version (WHO, 1998). They were physical, psychological, social, and environment. The WHOQOL-BREF has 26 items expressed on a 5-point Likert-type scale and has been proven to have strong cross-cultural applicability and good psychometric qualities (Li, Kay, & Nokkaew, 2009). The Chinese version WHOQOL-BREF questionnaire was culturally modified by Yao, Wang, and Chung (2007) by adding two additional items deemed meaningful for use in Taiwan. These two items are as follows: “Do you feel respected by others?” and “Are you usually able to get the things you like to eat?” The WHOQOL-BREF Taiwan has 28 items and the construct validity of the aforementioned four-domain structure as compared with the original WHOQOL-BREF was subsequently ascertained and thus was chosen as the instrument for measuring the quality of life in this study.
Paranormal belief
Survey instruments for measuring paranormal beliefs abound in literature. However, the most widely cited instrument may arguably be said to be the Revised Paranormal Belief Scale (RPBS) as developed by Tobacyk (2004) comprising seven supposedly orthogonal factors: traditional religious belief, psi belief, witchcraft, superstition, spiritualism, extraordinary life forms, and precognition. The applications of this instrument or its earlier version and reports of its psychometric properties appeared in many reputable journals across multiple disciplines (i.e., Aarnio & Lindeman, 2007; Watt et al., 2007). In a search of studies published between 1993 and 1999, Goulding and Parker (2001) reported a total of 43 different instruments claiming to measure paranormal beliefs and experiences, with Tobacyk’s Paranormal Belief Scale being the most widely used instrument. In this study, the Chinese version of Tobacyk’s RPBS as adapted by Shiah, Tam, Wu, and Chang (2010) for local application was used as a basis for measuring paranormal beliefs. The adaptation refers to modifications made to two items. Item 4 “Black cats can bring bad luck” was changed to “Voices of crow can bring bad luck,” and Item 18 “The number 13 is unlucky” was changed to “The number 4 is unlucky.” The Chinese RPBS contains 26 items expressed on a 7-point Likert-type scale with 1 indicating the least degree of belief and 7 indicating the strongest. One item was reversely scored (Item 23).
No summative subscale scores as defined in the original RPBS were used in this study. Instead, factor scores were used to represent the latent constructs underlying RPBS. When the principal component factor analysis was applied to the 26 RPBS items, six factors with eigenvalues greater than one were retained accounting for 61.33% of the total variance. Both orthogonal and nonorthogonal factor structures after rotation were examined. The factor structure after orthogonal rotation yielded distinctly clear interpretation of the resulting factors, which were thus retained for later analysis. These six factors were identified as precognition (Items 7, 14, 21, 26), psi power (2, 9, 16), sorcery/other forms of life (3, 8, 10, 13, 20), traditional religious belief (1, 15, 22), superstition (4, 6, 11, 18), and telepathy (23). Despite all effort being made to ensure that the respondents answer all questions during the interview, one person, however, provided incomplete data in this section. This individual’s responses to questions in other sections were nevertheless complete.
Statistical Analysis
The principal component factor analysis was used to derive indicators for dissociative tendencies and paranormal beliefs. The decision to use factor scores as the latent variables for the dissociative tendencies and paranormal beliefs was predicated on the knowledge that neither constructs are well defined and universally accepted from one study to another found in literature. In the procedures of factor analysis, a factor underlying a postulated latent construct is separated from its associated measurement error, and thus, the resulting factor score may be considered a better measure of the putative latent construct than any directly calculated subscale scores. Because the presence of variance heterogeneity was evident on some of our criterion measures, nonparametric alternative statistical procedures were used in place of their parametric counterparts where applicable. The effect of religious piety on paranormal beliefs, dissociative tendencies, and quality of life were assessed by contrasting the high religious piety group to the low religious piety group using Wilcoxon’s rank-sum test, which is the nonparametric alternative to the more familiar two-group independent t test. The effect of self-reported religion type and three-level religious piety on paranormal belief, dissociative tendency, and quality of life were subjected to Kruskal–Wallis chi-square approximation test. The Kruskal–Wallis test is the nonparametric equivalent to the one-way ANOVA. Both forward and backward stepwise regression procedures were used to examine whether dissociative tendencies were predictive of paranormal beliefs. Finally, the tenability of the hypothesis regarding the advantage of dissociation according to the ritual healing theory was subjected to the tests of zero-order Spearman rank correlations between quality of life domains and dissociative tendencies for the religiously pious and nonreligiously pious separately.
Results
The dissociative tendencies and paranormal beliefs as derived from factor analysis were normally distributed with a mean of 0 and a standard deviation of 1. The quality of life indicators (physical well-being, mental health, social life, and environment satisfaction) were distributed with negative skewness ranging from −.50 to −.73. This, together with all four means (ranging from 3.42 to 3.66) being higher than the midpoint 3 on the measurement scale, indicated that Taiwanese older people were more often than not satisfied with their quality of life. The standard deviations ranged from .47 to .54.
Effects of Religious Piety
The means and standard deviations of paranormal belief, dissociative tendencies, and quality of life variables were reported separately for high religious piety group (n = 64) and low religious piety group (n = 44) in Table 1, together with the z approximations for testing the differences between these two groups. As seen, the high religious piety group scored significantly higher than the low religious piety group in only the traditional religious belief domain of the putative paranormal belief construct (z = 5.54, p < .000). This should come as no surprise as more religiously pious people certainly hold stronger conviction about the existence of God/gods and the existence of paradise and hell. Religious piety did not seem to affect dissociation in any of the four dissociative tendencies. With regard to quality of life, religious piety was not significantly associated with physical well-being, marginally associated with environment satisfaction (z = 1.34, p < .0898), and positively associated with social life (z = 1.65, p < .0490) and mental health (z = 3.02, p < .0013).
Descriptive Information and Tests of Difference Between High and Low Religious Piety Groups.

z value was approximated by using Wilcoxon rank-sum statistic for testing the difference between two independent group means.
Effects of Religious Piety and Religion Type
In this section, 158 respondents whose level of religious piety fell between high and low were also included in the analysis. There were three levels of religious piety (Piety): high, medium, and low. The chi-square values and their associated p values from the Kruskal–Wallis tests of differences due to Piety were reported in juxtaposition with those due to the four self-reported religion types (Type) in Table 2. In terms of paranormal belief, Piety was observed to have a large effect on the traditional religious belief (χ2 = 38.30, p < .0000) and a marginal effect on precognition (p < .0534) and psi (p < .0925). Further examination of the means at the high, medium, and low levels of Piety revealed that the disparate pattern of traditional religious belief means was indeed in the expected direction (.48, .00, and −.72, respectively). When the tendencies of dissociation were concerned, Piety was significantly related to depersonalization/derealization (p < .0473) and amnesia (p < .0445). A positive relationship was observed with depersonalization/derealization with the means .06, .02, and −.15 at high, medium, and low levels of Piety, respectively. The Piety’s relationship with amnesia is less interpretable, in that the highest mean (.08) was associated with the medium level when contrasted with high and low levels of Piety (−.08 and −.15, respectively). With respect to quality of life indicators, Piety had a strong positive effect on mental health (means from high to low as 3.57, 3.41, and 3.22, respectively, p < .0036) and a marginally positive effect on environment satisfaction (means from high to low as 3.77, 3.63, and 3.62, respectively, p < .0575).
Kruskal–Wallis Tests of Religious Piety and Religion Type Effects (n = 266).

Type showed strong effects on paranormal belief with respect to precognition (p < .0026), traditional religious belief (p < .0000), and telepathy (p < .0051), and marginal effect with respect to psi (p < .0506). The examination of the means at each level of Type revealed that the patterns of paranormal belief means were also in the expected direction: Christians had the largest mean (.53) on traditional religious belief (belief in existence of God and heaven/hell), followed by Buddhists (.14), Folk-religion followers (−.10), and Atheists (−.86). The means of precognition for Buddhists, Christians, Folk-religion followers, and people of no religion were .19, −.44, .08, and −.59, respectively. The means of telepathy were .20, .45, −.14, and −.15, respectively. When the tendencies of dissociation were concerned, Type was found to be strongly related to amnesia (p < .0016) with the largest mean associated with Christians (.53), followed by Buddhists (.18), people of no religion (.06), and Folk-religion followers (−.17). No differences in any of the four quality of life facets could be attributed to Type.
When placed in juxtaposition as shown in Table 2, it is easy to see that Type had stronger effects on paranormal beliefs than Piety, whereas Piety had more impact on the quality of life. These results were consistent with the research hypothesis in this study. The influences of Piety and Type on dissociative tendencies appeared to be more complicated in that they were not related to the nonpathological aspect of dissociation as represented by forgetfulness and psychological absorption. Both Piety and Type were related to the pathological aspect of dissociation as represented by amnesia, and the strength of such an association was much stronger with Type than Piety. Post hoc analysis revealed that the differences in amnesia among the four religion types were mainly attributed to the mean difference between Christians and Folk-religion followers (.528 and −.166, respectively). The depersonalization/derealization aspect of pathological dissociation was only significantly but weakly related to Piety with greater complexity. While Piety was positively related to depersonalization/derealization, its association with amnesia was not. Instead, it was the medium-level Piety that produced the highest mean in amnesia (.077), as compared with the means of the high and low levels (−.083 and −.155, respectively).
Paranormal Belief and Dissociation
The standardized regression coefficients (β coefficients) from multiple regression models of predicting each dimension of paranormal belief from four dissociative tendencies were summarized in Table 3. As seen, some of the paranormal beliefs were indeed significantly related to some dissociative tendencies, but none of which was predictive of all paranormal beliefs. The effect sizes of the predictable relationships were judged to be small as indicated by small R2 values with the largest value of .0716 falling on telepathy, which was significantly and positively related to forgetfulness (β = .196, p < .005), amnesia (β = .122, p < .05), and psychological absorption (β = .131, p < .05). Belief in psi was positively related to amnesia (β = .189, p < .005) and depersonalization/derealization (β = .150, p < .05). Belief in the existence of other forms of life was positively associated with amnesia (β = .170, p < .01), but negatively associated with forgetfulness (β = −.120, p < .05). Superstition was found to be predictable from depersonalization/derealization (β = .149, p < .05). Neither precognition nor traditional religious belief could be attributed to any of the four dissociative tendencies.
Standardized Regression Coefficients for Predicting Paranormal Belief From Dissociative Tendencies (N = 266).

p < .05. **p < .01. ***p < .005.
Beneficial Effects of Dissociation by Religious Piety
The tenability of the beneficial effects of dissociation on older people’s quality of life derived from McClenon’s (2005) ritual healing theory was examined by contrasting the zero-order correlations between the four dissociative tendencies and four aspects of quality of life separately by separating the religiously pious from the rest. If dissociation had any beneficial effect at all for the religiously pious, the zero-order correlations observed in this group should be positive in contrast to those observed in the other group. The Spearman rank correlations were summarized in Table 4. All the significant correlations were in the negative range. The largest correlation (r = −.27, p < .05) was found in the religiously pious group between forgetfulness and environment satisfaction. The same correlation was also negative in the other group (r = −.14, p < .05). Therefore, it was fair to conclude that the beneficial effects of dissociation for the religiously pious older people were not empirically supported in the current sample.
Zero-Order Spearman Rank Correlations of Dissociative Tendencies With QOL: Contrasting High Religious Piety People (n = 64) With the Rest (n = 202).
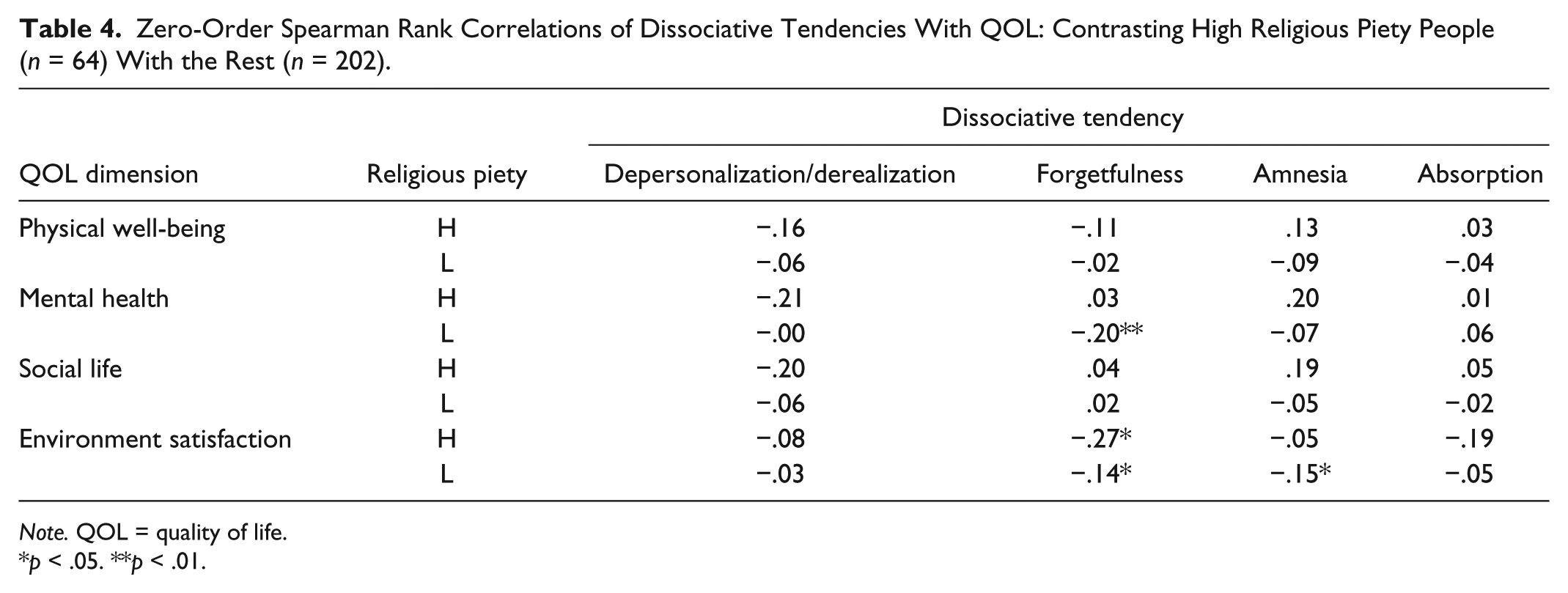
Note. QOL = quality of life.
p < .05. **p < .01.
Conclusion
When taking into consideration Gries et al.’s (2012) recommendation that a positive-sum approach for measuring religiosity be used in the Taiwanese context instead of the commonly used zero-sum approach in medical research, the first two hypotheses regarding the relationship between religiosity and quality of life were confirmed. The effects of the qualitatively derived index of religious piety were juxtaposed with those of the self-reported religion type on Taiwanese older people’s quality of life. The results revealed that religious piety had more influence on the quality of life in our respondents than religion type, especially in terms of mental health. While self-reported religion type did display significant differences in paranormal belief, they failed to account for the differences in dissociation and quality of life and the importance of religion type changed from one paranormal belief to another. In contrast, the finding of a clear and unambiguous positive relationship between religious piety and quality of life, especially in terms of mental health, is consistent with Bonelli and Koenig’s (2013) review of western medical research literature in which religiosity was mostly represented by religious attendance, sacraments, and rituals. Indeed, the fact that religious piety, as defined in this study, also produced compatible results as reported in an earlier local study on the relationship between religion and personality (Chou & Chen, 2005) in which religious piety was represented by “faith type” measured by “love of God” and “love of man” suggests that the effect of religiosity, if defined with cultural sensitivity, is robust and universal.
With regard to the third hypothesis, the results of this study were consistent with earlier studies that revealed a somewhat strong relationship between specific facets of dissociation and different types of paranormal belief (Irwin, 2004; Wolfradt, 1997). Moreover, the pattern of differences in paranormal beliefs was found to be compatible with religion type as predicted in the second hypothesis. Despite the similarities, the psychopathology of dissociation (depersonalization/derealization and amnesia) appeared less clear in the current study. Certain types of paranormal beliefs have been linked to undesirable personality traits, such as high scores in superstition relating to a belief in fate and lack of control (Watt et al., 2007; Wiseman & Watt, 2006) and low scores in psi belief (a person’s thought can impact the movement of a physical object) enhanced the level of depersonalization/derealization (Irwin, 2000). All of these earlier studies used young adults such as college students as their subjects. This study used older people and found that depersonalization/derealization appeared to influence their psi and superstitious beliefs in the same way. Moreover, amnesia, a form of pathological dissociation, tended to influence paranormal beliefs in psi, other forms of life, and telepathy in the same way. The phenomenon that medium level of religious piety was linked to highest level of amnesia in contrast to its positive linear relationship with depersonalization/derealization may suggest that what’s considered as pathological dissociative tendencies in fact play different roles in relation to their level of religious piety. Further scientific inquiry into this discrepancy may lead to important discoveries.
The biggest surprise was found with the last hypothesis. The beneficial effects of dissociation on quality of life in older people were not empirically supported in this study, neither for the religiously pious nor for the religiously not so pious. The role of dissociation in ritual healing theory in effect portrays psychosis and spirituality in the form of religious beliefs as a continuum with spiritual experiences on the positive and healthy side of this continuum (Clarke, 2010). In this paradigm, religious beliefs are derived from dissociative processes that protect believers from potentially harmful consequences created by exposure to unpleasant realities. The implied connection between religiosity and dissociation would lead researchers to believe that dissociation is beneficial for the elderly who are truly religious, but not so or could even be pathological for others because the beliefs formed by those outside the realm of a proper religion may very likely deviate from acceptable social norms. An essential element in the paradigm overlooked in this study could be the “exposure to unpleasant realities.” Only a very small percentage (<10%) of our sample spoke of unpleasant experiences in their past, and they were all healthy at the time of interview. For the ritual healing theory to demonstrate its usefulness, the subjects may have to be experiencing some sort of physical or mental distress for the “rituals” to take effect. For instance, Hewson, Rowold, Sichler, and Walter (2014) did an experiment with a 6-hr healing ceremony given to 25 adults with various diseases. Health data were collected at three time points: 4 weeks before ceremony, 2 days before ceremony, and 4 weeks after ceremony. Hewson et al. concluded that participation in the ceremony significantly improved the subjects’ mental, physical, and emotional quality of life. In another research, a North American community survey was given to 965 African American adults with schizotypal experiences and other psychological symptoms. McClenon (2012) successfully confirmed hypotheses derived from the ritual healing theory and suggested that religion-based cognitive behavioral therapy be used for distressed people. The discrepancy observed between this current study and its clinical counterparts point to the need for future studies to identify the subjects’ physical conditions and the specific elements of these ritualistic ceremonies under which the beneficial effects of dissociation may be reliably observed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was funded by a grant (NSC102-2410-H-250-012) from Taiwan’s Ministry of Science and Technology, also known as Taiwan National Science Council prior to January 2012.