
Abstract
This study reports on the stability of social-cognitive determinants, and on associations between social-cognitive determinants to show insight in the theory of planned behavior (TPB). In all, 278 health professionals who encourage patients to become physically active completed online TPB-based surveys at baseline (Time 1 [T1]) and six months later (Time 2 [T2]). No intervention took place. No differences were found for all social-cognitive determinants measured at T1 compared with T2 (6 months later), except for intention (t test = 5.18, p < .001). Structural equation modeling—χ2(5, N = 278) = 2.35, p = .80, root mean square error of approximation = 0.00—showed that behavior T1 and attitude T1 predicted intention T1 (R2 = .57, p = <.001); that behavior T1 and barriers T1 predicted behavior T2 (R2 = .38, p = <.001); and that behavior T2, intention T1, and attitude T1 predicted intention T2 (R2 =.60, p = <.001). Intention T1 did not predict behavior T2. The model achieved a good fit with the data. Findings revealed that social-cognitive determinants remained stable over time, with intention being instable. Without intervention, the intention decreased, while the social-cognitive determinants (attitudes, perceived behavioral control, and subjective norms) for intention and the corresponding behavior remained unchanged. For intervention development it seems important to value health professionals’ previous or past encouraging behavior (T1), this to change intention and behavior, or to initiate new behavior. Behavior T1 showed a predictive variable and predicted attitude T1, intention T1, barriers T1, and behavior T2. Barriers that obstruct health professionals’ encouraging behavior are encountered, and barriers influence attitudes T1 and the behavior T2 to encourage patients.
Keywords
Background
The theory of planned behavior (TPB) is a robust model, extensively studied and evaluated as an important model to predict intention and behavior, for all kinds of (health) problems and (health care) settings (Ajzen, 1980, 1991; Albarracín, Johnson, Fishbein, & Muellerleile, 2001; Albarracín & Wyer, 2001; Armitage & Conner, 2001a; Godin & Kok, 1996; Hagger, Chatzisarantis, & Biddle, 2001; Hausenblas, Carron, & Mack, 1997; McEachan, Conner, Taylor, & Lawton, 2011). People intend to engage in (health) behaviors when they evaluate their behavior as positive, when they considered the behavior to be under their personal control, and when they considered that significant others find their behavior to be meaningful. The social-cognitive determinants attitude as the evaluation of the (dis)advantages and consequences of the behavior, perceived behavioral control (PBC) as the confidence in the ability to perform the behavior, and subjective norm as the perceived social approval for the behavior, determine intention. According to the TPB, (health) behavior can be predicted by the corresponding behavioral intention and PBC, and hindered by barriers (Ajzen, 1991, 2002; Armitage & Conner, 2001a, 2001b; Bandura, 1987, 1997; Conner & Armitage, 1998; Fishbein & Ajzen, 2010; Godin, Bélanger-Gravel, Eccles, & Grimshaw, 2008; Godin & Conner, 2008; Godin & Kok, 1996; Hagger et al., 2001; Rhodes & Courneya, 2003; Rodgers, Conner, & Murray, 2008; Sheeran, Trafimow, & Armitage, 2003). The behavioral intention concerns the conscious planning of the intended (health) behavior, and according to the theoretical background of the TPB, intention is an important predictor of behavior (McEachan et al., 2011). Intention is important because it prompts a person to engage in the behavior (McEachan et al., 2011). Intention has a significant impact on behavior, so changing behavioral intentions will engender behavior change. Meta-analytic reviews showed the predictive power of the TPB; however, social-cognitive variables should remain stable until the behavior is performed (Armitage & Conner, 2001a; Conner, Povey, Sparks, James & Shepherd, 2003; Cooke & Sheeran, 2004, McEachan et al., 2011). The intention–behavior relationship is stronger when intentions are stable, and this intention stability might moderate the relationship between intention and behavior (Conner & Godin, 2007; Conner, Sheeran, Norman, & Armitage, 2000).
When the intention is strong, the more likely the behavior will take place (Fishbein & Ajzen, 2010). In a meta-analysis, it was shown that medium-to-large changes in intention lead to small-to-medium changes in behavior. The intention–behavior relationship is influenced by barriers and habit. Barriers can obstruct the behavior even though the intention corresponding with the behavior is positive. Habit can predict behavior as it concerns the personal experience with a specific behavior (Brug, de Vet, de Nooijer, & Verplanken, 2006). How well intentions predict behavior depends, on one hand, on the frequency of behavior and, on the other hand, on the stability of the context in which the behavior takes place (Ouelette & Wood, 1998; Triandis, 1980). Intentions have less impact on behavior when the performance of the behavior is conductive to habit formation.
Behavior measured at Time 1 is most likely individual’s frequent performed behavior (Triandis, 1980). According to the TPB, previous behavior does not play an important role in the model, but “the effects of past behavior has proved a challenge for the TPB” (Hagger et al., 2001; McEachan et al., 2011, p. 98). The influence of previous behavior in the TPB is probably not direct but occurs as a predictive variable. Previous behavior will most likely change individual’s beliefs and evaluations and influence intention, and this makes previous behavior a predictive variable (Fishbein & Ajzen, 2010). A study stated that previous behavior influences future behavior, mediated indirect by attitude change (Albarracín & Wyer, 2000). Another study stated that previous behavior is habitually performed behavior, and this habitually performed behavior appeared to come under the control of habits that reduces the impact of intentions on behavior (Ouelette & Wood, 1998; Triandis, 1980).
Nowadays it is common to use the TPB to facilitate the development of effective interventions because we must understand what constitutes intention and (health) behavior before trying to intervene and change intention and (unhealthy) behavior. The assumption is that when we measure social-cognitive determinants and intention at Time 1 and behavior at Time 2, we will have a clear focus on the behavior under study (Fishbein & Ajzen, 2010). Intention and behavior can be changed in a positive direction by implementing carefully designed behavior change interventions (Bartholomew, Parcel, Kok, Gottlieb, & Fernández, 2011; Kok, Schaalma, Ruiter, van Empelen, & Brug, 2004). We hypothesized that when no intervention is implemented, social-cognitive determinants are stable and determinants measured at Time 1 will not differ from those measured at Time 2. This stability of cognitions is a relevant consideration for health professionals because we assume that their professional intention and behavior is stable over time. Parallelly, we hypothesized that because health care professionals are experienced in encouraging patients, behavior T1 is a predictive variable. The objectives of this study were to explore the stability of social-cognitive determinants measured at Time 1 and Time 2, and were to explore the association between social-cognitive determinants measured at Time 1 and Time 2, to predict the intention and encouraging behavior of health professionals.
Method
In a longitudinal design, health professionals were asked to participate in online surveys, at baseline and 6 months later. Participants were former students of the University of Applied Sciences, Utrecht, in The Netherlands. Health professionals who conduct consultations with patients with cardiovascular risk factors and with a bachelor’s degree in nursing (40%) or physiotherapy (60%) were part of this study. We invited 739 health professionals to complete the online survey. In total, 572 health professionals completed the survey at Time 1 (T1, April 2009). In total, 278 of these health professionals completed the survey at Time 2 (T2, October 2009). Three reminders were sent at T1 and also at T2. The content of the questionnaire was derived from a literature review. Also in-depth interviews with health care professionals on how to encourage patients were held and the content was used. There were eight elicitation interviews held and health care professionals were observed in their professional activities for a regular working day. The construction of the questionnaire is according to the TPB, specific to the definition of the behavior and also specified for the population under study (Fishbein & Ajzen, 2010; Kok et al., 2004). The questionnaire is an application of the TPB with the additional variables habit and moral norm. The questionnaire was developed by applying the guidelines how to measure each specific social-cognitive determinant (Fishbein & Ajzen, 2010). The questionnaire was piloted; as a result, no revisions were made.
We collected data at Time 1 (T1) with a repeated measurement at Time 2 (T2), and all answers ranged on a 7-point scale from none/definitely not/very difficult/ and so on (1) to all/most definitely/very easy/ and so on. (7). At T1, the baseline measurement, and at T2, the follow-up measure, we measured social-cognitive determinants, the intention and the behavior of health professionals to encourage patients with cardiovascular risk factors to become physically active. We assessed behavior with two questions: “Do you encourage cardiovascular patients (CVP) to become physically active?” and “In the past month, how many of your CVP did you encourage to become physically active?” (Cronbach’s α = .64). Intention was indexed with three items: “Do you intend to encourage CVP to become physically active tomorrow and the day after tomorrow?” “Do you expect to encourage CVP to become physically active tomorrow and the day after tomorrow?” and “Of the first 10 CVP you see, how many do you intend to encourage to become physically active?” (Cronbach’s α = .82). Attitude was assessed by “In my view, encouraging CVP to become physically active is very good–very bad” and “Encouraging CVP is very useful–very useless.” Then we asked, Is it useful to: assess CVPs’ motivation, assess CVP pros and cons of physical activity, teach CVP how to resist social pressure, teach CVP specific skills pertaining to physical activity, teach CVP how to handle barriers in regard physical activity, formulate physical activity goals together with CVP, teach CVP how to handle relapses, and help CVP understand the relationship between the specific health problem and physical inactivity?
These eight items (“Is it useful to . . .”) were averaged and that score was averaged with the first two item scores to represent attitude (Cronbach’s α = .63). PBC was assessed by “Do you think that you have the skills and knowledge to encourage CVP to become physically active?” “Do you think you can rely on your skills and knowledge to encourage CVP to become physically active?” and third, we asked, “Encouraging every CVP to become physically active is very difficult (1)–very easy (7).” PBC was further assessed by eight items that paralleled the eight items used for attitudes. It is very difficult (1)–very easy (7) to assess CVPs’ motivation, assess the pros and cons of physical activity, teach CVP how to resist social pressure, teach CVP specific skills pertaining to physical activity, teach CVP how to handle barriers in regard physical activity, formulate physical activity goals together with CVP, teach CVP how to handle relapses, and help CVP understand the relationship between the specific health problem and physical inactivity?
Once again, this scale score was calculated and combined with the previous three items as a measure of PBC (Cronbach’s α = .68). Subjective norm was measured by four items: “Most colleagues who are important to me think I should encourage CVP to become physically active,” “Most colleagues value that I encourage CVP to become physically active,” “Patients value that I encourage them to become physically active,” and “The organization I work for values that I encourage CVP to become physically active” (Cronbach’s α = .73). Moral norm was assessed by three questions: “Encouraging CVP to engage in physical activity is . . . my professional duty, . . . a moral obligation, and: . . . an obvious part of my job” (Cronbach’s α = .76). Habit was measured by two questions: “Encouraging patients to be physically active is something I do without thinking, and . . . something I do automatically” (Cronbach’s α = .75). Barriers were indexed by two questions that focused on encouraging patients “even when one is busy” and “even when one’s organization makes it difficult to encourage patients” (Cronbach’s α = .69). Determinant scores were calculated. The questionnaire was also used in two other studies. The questionnaire was used to predict social-cognitive determinants, and in this study we used all T1 data en only behavior T2, and the questionnaire was used in a randomized controlled trial (Sassen, Kok, Schepers, & Verhees, 2014; Sassen, Kok, & Verhees, 2011). The aim of this research was to study the theoretical model of interest. The number of items used to measure a construct affects the reliability of the sum score. The variance of the measurement error of the sum score is larger for questionnaires that use fewer items. More measurement error implies less power to detect any associations between constructs. We were able to find associations between constructs despite a (possibly) large measurement error.
Statistical Analysis
Descriptive statistics were calculated to characterize the study group. To explore the stability of social-cognitive determinants at T1 and T2, we used paired-samples t tests. We postulated a model for the association between social-cognitive determinants of the TPB when measured at T1 and T2. Structural equation modeling (SEM) was conducted to test this model. In Figure 1 (Path model of the Prediction of Intention and Behavior), the TPB model has been shown in gray and black lines. SEM permits to examine direct, indirect, and total effects simultaneously in a single model and to test the validity of the underlying theory (Bentler, 2010; Brown, 2006; Bryan, Schmiege, & Broaddus, 2007; Cole & Maxwell, 2003; Kline, 2011). SEM is based on explaining the covariance between measured variables, and shows the underlying multivariate analyses in regression models (Cole & Maxwell, 2003; Kline, 2011). Standardized estimates of path coefficients were evaluated with t test and a path was left out when it showed not to contribute to the model (t score <2). The variances of the residuals were used as a measure of the unexplained variance for the variable in question. Modification indices were used to decide which path(s) should be included, in addition to the established relationships between the social-cognitive determinants in the TPB. SEM yields a chi-square value to test the null hypothesis that the model fits the data. The root mean square error of approximation (RMSEA) is an additional statistic used as an indication of the adequacy of fit of the path model. The RMSEA indicates a good fitting model when it is ≤.05 (Bryan et al., 2007; Kline, 2011). Significance level was set at α <.05. Statistical analyses were undertaken with SPSS version 17.0 (SPSS, 2009) and with LISREL version 8.80 (Jöreskog & Sörbom, 2004).

Path model of the predicting of intention and behavior (in black and black dotted lines).
Results
Table 1 shows the descriptive statistics for the study sample. In total, 278 health professionals (73.7% female, mean age 36.2 ±10.1 years) completed measurement T1 and T2. Their professional experience was 8.58 (±7.7) years. Time spent on health education during consultation time was 60.4%.
Characteristics of the Study Population (N = 278).
Stability of Social-Cognitive Determinants
Analyses were undertaken to explore differences between social-cognitive determinants measured at T1 compared with the social-cognitive determinants measured at T2 (Table 2). Paired samples t tests showed no differences on all social-cognitive determinants measured at T1 compared with T2, except for intention (t test = 5.18, p < .001). The lowest observed difference was 0.02, the highest of the non-significant differences was 0.09; with the exception of intention. The significant difference for intention T1 compared with T2 was 0.28, meaning a lower intention at T2 to encourage patients with cardiovascular risk factors to become physically active. Analysis showed a strong association for health professionals’ intention at T1 and T2 (r = .53). The behavior remained stable, and analysis showed a strong association for health professionals’ behavior at T1 and T2 (r = .61). Health professionals’ behavior T2 showed a strong association with intention T2 (r = .73), and a moderate association for intention T1 (r = .44). Health professionals’ behavior at T1 showed a strong association with intention T2 (r = .57), and with intention T1 (r = .70). Although the intention changed at T2, changes in attitude, PBC, and subjective norms were not detected. Also moral norms, as well as habit and barriers showed to remain stable over time. Strong associations were found between attitudes T1 and T2 (r = .53), between PBCs T1 and T2 (r = .60), and also between subjective norms T1 and T2 (r = .53). Strong associations were found between habits T1 and T2 (r = .48), and barriers T1 and T2 (r = .50); but only a weak association between moral norms T1 and T2 (r = .19).
Differences Between Social-Cognitive Determinants Measured at T1 and T2 (N = 278).

Note. Values are M ± SD. Social-cognitive variables range from 1 to 7. ns = non-significant.
p < .05, **p < .01. ***p < .001.
Associations Between Social-Cognitive Determinants
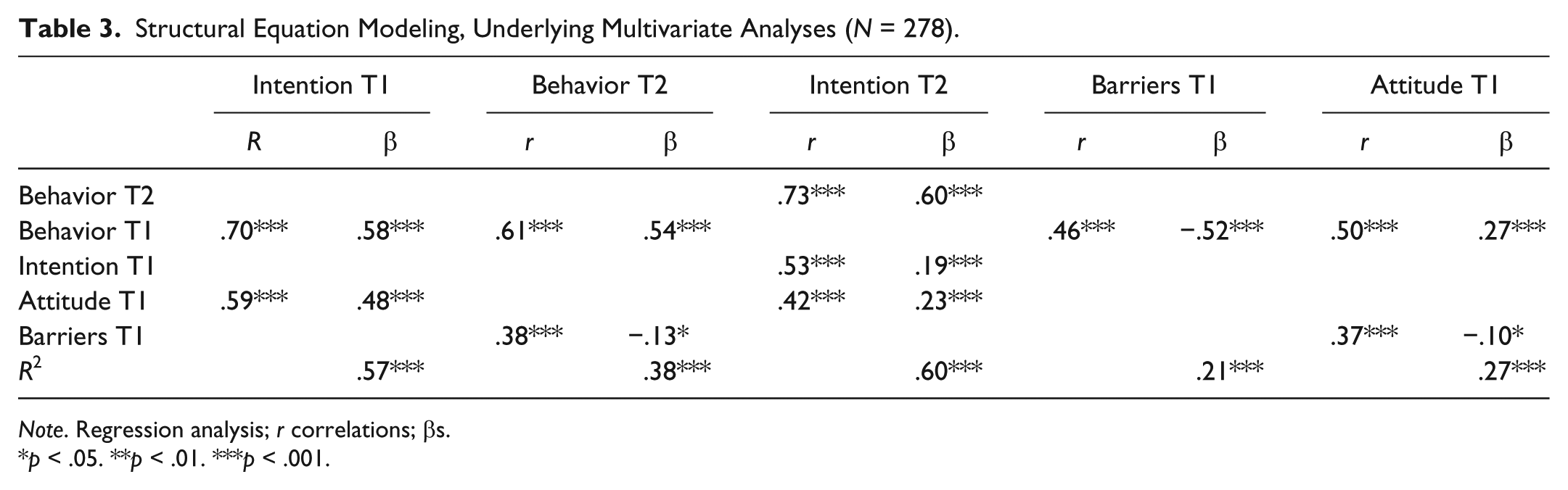
The conducted path model (shown in dark lines in Figure 1) confirmed that we should accept the null hypothesis that the model fits the data, χ2(5, N = 278) = 2.35, p = .80; RMSEA = 0.00, with 90% confidence interval (CI). The RMSEA-value indicated that we created a fitting model and were able to explain the pattern of intercorrelations very well (Table 3). The path model showed five distinguishable insights, together representing the dark lines in Figure 1.
Structural Equation Modeling, Underlying Multivariate Analyses (N = 278).
Note. Regression analysis; r correlations; βs.
p < .05. **p < .01. ***p < .001.
1. Intention T1 of health professionals (to intend and expect to encourage patients with cardiovascular risk factors to become physically active) could be predicted with behavior T1 and attitude T1 (i.e., that the encouraging behavior is evaluated as positive). Behavior T1 (β = .58, p < .001) and attitude T1 (β = .48, p < .001) predicted intention T1 (R2 = .57, p = <.001). There was no significant contribution detected in the path model for PBC T1 (i.e., their personal control over the encouraging behavior) and subjective norm T1 (i.e., if significant others find the encouraging behavior to be important). In the path model, residuals for intention T1 indicated that an important part of the variance in intention T1 has been explained (RS [residual variance] = .38).
2. Behavior T2 of health professionals (to encourage patients with cardiovascular risk factors to become physically active) could be predicted with behavior T1 and barriers T1 (as the obstructions of the behavior). Behavior T1 (β = .54, p < .01) and barriers T1 (β = –.13, p < .01) predicted behavior T2 (R2 = .38, p = <.001). With respect to the relationship between intention T1 and behavior T2, there was no significant contribution detected in the path model for intention T1 (i.e., to intend and expect to encourage patients). Also, there was no significant contribution detected in the path model for habit T1 (i.e., their personal experience with the encouraging behavior). In the path model, residuals for behavior T2 indicated that an important part of the variance has been explained (RS = .51).
According to SEM procedures, we made use of modification indices as a guide to detect omitted paths or disregard unnecessary ones. In the test of omitted paths, we compared the full path model (with a path from intention T1 to behavior T2) with a reduced model (without a path from intention T1 to behavior T2). The t test indicated a weak relationship between intention T1 and behavior T2, and for this we omitted this path in our model. After omitting the path between intention T1 and behavior T2, t tests indicated all significant contributions of the variables. When using modification indices, also no previously unspecified path for intention T1 was detected.
3. The intention T2 of health professionals (i.e., to intend and expect to encourage patients) could be predicted with behavior T2, intention T1, and attitude T1. Behavior T2 (β = .60, p < .001), intention T1 (β = .19, p < .001), and attitude T1 (β = .23, p < .01) predicted intention T2 (R2 = .60, p = <.001). There was no significant contribution detected in the path model for attitude T2, PBC T2, and subjective norms T2. In the path model, residuals for intention T2 indicated that a part of the variance has been explained (RS = .33).
4. The barriers at T1 (i.e., that will withhold health professionals from encouraging patients with cardiovascular risk factors to become physically active) could be predicted with behavior T1. Behavior T1 (β = –.52, p < .001) predicted barriers to be expected at T1 (R2 = .21, p = <.001). In the path model, residuals for barriers T1 indicated that an important part of the variance has been explained (RS = .83).
5. The attitude at T1 of health professionals (as the evaluation of the (dis)advantages and consequences of the behavior) could be predicted with behavior T1 and were withheld by barriers T1. Behavior T1 (β = .27, p < .001) and barriers T1 (β = –.10, p < .01) predicted attitude T1 (R2 = .27, p = <.001). When we applied modification indices following SEM procedures, a previously unspecified path between barriers T1, as the predictor of attitude T1, was shown. In the path model, residuals for attitude T1 indicated that a part of the variance has been explained (RS = .26).
The standardized path coefficients in the path model showed that behavior T1 (to encourage patients to become physically active) had a strong relationship with the encouraging behavior at T2 (path coeff. = .54). Also, the standardized path coefficients in the path model showed that behavior T1 had a strong relationship with intention T1 (to intend and expect to encourage patients, path coeff. = .58). The standardized path coefficients in the path-analysis showed that attitude T1 had an important relationship with intention T1 (path coeff. = .48) and also a relationship with intention T2 (path coeff. = .23). So attitude T1 as the evaluation of the (dis)advantages and consequences of encouraging patients showed to be important in the prediction of intention T1 and also in the prediction of intention T2. Subjective norms as the perceived social approval for the behavior to encourage patients (T1 as well as T2) and PBC as the confidence in the ability to perform the encouraging behavior (T1 as well as T2) did not contribute to the path model.
We explored the encouraging behavior of health professionals measured at T2, and found that particularly behavior T1 and also barriers T1 predicted behavior T2. For behavior T2, there was not a significant contribution detected in the path model for intention T1, barriers T2, or for habit T1 and T2. We explored intention T2 (to intend and expect to encourage patients) and found that intention T1 (path coeff. = .10) and attitude T1 (path coeff. = .23) predicted intention T2, but the path-analysis also showed a strong relationship with behavior T2 (path coeff. = .60).
Discussion
This study reports on the stability of social-cognitive determinants as the predictors of intention and behavior, and on the association between social-cognitive determinants, intention, and behavior to show insight in the TPB.
Stability
We started our study by exploring the differences between social-cognitive determinants measured at T1 compared with social-cognitive determinants measured at T2. We hypothesized that when no intervention is implemented, there will be no difference between social-cognitive determinants measured at T1 compared with T2. The results showed that social-cognitive determinants are indeed stable over time when no intervention is implemented, except for intention. The results showed a discrepancy for intention with a lower intention at T2, but the behavior remained stable over time. Fishbein and Ajzen (2010) described the possibility of instable behavior, but not of an instable intention. A study showed that when intentions are stable, they strongly predict the behavior; but when intentions are unstable, the prediction of the intention–behavior relationship became weaker (Conner et al., 2000). The results indicated that though the intention T2 (i.e., health professionals intend and expect to encourage patients) decreased, the attitude, PBC, and subjective norms of health professionals remained unchanged. Theoretical insights in the TPB showed that if professionals have a strong intention to encourage patients, the encouraging behavior is more to be expected; if professionals lower their intention, the encouraging behavior is less to be expected (Fishbein & Ajzen, 2010). But in our study the intention planning the behavior decreased; this while the input social-cognitive determinants for intention and the corresponding output variable encouraging behavior stayed unchanged. A reason for this may be that behavior T1 is easily remembered, but the intention (planning and intending to show the favorable behavior), can be inadequate; a person lowers his intention and the behavior stayed unchanged. People perceptions of their previous behavior frequently influence their decisions to repeat the behavior. But also, motivational and situational beliefs next to previous behavior might influence the future behavior of people. We examined the impact of social-cognitive variables stability when assessed over the same time period as the intention and behavior. Compared with unstable intentions, correlation studies showed stable intentions were significantly more strongly related to attitude and subjective norms (Conner et al., 2000). Attitude, PBC, and past behavior were strong correlates of stable intentions and weaker correlates of unstable intentions (Conner et al., 2000).
Associations
We continued our study by exploring the associations between social-cognitive determinants. We showed that by analyzing social-cognitive determinants, intention, and behavior in a longitudinal design, the time frame of the TPB could be highlighted.
We explored intention at Time 1, and found that behavior T1 and attitude T1 showed to be important; with no significant contribution detected in the path model for PBC T1 or subjective norms T1. For intention T1, 57% of the variance could be explained. Attitude T1 showed to be especially important in the prediction of intention T1 and also in T2. This finding corresponds with previous studies about the dominant role of attitude in the prediction of intention (Ajzen, 1991; Godin, 1994; McEachan et al., 2011).
We explored behavior T2, and found that particularly behavior T1 and barriers showed to be important. For behavior T2, 38% of the variance could be explained. There was no significant contribution detected in the path model for barriers T2, or for habit T1 and T2. That habit did not contribute was different from than expected. Another study showed that previous behavior appeared to come under the control of habits, corresponding with a reduction of the impact of intentions on behavior (Ouelette & Wood, 1998). Research showed that intentions captured the motivational factors that influence behavior and that intentions had a significant impact on behavior. Intention T1 showed less important than we expected to find on the basis of theory and other studies. With respect to the relationship between intention T1 and behavior T2, we showed that no relationship between intention T1 and behavior T2 could be detected. Also in a meta-analysis it was reported that behavior may be the cause of the reported intention.
We explored intention T2, and found that intention and attitude both at Time 1 predicted intention T2, but that there was also an important contribution of behavior T2 in this relationship. In the path model, residuals for intention T2 indicated that we explained 60% of the variance. We explored barriers T1, and found that behavior T1 is an important predictor, explaining 21% of the variance. We explored attitude T1, and found that behavior T1 and barriers T1 were important predictors, explaining 27% of the variance. In a meta-analysis controlling for the effects of past behavior, the TPB explained 19.3% of the variance in behavior and 44.3% of the variance in intention (McEachan et al., 2011). This meta-analysis also showed that without controlling for the effects of past behavior an additional 10.9% variance to the prediction of behavior, and an additional 5% variance to the prediction of intention, could be explained (McEachan et al., 2011).
Though the path model supports essential prerequisites of the TPB, our findings are slightly different. The path model and especially the path coefficients, showed the importance of behavior T1. This (previous or past) behavior T1 is the encouraging behavior already practiced by, in our study, health professionals. A study stated that previous behaviors are probably of substantial importance for later behaviors (Ouelette & Wood, 1998). We showed that behavior T1 had a strong relationship with intention T1, with behavior T2, with barriers T1, and a moderate relationship with attitude T1. Behavior T1 is most likely the result of education and learning and this will probably result in specific attitudinal changes, that is, changes in beliefs and evaluations (Bryan et al., 2007). Fishbein and Ajzen (2010) do not position behavior T1 in the TPB but theorize that behavior T1 is an exogenous variable that “predicts” cognitions and beliefs, and changes attitudes (Albarracín & Wyer, 2001; Bryan et al., 2007). Past behavior may contribute to the prediction of future behavior, possibly due to the nature of the measures (Ajzen, 2011). Another study showed that people base their attitudes as well as their intentions on their previous behaviors and that their previous behavior had (a small) influence on future behavior (Albarracín & Wyer, 2001). We showed that behavior T1 indeed acts as an exogenous variable and predicted attitude. But next to this result, we showed that behavior T1 acts as an important predictor of behavior T2, intention T1, and of barriers T1. In line with other studies, we think that behavior T1 is important to understand intention and behavior (Amireault, Godin, Vohl, & Pérusse, 2008; Hagger & Chatzisarantis, 2005; Hagger et al., 2001; Ouelette & Wood, 1998; van Osch et al., 2010). The TPB can be extended when a variable explains a greater part of the variance than without that variable, but only if it is a causal antecedent of intention (Ajzen, 2011; Fishbein & Ajzen, 2010).
The way health professionals encourage their patients to become physically active is closely related to the way they will encourage patients in the future. In line with other research, this research indicated that the influence of previous behavior on future behavior is more to be expected when behavior is habitual and occurs in stable contexts (Ouelette & Wood, 1998). Another study showed that previous behavior predicted future behavior, but compared with previous behavior with a reduced role for intentions (Amireault et al., 2008; Hagger & Chatzisarantis, 2005; Hagger et al., 2001; Ouelette & Wood, 1998; van Osch et al., 2010). This reduced role for intention is shown when the behavioral context is stable, as in the encouraging behavior under examination in the current study (Ouelette & Wood, 1998).
The previous encouraging behavior of health professionals made them encounter and try to handle difficulties when encouraging patients. The barriers that obstruct the encouraging behavior are encountered, and barriers influence attitude and the future behavior to encourage patients.
In our study, behavior T1 predicted intention T1, but intention T1 did not predict behavior T2. This finding is different from what we expected on the basis of previous research, except one meta-analysis. A meta-analytic review showed that intentions accounted for a considerable proportion of the variance in behavior (Armitage & Conner, 2001a). Correlational studies indicated that intentions occasionally predict previous or past behavior better than future behavior. When people state their intention, it brings to mind their previous behavior. This can result in an intention more consistent with previous behavior (Albarracín & Wyer, 2001; Fishbein & Ajzen, 2010). A study showed that intentions sometimes poorly predicted behaviors (Kor & Mullan, 2011), that the predictive validity of the TPB is limited (Sniehotta, Presseau, & Araújo-Soares, 2014), but that theory can be changed using available evidence (Kok & Ruiter, 2014).
Our path model showed that behavior T1 predicted intention T1, and also that intention T1 predicted intention T2. Research indicated in a three-factor path model (intention, and previous and future behavior) that routine behavior can be predicted from previous behavior and intention, but with a stronger direct effect of previous behavior on future behavior than for intention (Ouelette & Wood, 1998). A study showed that stable intentions were more predictive for future behavior, and when intentions are instable, the influence of previous behavior increased (Sheeran, Orbell, & Trafimow, 1999). In three out of six studies, it was shown that previous behavior had a significant relationship with future behavior (Conner & Godin, 2007). This study also showed that when intentions are stable, they can diminish the influence of previous behavior, but when intentions are instable the influence of intention as a predictor of behavior is less apparent (Conner & Godin, 2007). Our measure of intention T1 showed instable; this increased the influence of previous behavior in the path model, making intention less predictive for future behavior. Also a meta-analysis showed that “past behavior was the most important predictor of behavior but not intention” (McEachan et al., 2011, p. 125).
Health professionals are experienced in encouraging patients with cardiovascular risk factors to become physically active to decrease cardiovascular risk, and professionals probably have learned during education and in practice how to encourage patients. For intervention development and evaluation, previous or past behavior should be taken into account as it can explain behavior, that is, predict intention and future behavior (Kok & Ruiter, 2014). Implications for changing the intention and behavior of health professionals may be that previous or past behavior can have a positive or negative influence on present or future behavior. In line with Ouelette and Wood (1998), it seems important for intervention development to value individuals’ previous behavior not only to change existing behavior but especially to initiate new behavior. To initiate new behavior requires decision making, the formulation of explicit plans to initiate and implement a new behavior, and to restrain from previous, well-practiced behavior (Conner et al., 2000; Gollwitzer & Schaaol, 1998; Ouelette & Wood, 1998). Previous or past behavior is possibly more difficult to change than other TPB social-cognitive determinants (McEachan et al., 2011) and needs specific methods for behavior change and the development of change interventions (Kok & Ruiter, 2014). Implications for intervention design and implementation is also that attention should be directed at increasing intention stability by persuasive techniques targeting attitudes, by prioritizing advances and consequences of the behavior (Conner et al., 2000).
Strengths of this study are the longitudinal design as this rules out the possibility that measurements at T2 influenced measurements at T1. Also that all social-cognitive variables were measured on the same scale, which increases the predictive validity of intention and behavior (Fishbein & Ajzen, 2010). The study’s sample size is an additional strength, because it was sufficiently large for all t tests, tests of path coefficients, and multiple regressions in SEM to be statistically significant with 95% confidence intervals. Limitations of the study included a possible restricted sample because the professionals were recruited from the same institute and this may limit generalization of the outcomes. A limitation is also the response rate at T2, with the possibility of selection bias, although we could not detect difference in health professionals’ characteristics. Further studies are needed across different groups and different (health) behaviors to further explore the influence of behavior T1, the undetected path from intention T1 to behavior T2, and the path from behavior T1 to intention T2. Probably it is desirable to better test the sequence of the intention and behavior-related questions in the questionnaire. Another factor would probably be to ad measurements of social-cognitive variables at Time 3, possibly only for behavior. Also the detection of additional, theoretically interesting, variables to incorporate in a path model is probably needed, to lower residual coefficients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.