
Abstract
A public health approach to suicide prevention (SP) emphasizes using a comprehensive plan utilizing multiple strategies to address suicide in the community of interest. Universities using this approach are called to develop interventions to increase SP knowledge, reduce suicide risk factors, enhance protective factors, and examine their efforts scientifically to evaluate program effectiveness. The current study polled responding college students (N = 819) about their exposure to campus SP messaging materials, participation in SP activities, and whether they experiencedhavinga person close to them attempt or die by suicide during the three years of a SP program funded by the Garrett Lee Smith Memorial Act (2004). Students were also queried about their perceived level of SP knowledge, knowledge of suicide facts, and the stigma associated with receiving treatment for suicidal thoughts and behaviors using the Suicide Prevention Exposure, Awareness, and Knowledge Survey (SPEAKS). Simultaneous multiple regression analyses were used to examine relationships between study variables. Results indicated that exposure to SP messaging materials predicted a higher level of self-perceived knowledge and a lower level of perceived stigma. Participating in SP activities and having someone close to you attempt or die by suicide predicted both a higher level of perceived knowledge and actual knowledge of suicide facts. Self-identifying as male predicted a higher level of stigma. Implications for campus SP programming are discussed.
Introduction
Traditionally aged college students typically experience transition in many, if not most, areas of their lives during their college careers. During this period of developmental transition, many students function relatively well, but many experience difficulty adjusting, distress, and mental health problems (Brooks & DuBois, 1995). On a recent administration of the National College Health Assessment (American College Health Association, 2013), 45% of students sampled endorsed that they “felt things were hopeless,” 31% indicated that they were “so depressed it is difficult to function,” and 7% “seriously considered suicide” within the 12 months prior to being surveyed. There has been an increased incidence of serious mental health difficulties among college students in the past 15 to 20 years (Kadison & DiGeronimo, 2004). The rate of adolescent suicide in America tripled between 1950 and 1990 (CDC, 1992).
In response to the increasing mental health needs of college students and the concerning rate of suicide in this population, several important developments have occurred. In 2004, the federal government, after recognizing the need for college suicide prevention (SP), funded the Garrett Lee Smith Memorial Act (GLSMA; 2004). The Act provided monies to college and university grant recipients to conduct SP activities. Recipients were encouraged to consider using a public health approach following the National Strategy for Suicide Prevention (United States Department of Health and Human Services [USDHHS], 2012). The public health approach advocates a paradigmatic shift from focus upon individuals at risk for suicide to a community approach, utilizing multiple strategies and a comprehensive plan to address suicide across the community. The United States Substance Abuse and Mental Health Services Administration (SAMHSA, 2004) requires grant recipients to participate in local evaluation of their efforts and in a coordinated evaluation of all grant funded institutions (cross-site evaluation). The hope is to accumulate an evidence-base of effective SP programs (SPP) and/or program components.
There are detailed recommendations for campus SPP (American College Health Association, 2002; Drum & Denmark; 2011; Jed Foundation, 2006; Suicide Prevention Resource Center [SPRC], 2004). These recommendations include stigma reduction and social marketing campaigns; augmenting and/or creating inclusive, caring, and responsive campus communities; suicide education; early identification of at-risk students; effective assessment and intervention (increased counseling center staff skill and responsiveness); and improved organization policies and procedures. Colleges and universities have implemented the SP activities that fit with their budget, philosophy, aims, and unique campus culture (Stevens, 2013). Prevention efforts vary widely with some programs having a large scope and seeking to address wide segments of the campus and others having more limited focus, seeking to address smaller and perhaps more influential campus members.
A literature review of campus SP efforts was initiated using PsycInfo database; key search terms included university/college, students, suicide prevention, and suicide. Reviews of campus interventions/programs directly involving students have provided mixed results. Several pre-packaged gatekeeper-training programs have widely been used on campuses. Most of these programs educate participants about suicide and seek to influence their attitudes about suicide and help seeking. In addition, programs may train participants to query about suicide and refer to mental health professionals if they encounter someone at risk. The Question, Persuade, Refer (QPR) program is a gatekeeper-training program (Quinnett, 1995) that is used on many campuses and has probably received the most scrutiny. QPR is considered evidence-based and is cited in the registry of such programs by the SPRC. Studies of the effectiveness of QPR have found that participants increase not only their awareness and knowledge of suicide, but also their appraisal of their own competency and readiness to intervene with someone at risk (Indelicato, Mirsu-Paun, & Griffin, 2011; Mitchell, Kader, Darrow, Haggerty, & Keating, 2013; Tompkins & Witt, 2009; Wynman et al., 2008). However, Mitchell et al. (2013) found that participants returned to baseline levels in their beliefs about whether it is appropriate to ask someone about suicide after some time had passed. Although there are clear benefits for the participants trained in a gatekeeper programs, they may not retain knowledge, may not act to intervene with someone at risk, and/ or may not ever encounter a potentially suicidal person. Another disadvantage of gatekeeper-training programs is that they usually only reach a section of the campus community (Moore, 2012).
Other programs aim to reach larger numbers of campus members. Social marketing approaches to SP on college campuses use the principles and methods of commercial marketing to craft and disseminate messages to promote help seeking; increase information about suicide, prevention, and mental health resources; and decrease the stigma associated with mental illness and mental health treatment (Chambers et al., 2005). Some social marketing approaches are often appealing and seem successful. Whether these approaches change behavior is difficult to measure, and attributing causality to a social marketing approach is impossible (Smith, 2006). Approaches using widely available technologies have become increasingly popular as a means to reach students with SP content. These approaches include online mental health screening, phone apps, online videos, and interactive websites. Anecdotal evidence, website “hits,” and number of students who use an “app” and/or participate online for mental health difficulties can provide some information about the success of these initiatives.
There have been some studies of the effectiveness of multicomponent SPP for specific communities reported in the literature. One program that has been researched and has received much acclaim is the SPP developed for the United States Air Force (USAF, 2001). The USAF Suicide Prevention Program (USAFSPP) is a community-oriented approach to reducing suicide risk containing 11 components. The program seeks to enhance psychosocial protective factors, raise awareness of suicide, improve the identification and treatment of those at high risk, and promote help seeking (Knox, Litts, Talcott, Feig, & Caine, 2003). Program results showed a sustained decrease in the rate of suicide among Air Force personnel. University or college-based programs that have adopted multicomponent strategies have been described in the literature, but few have presented data for program effectiveness. A notable exception is a University of Illinois program that reduced the rate of suicide in that institution’s county substantially and over many years (Joffe, 2008).
The present study investigated the awareness, knowledge, and presence of stigmatizing beliefs about suicide among students at one university during the 3-year period of GLS funding. Over the grant period, the university’s SPP created and implemented a community-based, multicomponent SPP based loosely on the USAFSPP. The program offered many of the recommended elements for college and university SP programming including the following:
In-person trainings promoting awareness and information about suicide and mental health resources for selected groups and student leaders.
Health education theater productions with SP infused content
Informational messaging materials increasing awareness of suicide and mental health resources.
Social marketing messages aimed at reducing social stigma and promoting help seeking for mental health concerns.
Purpose of Study
This study presents local data from a large Midwestern university. The data were also collected as part of a cross-site evaluation that included all GLS campuses (see Goldston et al., 2010). This study did not measure outcomes related to discrete SP activities. Rather, the present study sought to examine the following research questions:
Method
Data Collection
Random samples of students across the entire student population were electronically recruited to participate in this study using the Dillman (2000) method. There were three waves of survey administration (2007, 2008, 2009) using a cross-sectional design. A total of 6,626 surveys were sent to students, resulting in a response rate of 12.4% (N = 819). Student samples were stratified by gender, race/ethnicity, and academic level (e.g., freshman, graduate student) to ensure that sample demographics reflected the campus population. Respondent lists were uploaded to a secure server, email addresses were verified, and duplicate email addresses were removed. Email notifications were initially sent about the survey, followed 1 week later by an email with information about how to access the survey electronically with a unique password, then followed by two more notifications in 1-week intervals, to those who had not yet completed the survey.
Informed consent was obtained during the login process, where potential participants received information about the purpose of the study, content of the survey, administration procedures, potential risks, and contact information. No identifying information was collected on the survey itself. The University’s Human Subjects Institutional Review Board approved this study.
Participants
In total, 819 undergraduate and graduate students participated in the survey across three waves of administration. Most respondents were female (60.7%), and ages ranged from 17 to 56 years (M = 22, SD = 5.11). Reported ethnicities among respondents were Caucasian (91.1%), African American (5.4%), Asian (3.5%), and Hispanic (3.2%), representative of the student population. The majority of students (96.8%) self-reported as undergraduates. Due to missing variables, the student sample size for data analysis ranged from 819 to 815.
Instrument
The Suicide Prevention, Exposure, and Awareness Knowledge Survey (SPEAKS) is the web-based instrument developed specifically for GLS campuses. The SPEAKS–Student Version (SPEAKS-SV) includes 54 items and collects data on respondents’ demographics, self-reported exposure to SP messaging and awareness of campus SP activities, perceived SP knowledge (perceived knowledge), actual knowledge of suicide facts (facts), and social stigma associated with having a mental illness and mental health help seeking (stigma). The SPEAKS-SV takes about 15 min to complete and includes items that are multiple-choice, Likert-type scale, and true/false. There are no psychometric properties available for the total SPEAKS measure; however, two subscales were adapted from the literature, i.e., the Stigma Scale for Receiving Psychological Help (SSRPH; Komiya, Good, & Sherrod, 2000) and published suicide myths and facts (Fremouw, de Perczel, & Ellis, 1990).
Exposure to and Participation in SP Activities
The SPEAKS-SV includes two questions that measure exposure to SP messaging and participation in SP activities on campus. Specifically, survey participants were asked (a) whether they had been exposed to SP messaging on campus (e.g., brochures, posters, videos, radio messages, orientation materials), and (b) whether they had directly participated in any campus SP activities (e.g., seminars, workshops).
Perceived Knowledge
The SPEAKS includes six items that measure respondents’ perceived knowledge about suicide and its prevention on a scale from 1 to 5, ranging from “very little” to “a great deal.” For example, respondents are asked to rate their knowledge of (a) suicide facts, (b) suicide risk factors, and (c) how to assist someone in getting the help they need. The responses of these six items were then averaged, creating a perceived knowledge score. In the present study, internal consistency was high for this subscale with a total Cronbach’s alpha of .89.
Facts
The SPEAKS contains a 28-item Facts subscale that includes questions about published facts and myths regarding suicidal thoughts, risk factors, and behaviors (Fremouw et al., 1990). Participants’ answers were measured against correct answers to develop a total Facts subscale score. Examples of items included the following: (a) “People often attempt suicide without warning and out of the blue”, and (b) “Hopelessness is a risk factor for attempting suicide”. In the present study, total Cronbach’s alpha for this subscale was moderate (.52).
Stigma
The SPEAKS includes a five-item Stigma subscale with scores ranging from 0 to 5, and higher scores indicating a higher level of stigma. Questions on the Stigma subscale were adapted from the SSRPH, which was originally developed to assess perceived stigma associated with receiving psychological treatment in undergraduate students (Komiya et al., 2000). The original five-item scale has a one-factor structure and acceptable internal consistency (.72; Komiya et al., 2000). The SSRPH was modified in a prior study to reflect stigma associated with receiving treatment for depression (Pyne et al., 2004), and similarly modified on the SPEAKS to reflect stigma associated with receiving treatment for suicide-related problems. Examples of items on the Stigma subscale included the following: (a) “Receiving treatment for suicidal thoughts and behaviors carries social stigma”, and (b) “It is a sign of personal weakness or inadequacy to receive treatment for suicidal thoughts and behaviors”. Respondents endorsed items on a 4-point scale that ranged from strongly disagree to strongly agree. In the present study, internal consistency for this subscale was acceptable with a total Cronbach’s alpha of .77.
Preparation for Analyses
Diagnostic procedures (e.g., examine distribution, range, outliers, and test for multicollinearity) were conducted for each criterion variable (perceived knowledge, facts, stigma).
Analyses
Analyses were conducted using IBM SPSS Statistics 19. These analyses included (a) t test and chi-square analyses to compare results for student groups (female, male), and (b) simultaneous regression. An alpha level of .05 was used for all statistical tests.
Results
Exposure to and Participation in SP Activities
Among respondents, 383 (47%) reported having been exposed to some form of SP materials on campus. In contrast, only 54 (6.6%) respondents reported having participated in SP activities on campus.
Perceived Knowledge
Of the total sample, 241 (29.4%) reported having above average to a great deal of perceived knowledge about suicide facts. Almost half (379) reported having above average to a great deal of perceived knowledge about suicide risk factors. Twenty-five percent (207) reported having more than average to a great deal of perceived knowledge about how to ask someone about suicide. Thirty percent (248) reported having above average to a great deal of confidence in their ability to convince a person to seek help. Nearly a third reported having above average to a great deal of perceived knowledge about how to assist someone in getting the help that they need. Twenty-four percent (194) reported having above average to a great deal of perceived knowledge about local resources to refer someone to. No significant differences were found on this measure in terms of sample demographics.
Facts
Twenty-nine percent of the respondents (344) scored 80% or higher on the Facts subscale. A significant difference was found on the total subscale, with those identified as upper academic level (junior, senior, graduate student) scoring significantly higher (p = .040) than those identified as lower academic level (freshman, sophomore).
Stigma
The majority of the respondents (66%) believed that receiving treatment for suicidal thoughts and behavior carries social stigma. Twelve percent reported that they agree or strongly agree that it is a sign of personal weakness to receive treatment for suicidal thoughts and behaviors. Forty-six percent of the respondents reported that others would view a person who received treatment for suicidal thoughts or behaviors less favorably. Nineteen percent of the respondents reported that it is advisable to hide from others that she or he had been treated for suicidal thoughts or behaviors. Twenty-six percent of the respondents reported that persons who seek treatment for suicidal thoughts or behaviors tend to be liked less than others. A significant difference was found on the total Stigma subscale with males reporting a higher level of stigma (p = .002), when compared to females, see Table 1.
Demographic Characteristics of Sample.

Note. SP = suicide prevention.
Data missing for four respondents.
Preparation for Multivariate Analyses
Bivariate analyses were conducted between predictor and criterion variables. Pearson product–moment correlations were conducted between major study variables. Multicollinearity was not detected between predictor variables. For the predictor variables, age significantly correlated with educational level (positive, weak), exposure (negative, weak), and having someone close attempt or complete a suicide (positive, high). Exposure also correlated with participation (positive, weak) and academic level (negative, weak). Having someone close to you attempt or die by suicide was also correlated with gender (negative, weak).
For the criterion variables (perceived knowledge, facts, stigma), perceived knowledge and facts were found to have a significant (positive, weak) correlation. The Stigma subscale had a negative and weak correlation with both the Perceived knowledge and Facts subscales.
Multiple Regression Results
To examine the relative contribution of demographic variables, participation in SP activities, and/or having a person close to you attempt or die by suicide in predicting perceived knowledge, facts, and stigma, multiple regression analyses were conducted (see Tables 2-4). The six predictor variables were (a) age, (b) academic level, (c) gender, (d) exposure to SP materials, (e) participation in SP activities, and (f) having a person close to you attempt or die by suicide (1 = yes, 0 = no). Only variables that were significant at the bivariate level were included in the multivariate models.
Summary of Simultaneous Regression Analyses for Variables Predicting Perceived Knowledge (N = 814 a ).
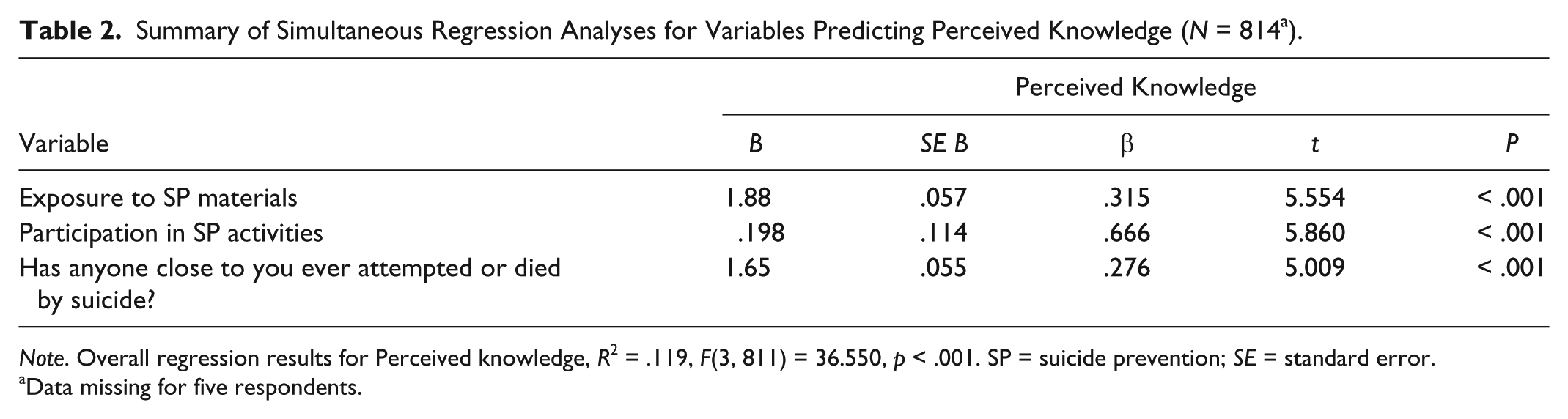
Note. Overall regression results for Perceived knowledge, R2 = .119, F(3, 811) = 36.550, p < .001. SP = suicide prevention; SE = standard error.
Data missing for five respondents.
Summary of Simultaneous Regression Analyses for Variables Predicting Facts (N = 814 a ).
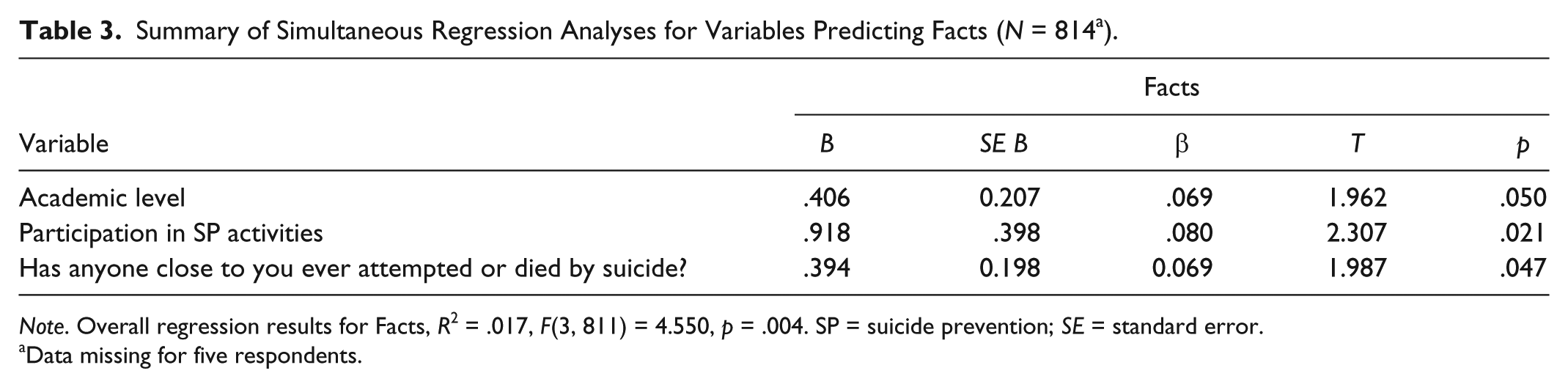
Note. Overall regression results for Facts, R2 = .017, F(3, 811) = 4.550, p = .004. SP = suicide prevention; SE = standard error.
Data missing for five respondents.
Summary of Simultaneous Regression Analyses for Variables Predicting Stigma (N = 814 a ).

Note. Overall regression results for Stigma, R2 = .026, F(3, 810) = 7.238, p < .001. SP = suicide prevention; SE = standard error.
Data missing for five respondents.
The model predicting perceived knowledge included the following predictors: (a) exposure to SP materials, (b) participation in SP activities, and (c) having a person close to you who attempted or died by suicide. Using the enter method, these variables predicted perceived knowledge (R2 = .119, < .001), adjusted R2 = .116. Each predictor variable entered significantly contributed to the model (see Table 2).
The model predicting knowledge of facts included the following predictors: (a) academic level, (b) participation in SP activities, and (c) having a person close to you who attempted or died by suicide. Using the enter method, these variables predicted greater accuracy of facts (R2 = .017, = .004), adjusted R2 = .013. Each predictor variable entered significantly contributed to the model (see Table 3).
The model predicting stigma included the following predictors: (a) gender, (b) exposure to SP materials, and (c) participation in SP activities. Using the enter method, these variables predicted stigma (R2 = .026, < .001), adjusted R2 = .023. Significant predictor variables included gender (β = .098, p = .005) and exposure to SP materials (β = −.101, p = .005; see Table 4).
In summary, having been exposed to SP materials predicted a higher level of perceived knowledge and a lower level of stigma. Participating in SP activities and having someone close to you attempt or die by suicide predicted both a higher level perceived knowledge and facts. Self-identifying as male predicted a higher level of stigma.
Discussion
Multivariate analyses of a large stratified random sample of university students sought to investigate how many students reported participating in SP programming or were exposed to SP messaging. Findings reveal that few responding students endorsed that they participated in SPP (6.6%), whereas significantly more students endorsed that they had been exposed to SP messaging (47%). These findings are consistent with GLSMA grantee cross-site data from 90 participating campuses (Cohorts 1-4, 2007-2012) that indicate 8% of the responding students participated in SP activities and 47% of responding students endorsed that they were exposed to SP messaging (Suicide Prevention Data Center, 2014).
We also sought to discover the overall level of perceived knowledge, facts, and stigma the respondents possessed. Most responding students did not perceive themselves as having a lot of knowledge about suicide, and most believed they would not be able to recognize suicide warning signs. These findings are consistent with King, Vidourek, and Strader (2008) who found that only 11% of students strongly believed they could recognize risk for suicide. Less than one third of our respondents felt confident in their ability to convince someone to seek help and perceived themselves as having more than average to a great deal of confidence in their ability to ask someone about suicide and intervene when someone is at risk. These findings are also similar to those found in previous research (Drum, Brownson, Denmark, & Smith, 2009; King et al., 2008; Westefeld et al., 2005).
The lack of confidence that most respondents had in their ability to ask someone about suicide poses a significant concern. Research has shown that a high percentage of suicidal persons disclose only to their intimates and not to mental health practitioners (Drum et al., 2009). Furthermore, many will not disclose their suicidal thoughts to others voluntarily and may disclose only when directly asked. These findings suggest that although general informational programs may increase SP knowledge, targeted interventions such as gatekeeper trainings are needed to assist students in taking action with a potentially suicidal peer. To prevent the erosion of learning and encourage active intervention, bolster gatekeeper-training sessions may be necessary.
Participation in SP activities predicted both a higher level of perceived knowledge and greater accuracy in facts. In this study, perceived knowledge is reflective of an individual’s perception of their skill and ability in recognizing and responding appropriately to those at risk for suicide. These findings suggest that SP activities may have been successful in educating students about suicide generally and increasing their confidence in their own competency in dealing with a suicidal peer. Students with higher academic level scored significantly higher on the Facts subscale compared with students with a lower academic level, consistent with McIntosh, Hubbard, and Santos (1985). Students with higher academic standing may be more knowledgeable about suicide than their younger counterparts due to repeated exposure over time to SP information on campus and other factors not measured by this study.
Exposure to SP messaging did not predict greater knowledge of suicide facts. although it did predict a higher level of perceived knowledge. Because SP messaging did not aim to increase knowledge of suicide facts, this finding is not surprising. It is encouraging that the messages aimed at increasing students’ awareness of suicide and mental health resources, and promoting help seeking for mental health concerns, may have been successful.
Two thirds of students agreed that having suicidal thoughts or behaviors carries social stigma, and nearly half of the participants endorsed that people who seek treatment for mental health concerns are stigmatized and viewed less favorably by others. Golberstein, Elsenberg, and Gollust (2008) identified perceived public stigma as the stigmatized beliefs people perceive others as having (the construct measured in the current study). They found that perceived public stigma does not interfere with help seeking, but personal stigma (the application of stigmatizing beliefs to the self) was significantly and negatively associated with help seeking among college students. If, as Corrigan, Watson, and Barr (2006) proposed, social stigma develops before, and is a precursor to personal stigma, changing culturally supported stigmatized beliefs about mental illness may be especially important to address. Although such attitudes are difficult to modify (Pescosolido et al., 2010), they must be addressed to further reduce barriers to accessing potentially life-saving assistance.
Interestingly, exposure to suicide prevention messaging predicted a lower level of stigma about receiving treatment for suicidal thoughts and behaviors, whereas participation in SP activities did not. It is tempting to suppose that the SP messaging may have been successful in its aims to reduce stigma, or there may be other variables not measured here that contribute to this finding. It may be that those with less stigmatized attitudes paid closer attention to and remembered suicide prevention messaging more frequently. Social marketing approaches in general have historically been most successful in influencing behaviors and less successful in changing attitudes (Daigle et al., 2006). More research is needed to determine how social marketing messaging may effectively reduce stigma about suicide and mental illness.
Male participants endorsed a significantly higher level of stigma. This finding is consistent with other studies showing that male gender is associated with increased mental health stigma (Eisenberg, Downs, & Zivin, 2009; Golberstein et al., 2008), decreased understanding of suicide behavior, and increased negative judgment (Spirito, Overholser, Ashworth, & Morgan, 1988). Greater male stigmatizing beliefs are likely to be reflective of gender differences in socialization, behavior, and/or personality traits. To reach males, programs and messaging must find a way to capture their attention and ultimately decrease stigma. This need is especially important given that males die by suicide more frequently than females (CDC, 2014) and are less likely to seek help for mental health difficulties (Syzdek, Addis, Green, Whorley, & Berger, 2014).
Nearly half of all responding students reported having someone close attempt or die by suicide. This experience predicted both a higher level of perceived knowledge and greater accuracy in facts. Although the association between having direct experience with a suicidal person and knowledge of suicide facts has not been widely studied, this finding suggests that exposure to suicide behavior (in intimates) may reduce one’s acceptance of suicide myths. This is in contrast to earlier research that found no association between knowing someone who attempted or died by suicide and level of SP facts (McIntosh et al., 1985). It also makes intuitive sense that an individual’s prior experience with another person’s attempt or death by suicide would contribute to their perception of themselves as having greater knowledge about how to intervene with someone at risk of suicide. No relationship was found between having someone close attempt or die by suicide and level of stigma.
Limitations
This study included participants from one university, and these participants may differ from members of other institutions. The response rate was low (12.5%), and although this is major limitation, it is not considered atypical for college student surveys (Dillman, 2000). It is unknown whether those who participated in the survey differed from those who did not. Selection bias may be a concern due to the low response rate, as it is unknown whether those who responded did so because of a special interest or antipathy for the topic. However, a relatively low response rate may not indicate the results are inaccurate (Visser, Krosnick, Marquette, & Curtin, 1996). The study was cross-sectional, and therefore, causality for outcomes is unknown. The homogeneity of the sample limits generalizability to other college/university populations.
Implications and Future Directions
Comprehensive and multicomponent programs have ambitious aims that are difficult to accomplish and evaluate. With limited funding and a finite number of staff hours available to SP, difficult programmatic decisions must be made. These decisions are best made after an assessment of the unique culture of each institution (SPRC, n.d.) and the students who are in attendance. Although more research is needed to determine which aspects of SPP are generally effective in increasing knowledge, decreasing stigma, and ultimately preventing suicide, we must also consider new and innovative ways to deliver messages and programs using the technological approaches that appeal to today’s students.
Conclusion
This study measured exposure to SP messaging, participation in SP activities, perceived knowledge, facts, and stigma in a sample of university students. Study findings support the need for ongoing comprehensive multicomponent SPP on college campuses. Effective SP campus programming necessitates targeted strategies to increase knowledge about suicide, increase the probability of effective intervention with persons at risk, and decrease the stigma associated with having mental health concerns and seeking treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This project was funded through the Substance Abuse and Mental Health Services Administration and the Garrett Lee Smith Memorial Act (GLSMA) College Suicide Prevention Grant Program.