
Abstract
The Alabama Lifespan Respite Resource Network™ enhances respite services for family caregivers. University evaluators conducted a statewide assessment of respite providers using multiple formats. The purpose was to determine met and unmet needs for respite training among providers serving family caregivers of individuals with disabilities and chronic illnesses. A total of 317 respite providers attempted and 191 completed survey items, revealing respite experience, disabilities and chronic illnesses, areas of difficulty, prior training and confidence, training needs and preferences. Results will be used by a state Network to match content and delivery of training to providers’ needs. Respite providers have important roles to play, sharing information about respite services and providers, advocating for caregiver eligibility to receive services, and participating in training paid and volunteer providers.
Introduction to the Lifespan Respite Care Program
In all, 8 of 10 adults requiring long-term care live at home or in the community; 90% of the care burden falls upon unpaid family caregivers (Aldrich, 2011; Family Caregiver Alliance, 2006, as cited in Collins & Swartz, 2011). Respite, planned short-term relief for family caregivers, has many benefits as articulated by service recipients: Respite services for the caregiver are very important. One person cannot handle “around the clock” care. It enables families to keep their children at home instead of placing in nursing homes due to total care. These services are very necessary for me to be able to go to doctor, dental appointments, get groceries, and being able to get out of the house for some time for myself. I don’t know what I’d do without this help to care for my mom. Respite really aids in providing a more normal life for my 20-year-old son with Duchenne Muscular Dystrophy . . . My husband and I are so happy that we can all be home together. It is crucial for us to have a break . . . They are needed so family members [with disabilities] can stay at home and it improves the health of the caregiver. (Geiger & O’Neal, 2012, p. 11)
An effective Lifespan Respite Care Program features dynamic collaboration among funders and service agencies providing respite to meet diverse needs of family caregivers. The Lifespan Respite Care Act (2006) defines Lifespan Respite as “coordinated systems of accessible, community-based respite services for all family caregivers of individuals with disabilities or chronic illness, regardless of age or special need.” Funding provided to eligible state agencies enables lifespan respite programs to (a) identify existing respite resources and service gaps, (b) coordinate respite resources and providers, (c) create new respite services to address service gaps, (d) recruit and train qualified paid and volunteer respite providers, (e) provide public awareness information, and (f) empower caregivers by connecting them to respite resources and providers. This article describes methodology and results for Task 1 (gathering information on existing needs, programs, and services through a planned needs assessment of respite service providers) in Alabama. Needs were assessed by experienced external evaluators; results will be used by Network members to improve respite care training and service delivery.
The U.S. Administration on Aging, the federal agency that administers Lifespan Respite Care Program, guides states to collect baseline information needed to plan effective respite:
population of family caregivers as defined by number by geographic area, age, family size, income level among other traits;
specific respite care needs of family caregivers;
existing respite care services and unmet needs in the following areas: capacity to provide respite care services to family caregivers;
number and types of caregivers served; and
coordination of respite care information and services within the state and localities.
A needs assessment is the foundation to build a state Lifespan Respite system. According to the Work Group for Community Health and Development at the University of Kansas (2011), “needs can be defined as the gap between what is and what should be.” Data from service providers will indicate needed improvements in professional preparation, for instance, most often requested training topics and preferred formats.
Method
The Alabama Department of Senior Services (ADSS) received a federal award enabling collaboration with the Alabama Lifespan Respite Resource Network™ (Respite Network) and its Coalition. Members include state and nonprofit agency professionals, respite providers, and consumers. The purpose is to plan and implement better access to respite resources for all Alabama family caregivers. According to federal law, “family caregiver” means an “unpaid family member, a foster parent, or another unpaid adult, who provides in-home monitoring, management, supervision, or treatment of a child or adult with a special need” (The Lifespan Respite Care Act, 2006). The National Alliance for Caregiving and American Association of Retired Persons (NAC & AARP, 2009) estimated that 65.7 million people in the United States served as unpaid family caregivers to an adult or a child.
Evaluators assessed needs of caregivers and their respite providers and monitored achievement of grant goals and objectives. The evaluation of the Alabama program addressed the mandated priorities of the federal grant. Three goals guided the evaluation: (a) to measure current capacity and improvement of Alabama Respite Network as perceived by family caregivers, agencies, and providers; (b) to identify needed enhancements to respite worker training and service delivery; and (3) to identify facilitators and barriers to a coordinated system of lifespan respite care in Alabama. Effective planning of respite requires understanding caregivers’ needs, perceptions, and experiences (Geiger & O’Neal, 2012).
Evaluators collaborated with members of the state Respite Network and its Capacity Work group to develop two survey tools, and to invite family caregivers and agency service providers to participate. The focus of this article is on methods and results of the second survey developed to gather perceptions from respite service providers. The purpose is to determine providers’ preparation, service history, and unmet training needs.
Authors reviewed the helpful guide published by ARCH National Respite Network and Resource Center (2002), Evaluating and Reporting Outcomes: A Guide for Respite and Crisis Care Program Managers. Network members and service providers offered suggestions about survey content and format during two public meetings, and by email and telephone messages. Consistent with the Stress Process Model of Caregiving, Network members were concerned about the quality of life among family caregivers who prioritize loved ones’ immediate needs before their own. Short-term respite care may ameliorate primary (impaired health, disabilities, limitations) and secondary (role demands, anxiety, depression) stressors among caregivers (Jansen et al., 2009; Mensie & Steffen, 2010; Pearlin, Mullan, Semple, & Skaff, 1990; Robison, Fortinsky, Kleppinger, Shugrue, & Porter, 2009; Schulz & Sherwood, 2008; Tompkins & Bell, 2009).
This article presents method, results, and discussion regarding one survey tool, the Survey of Alabama Respite Service Providers. This survey contains 71 items in general categories: training needs—content, frequency, and format (23 items); identification of respite service providers and agencies (19 items); respite provider history (12 items); consent and demographics (9 items); and previous training and confidence (8 items). Estimated length of time to complete the survey is 30 min. Participants did not receive compensation (Geiger & O’Neal, 2012).
Respite providers support family caregivers of individuals with a wide array of needs and abilities, such as developmental disabilities and progressive physical illness. Each state and nonprofit agency determines eligibility to receive lifespan respite care according to rules established by federal, state, and private funders. Agency representatives invited respite providers to participate anonymously in the needs assessment through established service contacts. Some were paid professionals or family caregivers, whereas others were unpaid volunteer providers.
The survey was provided in different formats (printed and online forms, including large print and telephone), enabling many providers to participate. Five agencies posted announcements plus links to the online survey on homepages, and three agencies included announcements about the survey in newsletters distributed statewide. Several agencies distributed printed forms and information sheets during supervision and training events for respite providers. These methods protected privacy of individuals as university researchers did not receive lists of names and contact information. Those who desired physical assistance to participate requested this from project evaluators. The Institutional Review Board for Human Use granted expedited approval for the survey protocol.
Results
A total of 317 respite providers attempted and 191 completed the survey. Respondents could choose not to answer questions; therefore, the total number of responses varied from item-to-item. From 255 to 265 respite providers answered demographic items. Among those indicating their relationship to the individual with a disability or chronic illness, 60% are family members, 28% are paid respite workers, and 8% are volunteer respite workers or aides. The majority of respondents (69%) are White, 30% are Black, and 91% are female. The mean age of respondents is 46 years.
Respite Provider History
Between 209 and 217 participants completed items about their past respite provider experiences. Two thirds have been respite providers for more than 3 years. Responses to the question, “For how many individuals with disabilities or chronic illness did you provide respite care in 2010?” ranged between 1 and 200 (M = 8). Caregiver respite is most often provided in the family home (35%), residence of the individual with a disability or chronic illness (28%), or provider’s home (20%) as shown in Figure 1.

Places where caregiver respite is provided (n = 217).
Almost half (42%) of the respondents provided respite services daily and 26% did so weekly. The age group of those for whom participants provided the most care in 2010 was 19 to 59 years as presented in Figure 2.
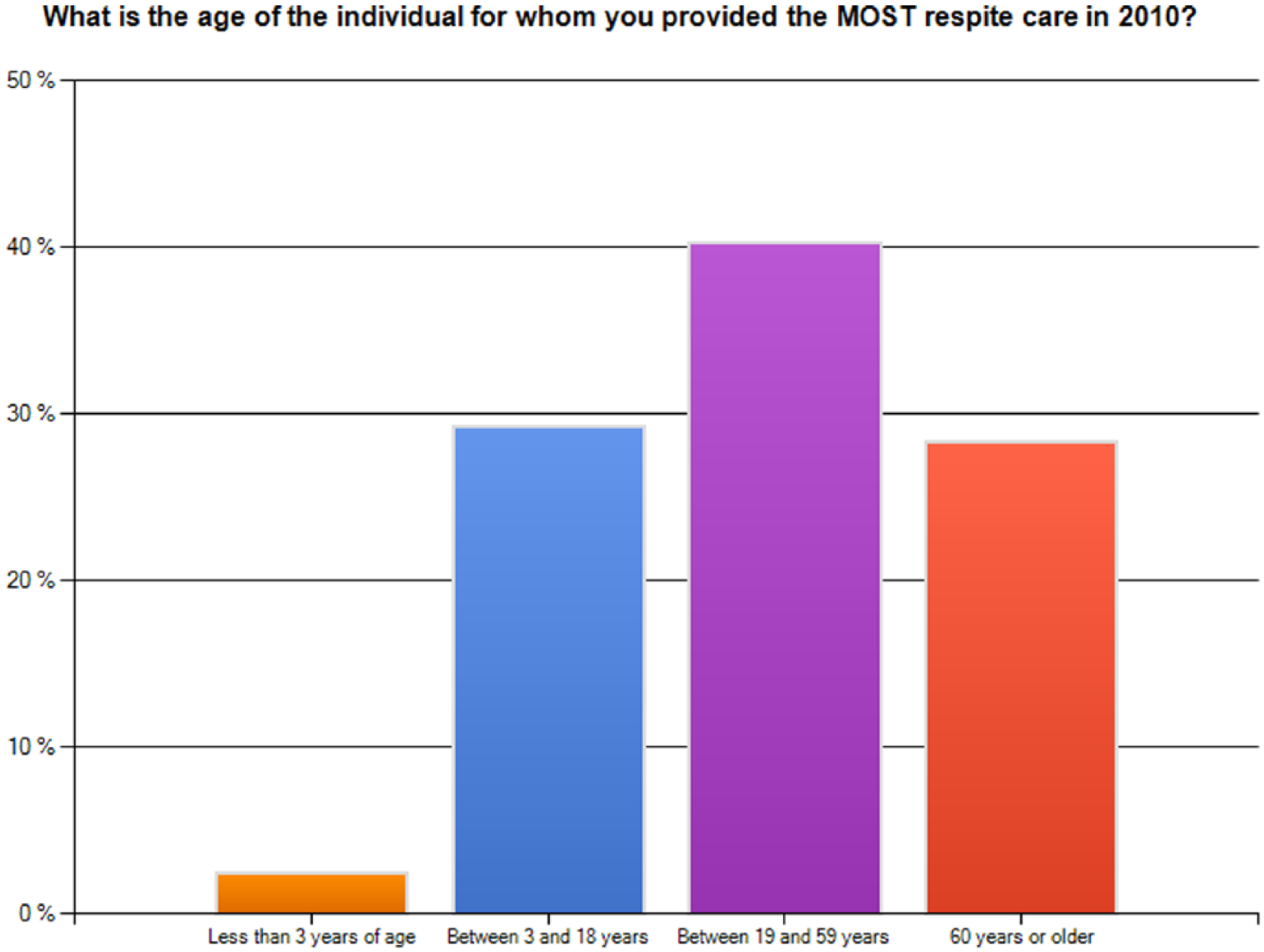
Ages of individuals who received respite care in 2010 (n = 209).
Respite service providers selected one or more commonly encountered disabilities or chronic illnesses among those they aided. As shown in Figure 3, the most frequent responses were long-term physical conditions (64%), intellectual disabilities (45%), and emotional or mental health issues (39%). Short-term physical conditions were least frequent (9%). Responses included in the Other category were autism spectrum disorder and muscular skeletal disorders (muscular dystrophy, cerebral palsy). Respite providers may experience greater demands when caring for individuals with severe cognitive impairment (intellectual disabilities, Alzheimer’s), behavioral, and functional limitations.

Most frequent disabilities or chronic illnesses encountered by respite providers (n = 216).
When asked to rate the level of difficulty you have experienced as a respite provider for a series of items, one fourth reported great difficulty “getting financial help for the individual for whom you care,” and 22% had great difficulty “locating agencies and programs offering support services.” This group of respite providers reported least difficulty “obtaining emergency assistance.”
Previous Respite Training and Confidence
Of 200 respondents who indicated whether they had completed caregiver training, 110 (55%) reported that they had done so. As Figure 4 shows, among the 104 respite providers who selected one or more types of training, the most common response was informal training from a family member or other caregiver (62%), likely about specific preferences and techniques. More formal training included orientation or other classes about respite provided by an agency (58%), conference or workshop for respite providers (39%), and online training courses or webinars (12%).

Type of training completed by respite providers (n = 104).
A total of 183 respite providers rated their confidence to complete each of five caregiver tasks. More than half were very confident to identify families in need of care (53%) and communicate to families the purpose of respite care (55%). At least 40% were somewhat confident to identify respite providers in their community, match respite service needs to available resources, and determine respite benefits for specific families.
Identification of Respite Service Providers and Agencies
When asked who they rely on for information about respite care, the majority of 186 respondents indicated three options: family, friends, and other caregivers (84%); health care providers (doctor, nurse, social worker, therapist; 62%); and the Alabama Lifespan Respite Resource Network (54%). Furthermore, at least 60% respite providers indicated which sources they had never used for information about respite: Governor’s Office on Disabilities (GOOD; 77%), Alabama Department of Education (ASDE; 73%), Veterans Administration (VA; 70%), Health InfoNet of Alabama (66%), Alabama Council for Developmental Disabilities (ACDD; 61%), and the ADSS (60%). It is important to note that a response of never used may indicate that the respite provider is unaware of the role and services of the agency, is not eligible for services, or does not know whom to contact for referral information. Although 41% said that they searched on the Internet for respite resources, 39% had not done so. Without specific knowledge of information and services that will be most helpful to families, providers may not effectively target resources to meet caregivers’ needs (Montgomery & Kwak, 2008).
Training Needs—Content, Frequency, and Format
Respite providers indicated how often they need training on each of the eight topics specific to providing direct care for individuals with disabilities or chronic illness as shown in Figure 5. Among the 191 participants responding to this item, at least 40% indicated the need for one-time training for five topics, specifically, moving and lifting, bathing and personal hygiene, handling incontinence, feeding and nutrition, and managing medications. At least 30% of providers desire annual training on four topics, that is, feeding and nutrition, managing challenging behaviors, keeping individuals safe at home (first aid, cardiopulmonary resuscitation [CPR], emergency response, fall prevention), and understanding complex care needs of individuals. Fewer providers chose the response option never. Around 24% to 28% of respondents indicated never as the desired frequency for four topics, specifically, moving and lifting, bathing and personal hygiene, handling incontinence, and managing medications. Complex care regimens and declining patient functioning increase burden on family caregivers and respite providers. Reducing caregiving burden through respite is more likely when specific needs are addressed and sufficient services are provided (Montgomery & Kwak, 2008).

Frequency of caregiver training needs by topic (n = 191).
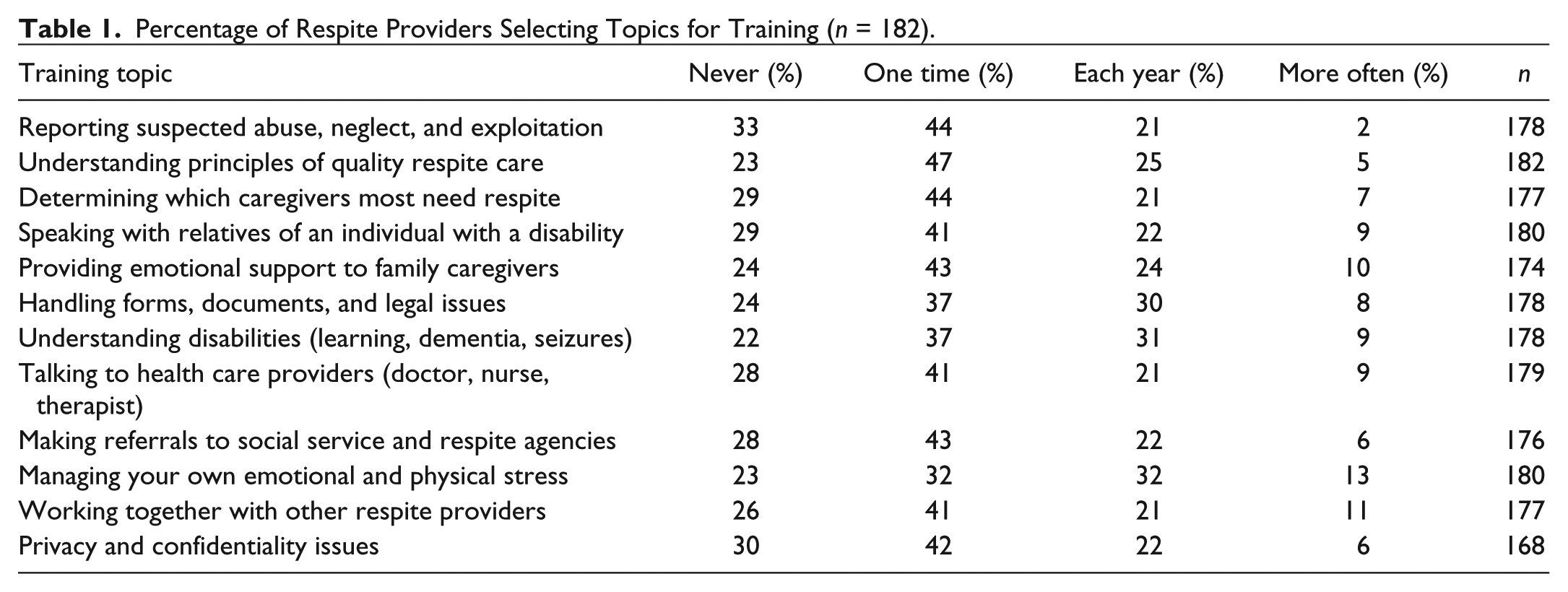
A total of 182 respite providers identified training needs for each of 12 additional topics related to respite care as shown in Table 1. One-time training was selected most frequently for nearly all topics. The four topics selected by the greatest percentage of respite providers for one-time training included understanding principles of quality respite care; reporting suspected abuse, neglect, and exploitation; determining which caregivers most need family respite; and making referrals to social service and respite agencies. At least 30% selected three topics for annual training: handling forms, documents, and legal issues; understanding disabilities (learning, dementia/Alzheimer’s, seizures); and managing their own emotional and physical stress.
Percentage of Respite Providers Selecting Topics for Training (n = 182).
When planning training for respite providers, it is necessary to consider trainees’ preferences, existing programs, and capacity. As shown in Figure 6, a total of 52% of 181 respondents prefer group training held on a weekday, and 26% desire weekend group training. Many providers appear to desire nontraditional formats for caregiver training, including online webinars (44%) and video or audiotaped programs available on demand (39%). These may represent new opportunities for the state Network to provide a service, particularly by connecting providers to existing professional development programs administered by federal, state, and nonprofit agencies. Finally, 35% chose the option, individualized training from a family or other caregiver.

Respite providers’ preferences for caregiving training (n = 181).
Finally, respite providers shared additional comments about training needs. Verbatim anonymous comments indicate the types of needs: I answered this survey as the caregiver for a 15-year-old daughter with DS [Down Syndrome] and autism, but [I] am also the caregiver for my 76-year-old mother who has had cancer and a stroke. The needs are very different for these two individuals—would like to see training tailored a little to be more specific. [I need] augmentative communication training [and] transitional training. Training for families on how to hire/select a caregiver. I think every respite worker should be trained at least once a year. My company prepares us well before sending us out. One-on-one [training] is definitely a plus. How do we teach children to play appropriately? Need ideas. Also, need to know how to regulate behavior and how to speak to them. Where do you go to find respite training? They should be specific and detailed. Our caregivers must act accordingly for many kinds of situations (e.g., Alzheimer’s, incontinence, families), and should know how to respond. I began having classes for new employees months ago. I retrain employees that come from other agencies. I want them trained right away! We are a church program with individual (one-on-one) volunteers working with children with special needs for only 4 hours each month. Our situation is a little unique in that the parents provide the training for the volunteers on their specific child. We would need little training except as it relates to behavioral issues and more information about various disabilities (autism spectrum, Down syndrome, etc.).
Limitations of the Needs Assessment
This article summarizes methods and results of a cross-sectional survey of respite service providers in a southern state conducted on behalf of a state Network. Participation was voluntary and anonymous. Results may not be generalized beyond the sample of respondents. It is possible that some providers who did not respond may have different perspectives about training needs. There are likely differences among paid professional, family, and volunteer providers that are not apparent when examining aggregate data. For instance, respite providers who live in the same household as the care recipient may experience greater social isolation and role conflict than providers from an agency or an organization (Robison et al., 2009).
Conclusion and Recommendations
The Public Health Act was amended in 2006 permitting eligible state agencies to receive support for lifespan respite services: (i) to develop or enhance lifespan respite care at the State and local levels; (ii) to provide respite care services for family caregivers caring for children or adults; (iii) to train and recruit respite care workers and volunteers; (iv) to provide information to caregivers about available respite and support services; and (v) to assist caregivers in gaining access to such services. (The Lifespan Respite Care Act, 2006)
The anticipated outcome of respite is reduced burden on families who care for relatives with disabilities and chronic conditions, reducing the need for institutional care (Phillipson & Jones, 2011; Tompkins & Bell, 2009).
A total of 317 respite providers attempted and 191 completed a survey about training needs. The typical respondent was a 46-year-old White (184), female (237) family member (157) of an individual with a disability or chronic illness. Two thirds provided respite services daily or weekly and have done so for more than 3 years. Most cared for adults less than 60 years of age with long-term physical conditions. The profile of an average respite provider in a southeastern state, who is often a family caregiver, is similar to the data from the 2009 National Caregiving Survey (NAC and AARP, 2009). It may be anticipated that mean age of caregivers including respite providers in this state and nation will increase as the population ages.
External evaluators presented to the state Network the purpose, method, and results of the respite provider needs assessment, highlighting its strengths and gaps. Results were presented within the context of related literature. Despite progress made since receipt of federal funding, there are unmet needs of caregiver respite in Alabama. There is a dearth of knowledge about experience and training needs among respite care providers. Most of the providers in this sample had not completed formal training, such as that offered by a respite agency, online training course or webinar, workshop or conference. Collins and Swartz (2011) also reported that “a majority of caregivers feel inadequately trained for the skills that they perform, having never received any formal education in caregiving” (p. 1310).
Responses to the Alabama survey revealed that many respite providers had never used and may not know of missions and services of state and local agencies providing referrals and respite services to families. The most frequently identified sources of information about respite care were informal networks (family, friends, and other caregivers), health care providers, the state Network, and websites. Perhaps there are opportunities for the state Network to focus its print, broadcast, and electronic messaging on increasing awareness among consumers about whom to contact and how to access available respite services.
More than half of this sample of respite providers found it easy to obtain emergency assistance; however, nearly one fourth experienced difficulty locating agencies and programs offering family support, and getting financial help for those for whom they care. At least 40% of the sample of respite providers needed one-time training on five topics specific to direct care of individuals with disabilities or chronic illness: moving and lifting, bathing and personal hygiene, handling incontinence, feeding and nutrition, and managing medications. Furthermore, two thirds or more desired one-time training on 11 of 12 caregiving topics, most frequently understanding principles of quality respite care; reporting suspected abuse, neglect, and exploitation; determining which caregivers most need respite; and making referrals to social service and respite agencies.
Three topics were most often requested by Alabama respite providers for annual training, that is, managing your own emotional and physical stress, understanding disabilities, and handling forms, documents, and legal issues. These are suitable topics for informal or formal training. These results may be compared with recommendations to family physicians to assess caregiving burden and encourage caregivers to use respite care, join support groups, and complete skills training (Collins & Swartz, 2011). Tompkins and Bell (2009) reported successful outcomes for participants in the Savvy Caregiver Program, including increased use of community supportive services and improved caregiver depression scores, even when financial assistance was not provided to families.
It is beneficial to compare results of parallel surveys of providers and family caregivers when planning outreach education and respite services. Nearly 900 family caregivers in the same southeastern state indicated one or more expectations for how respite services will help their family. Responses were grouped into five categories for analysis: (a) attending to family caregiver’s needs, (b) helping with activities of daily living (ADL), (c) caring for others in the family, (d) providing financial assistance to pay for respite, and (e) caregiver continuing education, providing therapies, or medical treatment (listed in rank order; Geiger & O’Neal, 2012).
Results of a 2013 national survey conducted by AARP confirmed that 17% of workers aged 45 to 74 years took time off from work to care for an adult family member. Workers in middle- and lower income families often lack financial reserves to take time off from work for caregiving; respite may reduce caregiver strain (AARP, 2013a, 2013b; Robison et al., 2009). Respite providers may need additional information and training to match services to needs of family caregivers.
Events leading to the most recent request for respite services were identified by 884 Alabama family caregivers. The four most common responses were to “relieve stress” (73%), “care for myself” (46%), “care for personal business” (31%), and “improve relationship with my spouse or partner” (30%). Some family caregivers may be reluctant to use respite services due to normative expectations that they must always care for their loved ones or due to concerns about locating competent providers capable of managing difficult behaviors (Phillipson & Jones, 2011). Roles of respite agencies include informing families of benefits of respite, their eligibility, provider qualifications and training, and service availability. Respite providers must be trained to identify caregiver burden and respond appropriately with services and referrals (Collins & Swartz, 2011).
During 2013-2015, the state Network plans to develop a directory of respite care providers by county, improve coordination among respite services across state and nonprofit agencies, expand capacity of a respite referral service for consumers, and increase training for respite volunteers (especially through faith-based organizations). More than half of the respite providers responding to the survey desired group training held on a weekday, one fourth requested weekend group training, and 4 of 10 respondents preferred online webinars and taped programs available on demand.
Furthermore, the Network has implemented Sharing the Care training programs for respite providers, building capacity within communities (Jansen et al., 2009). Training for providers includes responding to actual needs of caregivers within rules established by the program and requesting additional assistance when needed. Anticipated outcomes of successful training programs are enhancing consumer confidence and satisfaction and preparing providers to offer needed services (Byrne, Sims-Gould, Frazee, & Martin-Matthews, 2011).
The state Network may tap into existing databases of services and professional development programs provided by collaborators in other states, including (a) AARP’s Planning Guide for Families—Prepare to Care (http://assets.aarp.org/www.aarp.org_/articles/foundation/aa66r2_care.pdf), and webinars and teleconferences shared by (b) ARCH National Respite Network and Resource Center (http://arch-respite.org/webinars-and-teleconferences); (c) National Association of Social Workers (http://www.social-workers.org/sections/teleconferences/tcourses/default.aspx?returnpath=sections&type=teleconferences&;pageid=); (d) Chapel Hill Training-Outreach Project, Inc. (http://chtop.org/video-directory-on-respite-care/89-webinar-respite-in-the-faith-community); (e) Rosalynn Carter Institute for Caregiving (http://www.rosalynncarter.org/national_quality_caregiving_network/); (f) Video Caregiving (http://www.videocaregiving.org/); (g) Canadian Virtual Hospice (http://www.cana-dianvirtualhospice.ca/en_US/Main+Site+Navigation/Home/Topics/Topics.aspx); and (h) Family Care NavigatorSM hosted by the Family Caregiver Alliance™, linking caregivers to resources in their state (https://caregiver.org/family-care-navigator); and (i) conferences, respite news, and a directory of medical respite programs hosted by the National Healthcare for the Homeless Council (http://www.nhchc.org/?s=respite).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This project was funded by the U.S. Administration on Aging, HHS-2009-AOA-LR-0916, through an award to the Alabama Department of Senior Services. The authors greatly appreciate contributions from the members of the Alabama Lifespan Respite Resource Network™ and its Coalition.