
Abstract
The aims of this article were to (a) investigate whether practicing Tai Chi has an effect on stress, self-esteem, and perceived life expectancy and (b) contrast a structural model of relation between the three latter variables taking into account age. One scale to assess stress, another scale to assess perceived life expectancy, and the 10-item Rosenberg’s Self-Esteem Scale were administrated to a nonprobability sample of 86 Tai Chi practitioners and 91 sedentary persons. Tai Chi practitioners had a lower level of stress, a greater self-esteem, and a greater perceived life expectancy than sedentary persons. Self-esteem had an effect on stress and perceived life expectancy, and stress had an effect on perceived life expectancy in both Tai Chi practitioners and sedentary persons. Age was correlated to self-esteem among sedentary persons, but not among Tai Chi practitioners. Age had a direct effect on perceived life expectancy among Tai Chi practitioners, but not among sedentary persons. It is concluded that Tai Chi practice has a beneficial effect on stress, perceived life expectancy, and self-esteem.
Introduction
Exercise is a planned, structured, and repetitive physical activity, with increased energy consumption in comparison with baseline energy consumption, which aims to achieve a better functioning of the body and to improve health, body figure, performance, and/or motor skills (Center for Desease Control and Prevention, 2011). When persons systematically practice exercise they begin to experience positive effects, both physical and psychological, such as improved glycemic control, improved weight control, increased bone density, improved muscular elasticity and strength, lower levels of stress, tendency to bring blood pressure into a healthy range, better quality of sleep, and perception of increased vitality (Martins et al., 2011; Subirats, Subirats, & Soteras, 2012; Thornton, Sykes, & Tang, 2004). Constant physical activity also increases self-confidence and the sensation of well-being, and these effects are not only of general interest for general population (Campos et al., 2003; Payette et al., 2011) but also for the treatment of psychological disorders such as stress, anxiety, or depression (Lubans, Plotnikoff, & Lubans, 2012). Thus, physical activity turns out to be an excellent means of therapeutic support (Tarakci, Yeldan, Mutlu, Baydogan, & Kasapcopur, 2011).
Lopez (2009) points out that activities involving a moderate effort and relaxation can be practiced as an efficient means to achieve the prevention of premature aging and to relieve the somatic symptoms and syndromes associated to stress, such as hypertension, headache, migraine, insomnia, asthma, or allergies. It should be mentioned that the importance that people grant to exercise to increase their life expectancy, quality of life, and prevent diseases increases the probability of adherence to this habit and its incorporation as a part of a healthier lifestyle (Moral, 2011).
Among the types of exercise that can be recommended to reach the two objectives mentioned above is Tai Chi (Tarakci et al., 2011). This is an exercise consisting of soft low-impact movements, involving a high level of coordination between the movements of the body and the breathing process, as well as a high level of bodily awareness and self-consciousness. Nowadays, Tai Chi has become a popular means to improve health and obtain a longer life expectancy and, owing to this reason, it has been included in the approach to several physiological and psychological problems in some medical centers and hospitals (Nomura et al., 2011).
Tai Chi is an activity involving meditation in motion and consists of many coordination exercises which connect bodily awareness with movement, movement with breathing, and breathing with perception of vitality; Tai Chi stimulates the production of endogenous chemical compounds, such as β-endorphins (Zhang, Layne, Lowder, & Liu, 2012), which promote body relaxation, quietness, internal balance, peace of mind, and joy for life (Lan, Wolf, & Tsang, 2013).
There are many studies which have suggested that Tai Chi might be of benefit for patients living with diseases such as multiple sclerosis (Bowling, 2010), osteoarthritis (Fransen, Nairn, Winstanley, Lam, & Edmonds, 2007), cardiopathies (Taylor, Haskell, Stotts, & Froelicher, 2006), hypertension (Yeh, Wang, Wayne, & Phillips, 2008), rheumatoid arthritis (Wang, 2008), fibromyalgia (Wang et al., 2009), and sleep disorders (Irwin, Olmstead, & Motivala, 2008). In older adults, Tai Chi seems to be helpful to improve Parkinson’s disease (Hackney & Earhart, 2008) and several disorders of motor control and balance (Y. Li, Devault, & Van Oteghen, 2007). In individuals with lower-limb disabilities, it has been found that Tai Chi improves shoulder movements as well as cardiovascular and pulmonary functions (Cheung, Tsai, Fung, & Ng, 2007).
In addition to the physical benefits, Tai Chi, like other modalities of physical exercise, has positive psychological effects, such as an increase of self-esteem (Adler & Roberts, 2006; Greenspan, Wolf, Kelley, & O’Grady, 2007). It should be mentioned that self-esteem is a very important achievement in the development of every human being, because it involves harboring a positive assessment and acceptance of self and becomes a protector factor for mental health; on the contrary, a low self-esteem may be a risk factor for psycho-pathological disorders (Melendez & Rojas, 2006).
As previously mentioned, one of the psychological benefits of exercise might be the reduction of stress. Stress is a psychological phenomenon emerging from the impossibility or difficulty to satisfy the requirements or demands of the environment (Folkman, 2011). Chronic exposure to stress during extended periods produces harmful biological effects for the individual as a consequence of high levels of cortisol (McEwen, 2004). After the so-called phase of resistance, the organism develops a physiological deterioration and finally enters into a phase of exhaustion, which might lead to death. Nowadays, it can be contended that many of the common and deadly diseases are associated to stress-related disorders, for example, cardiovascular pathologies, asthma, cancer, hypertension, osteoporosis, insomnia, memory loss, and even premature aging (Folkman, 2011).
The research on the effect of Tai Chi on reduction of the levels of stress has been carried out in clinical samples, and there seems not to be studies carried out in samples from the general population. As a hypothesis, it could be anticipated that Tai Chi will reduce and prevent the effects of stress, because this modality of physical activity seems to be a protective factor against diseases associated to the physiological deregulator effects of stress (L. Y. K. Lee, Lee, & Woo, 2009).
Research has shown that Tai Chi practice extends life expectancy and is associated with greater self-esteem. Nevertheless, it has not been studied the construct ‘perceived life expectancy’, that is, if the persons believe and feel that they will enjoy for a longer period of life. Perceived life expectancy is probably influenced by stress and self-esteem. It could be asked which ones are the effects of stress and self-esteem on perceived life expectancy among persons who practice or do not practice Tai Chi.
Tai Chi is practiced by a lot of people in China. Outside of China, in Western countries, women and older adults of high–medium socioeconomic status have a greater representation among practitioners of Tai Chi (Hong, 2008). It is known that age has a depressant effect on self-esteem (Orth, Trzesniewski, & Robins, 2010) but an over-optimistic effect on the estimation of life expectancy because of the fear of death (Pew Research Center, 2008). Practicing Tai Chi among older adults could reduce this depressant effect of the age on the self-esteem (M. S. Lee, Choi, & Ernst, 2010; Mustian et al., 2004; Wang et al., 2010), could reduce the levels of stress (Wang et al., 2010), and might even provide a more realistic perceived life expectancy. To perceive the beneficial effects of Tai Chi on health, a minimum practice of 3 hr a week during 3 months is required (Hong, 2008).
The aims of this investigation are to (a) investigate whether practicing Tai Chi has an effect on stress, self-esteem, and perceived life expectancy and (b) study the influence of self-esteem on stress and perceived life expectancy, and the effect that stress has on this expectancy, specifying and contrasting a predictive model.
A lower level of stress, a higher level of self-esteem, and a greater perceived life expectancy is expected among Tai Chi practitioners than among sedentary persons, as having physical activity (Tai Chi practice vs. sedentarism) leads to a medium or large effect size on stress, self-esteem, and perceived life expectancy. Practicing exercise like Tai Chi has a modulating effect on the autonomic nervous system, and therefore the level of stress is expected to be lower among Tai Chi practitioners than among sedentary persons (Motivala, Sollers, Thayer, & Irwin, 2006). Development of motor abilities and the positive effect of Tai Chi on the mood seem to affect self-esteem, a higher level of self-esteem being expected among Tai Chi practitioners (Mustian et al., 2004). Nevertheless, the effect size of practicing Tai Chi on self-esteem could be lower than the effect on stress owing to the more complex and stable nature of self-esteem and the physiological changes of autonomic nervous system directly related to stress (McEwen, 2004). The positive effect of this activity on practitioners’ health could reinforce the belief of having a longer life expectancy; therefore, it is expected that Tai Chi practitioners experience a greater perceived life expectancy than the sedentary persons (L. Y. K. Lee et al., 2009). From these expectancies, a predictive model is proposed in which self-esteem has a direct effect on stress and perceived life expectancy, and stress has a direct effect on the perceived life expectancy.
Having been proved that self-esteem is a protective factor against stress (Motivala et al., 2006), it is expected that it will have a significant effect that will be associated to a lower level of stress both among Tai Chi practitioners and sedentary persons. Persons with greater self-esteem will probably have a deeper belief of living more years owing to the self-confidence in their abilities to have success in life and coping with difficulties. Stress being a state of emotional discomfort, it was considered that it would lead to a negative, pessimistic, and defeatist perception that would have a negative effect on perceived life expectancy.
This nonexperimental study is important because its results may support the recommendation to include Tai Chi in health prevention programs as a means to reduce stress, raise self-esteem, and increase perceived life expectancy; these latter changes might also lead to a better quality of life, as L. Y. K. Lee et al. (2009) have pointed out. The present data on stress and self-esteem complement the results obtained from previous studies in this field, which have been mostly carried out in clinical population from the United States of America; besides, the present research provides new data on perceived life expectancy.
Method
Participants
The inclusion criteria for the participants of this study were age ≥ 18 years old, to know how to read and write Spanish language, and to provide an explicit consent to participate. The additional inclusion criteria for the Tai Chi group participants were to be ascribed to a Tai Chi academy from Monterrey and its metropolitan area, in Mexico, and to have regularly attended to classes for more than 3 months. An additional criterion for the sedentary group participants was not to have practiced any sport activity in the last 5 years. The exclusion criterion was to leave four or more items or questions without an answer (this exclusion criterion did not apply to monthly incomes because many persons did not report it owing to security reasons).
The nonprobability sample of Tai Chi practitioners was composed of 86 participants. All of them had been practicing Tai Chi for more than 3 months, three times a week, an hour per class, with a structure composed by warm-up exercises, basic techniques, and forms. To recruit the group of Tai Chi practitioners, the survey takers visited 14 Tai Chi academies. These ones were randomly chosen from a list provided by the Association of Wu Shu of the State of Nuevo Leon, Mexico. The possible participants were asked whether they had been practicing Tai Chi regularly for more than 3 months. In the cases of affirmative answers, the survey takers explained the objectives and identified the responsible researchers of this investigation. Then the participants were requested to provide an explicit consent. In the first page of the questionnaire, the aims of study, content of scales, names, and institutional adscriptions of researches were provided. In this first page the informed consent was made explicit by participants (marking the appropriate box [yes/no], without signature). After the participants had finished responding the questionnaire, they deposited it in a closed box similar to the urns used in the elections of political candidates.
The nonprobability sample of sedentary persons was composed of 91 participants. To obtain the group of sedentary persons, the survey takers approached adults who were at the city’s Macroplaza Park and asked them whether they practiced any type of sport activity. In the cases of negative answers, they were asked to give their explicit consent as it has been previously explained, and the questionnaire was applied only if this consent was granted. Once they had finished responding to the questionnaire, they deposited it in a closed box.
The groups of Tai Chi practitioners and sedentary persons had a number of participants statistically equivalent (binomial test, p = .76). Likewise, both groups were statically equivalent in frequencies of sex, χ2(1, 177) = 0.65, p = .42. The total sample included 131 (74%) women and 46 (26%) men. The Tai Chi practitioners were 66 (77%) women and 20 (23%) men. The sedentary persons were 65 (71%) women and 26 (29%) men. The average age among Tai Chi practitioners was 60.12 years (SD = 10.74), and that among sedentary persons was 60.52 years (SD = 10.70). The average ages of both groups were statistically equivalent, t(175) = 0.25, p = .80. The average level of education among Tai Chi practitioners was 9.45 years (SD = 4.32), while that among sedentary persons was 7.55 years (SD = 4.39). The average level of education was significantly higher among Tai Chi practitioners than among sedentary persons, t(175) = −2.91, p < .01. The average of monthly incomes among Tai Chi practitioners (M = 13,800 Mexican pesos [around US$1,000], SD = 18,136) was significantly higher, t(57.45) = 2.48, p = .02, than that among sedentary persons (M = 6,565 Mexican pesos [around US$500], SD = 6,588).
Instruments
The questionnaire was composed of four questions about socio-demographic information (sex, age, level of education, and monthly income) and 25 items to assess the three constructs of the study: 9 items for assessing stress, 6 items for assessing perceived life expectancy, and the 10 items from the Rosenberg’s Self-Esteem Scale (RSES), in its Spanish version obtained through back-translation . The 25 items were randomly distributed and were printed in that order to avoid or reduce response biases.
The scales for assessing stress and perceived life expectancy were elaborated for this study, and their psychometric properties are shown in the section of results. The items composing these two scales proceed from the worries, fears, beliefs, and opinions more frequently expressed by participants in workshops on stress management and perceived life expectancy carried out by the authors of this article (data unpublished).
The nine items for assessing stress were, “I feel uncomfortable because other people are more competent than I am,” “I think that I have the sufficient abilities to face the challenges of my life,” “It worries me that people think that I’m a bad person,” “I feel that life demands of me more than I can comply with,” “I’m afraid of not being accepted by the others,” “I am worried about the diseases I have,” “I am worried about not having enough money for my own life,” “Thinking of coping new challenges in my life worries me a lot,” and “I have control over diseases that I suffer.”
The answers to the positively keyed items were scored with value 4 for definitively agree, 3 for agree, 2 for disagree, and 1 for definitively disagree, whereas the negatively keyed items were inversely scored with value 1 for definitively agree, 2 for agree, 3 for disagree, and 4 for definitively disagree.
The RSES was created by Rosenberg (1965) to evaluate the psychological construct of self-esteem. It is a 10-item Likert-type scale with items that are answered on a 4-point scale (from strongly agree to strongly disagree). Five of the 10 items are positively worded, and the remaining 5 items are negatively worded. The internal consistency of its 10 items ranks from 0.45 to 0.90 with an average of 0.81, and it has a factor structure of two correlated factors composed of 5 items each 1 (5 positively worded statements and 5 negatively worded statements). The total variance explained by the two factors extracted through component analysis ranks from 25% to 54%, with an average of 41% (Schmitt & Allik, 2005).
The six items for assessing perceived life expectancy were “I have a very good health,” “I have a very bad health,” “I have a lot to live ahead,” “I have few years to live,” “I feel that I’m going to live many years,” and “I feel that my life is over.”
Procedure
The eight voluntary survey takers received special training before applying the questionnaire. This study complied with the ethical norms of investigation of the American Psychological Association (2002) and was approved by the committee of Ethics of the Facultad de Organizacion Deportiva (Doctorate Committee) of the Universidad Autonoma de Nuevo Leon. Each one of the persons who participated in the survey was informed about the objectives of the investigation project and the content of the scales that composed the questionnaire. They were asked to give their explicit consent to participate after having received a brief description of the investigation project. Anonymity and confidentiality for the information supplied were guaranteed. For this reason any personal identification data were not requested.
Each participant was instructed to leave in blank those questions that they did not want to answer; however, they were encouraged to answer all the questions and check that they had not skipped any of them. The anonymity of the answers was guaranteed by not asking for personal identification data and by depositing the answered questionnaire inside a closed urn.
Analysis of Data
The Student’s t test for two independent samples was used to compare means of stress, self-esteem, and perceived life expectancy between the group of Tai Chi practitioners and the group of sedentary persons. The Levene’s test was used to contrast the equality of variances. In case of sustaining the null hypothesis of equality of variances, the pooled standard error was used to calculate the statistic of mean comparison (t test), and in case of rejection of the null hypothesis, the Satterthwaite’s approximation was used. The standardized effect size of the physical activity (Tai Chi vs. sedentarism) on stress, perceived life expectancy, and self-esteem was calculated by Cohen’s d statistic. Values of Cohen’s d statistic lower than 0.20 were interpreted as a trivial effect size, between 0.20 and 0.49 as a small effect size, between 0.50 and 0.80 as a medium effect size, and higher than 0.80 as a large effect size (J. Cohen, 1988; Ellis, 2010). Analysis of covariance (ANCOVA) was performed for statistically controlling for the effect of levels of schooling in these mean comparisons. The standardized effect size was calculated by partial eta squared (partial η2). Values of partial η2 between 0.02 and 0.14 were interpreted as a small effect size, between 0.15 and 0.34 as a medium effect size, and 0.35 or higher as a large effect size (J. Cohen, 1988; Ellis, 2010).
The internal consistency of the scales was calculated by Cronbach’s alpha coefficient. Internal consistency values equal to or greater than 0.70 were considered high, equal to or greater than 0.60 were considered acceptable, and lesser than 0.60 were considered low.
The path analysis was employed to contrast a model of predictive relations among the variables of stress, perceived life expectancy, and self-esteem. Confirmatory factor analysis was employed to validate the measurement models for scales of stress, self-esteem, and perceived life expectancy. The discrepancy function was estimated by maximum likelihood (ML). Ten fit indexes were considered: Pearson’s chi-square test (χ2), quotient between chi-square statistic and its degrees of freedom (χ2/df), Joreskög–Sorböm goodness of fit index (GFI), Joreskög–Sorböm adjusted goodness of fit index (AGFI), Bentler–Bonett normed fit index (NFI), Bentler’s comparative fit index (CFI), minimum value of discrepancy function (FMIN), quotient between non-centrality parameter and sample size (F0) and Steiger–Lind root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMS). The following criteria were stipulated for defining close fit to the data: p > .05 for chi-square test; χ2/df ≤ 2; FD and F0 ≤ ¼ values corresponding to independent model; GFI ≥ 0.95; AGFI, NFI, and CFI ≥ 0.90; and RMSEA and SRMS ≤ 0.05. The criteria for defining acceptable fit to the data were p > .01 for chi-square test; χ2/df ≤ 3; FD and F0 ≤ 1/3 values corresponding to independent model; CFI ≥ 0.85; AGFI, NFI, and CFI ≥ 0.80; and RMSEA and SRMS ≤ 0.08. The fulfillment of assumption of multivariate normality was assessed through the standardized value of Mardia’s multivariate kurtosis; a value higher than 10 was considered as indicator of deviation from multivariate normality. In case of unfulfillment of the assumption of multivariate normality, bootstrap procedures were used (bias-corrected percentile method for contrasting the statistical significance of estimated parameters and Bollen–Stine bootstrap probability for contrasting the goodness of fit of the model). Standardized (direct and indirect) effect sizes of structural weights were calculated; values lower than 0.10 reflected a trivial effect, between 0.10 and 0.29 a small effect, between 0.30 and 0.49 a medium effect, and equal or higher than 0.50 a large effect (Kline, 2010).
The missing values of each variable were substituted by the mean of the corresponding variable. In the case of the variable related to monthly incomes, this substitution was not considered adequate because approximately 50% of the participants did not report this information. The statistical analysis was performed with SPSS (Version 21) and AMOS (Version 16).
Results
Internal Consistency and Factor Structure of the Three Used Scales
One-factor measurement models were defining and contrasting for the scales of stress, self-esteem, and perceived life expectancy through confirmatory factor analysis using ML method. The analyses were done in the total sample of 177 participants.
The one-factor model for the nine-item stress scale had a close fit to the data: χ2(27, N = 177) = 24.57, p = .60, χ2/df = 0.91, GFI = 0.97, AGFI = 0.95, NFI = 0.94, CFI = 1, FD = 0.14 (FDIM = 2.38), F0 < 0.01 (F0IM = 2.18), RMSEA < 0.01, and SRMS = 0.04. Mardia’s multivariate kurtosis was 22.08, and its standardized value was 10.44, so that the assumption of multivariate normality was unfulfilled, and thus it was necessary to apply bootstrap procedures. Bollen–Stine bootstrap probability, extracting 2,000 bootstrap samples, showed also a close fit to the data. The model fit better in 433 bootstrap samples and fit worse in 1,567 bootstrap samples than in the observed sample (Bollen–Stine bootstrap, p = 1,567/2,000 = 0.78). The 18 estimated parameters were statistically significant for both ML and bias-corrected percentile methods. The measurement weights for the nine items ranged from 0.34 to 0.75 with a mean of 0.57 (estimated by ML method).
The internal consistency of 10 items of the self-esteem scale was high (α = .72). The five positively keyed items also had a high internal consistency (α = .76). The negatively keyed five items had a low internal consistency (α = .56); their internal consistency was increased with the deletion of the item “I feel I do not have much to be proud of” (α = .63), but it still remained lower than 0.70. The model of two correlated factors (with five indicators for each one of two factors) had an acceptable fit to the data. Mardia’s multivariate kurtosis was 79.52, and its standardized value was 34.15, so that the assumption of multivariate normality was unfulfilled, and thus it was necessary to apply bootstrap procedures. Seven indexes showed a close fit to the data (Bollen–Stine bootstrap probability = 537/2,000 = 0.27, χ2/df = 1.70, AGFI = 0.91, CFI = 0.94, FMIN = 0.33 [FMIN of the independence model = 2.55], F0 = 0.14 [F0 of the independence model = 2.30], and RMSEA = 0.06, 90% CI [0.03, 0.09], p = .21 for H0: RMSEA ≤ 0.05), 2 indexes showed an acceptable fit (GFI = 0.94, SRMS = 0.06), and 2 indexes showed a bad fit, χ2(34, N = 177) = 57.72, p < .01, NFI = 0.87. The 21 estimated parameters of the model were statistically significant for both ML and bias-corrected percentile methods, excepting the item that had exhibited problems of internal consistency. The measurement weights for the 10 items ranged from 0.14 to 0.79 with a mean of 0.57 (estimated by ML method). With the specification of one modification (one correlation between two measurement residuals), the fit to the data was close: Bollen–Stine bootstrap probability = 946/2,000 = 0.47, χ2(33, N = 177) = 46.55, p = .06, χ2/df = 1.41, GFI = 0.95, AGFI = 0.92, NFI = 0.90, CFI = 0.97, FMIN = 0.26 (FMIN of the independence model = 2.55), F0 = 0.08 (F0 of the independence model = 2.30), and RMSEA = 0.05 (90% CI = [0, 0.08], p = .51 for H0: RMSEA ≤ 0.05), and SRMS = 0.05. The fit of the modified model was significantly better than the fit of the model without the correlation between two structural residuals, Δχ2(1, N = 177) = 11.17, p < .01. The 22 estimated parameters of the modified model were statistically significant for both ML and bias-corrected percentile methods. The measurement weights for the 10 items ranged from 0.13 to 0.81 with a mean of 0.57 (estimated by ML method).
The one-factor model for the six-item scale of perceived life expectancy, modified with a correlation between two residuals (corresponding to Items 2 and 5), had a data fit from acceptable, χ2(8, N = 177) = 16.94, p = .03, χ2/df = 2.12, and RMSEA = 0.08 (90% CI [0.02, 0.13], p = .16 for H0: RMSEA ≤ 0.05) to close (GFI = 0.97, AGFI = 0.93, NFI = 0.95, CFI = 0.97, FD = 0.10 [FDIM = 1.84], F0 = 0.05 [F0IM = 1.75], and SRMS = 0.04). Mardia’s multivariate kurtosis was 29.35, and its standardized value was 19.93, so that the assumption of multivariate normality was unfulfilled, and thus it was necessary to apply bootstrap procedures. Bollen–Stine bootstrap probability, extracting 2,000 bootstrap samples, showed a close fit. The model fit better in 1,455 bootstrap samples and fit worse in 545 bootstrap samples than in the observed sample (Bollen–Stine bootstrap p = 545/2,000 = 0.27). The 12 estimated parameters were statistically significant for both ML and bias-corrected percentile methods. The measurement weights for the six items ranged from 0.56 to 0.80 with a mean of 0.64 (estimated by ML method).
The internal consistency of the nine items of stress was high in the three samples (0.81 total sample, 0.83 sedentary persons, and 0.71 Tai Chi practitioners), the internal consistency of the 10 items of self-esteem was high in the total sample (0.72) and sedentary persons (0.71) and acceptable in Tai Chi practitioners (0.64), and the internal consistency of the six items of perceived life expectancy was also high in the three samples (0.82 total sample, 0.82 sedentary persons, and 0.71 Tai Chi practitioners). Therefore, the three used scales were reliable in the three samples.
Mean Difference Between Tai Chi Practitioners and Sedentary Persons
The scores of the three scales were obtained by means of the sum of their items (9 items for stress, 10 items for self-esteem, and 6 items for perceived life expectancy). After dividing the sum score of each scale by its number of items, the ranges of the three scales were reduced to a continuum from 1 to 4. To interpret this continuum of values, the scores were grouped in four intervals of constant amplitude ([maximum score on an item − minimum score on an item] / number of intervals = [4 − 1] / 4 = 0.75) to make them correspond to the four discrete values of answers of the items. In this way, it was possible to interpret these intervals from the item answer labels: from 1 to 1.74 (discrete value 1 = definitively disagree), from 1.75 to 2.49 (discrete value 2 = disagree), from 2.50 to 3.24 (discrete value 3 = agree), and from 3.25 to 4 (discrete value 4 = definitively agree).
The mean of stress scale among the sedentary persons was 2.06 (95% CI [1.92, 2.20]) and among the Tai Chi practitioners was 1.67 (95% CI [1.57, 1.78]), this difference being statistically significant, t(163.79) = 4.33, p < .01. The standardized effect size of the physical activity (Tai Chi vs. sedentarism) on stress was medium (−0.66, 95% CI [−0.95, −0.35]) by Cohen’s d statistic. The participants who practice Tai Chi presented lower level of stress than the sedentary participants. The mean of Tai Chi practitioners was within the interval “definitively disagree” (absence of stress) and the mean of sedentary persons was within the interval “disagree,” which could be interpreted as low level of stress, probably with no clinical relevance (Figure 1).

Graph of means of stress, self-esteem, and perceived life expectancy for the two compared groups.
The mean of self-esteem scale among the sedentary persons was 3.23 (95% CI [3.14, 3.33]) and among the Tai Chi practitioners, it was 3.52 (95% CI [3.45, 3.60]), this difference being statistically significant, t(168.27) = −4.76, p < .01. The standardized effect size of the physical activity (Tai Chi vs. sedentarism) on self-esteem was medium (0.71, 95% CI [0.40, 1.01]) by Cohen’s d statistic. The participants who practice Tai Chi presented higher self-esteem than the sedentary participants. The mean of Tai Chi practitioners was within interval “definitively agree,” which corresponds to the highest level of self-esteem, and mean of sedentary persons was within interval “agree,” which corresponds to a high level of self-esteem (Figure 1).
The mean of the perceived life expectancy scale among the sedentary persons was 3.18 (95% CI [3.05, 3.31]) and that among the Tai Chi practitioners was 3.52 (95% CI [3.43, 3.61]), this difference being statistically significant, t(157.01) = −4.30, p < .01. The standardized effect size of the physical activity (Tai Chi vs. sedentarism) on the perceived life expectancy was medium (0.63, 95% CI [0.33, 0.94]) by Cohen’s d statistic. The participants who practice Tai Chi expressed higher perceived life expectancy than the sedentary participants. The mean of Tai Chi practitioners showed a definitive agreement with the concept that exercising is a means to prolong own life and the mean of sedentary persons showed an agreement that was not definitive with this concept (Figure 1).
The mean differences of levels of schooling and monthly incomes between the two groups were statistically significant. This way, it was necessary to statistically control these two variables to verify whether the mean differences continue being significant. The monthly incomes were not taken into account owing to the high number of missing values and suspicion of little reliability. After controlling statistically the levels of schooling, the three differences continued being significant: stress, F(1, 174) = 12.12, p < .01, with a small effect size (partial η2 = 0.07); self-esteem, F(1, 174) = 15.80, p < .01, with a small effect size (partial η2 = 0.08); and perceived life expectancy, F(1, 174) = 11.53, p < .01, with a small effect size (partial η2 = 0.06). The levels of schooling had significant effect, as a covariate in the general lineal model, on stress, F(1, 174) = 17.88, p < .01; self-esteem, F(1, 174) = 14.31, p < .01; and perceived life expectancy, F(1, 174) = 20.99, p < .01, with small effect sizes (partial η2 = 0.09, 0.08 and 0.11, respectively).
Predictive Model From a One-Group Analysis (Total Sample)
In both groups, the same model was contrasted. The exogenous (not explained by the model) variable self-esteem predicted the level of stress and perceived life expectancy. The endogenous (explained by the model) variable stress predicted perceived life expectancy. The three variables were specified as manifest variables (sum score). Because the model did not have degrees of freedom, the age was introduced as an exogenous manifest variable. Age predicted the perceived expectancy life and correlated to self-esteem, and thus the model had one degree of freedom. It is expected that self-esteem declines with age.
In the total sample of 177 participants, the standardized value of Mardia’s multivariate kurtosis was 2.01, and therefore it was not necessary to use bootstrap procedures for complementing the estimations of parameters and fit indexes.
All the parameters were significant by ML estimation. It was explained by 49% of variance of perceived life expectancy and 52% of variance of stress. The standardized direct effect of self-esteem on stress was large (β = −.72) and medium on perceived life expectancy (β = .35). The standardized indirect effect of self-esteem on perceived life expectancy (mediated by stress) was small (β = .27), giving a large total effect size of self-esteem on perceived life expectancy (β = .62). The standardized direct effect of stress on perceived life expectancy was medium (β = −.37) and that of age was small (β = −.13). The magnitude of relationship between self-esteem and age was small (r = −.16; Figure 2).

Model with standardized parameters calculated by maximum likelihood in the total sample (one-group analysis).
The null hypothesis of goodness of fit was sustained by the chi-square statistic, χ2(1, N = 177) = 0.15, p = .70. All other indexes showed a close fit to the data: χ2/df = 0.15, GFI = 1, AGFI = 0.99, NFI = 0.99, CFI = 1, FMIN < 0.01 (FMIN of the independence model = 1.42), F0 < 0.01 (F0 of the independence model = 1.39), RMSEA = 0 (90% CI = [0, 0.15], p = .76 for H0: RMSEA ≤ 0.05), and SRMS = 0.01 (Table 1).
Fit Indexes to Test the Invariance of the Predicted Model Between Sedentary Persons and Tai Chi Practitioners Using Nested Models in Constrains.
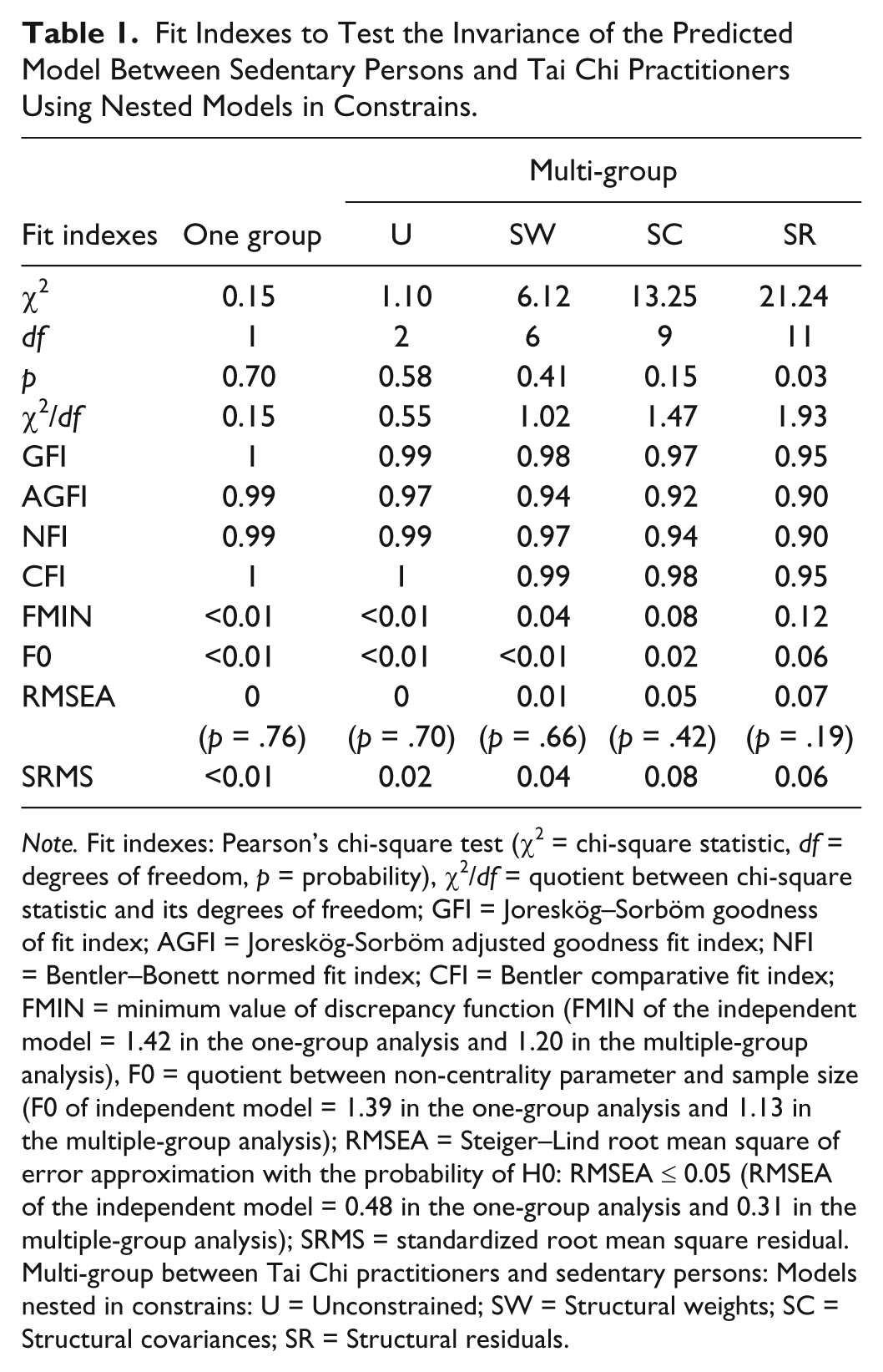
Note. Fit indexes: Pearson’s chi-square test (χ2 = chi-square statistic, df = degrees of freedom, p = probability), χ2/df = quotient between chi-square statistic and its degrees of freedom; GFI = Joreskög–Sorböm goodness of fit index; AGFI = Joreskög-Sorböm adjusted goodness fit index; NFI = Bentler–Bonett normed fit index; CFI = Bentler comparative fit index; FMIN = minimum value of discrepancy function (FMIN of the independent model = 1.42 in the one-group analysis and 1.20 in the multiple-group analysis), F0 = quotient between non-centrality parameter and sample size (F0 of independent model = 1.39 in the one-group analysis and 1.13 in the multiple-group analysis); RMSEA = Steiger–Lind root mean square of error approximation with the probability of H0: RMSEA ≤ 0.05 (RMSEA of the independent model = 0.48 in the one-group analysis and 0.31 in the multiple-group analysis); SRMS = standardized root mean square residual. Multi-group between Tai Chi practitioners and sedentary persons: Models nested in constrains: U = Unconstrained; SW = Structural weights; SC = Structural covariances; SR = Structural residuals.
The statistical power of the contrast for the RMSEA was very high (φ = 0.99). The program developed by Preacher and Coffman (2006) was used to calculate this value. It was specified a significant level of .05, 1 degree of freedom, and a sample size of 177. The null hypothesis for the RMSEA was 0 (mean value of the specified model) and the alternative hypothesis for the RMSEA was 0.48 (mean value of the independent model).
Invariance of Model Between Sedentary Persons and Tai Chi Practitioners (Multiple-Group Analysis)
Four models nested in constrictions of parameter equality (between both groups) were specified: one unconstrained model and three models with cumulated constrains (in structural weights, structural covariances, and structural residuals), following Byrne’s (2008) recommendations.
The standardized values of Mardia’s multivariate kurtosis were lower than 2 in the group of sedentary persons (0.69) and in the group of Tai Chi practitioners (0.34). For this reason, it was not necessary to use bootstrap procedures for complementing the estimations of parameters and fit indexes.
All the parameters of the unconstrained model were significant in both groups by ML estimation, except the correlation between self-esteem and age among Tai Chi practitioners (r = −.05, covariance = −0.18, standard error = 0.41, Z = −0.45, p = .66; Figure 3) and the prediction of perceived life expectancy by age among sedentary persons (β = −.10, B = −0.006, standard error = 0.004, Z = −1.35, p = .18; Figure 4). The former parameter was significant in the constrained structural weight model (β = −.13, B = −0.007, standard error = 0.003, Z = −2.48, p = .01) and the latter parameter in the constrained structural covariances model (r = −.16, covariance = −0.71, standard error = 0.33, Z = −2.13, p = .03).

Unconstrained model with standardized parameters calculated by maximum likelihood in the group of Tai Chi practitioners (multiple-group analysis).

Unconstrained model with standardized parameters calculated by maximum likelihood in the group of sedentary persons (multiple-group analysis).
From ML estimation, in the unconstrained model of the group of Tai Chi practitioners, the standardized direct effect of self-esteem on stress was large (β = −.62) and that on perceived life expectancy was medium (β = .31). The standardized indirect effect of self-esteem on perceived life expectancy (mediated by stress) was small (β = .17), giving a medium total effect size of self-esteem on perceived life expectancy (β = .48). The standardized direct effects of stress and age on perceived life expectancy were small (β = −.27 and −.17, respectively). The magnitude of relationship between self-esteem and age was trivial and nonsignificant (r = −.05; Figure 3).
From ML estimation, in the unconstrained model of the group of sedentary persons, the standardized direct effect of self-esteem on stress was large (β = −.72) and that on perceived life expectancy was medium (β = .33). The standardized indirect effect of self-esteem on perceived life expectancy (mediated by stress) was small (β = .29), giving a large total effect size of self-esteem on perceived life expectancy (β = .62). The standardized direct effect of stress on perceived life expectancy was medium (β = −.40) and that of age was small and nonsignificant (β = −.10). The magnitude of relationship between self-esteem and age was small (r = −.25; Figure 4).
In the unconstrained model, the null hypothesis of goodness of fit was maintained by the Chi-Square statistic, χ2(2, N = 177) = 1.10, p = .58. Also all other indexes showed a close fit to the data: χ2/df = 0.55, GFI = 0.99, AGFI = 0.97, NFI = 0.99, CFI = 1, FMIN < 0.01 (FMIN of the independence model = 1.20), F0 < 0.01 (F0 of the independence model = 1.13), SRMS = 0.02, and RMSEA = 0 (90% CI [0, 0.13], p = .70 for H0 = RMSEA ≤ 0.05). The goodness of fit of the unconstrained model was statistically equivalent to the goodness of fit of constrained models in structural weights, Δχ2(4, N = 177) = 5.02, p = .29, and structural covariances, Δχ2(7, N = 177) = 12.15, p = .10. Also the goodness of fit was statically equivalent between constrained models in structural weights and structural covariances, Δχ2(3, N = 177) = 7.14, p = .07. The constrained model in structural residuals was the one that had the worst fit to the data. Nevertheless, with a significance level of .01, its goodness of fit could be considered statistically equivalent to unconstrained model, Δχ2(9, N = 177) = 20.14, p = .02; constrained model in structural weights, Δχ2(5, N = 177) = 15.12, p > .01; and constrained model in structural covariances, Δχ2(2, N = 177) = 7.99, p = .02; Table 1.
The statistical power for the RMSEA was very high (φ = 1). It was specified a significant level of .05, 18 degrees of freedom, and a sample size of 86 (group of Tai Chi practitioners) or 91 (group of sedentary persons). The null hypothesis for the RMSEA was 0 (mean value of the unconstrained model) and the alternative hypothesis was 0.31 (mean value of the independent model).
Discussion
In what follows, the data are discussed in the same order in which the objectives were laid out to give answers to the questions that are implicit in them, observing whether data support the answers given in advance (hypotheses) with the limitations of a nonexperimental study with a cross-section design and nonprobability sampling.
Effect of Practicing Tai Chi on Stress, Self-Esteem, and Perceived Life Expectancy
As it was expected, a significant effect of Tai Chi on stress, perceived life expectancy, and self-esteem was found in the two nonclinical samples of the present study (Dechamps, Lafont, & Bourdel, 2007; Wang et al., 2010). The effect size of this physical activity was medium on the three variables (without controlling level of schooling that was a differential variable between two groups).
It is known, from other research, that stress is directly influenced by physical activity, which modulates the sympathetic and parasympathetic activities, and this way physical activity allows a greater balance between these two functional branches of autonomic nervous system and improves the general parameters of health in several medical conditions (Motivala et al., 2006). Physical activity has a modulating effect on mood (Peluso & Guerra-de-Andrade, 2005). This latter effect, in conjunction with the enhancement of the general parameters of health, could lead to a greater perceived life expectancy. The positive effect of Tai Chi practice on self-esteem has been also found in other clinical studies that have used an experimental design (Mustian et al., 2004; Wang et al., 2010). As Hill and Buss (2006) point out, self-esteem is derived from an integration of the life experiences of the individual in a coherent, significant, and positive image. The Tai Chi practice, as part of individual experience, allows developing a greater self-efficacy for improving his or her health status and motor skills, and allows reaching a greater sense of control on the own life expectancy. In relation to this greater sense of control, F. Li et al. (2005), in an experimental research, demonstrated that Tai Chi decreases the number of falls and the risk for falling in older adults. The accidents due to falls are a worry for older adults and health systems; thus, the greater level of motor control and muscle tone achieved through the Tai Chi practice, compared with sedentary older adults, are a source of self-esteem and well-being (Bunn, Barnet-Page, McInnes, Dickinson, & Horton, 2008).
The enhancing effect of Tai Chi practice on self-esteem is well established by experimental studies (M. S. Lee et al., 2010; Mustian et al., 2004; Wang et al., 2010). Nevertheless, self-esteem being a stable variable that forms part of personality, the greater level of self-esteem could also be a cause (motivation) and not just an effect of Tai Chi practice in older adults from the general population. This possibility needs further research. The present study, because it is not experimental, does not allow resolving this issue, and there is no research about this possible path.
The two groups of participants in this nonexperimental study were paired in the socio-demographic variables of sex and age; they differed in levels of schooling and monthly incomes, which are two variables related to stress (S. Cohen, Doyle, & Baum, 2006; Folkman, 2011), self-esteem (McMullin & Cairney, 2004; Mruk, 2006), and life expectancy (Alves & Rodrigues, 2005; Hancock, 2010). Lower levels of schooling and monthly incomes are related to higher level of stress, lower level of self-esteem, and lower life expectancy. The group of sedentary persons had lower levels of schooling and lower monthly incomes than the group of Tai Chi practitioners. Thus, the higher level of stress and the lower levels of self-esteem and perceived life expectancy among the sedentary persons might be attributed to the socio-demographic variables of schooling and incomes. To rule out this possibility, it was necessary to statistically control these two socio-demographic variables. The variable monthly income was disregarded before performing the statistical control owing to its questionable reliability and high number of missing values. Nonetheless, the variable level of schooling, closely related to monthly income (U.S. Department of Commerce, Bureau of the Census, 2013), was reliable and did not have missing values, being useful for statistical control. After statistically controlling for levels of schooling, the three differences remained significant. Therefore, despite the limitations of the study regarding the lack of pairing between sedentary persons and Tai Chi practitioners in levels of education and monthly incomes, the effect of the Tai Chi practice on the three variables remained significant. In other words, statistical analysis allowed overcoming the limitation introduced by the lack of pairing of the two groups in levels of schooling and monthly incomes.
Contrast of a Structural Model of the Effect of Self-Esteem on Stress and Perceived Life Expectancy, and the Effect of Stress on Perceived Life Expectancy
The specified model proposes that self-esteem, which is a relatively stable and persistent variable, has a direct effect on stress (protector effect) and perceived life expectancy (enhancing effect); besides, the model proposes that stress has a direct effect on perceived life expectancy (decreasing effect). Consequently, because self-esteem is a determinant variable of stress, self-esteem might also have an indirect effect (mediated by stress) on perceived life expectancy, expecting an enhancing effect. Besides these three paths, the model posits that age has a direct effect on perceived life expectancy (decreasing effect) and is negatively correlated to self-esteem. This model was valid for the total sample, in other words, showed a close fit to the data after pooling sedentary persons and Tai Chi practitioners in one sample. In accordance with hypotheses, the four direct paths were significant, as well as the indirect path and the correlation between age and self-esteem.
After studying the invariance of this structural model between Tai Chi practitioners and sedentary persons, using models nested in constraints of equality of parameters, the 10 indexes showed a close fit in the four models, except 2 indexes that showed an acceptable fit in the model with stricter constraints. In this latter model (constrained in structural residuals), all the parameters were significant, and its fit was statistically equivalent to the fit of the other three models with a significant level of .01. In the unconstrained model, although all indices showed a close fit to the data, two parameters were not significant (the total effect of age on perceived life expectancy in the group of sedentary persons and the correlation between age and self-esteem in the group of Tai Chi practitioners). These two parameters were significant only after applying the corresponding constraint (the former after constraining the structural weights and the latter after constraining the structural covariances). Therefore, the model has very adequate properties of invariance among Tai Chi practitioners and sedentary persons. It should be pointed out that there are two little differential aspects between sedentary persons and Tai Chi practitioners. What are these two differences?
In the group of Tai Chi practitioners, age was independent of self-esteem; in contrast, self-esteem decreased with age among sedentary persons, as it is observed in research carried out in general population (Orth et al., 2010). In agreement with the hypothesis of beneficial effect of Tai Chi, Tai Chi practice had an effect on self-esteem, preventing its diminution with age (nonsignificant correlation). Even the level of self-esteem among Tai Chi practitioners was significantly higher than that among sedentary persons (mean comparison), without this difference being attributed to higher level of schooling among Tai Chi practitioners, as ANCOVA showed.
In the group of Tai Chi practitioners, age had a significant effect on perceived life expectancy, decreasing with aging; in contrast, it was independent among sedentary persons. The Pew Research Center (2008) carried out a research in U.S. older adults from general population and reported discrepancies among expectations and real data. The participants perceived themselves as younger than they were; the age of start of aging and the years left to live increased as the participants grow older. This discrepancy might be attributed to the fear of death and the desire of a healthy long life. The fact that the depressant effect of age on perceived life expectancy was statistically significant among Tai Chi practitioners, but not among sedentary persons, might be due to lesser fear of aging and loss of health with age among Tai Chi practitioners than among sedentary persons. The self-confidence allows coping with these developmental fears (Erikson, 1997). The Tai Chi practice might increase both self-esteem and self-confidence to cope aging and death, which is consistent with the effect of Tai Chi on psychological well-being, as it was found in a meta-analysis performed by Wang et al. (2010); this issue requires further research.
Limitations
Even though this study is not an experiment, with measurements taken before and after the treatment and random assignment of participants to the experimental group and control group, the fact that both groups were paired in the socio-demographic variables of sex and age and that level of schooling was statistically controlled gives validity to the significant effects of Tai Chi on stress, self-esteem, and perceived life expectancy. These significant effects are in agreement with the hypothesis derived from experimental studies (Dechamps et al., 2007; Mustian et al., 2004; Wang et al., 2010).
This study selected sedentary persons as the comparison group to have a case that was opposite to the situation of Tai Chi practice, thus being more probable to attribute the differences to such activity, because both groups were paired in the socio-demographic variables relevant to stress (S. Cohen et al., 2006; Folkman, 2011), self-esteem (McMullin & Cairney, 2004; Mruk, 2006), and perceived life expectancy (Alves & Rodrigues, 2005; Hancock, 2010). The sample cannot be considered small. The proportion of number of participants and parameters to be estimated (N:q) was 14:1, what represents an acceptable proportion with a significant effect on statistical power (Jackson, 2003), as it was reflected by the statistical power calculated for the RMSEA.
The findings of this study are important with respect to other studies made in this field. Most of them have been made with experimental designs in clinic-based settings, using a small sample size, and although they possess the strength of internal validity, in the sense of a greater certainty in the causal link between the independent and the dependent variables, they lack the necessary external validity to generalize the findings toward the population from which their samples were extracted. Even though the study was carried out with a nonprobability sampling, it can be said that it has enough ecologic validity, because the Tai Chi group belongs to the nonclinical, “natural” population of regular Tai Chi practitioners, mainly older women.
Conclusion
Tai Chi practitioners who participated in this nonexperimental research (mainly older women) had a lower level of stress, higher level of self-esteem, and greater perceived life expectancy than sedentary participants. The effect sizes of practicing Tai Chi on stress, self-esteem, and perceived life expectancy were medium without statistically controlling the level of schooling, but were small when level of schooling was statistically controlled (covariable differential between two groups). From the hypotheses of the beneficial effects of Tai Chi practice, a model was specified in which self-esteem had a direct effect on stress and perceived life expectancy, stress had a direct effect on perceived life expectancy, and age had a direct effect on perceived life expectancy and correlated to self-esteem. This model showed a close fit to the data in the total sample (without considering the variable practicing or not practicing Tai Chi). The properties of invariance of this model between Tai Chi practitioners and sedentary persons (considering the variable practicing or not practicing Tai Chi) were very acceptable. It should be pointed out that, in the unconstrained model, the direct effect of age on perceived life expectancy was not significant among sedentary persons, but this effect was significant among Tai Chi practitioners and became significant in both groups once the structural weights were constrained. This reflects the protective effect of Tai Chi practice on self-esteem during aging. In Tai Chi practitioners, the correlation between self-esteem and age was not significant, but this correlation was significant among sedentary persons and became significant in both groups once the structural covariances were constrained. This might reflect the enhancing effect of Tai Chi practice on self-confidence to cope with aging and fear of death.
Recommendations
Tai Chi practice for older adults is suggested as an effective means to reduce stress, increase self-esteem, and create a greater perception of life expectancy. It might be that those persons with greater self-esteem might be more willing to practice Tai Chi. Therefore, the role of the self-esteem as an antecedent (motivation) of the Tai Chi practice requires further research in older adults from the general population. The nonexperimental design of the present research does not allow clarifying this issue. Contrary to the formulated hypothesis, Hong (2008) found that common motivations for practicing Tai Chi among Western practitioners are to treat physical illnesses (v gr., cancer), psychosomatic diseases (v gr., irritable bowel), or mental disorders (v gr., anxiety disorder).
Finally, it is recommended to include Tai Chi practice in public health programs to widen its scope to whole population of older adults. Probably, the free access to the groups of Tai Chi practice could make the mean differences in levels of schooling and monthly incomes disappear when the comparisons between Tai Chi practitioners and sedentary persons are done in future research.
Although the used instruments of assessment had high internal consistency as well as construct and content validity, in the replication of this study the stress could be evaluated by means of a more frequently used measurement instrument, for instance the Perceived Stress Scale, which would allow that the data were more comparable with other research (S. Cohen & Janicki-Deverts, 2012).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.