
Abstract
This qualitative descriptive study explores the stress experiences, appraisal, and coping strategies of newly graduated nurses. The transition to professional practice is inherently stressful, and based on the transactional theory of stress and coping, effective appraisal and coping are crucial for stress management. Semi-structured interviews were conducted with 23 NGNs, and data were analyzed using qualitative content analysis until saturation was achieved. The findings revealed three major themes: (1) primary appraisal: highlighting stressors related to work task and interpersonal relationships; (2) secondary appraisal: involving internal and external resources; and (3) coping: including problem-focused and emotion-focused coping. Notably, problem-focused coping was identified as more sustainable, whereas emotion-focused coping was often short-term and required reflection and replacement. The study concludes that targeted occupational psychoeducation and robust support systems are essential to enhance NGNs’ stress appraisal and coping capacities. Nursing managers should promote positive problem-focused coping and address short-term emotion-focused coping through reflective practice and training. These insights are highly relevant for clinical practice, emphasizing the need to reduce NGNs’ stress by focusing on appraisal processes and fostering effective coping mechanisms.
Plain Language Summary
Starting out as a newly graduated nurse is a stressful time. This study interviewed 23 new nurses to understand their stress, how they handle it, and what helps them cope. We found their main stresses come from heavy workloads and challenges with workplace relationships. To manage this stress, nurses use a mix of their own inner strength and support from colleagues and family. They also use different coping strategies: directly tackling problems (which works well long-term) and managing their emotions (which helps short-term but may need to be replaced with more sustainable approaches). The study concludes that hospitals should provide better training and support systems to help new nurses develop effective, long-term coping skills, focusing on problem-solving and reflecting on their emotional responses.
Background
Newly graduated nurses (NGNs) refer to nurses who are engaged in clinical work within one year after graduation (Doughty et al., 2018). Studies have revealed that nursing is a stressful profession worldwide, and the transition from student to nurse is particularly demanding and occurs under tremendous pressure. Studies have revealed that NGNs encounter multifaceted stressors, including excessive workload, experiences with patient death and dying, inadequate preparation, and lack of support from colleagues and superiors (Han et al., 2022; Mammen et al., 2023). Many NGNs also report feelings of incompetence, low self-esteem, and frustration due to gaps between academic preparation and clinical demands (See et al., 2023).
The impact of stress on NGNs extends beyond individual well-being to broader healthcare outcomes. Research demonstrates that stress influences both the quality of care and patient satisfaction during hospital stays (Singh et al., 2020). High stress levels are associated with emotional and mental health issues, physical injury, burnout, sick leave, reduced job satisfaction, and elevated turnover rates (Sundram et al., 2024; Wong, 2024). Notably, a survey in the USA showed that 27.6% of NGNs left their positions within their first year of employment (Ulupinar & Aydogan, 2021).
The transactional theory of stress and coping by Lazarus and Folkman (Folkman et al., 1986; Figure 1) provides a robust theoretical framework for understanding this phenomenon. This model conceptualizes stress as a dynamic transaction between an individual and their environment, mediated by cognitive appraisal. The appraisal process is critical, consisting of primary appraisal (evaluating whether an encounter is stressful), secondary appraisal (assessing one’s coping resources and options). And the stress initiates coping strategies, which aim to either directly manage the stressor (problem-focused coping, PFC) or regulate emotions arising from the stressful encounter (emotion-focused coping, EFC). Existing literature on NGNs has extensively cataloged both stressors and the subsequent coping strategies employed. Commonly identified PFC include planning, active coping, and seeking help, while EFC encompasses acceptance, positive reframing, and emotional regulation (Han et al., 2022; Jan et al., 2017). Furthermore, factors such as emotional intelligence, resilience, and organizational support systems like mentorship and structured orientation are recognized as key moderators influencing this process (Gardiner & Sheen, 2016; Masso et al., 2022; Zhu et al., 2022).
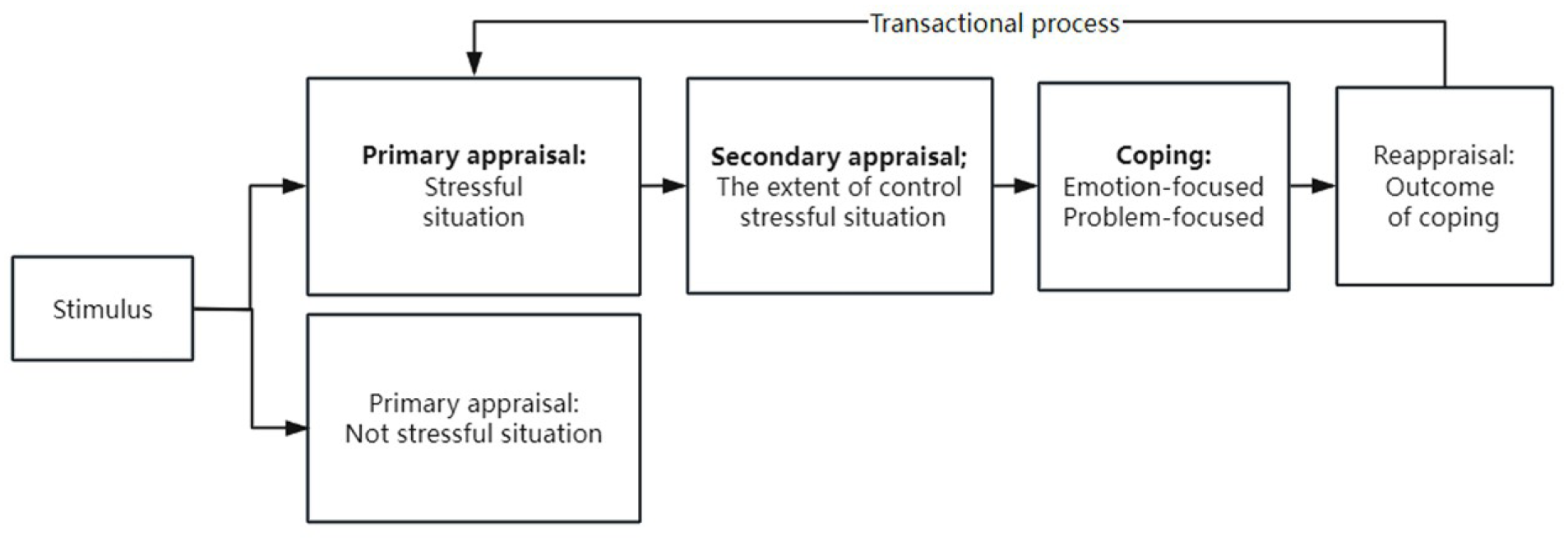
The transactional theory of stress and coping.
However, despite these insights, qualitative evidence exploring the cognitive process of secondary appraisal remains limited. It is unclear that how NGNs personally evaluate their coping resources and capabilities when facing workplace stressors. This gap is particularly evident in specific contexts such as Chinese tertiary hospitals, where unique organizational cultures and high-workload environments may shape distinctive appraisal patterns. Understanding this crucial component of the “stress-appraisal-coping” transaction is essential for developing effective support mechanisms. Therefore, this study aims to conduct in-depth qualitative interviews to explore NGNs’ stress experiences, with particular focus on their secondary appraisal processes and coping mechanisms in clinical practice.
Methods
Design
A qualitative descriptive design was employed to gain a rich, straight description of NGNs’ experiences. The study was conducted between June and August 2022 and is reported following the Consolidated Criteria for Reporting Qualitative Studies (COREQ) reporting guidelines (Du et al., 2022; Supplemental Material 1).
Participants and Setting
Participants were recruited from six hospitals in Changsha, China, comprising four tertiary hospitals and two secondary hospitals, to capture a diverse range of clinical environments. Purposeful sampling was utilized to recruit NGNs who met the following inclusion criteria: (1) a registered nurse, (2) working in a hospital for the first time, (3) with less than 1 year of work experience, and (4) voluntary participation. These criteria were chosen to ensure that participants were in the pivotal transition period from student to practitioner, which is central to the study’s aim of exploring early career stress and coping. Exclusion criteria were: (1) a diagnosed severe mental illness or cognitive dysfunction, (2) inability to complete the interview, or (3) working in a non-clinical position. These exclusions were implemented to focus the study on the experiences of clinically active NGNs who could reliably articulate their experiences.
Initial recruitment used convenience sampling via recruitment advertisements posted within the participating hospitals. Subsequently, snowball sampling was employed where participants recommended other eligible NGNs. Recruitment continued until data saturation was achieved, meaning that subsequent interviews yielded no new themes or insights relevant to the research questions. A final sample of 23 NGNs participated in the study.
Data Collection
Face-to-face, semi-structured interviews were conducted by the first author in private, quiet rooms to ensure confidentiality. Only the interviewer and the participant were present. Prior to the interview, participants completed a brief demographic questionnaire (Table 1). A semi-structured interview guide (Table 2), developed based on the transactional model of stress and a review of the literature, was used to guide the conversations. The interview guide was not pilot-tested formally but was reviewed for clarity and relevance by the research team, including an experienced qualitative researcher. All interviews were audio-recorded and lasted between 20 and 60 min. The recordings were transcribed within 24 hr after the interview. A summary of the interview was presented to the participant to enhance the credibility of the information after it ended in case any inconsistencies occurred.
General Information About 23 NGNs.

Interview Guide.

Data Analysis
Numerical codes (P1 through P23) were assigned to the participants, and any personal information was removed from the interview transcripts to ensure anonymity. Thematic analysis, as described by Braun and Clarke, was then used to identify, evaluate, and summarize themes within the qualitative data (Braun & Clarke, 2006). The six-phase analytical process was also used to interpret the raw data: (1) familiarizing oneself with the data, (2) generating codes, (3) constructing themes, (4) reviewing potential themes, (5) defining and naming themes, and (6) producing the report (Campbell et al., 2021; Hole, 2024). The transaction-based theory of stress informed the investigator’s conceptual framework regarding stress and coping in this study. Consistent with the philosophy and underpinning of qualitative description used in the current work, this study includes no manipulations of pre-selected variables or prior commitment to any one theoretical view. Concepts from the transaction-based theory of stress and coping guide the organization of themes and sub-themes (Folkman et al., 1986). A predominantly inductive approach was adopted in this study; the data were open-coded, and respondent- and data-based meanings were emphasized. A degree of deductive analysis was employed to ensure that the open coding contributed to producing themes that were meaningful to the research questions and that the data-based meanings emphasized were relevant to the research questions (Byrne, 2022). While an older version, NVivo 8 provided robust functionality for the core tasks of data storage, coding, and retrieval required for this analysis. To ensure the reliability of the coding process, all initial codes and the subsequent themes were critically reviewed and discussed by the first author and her research supervisor, an experienced professor with expertise in qualitative methods, until a consensus was reached. Data analysis ceased upon reaching data saturation. A total of three themes and six subthemes were derived.
Ethics
Institutional Review Board approval was obtained from Xiangya Nursing School, Central South University (approval No. E202236) on April 20th, 2022. This study was conducted in accordance with the principles of the Declaration of Helsinki. And the risk of the qualitative interview was potential psychological discomfort of participants, which was mitigated by allowing participants to pause or withdraw at any time without consequence. The benefits of the research, including its potential to inform support systems for new nurses and the reflective value of the interview for participants themselves, were judged to substantially outweigh these minimal risks. Prior to participation, all individuals received a comprehensive information sheet detailing the study’s purpose, procedures, and data management. They were given sufficient time for review, after which the researcher verbally summarized the key points, including confidentiality, anonymization, and the audio-recording process. Written informed consent was obtained from each participant immediately before the interview commenced. All data were anonymized and stored securely in an encrypted database to protect participant confidentiality.
Research Team and Reflexivity
A female interviewer (the first author) conducted the interviews. She was a nursing student with a Master’s degree and had received training in qualitative research. The interviewer kept a reflective journal before and after interviews to bracket previous assumptions and expectations regarding NGNs’ stress. These preconceptions, shaped by prior literature and clinical exposure, were openly discussed within the research team to mitigate the potential impact on data collection and interpretation. The relationship with participants was established at the beginning of each interview, where the interviewer introduced herself as a student researcher interested in understanding their work experiences.
Results
General Information About the Study Population
A total of 23 NGNs completed interviews in this study. Their general information is shown in Table 1.
Major Themes and Subthemes
Through an iterative analysis of transcripts from 23 NGNs, three major themes (Primary appraisal, Secondary appraisal, and Coping) and six subthemes related to work adaptation for NGNs were identified (Figure 2).

Major themes and subthemes mapped in the transactional theory of stress and coping.
Primary Appraisal
This theme encompasses the NGNs’ primary appraisal of their work environment as stressful. The analysis identified two primary sources of this stress: the inherent demands of clinical tasks and the complexities of interpersonal relationships.
Stressful Work Task
A predominant concern for almost all NGNs was the daunting nature of clinical responsibilities upon entry into the workforce. The central challenge stemmed from the theory-practice gap, leading to a period of adjustment where familiarity with workflows and procedures had to be rapidly acquired. This often resulted in feelings of being overwhelmed and apprehensive.
N6: When I first came to the department, I wasn’t familiar with the workflow and worked in a panic. For example, some patients asked me specific questions about my profession that I did not know, and I felt overwhelmed. N9: In the ICU, most patients received postoperative treatment, and their physical condition underwent significant changes within a few seconds. I felt apprehensive about this, and I was afraid I might be unable to control the patient’s physical condition. N12: No one taught me how to do it (some work tasks), but everyone thought I could. I had to learn it all by myself because I never encountered it before, and it was the first time I had done it.
Stressful Interpersonal Relationship
Interpersonal dynamics constituted a significant stressor, with challenges arising from multiple directions within the hospital hierarchy and patient interactions. Many NGNs reported experiencing criticism from colleagues and supervisors concerning their clinical skills and efficiency. Furthermore, navigating relationships with senior colleagues was often tricky, leading to subtle friction or overt conflict. Finally, interactions with patients and their families were a common source of stress, ranging from non-cooperation to verbal aggression.
N9: Some colleagues were not friendly. She made me very unsure of my working ability and undermined my confidence. Criticism significantly impacted NGNs. N19: In the last department, when I first entered the department, I expressed too many opinions in my work, so I had difficulties getting along with colleagues. Although my colleagues were polite to me on the surface, they said something terrible about me behind my back. N11: Some patients did not cooperate with us and then spoke ill of us. In addition, the intoxicated patient got drunk and crazy in ambulances, even hitting and kicking us. When I was tired and busy rescuing patients, I was very angry with such a person and wanted to complain.
Secondary Appraisal
Following the identification of stressors, NGNs engaged in a secondary appraisal to assess their capacity to manage these demands. This process centered on the availability of internal psychological assets and external sources of support.
Internal Resources
Many participants highlighted the critical role of their psychological attributes in mitigating stress. Key internal resources included confidence in their developing abilities, resilience in the face of setbacks, and cognitive flexibility that allowed them to reframe challenging situations, particularly interpersonal conflicts, in a more objective and less personal light.
N5: I recognized my abilities. Even if someone pointed out my shortcomings, I would not feel inferior because of them. N16: My colleagues were dissatisfied with me, such as complaining about my low efficiency or not doing my job well. I reminded myself that it didn’t matter even if I was criticized, and then wrote in my diary to boost my spirits. I believed I would do better next time. N15: When conflicts arose, I thought about them more objectively. Some patients may be angry and impolite. However, they were not against you; something was not going their way. How I saw and perceived it was more important than what it was.
External Resources
The presence of supportive external figures was consistently identified as a crucial buffer against stress. Most NGNs emphasized the indispensable role of a supportive and competent preceptor, who provided not only clinical guidance but also psychological safety, thereby facilitating a smoother transition.
N11: I thought the most important factor was my preceptor. She was very good-tempered and not mean to me. She would not complain to the head nurse if I made a mistake. She helped me correct it and supervised my work, and then I adapted more quickly.
Coping
In response to their appraisals, NGNs adopted a variety of coping strategies, which aligned with the PFC and EFC. The choice of strategy appeared to be influenced by the nature of the stressor and the resources available.
Problem-Focused Coping
This strategy involved direct efforts to address the stressor itself. To manage demanding work tasks, NGNs proactively sought knowledge from colleagues and engaged in introspection to improve their methods. In managing interpersonal relationships, they attempted to adjust their communication and behavioral styles to foster better connections, though this was sometimes reported as emotionally taxing.
N20: Firstly, I asked them for advice on the shortcomings in my work, and I continued to learn and work hard. The second was to summarize my methods in clinical work by writing a diary to introspect my daily work. It allowed me to become more competent in my work more quickly and made up for deficiencies that existed at work. N17: If I stayed in this department, I would have to find ways to establish good relationships with others. For example, I had to manage my relationship with the preceptor. Even if she didn’t like me, I still tried to compliment and please her to help me. N22: I once tried to integrate into the department by joking with colleagues or offering flattery, but I later felt exhausted and gave up. I decided to focus solely on my job. Furthermore, I hardly rested and strived to do my job well. I helped my colleagues as long as they asked. When I was capable of my job, my colleagues treated me better. N10: When conflicts arose at work, I was not controlled by my negative emotions due to the accusations of patients. I focused on solving problems. The patient’s attitude would improve as long as the problem was solved.
Emotion-Focused Coping
EFC aims to regulate emotions arising as a consequence of the stressor. According to Lazarus’s study, various forms of EFC include self-control, escape avoidance, distancing, and seeking social support. When NGNs face criticism, accusations, or unfair treatment at work, they manage their emotions and process these negative feelings, demonstrating self-control. Escape-avoidance was applied when NGNs immersed themselves in solving work tasks and focused on the moment to avoid negative emotions. Distancing means that NGNs establish psychological boundaries to avoid stressful interpersonal relationships. Almost all NGNs sought external support. They talked to their close friends and families for emotional comfort.
N14: I still wanted to improve my colleagues’ relationships, but the reality was complex, and some problems always existed. I can only do my own thing and take its course. N9: I did not have time to think about these workplace interpersonal problems. I was busy thinking about how to handle my many patients. After work, I went out with friends and did not think about these problems. This was a significant reason that interpersonal problems did not trouble me much. N13: I pretended that I heard nothing when some colleagues spoke ill of others behind their backs. I tried to behave very obediently and diligently, and as a result, I did not get involved in any other issues within the department. N15: Sometimes, when I was in a bad mood or stressed at work, I returned home and talked to my friends. This was a way to vent negative emotions.
Discussion
This qualitative study explored the stress experiences, cognitive appraisal processes, and coping mechanisms of NGNs, with a specific focus on the often-overlooked stage of secondary appraisal. Our findings reveal that NGNs navigate a complex transition characterized by significant stressors related to clinical tasks and interpersonal relationship. A central finding is the critical role of secondary appraisal, where NGNs consciously evaluate both internal psychological resources and external support before selecting coping strategies. This appraisal process acts as a pivotal mediator between encountering a stressor and initiating a coping response.
From the initial assessment, the primary sources of stress were identified as work-related tasks and interpersonal relationships. There is a gap between current school theory and clinical practice. NGNs feel nursing operations are diverse and delicate, requiring repeated practice. Moreover, they cannot be proficient quickly (Labrague et al., 2020). Other colleagues challenged NGNs’ work skills, and they struggled to gain acceptance at work. The colleagues’ criticism and mistrust due to NGNs’ low efficiency and poor work skills are common but adverse for NGNs at the beginning of their careers, undermining their confidence and initiative (Hu et al., 2017). Some studies have shown that NGNs experience conflict with colleagues or patient (Hawkins et al., 2019). The lack of social experience and communication skills places NGNs in the position of newcomers and service providers, making them vulnerable to workplace incivility. These interpersonal conflicts increase NGNs’ depression, even anger and indifference toward colleagues or patients (Cakal et al., 2025). Both workplace incivility and increased workload contributed to higher burnout. Heightened burnout correlated with increased turnover intention and lowered job satisfaction (S. E. Lee et al., 2024).
Secondary appraisal refers to the regulation and control of one’s response behavior. This is primarily concerned with the ability to control the stimulus, which can be conceptualized as a kind of control judgment. NGNs identify and evaluate their coping resources matters in the stress process and coping resources are mainly divided into internal psychological resources and external support. This study provides a nuanced understanding of the secondary appraisal process, extending beyond the factors identified in previous quantitative studies. It identified that internal psychological resources include confidence, resilience, and cognitive flexibility. Prior research has established confidence and resilience as individual protective factors. Resilience can help to bounce back or recover when confronted by adversity, trauma, misfortune, or change (Fernandez et al., 2020; Kim, 2021) and confidence is an essential trait for NGNs to possess in order to provide quality patient care (Ortiz, 2016). We also explored that cognitive flexibility promote individuals’ positive understanding of adverse events and previous study confirmed that it is associated with fewer depressive symptoms and greater mental wellbeing (Kruczek et al., 2020).
This study also illuminates how these internal resources are actively mobilized. NGNs in our study described a conscious cognitive process of gauging their own psychological resources when faced with a challenge, which directly influenced whether they felt equipped to engage in problem-solving or defaulted to emotional regulation. In terms of external resource. The instrumental support from preceptor helps NGNs familiarize themselves with the work environment and masterwork tasks quickly. Additionally, emotional support from preceptors enhances the NGNs’ sense of belonging to the department. Preceptor have been shown to help enhance new nurses’ clinical knowledge and skills, as well as promote their sense of belonging in other studies (Han et al., 2022; Irwin et al., 2018). Conversely, a lack of support led to appraisals of the environment as threatening, depleting the cognitive resources necessary for PFC and fostering a reliance on EFC such as distancing or avoidance. This finding underscores that secondary appraisal is not a purely internal event but a transaction evaluated against the backdrop of the workplace environment.
Our results further delineate a temporal pattern in coping strategy utilization, adding depth to the categorical lists of strategies commonly reported (Zheng et al., 2023). In the immediate aftermath of a stressor, EFC strategies like self-control, deep breathing, and seeking emotional support were frequently employed to manage acute emotional distress. The regulation of emotions, involving “escape-avoidance” and “distancing,” minimizes the experience of disturbing feelings and temporarily protects the individual from unpleasant or unacceptable aspects of reality (Brody & Costa, 2020). Those are direct self-protection to decrease the psychological damage caused by stress, and it does not always work out in the long run. Studies showed that mindfulness and relaxation techniques like deep breathing, reading books, and praying effectively manage stress and improve their wellbeing (Rahman, 2022; Velana & Rinkenauer, 2021). This implementation of EFC can be understood as a necessary and functional short-term strategies. However, the transition to more sustainable, long-term adaptation was contingent upon the subsequent engagement in PFC. NGNs try various problem-solving methods to adapt to their work, especially in work tasks and interpersonal relationships, which is accordance with other studies (Baharum et al., 2023; H. Y. Lee et al., 2013). Moreover, our study found that this transition was not automatic. It was facilitated by a secondary appraisal that judged the situation as manageable with available resources. For instance, an NGN who felt supported by a preceptor was more likely to move from feeling overwhelmed (EFC) to actively seeking guidance and planning tasks (PFC). This observed dynamic explains why simply teaching coping skills may be insufficient; interventions must also ensure that the workplace context is perceived as supportive enough to make the use of those skills seem viable and effective. This nuanced view of the coping process as a potential pathway, rather than a simple choice, represents a significant contribution to the understanding of NGN adaptation.
The findings translate into clear, actionable implications for healthcare leadership. Support programs must be designed to directly augment the specific resources that NGNs evaluate during secondary appraisal. Firstly, investing in high-quality, structured preceptorship is critical; preceptors should be trained not only in clinical supervision but also in fostering self-efficacy and providing psychological safety. Secondly, organizational policies must actively cultivate positive team climates and reduce incivility, as a hostile environment directly sabotages effective coping by negatively skewing secondary appraisals. Furthermore, support should be conceptualized as tiered: providing immediate, accessible emotional first-aid to validate initial EFC needs, while simultaneously establishing systematic, competency-based development pathways that facilitate the natural transition to sustainable PFC. By strategically building these specific resources, healthcare organizations can directly positively influence NGNs’ core appraisal processes, ultimately promoting successful transition, enhancing well-being, and improving retention.
Limitations
This study has several limitations that should be considered when interpreting the findings. First, the reliance on convenience and snowball sampling methods may have introduced selection bias and limited the heterogeneity of the participant pool, which could affect the generalizability of the results. Second, the qualitative nature of the research design, while providing in-depth insights, inherently involves subjectivity in thematic analysis. Potential issues such as researcher bias and social desirability bias cannot be ruled out and may have influenced data collection and interpretation. Finally, the participant cohort consisted primarily of female nurses with bachelor’s degrees working in tertiary hospitals. Consequently, the findings may not fully represent the experiences of nurses in other settings, male nurses, or those with graduate-level education. Future research should employ more diverse sampling strategies and include participants from varied clinical contexts and demographic backgrounds to validate and extend these findings.
Conclusion
This study provides a nuanced understanding of the stress-coping process among NGNs by specifically examining the overlooked cognitive mechanism of secondary appraisal. Our findings reveal that NGNs’ coping strategies are not merely reactive but are determined by a conscious evaluation of both internal resources and external resources during the secondary appraisal stage. The temporal dynamic observed that initial EFC serves as a short-term stabilizer and the transition to sustainable PFC being contingent upon a positive resource appraisal. This provides a significant contribution to the transactional model of stress in this population. The novelty of this research lies in its qualitative illumination of how NGNs cognitively navigate this appraisal process, moving beyond the established what of stressors and coping strategies to explain the underlying why of their choices.
Based on these insights, we propose three concrete recommendations for practice: implementing pre-employment psychoeducation to prepare NGNs for the appraisal process; establishing structured, psychologically-informed preceptorship to provide a secure base for resource evaluation; and integrating brief, accessible emotional support interventions to manage immediate distress while building long-term adaptive capabilities. This focused investment in the resources NGNs themselves value most is paramount for fostering a sustainable and competent nursing workforce.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440251415508 – Supplemental material for Newly Graduated Nurses at Work: A Qualitative Study From the Stress Process Perspective
Supplemental material, sj-docx-1-sgo-10.1177_21582440251415508 for Newly Graduated Nurses at Work: A Qualitative Study From the Stress Process Perspective by Saiyu Gao, Wenlu Zhang, Jingping Zhang and Yun Peng in SAGE Open
Footnotes
Acknowledgements
The authors thank all the nurses who participated in the interviews.
Ethical Considerations
Institutional Review Board approval was obtained from Xiangya Nursing School, Central South University (E202236). This study was conducted in accordance with the principles of the Declaration of Helsinki. And the risk of the qualitative interview was potential psychological discomfort of participants, which was mitigated by allowing participants to pause or withdraw at any time without consequence. The benefits of the research, including its potential to inform support systems for new nurses and the reflective value of the interview for participants themselves, were judged to substantially outweigh these minimal risks. Prior to participation, all individuals received a comprehensive information sheet detailing the study’s purpose, procedures, and data management. They were given sufficient time for review, after which the researcher verbally summarized the key points, including confidentiality, anonymization, and the audio-recording process. Written informed consent was obtained from each participant immediately before the interview commenced. All data were anonymized and stored securely in an encrypted database to protect participant confidentiality.
Consent to Participate
Written informed consent to participate was obtained.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
We do not provide audio recordings or transcribed texts for ethical reasons.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.