
Abstract
We describe an original protocol Treating Depression Downhill (TDD) that was designed as a specific therapy for depression. Evolutionary theories of depression served as a basis for its development. We discuss the rationale for using evolutionary theory and describe the structure and integrative nature of TDD. We then present an observation on TDD’s application to group therapy of active duty military personnel. In the described sample, TDD demonstrated effectiveness and specificity for depression, differentiating it from anxiety and personality disorders.
Introduction
Depression has been known since the biblical times (1 Kings 19: 4-5, King James Version), but our success in treating it is relatively modest despite the growing and refined repertoire of interventions including antidepressant medications and psychotherapies. Major depressive disorder remains the most commonly diagnosed psychiatric condition and claims the most disability time among mental disorders (Kessler et al., 2005; Rai, Zitko, Jones, Lynch, & Araya, 2013). Recurrence is the norm in depression (Solomon et al., 2000; Wakefield & Schmitz, 2013) contributing to its prevalence.
Psychosocial interventions for depression have grown in diversity and sophistication. The list of psychotherapies used to treat depression is impressive (Jorm, Allen, Morgan, & Purcell, 2009). Yet, it is believed that about 20% or more of cases do not respond to conventional treatment (Fava, 2003; M. B. Keller et al., 1992; Souery & Pitchot, 2013). The many therapies currently used seem to have no obvious champion or gold standard (Shedler, 2010). There is also no consensus about the reasons behind the relatively limited success in treating depression. Trying to understand its resistance to therapy, we may consider two sets of factors: the distinct features and challenges of this condition and the way we approach its treatment.
Challenges to Treating Depression
Many therapists would attest to particular difficulty of treating a deeply depressed person. The unique feature of depression among other mood/affective disorders is that its main symptom, depressed mood (Diagnostic and Statistical Manual of Mental Disorders [5th ed.; DSM-5; American Psychiatric Association [APA], 2013]), is negative. When asked to describe their experience of depressed mood, many people have difficulty articulating it. They provide statements such as “I just feel blah,” “I just don’t feel right,” “I just don’t care anymore,” “I can’t be happy anymore,” “I’m not myself, it’s not me,” and so on. These statements reflect the low hedonic tone, that is an experience of lack of mood or its underinflated quality (discussion of the agitated or angry type of depression is beyond the scope of this report). Depressed people present with a slew of negative symptoms (DSM-5) such as anhedonia, loss of appetite, loss of interest and motivation, energy, presumably stemming from dysregulation of the motivation/reward circuitry, although the exact mechanism of such dysregulation is unclear (Bogdan, Nikolova, & Pizzagalli, 2012; Cao et al., 2010; Nestler & Carlezon, 2006).
Treating absence of mood and desire presents an obvious challenge, because the therapist is not in a position to replenish the deficit, and the client may be difficult to engage emotionally. It has been noted that depressed client’s hopelessness may create a perception of ineffectiveness and a helpless feeling in the therapist, making sessions with depressed clients feel draining, suffused with the sense of helplessness on both sides, and empty (Berzoff & Hayes, 1996).
The existing approaches either in pharmaco- or psychotherapy do not directly target the low hedonic tone, which is especially evident in the fact that such potent euphoric agents as amphetamines, cocaine, or opiates are not used as antidepressants, nor do the commonly used antidepressants have euphoric effect. Of note, the opioid and dopamine systems have lately been explored for development of new antidepressant medications (Carlezon, Beguin, Knoll, & Cohen, 2009; Carroll & Carlezon, 2013; Gershon, Vishne, & Grunhaus, 2007; Jutkiewicz, 2006).
The prevalence of negative symptoms presents a challenge to talk therapy due in part to the difficulty articulating the depressed state. In the incisive words of Lewis Wolpert (2008), “Clinical depression is a strange state, and I have claimed that if you can describe your severe depression, you haven’t truly experienced one” (p. 2).
Another challenge is the large gray area between ecologically valid depressed state and pathology. Cases of ecologically valid depression still may be diagnosed as illness and may end up in mental health clinics. Overdiagnosing depression appears to have become common (G. Parker, 2007; Wakefield & Schmitz, 2013), which creates a dichotomy in conceptualizing care as support versus treatment. Although it can be both, they call for different approaches.
Nevertheless, psychotherapy has been shown effective in treating depressive disorders. Common approaches include cognitive-behavioral therapy (CBT) and interpersonal, psychodynamic, and mindfulness-based therapies; cognitive-behavioral analysis system; and behavioral activation. All of them yield effect sizes comparable with CBT, whose effect size is close to that of antidepressant medications (Butler, Chapman, Forman, & Beck, 2006; Hollon, Thase, & Markowitz, 2002; G. Parker, Roy, & Eyers, 2003). For mindfulness-based therapies, see Hofmann, Sawyer, Witt, and Oh (2010); Ost (2008); Powers, Zum Vorde Sive Vording, and Emmelkamp (2009). Aerobic exercise, yoga, and massage therapy have also been shown effective for treating depressive symptoms (Cramer, Lauche, Langhorst, & Dobos, 2013; Dunn, Trivedi, Kampert, Clark, & Chambliss, 2005; Moyer, Rounds, & Hannum, 2004). Such wide an array of approaches give clinicians many options to choose from but has their downside, because the diversity of those approaches implies their lack of specificity for depression.
The Specificity Problem
Historically, psychological interventions were not designed for specific disorders but rather targeted symptoms or psychological problems. For example, psychoanalysis was originally designed to treat neuroses (Freud, 1966), whereas behavioral therapies targeted maladaptive information processing and resulting behaviors (Franks & Wilson, 1974). However, mental disorders are commonly viewed and classified as symptom constellations (DSM-5); hence, by design, psychotherapies were not specific to mental disorders.
Universality of a tool may become a trade-off against its effectiveness. Lack of disorder-treatment specificity has been suggested as one of the factors limiting the success in treating depression, and a new “choose horses for courses” paradigm has been advocated (G. Parker & Fletcher, 2007; G. Parker, Roy, & Eyers, 2003; G. B. Parker, Malhi, Crawford, & Thase, 2005). Although CBT is widely accepted as a therapy of choice for depression, the authors point out that neither theoretical considerations nor empirical data indicate that CBT is equally effective or superior to other interventions for all depressive disorders (G. Parker et al., 2003). They suggest choosing an approach specific to the nature of a depressive disorder, differentiating between psychotic, melancholic, secondary depression, and dysthymia.
Still, the general trend among more recently developed therapies has been toward universality rather than specificity. CBT, the most studied psychotherapy, was initially developed and is considered a first-line therapy for depressive disorders but has hitherto been used for a number of mental and psychosomatic disorders. Its low specificity (or high universality) has been highlighted in several reviews (Butler et al., 2006; Haby, Donnelly, Corry, & Vos, 2006; Hollon et al., 2002; G. Parker & Fletcher, 2007; Shedler, 2010). These reviews reflect on the low specificity of other therapies as well.
CBT is an exception among therapies used for depression in that it was developed specifically for depression based on a theory of its symptomatology (Beck, 1967), which has likely contributed to CBT taking the centerfield in treating depressive disorders. However, this may have also determined its limitations, because it was based on a theory of the symptoms rather than a theory of depression as a systemic response.
Treating Depression Downhill (TDD)
In an attempt to increase the efficacy of psychotherapy for depression, we aimed at making it more specific. High specificity can be achieved either empirically by trying different tools for the task until one proves a better fit than the others—“the right horse for the course,” or by using available heuristics to custom-design “the right horse.” Following the latter strategy, we decided to integrate the existing therapeutic approaches into a framework aligned with a theory of depression.
Theories of depression are many and range from the neurochemical to social levels, constituting a matrix of overlapping theories that are yet to be integrated into a unified general theory (Bogdan et al., 2012). We have chosen to base our approach on evolutionary theories of depression. Being a metatheory, evolutionary theory has the most explanatory power. Rather than explaining the mechanics of depression, it seeks an explanation of the origin and purpose of depressive process as a systemic response to the environmental pressure. Addressing the ecology of organism’s behavior, evolutionary theories seem best suited to provide a disorder-specific guidance to a therapist, because (a) ecology is the level where therapeutic encounter occurs and (b) the theories consider symptoms of depression not merely a constellation of organism’s reactions but a purposeful process with which a therapy could be aligned.
Perhaps most importantly for our endeavor, evolutionary theories consider depression not a breakdown of organism’s functioning but an adaptive process with its due course. Even untreated depressive episodes remit on average within 12 months (Furukawa, Kitamura, & Takahashi, 2000; Spijker et al., 2002; Whiteford et al., 2013). This implies that recovery may be part of depressive process. The recurrent nature of major depression speaks against its adaptive value, suggesting that not every depressive process may be adaptive. Evolutionary theories appear more instructive about the course of depression compared with more mechanistic theories that are mainly concerned with its etiology and factors determining vulnerability.
Evolutionary theory has its own limitations. As a descriptive theory, it is insufficient to elucidate the mechanism of depression. Instead, it accommodates its multiple etiologies. Watt and Panksepp (2009), for example, use a concept of “depressive matrix” referring to the multifactorial nature of the presumptive etiology of depression. This limitation, however, is not an obstacle to guiding a disorder-specific psychosocial intervention. Such intervention can be specific to the phenomenology of depressive process without the constraints of specificity to its etiology. We relied on evolutionary theories to establish a therapeutic framework that would parallel the natural course of depression.
A number of evolutionary theories of depression have been proposed and periodically reviewed and critiqued (M. C. Keller & Nesse, 2006; Nettle, 2004; Watt & Panksepp, 2009). All of them converge on the idea that depressive process has evolved as an adaptive response to insurmountable adversity, where behavioral and hedonic withdrawal is the main strategy achieved by downregulation of the motivation/reward system. Although evolutionary theory cannot by its nature be proven or falsified, widely used animal models of depression appear compatible with it.
Forced swimming test in rodents (Porsolt, Le Pichon, & Jalfre, 1977) has its theoretical base in the learned helplessness paradigm (Seligman, 1972). Another rodent model is social defeat (Koolhaas et al., 1990). Social defeat (often coupled with entrapment) has been identified as a central psychological construct in depression (Gilbert & Allan, 1998; Price, Sloman, Gardner, Gilbert, & Rohde, 1994).
Both models have been validated in experiments with chronic administration of antidepressants and demonstrated to involve dysregulation of the motivation/reward circuitry (Berton et al., 2006; Cervo & Samanin, 1988; Russo & Nestler, 2013; Tye & Deisseroth, 2012).
Loss is another major psychological state related to depression. Watt and Panksepp (2009) suggest that depression evolved as an adaption to terminate separation distress in mammalian infants. An animal model of social loss and associated depression was developed and studied in monkeys several decades ago (Bowlby, 1980). More recent work on separation distress has focused on the transition from protest to acquiescence. This transition has been recognized as a prototype of depression: “This sequence from protest to despair provides a powerful animal model of human clinical depression,” (Zellner, Watt, Solms, & Panksepp, 2011, p. 2). The authors consider it a prototype of such hallmark features of human depression as general resignation or “giving up” comprising apathy, social withdrawal, and hopelessness.
Distinguishing between helplessness, defeat, and loss may be useful for operationalizing these constructs in research, especially for developing animal models. For our purpose of designing a therapy specific to depression, we subsume the concepts of helplessness and loss under that of defeat, although they may reflect distinct psychological constructs. A state of defeat is tautological with helplessness, and irrevocable loss also connotes feeling defeated.
Most models of depression focus on its initial stages, which is understandable, as the main goal is to either prevent or abort the depressive process. Less attention has been given to finding a model of spontaneous recovery from depression. Yet, to be adaptive, the depressive state must be transitory, and there should be a natural mechanism of recovery. Such recovery is well illustrated by an old and now seldom used model of depression in monkeys. In that model, infant monkeys separated from their mothers go through the phases of protest, withdrawal, and recovery (Kaufman & Rosenblum, 1967). The recovery happens through the infants’ self-stimulation and exploratory behavior.
We designed our approach keeping in mind the three phases of depression highlighted by evolutionary theory and animal models. In our view, defeat triggers an adaptive depressive response, where after an initial phase of protest, the organism disengages from it through shutdown of its motivation/reward system. Once the organism is no longer in a state of protest, recovery becomes possible through a still poorly understood mechanism. That mechanism may involve activation of the motivation/reward system by stimulation and exploratory behavior. Recent studies of the effects of effort-based processes on the motivation/reward circuitry offer interesting clues about such possibility (Salamone, Correa, Farrar, & Mingote, 2007). Other theorists propose a cognitive route to recovery (Andrews & Thompson, 2009). Their “analytical rumination hypothesis” suggests that rumination, a ubiquitous symptom of depression, evolved to allocate attention to complex problems that had led to depression, thus facilitating their resolution.
Unlike most therapies that aim at reverting and abrogating the depressive process, our approach is to facilitate and accelerate it in a controlled way. Its initial two stages aim at completing the disengagement from protest and at acceptance of defeat, hence its name—Treating Depression Downhill (TDD). TDD includes three phases: exploration, acceptance, and behavioral activation, and, accordingly, combines three methodologies: psychodynamic, mindfulness, and cognitive-behavioral.
Methods and Participants
The Structure and Process of TDD
Exploratory phase
In this phase, the client explores his experience of defeat. The goal is for him to gain insight into the history and sources of his experience of defeat, whether perceived or factual. Sometimes, a state of defeat can be triggered by a singular recent event such as death of a loved one, but more often, there are developmental antecedents—past experiences of defeat. Some of them may be defended against and reside in the unconscious, others may be conscious but still unresolved.
Our rationale is that gaining insight would help clients complete the hypothesized protest phase of depression by uncovering and confronting their ego defenses and ineffective coping strategies. We use brief psychodynamic exploration (Luborsky, 1984; Strupp & Biinder, 1984) to seek insight into the underpinnings of the client’s defeat.
Our main strategy of gaining insight is reflecting on and analyzing the client’s reactions to others and his behavior (mainly in session but also on the outside). For example, excessive blaming combined with passivity is often a marker of unmet social needs that had been frustrated in the client’s past, constituting his unresolved defeat. We find early emotional neglect or abuse to be a frequent risk factor for depression, which is in line with the findings that childhood emotional maltreatment sensitizes people to stress, thus increasing their vulnerability to depression (Shapero et al., 2014).
The more difficult cases of developing insight are those of “spontaneous” depression without an obvious trigger in either the client’s present or past (conditions with clear physiological or chemically induced etiologies are beyond this discussion). Yet, even then, it is often possible to trace the vulnerability to personality traits such as neuroticism (Kotov, Gamez, Schmidt, & Watson, 2010). The insight in that case consists of the awareness, sometimes hitherto latent, of being “different,” which, in and of itself, constitutes a defeat to many.
Acceptance phase
The idea behind this phase is to terminate protest. Once a client identifies and acquires insight into her defeat, she learns to accept it as an immutable fact of her life. This is the centerpiece of our treatment, as it attempts to accelerate and complete the transition from protest to resignation/acquiescence. In this sense, the acceptance phase may be considered depressogenic. The main goal at this point is to help the client stop wishing for an escape or for things to be different. To that end, she learns to “sit” still at the hedonic bottom of her despair without falling back on protest. We aid such transition through training and practice of mindfulness. Our application of mindfulness differs from its use in other mindfulness-based therapies (Hayes, Strosahl, & Wilson, 1999; Williams, Teasdale, Segal, & Kabat-Zinn, 2007). Practice of mindfulness in our approach is agenda-driven, where the agenda is experiential learning of acceptance and tolerance of defeat. Mindfulness in our approach is tailored to the client’s defeat and therefore, contains an element of exposure therapy.
After having learned the basics of mindful meditation, which starts in the previous phase and continues throughout the treatment, clients learn to hold the image and feeling of their defeat and despair in their awareness. At the same time, they observe the state of their mind and body, thus utilizing a dual-attention process. They do it repeatedly over multiple sessions. Then, they start practicing the “letting go” meditation (Kabat-Zinn, 1990, 1994), which is a run up to the next phase.
In our experience, mindfulness obviates the difficulty of working with negative symptoms. It appears well-suited to deal with the sense of lacking and emptiness, as it does not require a target other than the present state of mind and does not call for it to be anything but what it currently is. Being mindful of one’s depressed state is accepting it.
It is common for our depressed clients to experience difficulty meditating especially on their own. Maintaining active concentration does, indeed, prove hard for depressed, often prone to rumination, people, so does self-initiating meditation in a state of apathy. We have found that regular guided meditation in session combined with detailed review of clients’ difficulties and experience of it helps develop their ability to engage in meditation. We also believe that accepting attitude to one’s difficulty, which is part and parcel of mindfulness (Kabat-Zinn, 1990, 1994), facilitates clients’ engagement.
Behavioral activation phase
This phase aims at jumpstarting the motivation/reward system, whose activation is believed to be the essence of recovery. It is based on the established behavioral activation approach (Jacobson, Martell, & Dimidjian, 2001). We, however, omit the functional analysis part, thus using a watered down version. Our protocol starts with practice of mindful experiencing of simple activities in session, for example, the “raisin exercise” (Kabat-Zinn, 1990), and proceeds to expending the repertoire of such activities outside sessions.
Clients are encouraged to establish their routine schedule of activities. Their experiences of those activities are monitored, their failure to adhere to the schedule is addressed, and suspected avoidant tendencies are identified. We especially emphasize social activities and encourage clients to increase their involvement with positive figures in their lives. In our practice, increased social engagement is often a telltale sign of recovery.
Not only does the use of mindfulness provide a bridge to the previous stage of treatment, creating continuity of the therapeutic process, it also serves the crucial, at this stage, function of overcoming the client’s resistance. Lack of interest, motivation, pleasure, and energy, all symptoms of depression (DSM-5), presents a formidable obstacle to the client’s engagement in activities. Practicing mindful, present-oriented, simple, and “feeling good” activities in session (sometimes in a “field trip”) helps model such engagement and circumvent the resistance.
Cognitive reappraisal
Cognitive reappraisal does not constitute a separate phase of TDD but is practiced throughout the treatment. We follow the usual cognitive therapy approach where we examine clients’ beliefs about their defeat, as they emerge. Possible distortions and questionable validity of those beliefs are pointed out and discussed. We watch for signs of overgeneralization, misattribution, and absolute and catastrophic thinking. In our experience, clients’ beliefs about their defeat usually change during the treatment. However, we often find that this change is facilitated by change in the affective tone, without which the client’s cognitive adjustment does not “stick,” reverting to the depressive patterns. This is why we do not segregate cognitive reappraisal into a separate phase but try to time it to the moments of clients’ apparent readiness to engage with such intervention.
Once we notice change in clients’ cognitive patterns, we bring it to their attention. The awareness of such change appears to further facilitate the therapeutic progress.
Although TDD proceeds forward from one phase to the next, it is seldom truly linear. It is practiced as a flexible therapy accommodating individual needs and pace, and is usually cyclical with recursive loops of exploration and cognitive reappraisal. The practice of mindfulness, however, evolves in a more linear fashion, as it begins with learning the skill and is applied henceforth in a phase-specific way, as described above. Overall, TDD unfolds according to its directional framework of facilitating the process of “letting go” of protest and accepting defeat, and then onto recovery through behavioral activation. We have developed and used TDD mostly for individual therapy. In this report, we describe its application to group treatment.
Participants
All participants were active duty U.S. military personnel stationed in California. The criterion for referral was a diagnosis of a depressive disorder including major depressive, dysthymic, and depression not otherwise specified (NOS) disorders. Exclusion criteria included active psychosis, ongoing substance abuse, bipolar disorder, and compromised cognitive functioning. Clients were referred by either their therapist or a clinician who did an initial assessment. All referred clients were accepted without screening due to administrative/logistic considerations.
This report presents the observation on two consecutive groups (six participants each) as one set of data. A total of 13 participants were recruited with 12 of them retained in treatment. The participants’ demographics were representative of the general client population in the clinic. Their mean age was 28 (SD = 8); females 4, males 8; Caucasian 6, Hispanic 4, African American 1, Native American 1. A depressive disorder was the basis for referral, and consequently, the participants had depressed mood as a common complaint; besides depressed mood, other common complaints included disturbed sleep, loss of interest and motivation, decreased concentration, and fatigue. Because clients were accepted without screening, the group turned out clinically diverse; whereas three participants carried a single diagnosis, the rest had two or more, with one client having a dual diagnosis of Alcohol Dependence, as shown in Table 1. Multiple diagnoses are a common occurrence for people with personality disorders, especially borderline personality (Zimmerman & Mattia, 1999), which is reflected in our sample as well (Table 1). All but one participant were medicated (Table 1); their regimens had been established at least 3 weeks prior to the group and did not change during it. Participants diagnosed with posttraumatic stress disorder (PTSD) and alcohol dependence were also in cognitive processing therapy for PTSD and in a substance abuse program.
Participant Summary.

Note. NOS = not otherwise specified; SS/NRI = selective serotonin- or norepinephrine reuptake inhibitor; MDD = major depressive disorder; PTSD = posttraumatic stress disorder; OCPD = obsessive compulsive personality disorder; PD = personality disorder; GAD = general anxiety disorder.
To protect participants’ confidentiality, they were randomly assigned a letter.
A class of medication that the participant was on during the group.
Participants who dropped out of the group before Session 12.
For the purpose of data analysis, the participants were divided into three groups according to their diagnoses (Table 1). One group (three participants), henceforth called depression subgroup, included participants carrying diagnoses of uncomplicated depressive disorders, and although one of them was also diagnosed with attention-deficit hyperactivity disorder (ADHD), his ADHD symptoms were not his complaint, and he was neither treated nor sought treatment for them. Another group (four participants), personality disorders subgroup, included participants diagnosed with a personality disorder comorbid (in two cases) with depression. The third group (five participants), anxiety disorders subgroup, included participants with anxiety disorders comorbid (in two cases) with depression.
Despite the requirement of a depressive disorder diagnosis, some of the participants were referred based on their complaint of “feeling depressed” without carrying a formal diagnosis of depression. Clinical diversity was not our intention; however; it afforded us a natural experiment, where the anxiety and personality disorders subgroups served as controls for the depression subgroup.
Group Process
The group went according to TDD protocol used in individual therapy and as described above. The protocol needed only minor adjustments to the group format, because its mindful meditation/acceptance and behavioral activation modules were by nature directive and easy to practice in group. The exploratory and cognitive reappraisal modules were modified to largely replace the therapist’s intervention with input from the group, which was driven by the group dynamics while controlled and directed by the facilitators. Such modification felt necessary to maintain the participants’ engagement, because too much input from facilitators might come across as lecturing, thus undermining that engagement.
Due to the structured and directional framework of TDD, the group’s style was a mix between workshop and a therapy group, because of the need to balance the use of group dynamics with skills training.
The group met for a total of 24 biweekly 90-min-long sessions guided by a leader and coleader. The treatment consisted of 2 cycles of 12 sessions, where the second cycle was a repeat of the first. Each cycle comprised three four-session modules: exploration, acceptance, and behavioral activation. Each session started and concluded with 10 to 20 min of mindful meditation, where the opening meditation was a body scan, and the closing one was adapted to the session’s content. We encouraged participants to practice mindfulness and mindful meditation between sessions, and their experiences were discussed in each session to address the difficulties they might have. Reflection on sessions’ content was encouraged and processed.
Despite the linear progression of TDD, it often proceeds in a recursive manner with returns to the previous phases, as mentioned above. In a group setting, participants process their experiences at a different pace. The two-cycle format (12 sessions each) was designed to accommodate the need for reprocessing and “catching up.”
To keep the group process consistent with the treatment goals and direction and to maintain treatment fidelity, the facilitators debriefed each other after sessions.
Assessment
Participants were evaluated and diagnosed by their referring clinicians. During the group, they were assessed with a set of self-report psychometric scales including Beck’s Depression and Anxiety Inventories, BDI-II (Beck, Steer, & Brown, 1996) and BAI (Beck & Steer, 1990), respectively, the short 10-item version of Positive and Negative Affect Scale (PANAS; Watson & Clark, 1999), and the “Ladder of life” Life-Satisfaction 11-point Likert-type scale (Cantril, 1965). The assessment was done at four time points: in the 1st, 8th, 16th, and 24th sessions.
Whereas BDI-II and BAI are commonly used for assessing symptoms of depression and anxiety, we additionally used PANAS as a measure of participants’ balance of affect, as much of the focus in TDD is on affective experience. The Life-Satisfaction Scale was used as a measure of subjective well-being. Multiple psychometrics, redundant as they may appear, helped tracking the participants’ emotional states with independent instruments, so that the emerging dynamics would carry more significance if converged onto a common trend. Given our small sample size insufficient for statistically sound conclusions, relying on temporal trends would be the remaining alternative. The leader and coleader also monitored participants’ progress based on their presentation and verbal self-report.
Psychometric Scales
BDI-II (Beck et al., 1996) is a self-report multiple-choice questionnaire consisting of 21 items representing different symptoms of depression rated by severity from 0 to 3. It was shown to have high test–retest reliability (r = .93) and internal consistency (α = .91). BAI (Beck & Steer, 1990) is also a self-report 21-item scale rated from 0 to 3 by severity of anxiety symptoms. Its test–retest reliability r = .75 and internal consistency α = .92. Both scales are scored by adding the scores for individual items, thus yielding an overall symptom severity value.
The short 10-item self-report I-PANAS-SF Scale (Thompson, 2007) consists of five positive and five negative affects rated by intensity from 1 to 5 and from −1 to −5, respectively. The overall value or balance of affect is calculated by adding the individual items’ scores. The positive affect items include Active, Alert, Attentive, Determined, and Inspired, whereas negative items are Afraid, Ashamed, Hostile, Nervous, and Upset. The reported test–retest reliability for the Positive and Negative subscales r = .84; the reported internal consistencies for Positive and Negative subscales αs = .78 and .76, respectively. The measure correlated well with its 20-item PANAS prototype at .92 for the Positive subscale and .95 for the Negative one.
The Cantril’s (1965) “ladder of life” is a single-item 11-point Likert-type scale, asking responders to rate their current life from the worst to the best possible.
Results
Psychometrics
Participants in depression subgroup were presenting ostensibly less depressed with brighter affect and were increasingly engaged as the group progressed. They also reported greater social involvement in their personal lives. The change was acknowledged by the participants themselves, as well as noted by the rest of the group. Table 1 details the change in participants’ BDI-II scores. The score range of 0 to 13 is considered minimal symptoms, 14 to 19, mild, 20 to 28, moderate, and above 28, severe. Some participants dropped out or failed to turn in the questionnaires, which further decreased our data sample (Table 1, Figure 1). The pre–posttreatment difference, although apparent in depression subgroup, does not reach statistical significance even for this group, which is not surprising given the subgroup’s size of three participants (Table 1). It has to be noted, though, that all of them showed a consistent downward tendency of their BDI-II scores, in contrast to the other subgroups (Figure 1).

Dynamics of Beck’s Depression (BDI-II) individual scores. I, II, III—depression, personality disorders, anxiety disorders subgroups, respectively.
All other measures are presented as dynamics of average scores for a given group (Figure 2). The initial mean score on a given psychometric scale was taken for 100% and the subsequent scores were presented as percent of the initial score. For analysis of the PANAS scores, its scale was transformed into all positive (0-10) values.
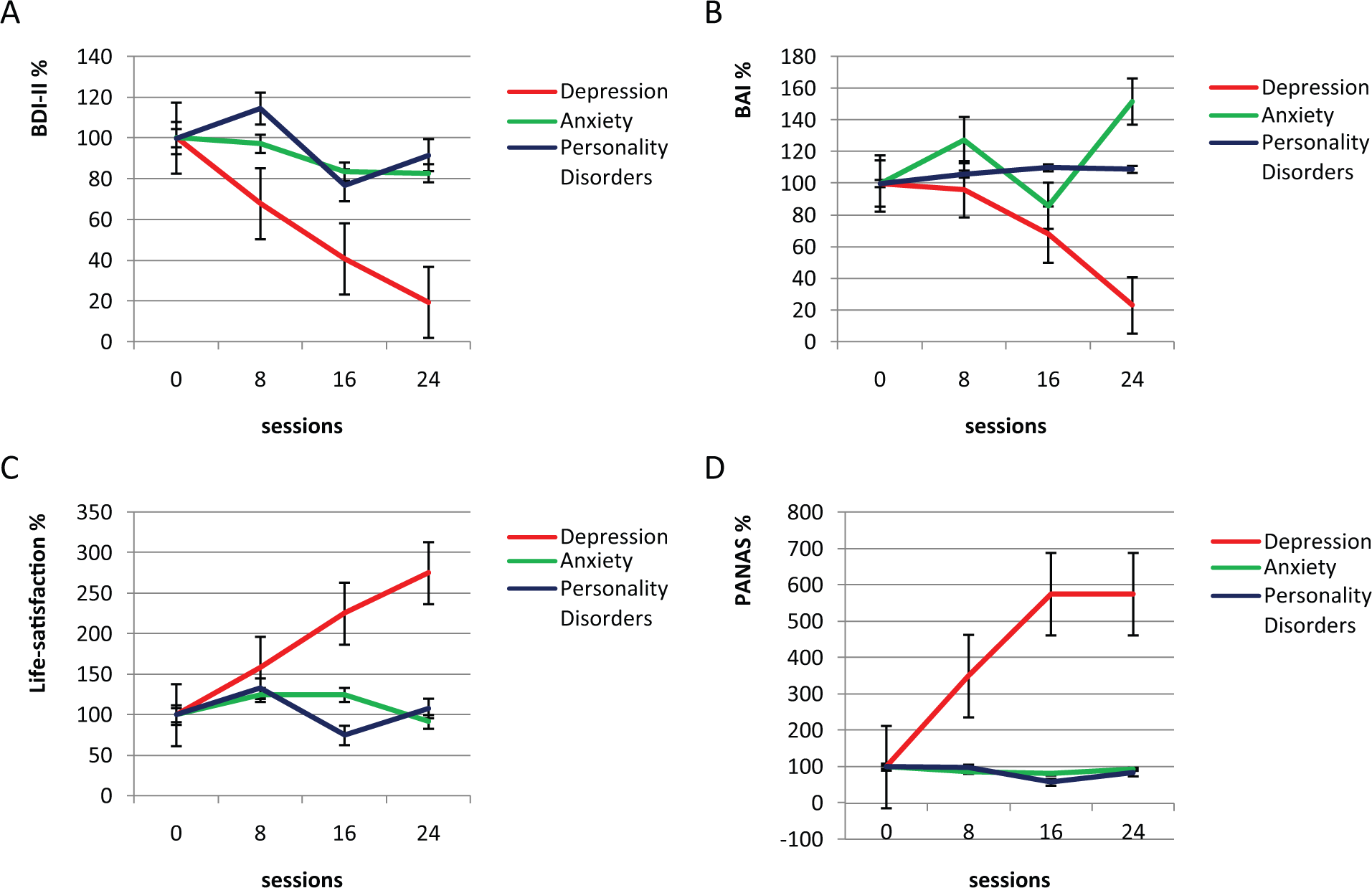
Dynamics of (A) Beck’s Depression (BDI-II), (B) Beck’s Anxiety (BAI), (C) Life-Satisfaction, and (D) PANAS average scores for the depression, anxiety, and personality disorders subgroups.
Depression subgroup showed a clear positive trend on every measure, whereas the other two showed no consistent tendency in their dynamics (Figure 2) with the exception of a tentative decrease of the BDI-II score in the anxiety subgroup. Noteworthy, in depression subgroup, 50% drop in BDI-II was around Session 12, the group’s middle point, whereas with BAI, it happened toward the group’s end around Session 20 (Figure 2). Fifty percent drop corresponds to scores 18 and 12 on BDI-II and BAI, respectively, which is below the cutoff for moderate depression and anxiety. Anxiety subgroup, while showing a tentative decrease on BDI-II, showed no decrease on BAI.
The presented tendencies in depression subgroup were not due to an individual outlier/s effect, as all the individual scores followed the subgroup’s tendency, as exemplified by BDI-II scores (Figure 1) and the other measures (not shown). In sum, the observed tendencies indicate that TDD may be effective with depressed clients in group treatment and that its effect appears to be specific for depression.
Individual Experiences
Participants’ individual experiences were changing depending on their diagnostic presentation and the group’s stage. In the initial exploration phase, the participants’ engagement was relatively low and mostly in response to the facilitators’ prompts. Toward the stage’s end, when the group’s cohesion increased, the participants were more willing to share their life experiences and would volunteer observations on each other, which appeared to have facilitated the development of insight. One example is the common trend of excessive blaming and use of projection defense among them, which the participants picked up on relatively quickly. Another example of a common experience was feeling marginalized by peers. The participants, guided by the facilitator, helped each other increase their awareness of the earlier experiences of marginalization. Especially helpful appeared their ability to realize that being different did not have to mean being “less than” or “not as good as them.”
By the beginning of the acceptance phase, the participants most engaged in the process appeared to have had higher motivation to engage in mindfulness training. Yet, some of those who did not appear very active in the previous phase, engaged in mindfulness practice as well, welcoming change in the group process. This phase proved the most difficult for two participants from anxiety subgroup, one of whom stated she could not do mindful meditation and refused to follow, and for the participant with Schizotypal personality disorder, who related poorly to the group in general.
During the behavioral activation phase, the participants from depression subgroup appeared “ahead” of both the facilitators and other participants. This impression is in agreement with the dynamics of their psychometric scores (Figures 1 and 2). They had an easier time increasing their activities and took initiative in diversifying them. There were mixed results with the rest, some of whom continued with their usual behavioral patterns, either making excuses or withdrawing from the group process.
The second cycle of the group was largely a replay of the first but with a wider divide between the participants, who had made progress in the previous cycle, and the rest. Those who made progress were more active in group, volunteering to both share their experiences and observations of others, as well as offering advice. That might have been a downside of the diagnostically diverse group, as it could feel discouraging to the participants, who were “behind.” This issue was not addressed during the group and was one of the reasons against inclusion of diverse diagnoses in the consecutive groups.
Discussion
We set out to design a therapy specific for depression. For that purpose, we developed a therapeutic framework that paralleled the natural depressive process as understood from the evolutionary perspective. We designed our treatment by integrating psychodynamic, mindfulness, and cognitive-behavioral approaches into a sequence of therapeutic phases. Designed for individual therapy, it has been used for 2 years with good results (not shown), usually yielding a significant symptoms reduction after six sessions. However, it is yet to be tested in randomized controlled studies in comparison with the established interventions for depression.
We have used this approach in group for the pragmatic reason of making it available to a larger patient population. Applying this treatment in a group setting, we were afforded a natural experiment that tested our approach on a clinically diverse group of clients (Table 1).
The treatment’s outcome (Table 1, Figures 1 and 2) appears to lend support to our expectation that TDD specifically targets depression, whereas anxiety and personality disorders are not susceptible to it. If this observation holds true in future research, this would, to our knowledge, be the first talk therapy that differentiates depression from anxiety. The differential effect of our treatment is unlikely to be due to therapist bias, because the analysis of participants’ records and their diagnostic classification were done after the group’s completion.
Anxiety is a ubiquitous symptom in depression and is listed as a specifier in DSM-5. High comorbidity between depressive and anxiety disorders is also well documented (e.g., Kessler, DuPont, Berglund, & Wittchen, 1999). The relationship between these conditions has been studied since long ago and is still unclear. Following the descriptive dimensional model developed by Watson and Clark (1991; Watson, 2005) and Higgins’ regulatory focus theory of their putative mechanisms (Klenk, Strauman, & Higgins, 2011), we consider anxiety and depression both independently driven and interdependent. In line with those views, the anxiety component in depression may be seen on the continuum from nonexistent to highly prevalent. Accordingly, we predict that the effectiveness of TDD will decrease from the former to latter.
With respect to differential effect of TDD on depression and anxiety, Acceptance and Commitment Therapy (ACT) has to be mentioned. ACT makes use of mindfulness and acceptance, as does TDD; however, it appears as effective for depression as it is for anxiety (Hayes, Luoma, Bond, Masuda, & Lillis, 2006; Ost, 2008; Powers et al., 2009). Comparative analysis of the two therapies is beyond the scope of this report, but we want to point out a substantial difference in their approaches that may be relevant to their different effects on anxiety. ACT targets clients’ “private events” or their mental representations of life-events. In that, it promotes acceptance of and distancing from those representations, trying for “comprehensive distancing,” as the authors call it (Hayes et al., 2006). Clients are encouraged to stay aware of the distinction between their mental events and the reality they represent.
Although also promoting awareness of clients’ mental events, TDD does not emphasize their distinction from reality. On the contrary, it could be called “comprehensive approaching” or immersion, as it promotes admitting defeat and accepting it as part of reality on “both sides of the skin” and not only as a mental representation, which may stoke up anxiety rather than alleviate it. People whose symptoms are driven by depressive process and who manifest signs of withdrawal may have better tolerance of “sitting” with defeat. The ones whose symptoms are driven by anxiety may be more in an avoidance mode and not ready to approach and submit to defeat.
We consider acceptance of defeat a central and crucial part of TDD. It is an equivalent of exposure therapy that has been widely used for anxiety disorders either as a stand-alone treatment or a component of a broader therapeutic frame (for a recent review, see Abramowitz, Deacon, & Whiteside, 2011). Although psychodynamic and behavioral activation approaches to treating depression have been shown effective (Shedler, 2010, and Jacobson et al., 2001, respectively), the necessity and effectiveness of the mindfulness/acceptance phase of TDD may be questioned. After all, most established therapies for depression are not predicated on this component. To determine what components of TDD are essential, and whether their combination is more effective than each of them individually, a component analysis study is needed. TDD’s modular structure lends it readily to such analysis.
TDD is based on well-established therapeutic techniques and can be readily adopted by interested practitioners. The described treatment was administered by the author, a licensed clinical social worker with 10 years of clinical practice, and a bachelor level counselor trained by him. For the purpose of this therapy, the behavioral activation and mindful meditation techniques do not appear to require extensive training and expertise, especially when implemented with an experienced cofacilitator. The psychodynamic and cognitive restructuring aspects, however, require both understanding and experience in those techniques. Therefore, at least one of the facilitators for such group should have a good grasp of basic psychotherapeutic techniques through appropriate education and training.
Limitations
This work was done with fairly young military personnel (M age = 28; Table 1), and it remains to be seen whether our observations can be generalized. Besides the age, the participants had many stressors in common that come from military lifestyle. We believe that these factors could facilitate the participants’ relating to each other and the group’s cohesion. Shared experiences and ease of relating might help them develop insight by facilitating the group dynamics. However, there was a felt divide in the group between those with war experience and the rest. The two participants with war experience (J, L) did not appear to have benefited from the group (Table 1, Figure 1).
It must be emphasized that the presented observations are a result of a natural experiment. Inclusion of multiple diagnoses in the group was not intentional but due to an administrative arrangement that precluded screening out the participants. That arrangement allowed us to compare the effects of our therapy among participants with different diagnoses, using them as controls for each other. At the same time, it came with significant limitations inherent to natural experiments.
The most limiting of them was that our experiment could not be reproduced due to ethical considerations; the participants with main diagnoses other than depression appeared to have benefited little from the treatment. Another obvious limitation was the small sample size. The main comparison group—depression subgroup—comprised three participants (Table 1, Figure 1). Therefore, the tentative trends in the dynamics of the participants’ scores we were able to observe did not reach statistical significance. This makes our report a preliminary pilot observation of TDD’s effects in a group therapy setting. In our opinion, it provides a rationale for follow up outcome studies of TDD in both individual and group therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.