
Abstract
Evolutionary theories suggest that depression has evolved as an adaptation to insurmountable adversity or defeat. One prediction stemming from these models is that individual attributes associated with defeat in a given social environment could be risk factors for depression. We hypothesized that in young military men, where physical prowess was important, short stature might constitute a risk of depression and that this risk would be specific to depression and not to other prevalent mental disorders such as anxiety. A preliminary analysis of the diagnostic profile of a sample of male military personnel treated for mental health indicates that men both shorter and taller than average by 1 standard deviation may be predisposed to higher rates of depressive but not anxiety disorders. Practical and theoretical implications of our findings are discussed.
Introduction
Does Size Really Matter?
Surprisingly, this question still remains a matter of debate (Ambler, Fairchild, & Wilkinson, 2013). In particular, researchers cannot reach a consensus on whether idiopathic or “normal” short stature (SS) confers health and psychological disadvantages. It has been established that SS people of both genders are subject to stigmatization and prejudice (Underwood, 1991), and SS children suffer greater psychosocial stress (Zimet et al., 1997). Conversely, tall stature (TS) is associated with perception of higher status and achievement (Jackson & Ervin, 1992; Lechelt, 1975; Wilson, 1968).
However, it remains unclear whether psychosocial stress associated with SS leads to substantial functional deficits. A number of large epidemiological studies have found SS to be associated with poorer mental health (Cheung et al., 2013) and lower health-related quality of life (Christensen, Djurhuus, Clayton, & Christiansen, 2007). In men, SS was additionally associated with poor educational achievement (Magnusson, Rasmussen, & Gyllensten, 2006) and higher risk of suicide (Magnusson, Rasmussen, Lawlor, Tynelius, & Gunnell, 2006). Other studies have concluded that height has negligible effect on health-related quality of life (Busschbach, Rikken, Grobbee, De Charro, & Wit, 1997; Coste, Pouchot, & Carel, 2012). Some studies on SS children did not find them significantly less well psychologically adjusted than their taller counterparts (Downie, Mulligan, Stratford, Betts, & Voss, 1997; Ulph, Betts, Mulligan, & Stratford, 2004).
Multiple factors may have contributed to this contradiction. Samples were drawn from different cultures, where societal attitudes to SS may differ; samples comprised different age brackets; and different measurements were used to assess people’s psychological adjustment and quality of life. Perhaps most important, the researchers framed their question differently.
Some put the emphasis on whether SS may compromise people’s competitiveness, as in the mentioned studies demonstrating the link between SS and lower academic achievements and perceived social status (Magnusson, Rasmussen, & Gyllensten, 2006; Magnusson, Rasmussen, Lawlor, et al., 2006). Others emphasized the question of whether SS directly affected functioning of short people. These researchers, for example (Coste et al., 2012), mostly focused on meticulously controlling for confounding variables such as socioeconomic status, parental education, health problems, and so on. After controlling for those variables, they found only “negligible” effects of SS, suggesting that these effects are largely mediated by other, likely social, factors.
Studies of stature’s effects on health and psychological adjustment did not specifically address the possible mediating role of stature as a marker of men’s social rank. One of the effects of stature on social rank is its role in mating competition. Men’s height correlates positively with their attractiveness to women and mating success (Pawlowski, Dunbar, & Lipowicz, 2000; Pierce, 1996). Importantly, men’s height is not linearly related to female mating preferences but has a U-shaped relationship, where both ends of the distribution show lower values than the above-average middle, although the short end is still inferior to the tall one (Hensley, 1994). As the authors of another study stated, “shortness is more of a liability than tallness is an asset”; they also demonstrated TS’s association with perception of high social rank (Jackson & Ervin, 1992, p 433). The very concept of masculinity is regarded as both bodily and culturally embedded with a complex relationship between the two realms, which has led to the notion of multiple masculinities and hegemonic masculinity as their overarching vector (Connell & Connell, 2005; Connell & Messerschmidt, 2005), where stature is but one contributing factor.
Even if the difference in psychological adjustment of short people is largely explained by concomitant social variables, the causal relationship (or lack thereof) between them and SS still needs to be elucidated. Evolutionary theory suggests organism’s inherited attributes, such as SS, as primary targets of environmental pressure. In application to men, it would mean that their SS as a marker of lower status would make them more vulnerable and shape their response to social pressure.
Involuntary Subordination
Defeat, social defeat in particular, has been identified as a core psychological state in depression (Gilbert, 2006). It has been conceptualized as a loss of social rank in a direct conflict or competition, which may result in depression-like symptoms including behavioral and social withdrawal, and subordinate behavior. Accordingly, depressive response has been conceptualized as an adaptation to defeat or involuntary subordination (Gilbert, 2006; Gilbert & Allan, 1998; Price, Sloman, Gardner, Gilbert, & Rohde, 1994). Submission can be adaptive, as it may help avoid a potentially lethal or damaging confrontation, thus increasing the fitness of the subordinate.
An animal model of depression based on social defeat was established a long time ago (Kudryavtseva, Bakshtanovskaya, & Koryakina, 1991). In its current form, it consists of repeated forced exposure of individual mice to larger and more aggressive ones. Such exposure produces a depressive-like phenotype. Importantly, this phenotype can be reversed by chronic but not acute administration of a selective serotonin reuptake inhibitor (SSRI) antidepressant, which supports the model’s validity (Golden, Covington, Berton, & Russo, 2011).
In humans, as in other animals, subordinate social status is associated with high chronic stress, depressive reactions, and poorer health (Sapolsky, 2004). Moreover, perceived social rank was found in closer association with health indicators than actual one (Adler, Epel, Castellazzo, & Ickovics, 2000). In humans, much of the research on social defeat has been conducted in the bully/victim paradigm that is believed to parallel the dominant versus subordinate model in other animals (Björkqvist, 2001). Victims, like subordinate animals, have been shown to suffer from chronic stress and depressive symptoms (Björkqvist, 2001). However, bullies have also been found to be at a greater risk of depression compared with general population (Kaltiala-Heino, Rimpelä, Marttunen, Rimpelä, & Rantanen, 1999).
Adolescence is an age when social standing among peers assumes high importance. In a study of a sample of adolescent boys in an all-boys school, their status in peer hierarchy correlated positively with self-esteem and negatively with their rate of depression (Fournier, 2009). Subjective social status has been shown to negatively correlate with depressive symptoms in a large sample of adolescents (Goodman et al., 2001).
Body size is likely an important contributor to social status, although it is but one of many contributing factors such as aggression, age, affiliations, social history, and so on (see Chase, Tovey, Spangler-Martin, & Manfredonia, 2002, for review). In adult humans of the industrialized world, height is a readily observable, easily measurable variable that is constant and independent of psychosocial factors. As mentioned above, it affects psychological adjustment and quality of life, with SS being perceived as a marker of low status.
Hypothesis
Our hypothesis stems from two independent evolutionary-based premises reviewed above: (a) that depressive symptoms evolved as an adaptive response to defeat, social defeat in particular; (b) that in men, height is a marker of masculinity, perceived mating value, and status. We hypothesized that in young men SS led to higher prevalence of depressive symptoms but not necessarily other common mental health symptoms such as anxiety.
Idiopathic SS is an out-of-group phenomenon usually defined as 2 standard deviations (SD) below the mean height of the reference population, one that matches in sex and age (Ranke, 1996). In order for SS to serve as a marker of status, an SS individual must be perceived as such among his peers, for which a threshold of significant shortness should be reached. Therefore, correlation between height and prevalence of depressive symptoms in men (if present) is also expected to be an out-of-group phenomenon, that is, no significant correlation is expected within the group. Once someone is perceived short statured, he is already stigmatized, and it matters relatively little how short he is within the SS group. The same is expected for the “normal” stature group. Then the highest correlation between height and depressive symptoms may be expected at the group’s margin. The height polymorphism in a given population is likely to affect the sensitivity of out-of-group perception and, consequently, the sensitivity of the hypothesized correlation. For example, a threshold of 0.5 SD in a low polymorphism population may be perceived as significant as 1 SD in a high polymorphism one.
Another prediction from our hypothesis is that the effects of SS are more pronounced in settings of intense intramale social competition, especially where physique is considered important.
In line with the situation–symptom congruency hypothesis (Keller & Nesse, 2006), the association of depressive symptoms with SS should be specific to some but not other symptoms that are unlikely to have evolved as an adaptation to social defeat. For example, we do not expect SS to be associated with increased anxiety because anxiety is not a useful adaptation to social defeat.
We made a preliminary observation in a group of active duty military men who received mental health care. That was a suitable model group as it consisted of young physically healthy men in a competitive mostly male environment, where physical prowess was valued.
Method
The data were taken from records of a mental health clinic serving active duty military personnel. We randomly selected a relatively homogeneous sample of 196 healthy (no major diagnosis of somatic illness) males of Caucasian background. Ethnic/racial groups may represent distinct reference populations because their mean body heights differ. Caucasians constituted a majority of the patients and were chosen as a sample for our analysis. As we were interested in depressive symptoms, we chose patients carrying depression-related diagnoses. Patients with anxiety-related diagnoses were taken as a control group representing the most prevalent cluster of mental disorders (Kessler et al., 2005). The diagnoses were established as part of routine care by mental health providers of the clinic (either psychiatrists or PhD-level psychologists, who were uninvolved in this project) according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994).The sample’s demographics and diagnostic profile are presented in Table 1.
Demographics and Diagnostic Breakdown of the Sample.

Note. PTSD = posttraumatic stress disorder.
To capture the severity of our patients’ condition along either depression or anxiety axis, we ranked their disorders according to the diagnostic hierarchy reflected in DSM-IV/Diagnostic and Statistical Manual of Mental Disorder (5th ed.; DSM-5; APA, 2013) and used the rank as a proxy for severity. Among depressive/depression-related disorders, the lowest in that hierarchy are the residual categories such as adjustment disorder with depressed mood and depression (not otherwise specified [NOS]) because these diagnoses are not given when the criteria for specific depressive disorders are met. So we rated them lower than the specific diagnoses of dysthymia and major depression and assigned relative values as follows: adjustment disorder with depressed mood—1, depression NOS—1, dysthymic disorder—2, major depressive disorder—2. We assigned relative values to anxiety-related disorders following the same logic: adjustment disorder with anxiety—1, anxiety NOS—1, generalized anxiety and panic, disorders—2. When an individual carried more than one diagnosis, he was assigned the highest value along both axes, for example, someone with depression NOS and major depressive disorders would be rated at 2, likewise, a patient with anxiety disorder NOS and panic disorder would be rated at 2.
The mean height was 178.7 cm (SD = 7), which is close to that of Caucasian males in the United States (Centers for Disease Control and Prevention, 2014)—176.0 cm. Military ranks in our sample were rated follows: privates—Category 1, lance corporals—Category 2, corporals—Category 3, sergeants—Category 4, staff sergeants—Category 5, and above staff sergeants—Category 6 (for the purposes of the analyses, the highest ranks were considered as one category). The total sample was divided into three groups: SS—1 SD below the mean, lesser than 172 cm; TS—1 SD above the mean, greater than 185 cm, and average stature (AS)—between 172 and 185 cm. We included the TS group in our analysis as a control group of height outliers.
We compared the three height groups (SS, AS, and TS) on severity of depression and anxiety diagnoses using one-way ANCOVAs with rank as a covariate considered as 6 categories. In addition, we performed a confirmatory analysis, where depression and anxiety diagnoses were used as yes/no dichotomous variables.
Results
A one-way ANOVA comparing the three groups (SS, AS, and TS) on depression severity revealed a significant effect of Group, F(2, 193) = 4.13; p = .02. Post hoc Least Significant Difference pairwise comparisons showed that both short individuals and tall individuals had significantly higher prevalence of depression diagnoses than AS individuals, short versus average: t(155) = 2.24; p = .03; tall versus average t(168) = 2.04; p = .04; short and tall individuals did not differ from each other (Figure 1). Because the distribution of depression severity scores deviated from normality, we confirmed the significance of these findings with nonparametric tests. The Mann–Whitney U test confirmed that both SS and TS individuals had significantly higher depression scores than AS individuals (SS: p = .02; TS: p = .04).
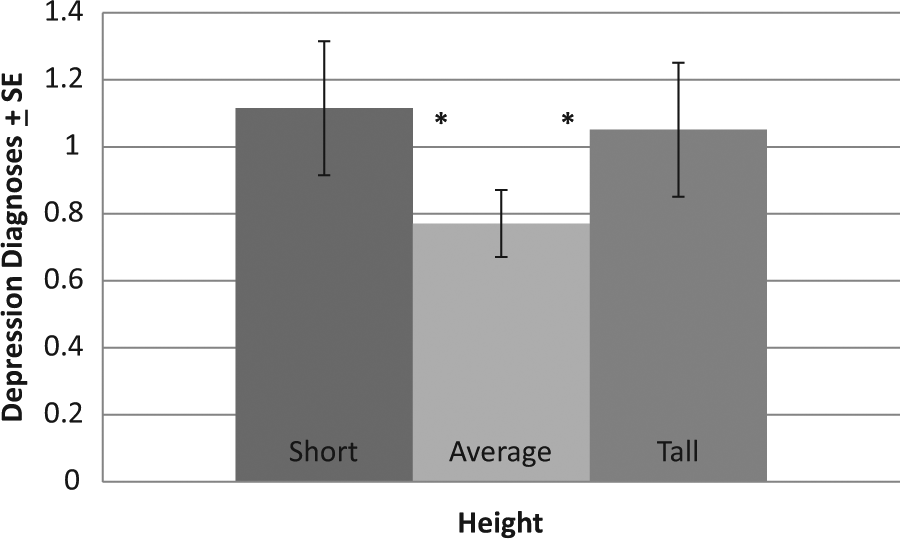
The levels of depression-related diagnoses in young military men of short, tall, and average stature.
A one-way ANOVA comparing the three groups (SS, AS, and TS) on anxiety severity did not reveal a significant effect of Group, F(2, 193) = 2.74; p = .11.
We next explored potentially relevant demographic and experiential covariates for inclusion into the primary analyses of the relationship between height and diagnostic severity. We found that number of combat deployments and military rank both negatively correlated with depression severity, deployments: Rho(196) = −.26; p < .0005; rank: Rho(196) = −.18; p = .01. This is in agreement with the earlier demonstrated correlation between military rank and stature (Mazur, Mazur, & Keating, 1984). Marital status was positively related to anxiety, Rho(196) = .16; p = .02, while age was not related to diagnoses. We therefore reanalyzed the data considering these covariates. In our analysis of depression, we did not consider the number of deployments as an appropriate covariate as the number of deployments was negatively associated with depression severity, and we reasoned it more likely that poorer functioning and performance in more depressed individuals resulted in fewer deployments, rather than more deployments improving depression symptoms. If so, using the number of deployments as a covariate would eliminate important depression-related variance. Hence, we only considered military rank as a covariate in the one-way ANCOVA comparing the three groups (SS, AS, and TS) on depression severity. The analysis revealed a significant effect of Group, F(2, 192) = 3.52; p = .03, and a significant effect of rank, F(1, 192) = 4.28; p = .04. Post hoc least significant difference pairwise comparisons confirmed that both short individuals and tall individuals had higher prevalence of depression diagnoses than AS individuals though the difference between short and average individuals was at trend level (short vs. average: p = .06; tall vs. average p = .03). The ANCOVA comparing the three height groups on anxiety severity with marital status as a covariate revealed a significant effect of marital status, F(1, 192) = 6.87; p = .009, but the effect of group was not significant, F(2, 192) = 2.51; p = .08.
Finally, we examined whether the presence of any clinically significant depression or anxiety differed as a function of height group. The chi-square test revealed that there were more depression diagnoses in the TS than AS individuals, χ2(170) = 6.62, p = .01, and there was a trend suggesting more depression diagnoses in SS than AS individuals, χ2(157) = 2.95, p = .07. For anxiety diagnoses, there were no significant differences between the groups (ps > .13).
There was no statistically significant correlation between height and symptoms prevalence in either the whole sample or within the groups (ps > .45).
Discussion
We present a preliminary analysis of diagnostic profiles of young male military personnel in relation to their height. We chose 1 SD cutoff for outlier SS and TS groups rather than the commonly accepted for idiopathic SS 2 SD, because a larger cutoff, for example, 1.5 SD, would have included only eight short men and significantly undercut the statistical power. Besides, using the 2 SD cutoff would be impossible because those men could not be recruited to the military. The sample available to us was of a relatively small size and afforded a limited scope of information; also, we had to rely on diagnostic impression of clinicians rather than standard measures of anxiety and depression. Still, the findings validate our initial suggestion that SS in men is associated with a higher level of depression but not anxiety (Figure 1) and that this is an out-of-group effect. Absolute body height was uncorrelated with the rates of depressive and anxiety diagnoses in our sample, and difference was only found, when outliers were compared with the rest. This is in accord with our prediction that the perception of being SS rather than absolute height adversely affects men’s psychological well-being. The trend of SS servicemen showing higher levels of depression remained after accounting for rank as a covariate although falling short of statistical significance (p = .06). The connection between SS and lower rank has been demonstrated before (Mazur et al., 1984), which confirms the general notion of short men achieving lower social status.
The analysis has revealed additional tendencies beyond the initial hypothesis. The most important among them is the finding that TS servicemen show elevated levels of depression, as SS do (Figure 1).
Which Size Matters?
Our initial hypothesis made no stipulations about TS men. On the surface, it may appear that while SS is a psychological vulnerability, being tall should provide protection and foster psychological well-being, because tallness is a marker of status and competitiveness. The important question, however, is how tall. The taller the better may not necessarily hold true. The available data on the effects of height on men’s status and achievements show that inordinately TS carries no benefits. Men’s attractiveness, for example, was shown to have a U-shaped relation to height with both tails of distribution losing to the above-average middle (Hensley, 1994), and so was men’s chance to be married (Manfredini, Breschi, Fornasin, & Seghieri, 2013).
Even if very tall men do not outcompete their counterparts of average to above-average height, it still leaves the question of their higher vulnerability to depression open. The answer to it has, by necessity, to be highly speculative at this point. One possibility to consider is that vulnerability of tall men may lie in their very strength. Perceived as highly dominant by others and themselves, these individuals may hold overinflated expectations of their performance and success, which may make them more vulnerable to instances of defeat, when they happen. That may elicit depressive response in very tall men with a higher frequency compared with men of AS.
It is also conceivable that marginalization itself is a depressogenic factor, regardless of the stature’s value. There is a large literature on vulnerability of marginalized groups to anxiety and depression (for a recent review, see Pieterse, Todd, Neville, & Carter, 2012). However, to our knowledge there have been no reports indicating that marginalization can have a differential effect on depression versus anxiety as in our case. We, therefore, favor a more nuanced explanation that considers interaction of status and marginalization with depressive and anxiety responses to them, as explicated below.
Depressive Versus Anxiety Response
The relationship between anxiety and depression has been of considerable interest for a long time. The two are highly comorbid, for example (Kessler, Nelson, McGonagle, & Liu, 1996), and anxiety is listed as an associated feature of major depression in DSM-5. Still, both depressive and anxiety symptoms may present separately. Several models account for interdependence and relative independence of anxiety and depression, including the descriptive dimensional model developed by Watson and Clark (Clark & Watson, 1991; Watson, 2005) and Higgins’s regulatory focus theory (Higgins, 1998; Klenk, Strauman, & Higgins, 2011). According to these models, there is a continuum of relationship between anxiety and depressive symptoms from inverse to concomitant.
Regulatory focus theory suggests that two autonomous but interacting systems are responsible for development of anxiety and depressive symptoms. The prevention system is responsible for negotiating threats, and its dysregulation may lead to anxiety symptoms, while the promotion system is responsible for meeting the organism’s needs, and its inhibition may lead to depressive symptoms. It is also hypothesized that the promotion and prevention systems are mutually inhibitory, which explains the high comorbidity of anxiety and depression—as the promotion system is downregulated, leading to depression, the prevention one is activated resulting in increased anxiety and vice versa (Higgins, 1998). This theory also implies a rather intuitive possibility that there are two main strategies to respond to adversity: anxiety and depressive responses that may to a certain extent be either mutually exclusive or complementary. This may account for instances of both separate and comorbid anxiety and depression. Depending on learned experience, genetic makeup, and cost–benefit analysis of a particular circumstance, individuals may rely more either on depressive or anxiety strategy.
From the premise that depressive symptoms evolved as a response to insurmountable adversity, lack of concomitant anxiety symptoms makes sense as responding with anxiety to a situation that can neither be avoided nor corrected would be maladaptive. In this sense, depressive response may be considered a defense against anxiety. Indeed, it has been suggested that depression evolved as a defense or a shutdown mechanism against separation distress in mammal infants (Watt & Panksepp, 2009). That view is in an apparent contradiction with the regulatory focus theory because it proposes that inhibition of the motivation (promotion) system leads to shutdown of separation distress, which can only be achieved by inhibiting the separation anxiety.
This contradiction can be reconciled by looking at the interaction of depressive and anxiety response from a dynamic perspective. It is possible that the initial stage of depression does indeed release anxiety, whereas at a later stage, as the depressive response matures it leads to inhibition of anxiety, resulting in transition from the “protest” to “despair” phase (Bowlby, 1980). These considerations await a more precise knowledge about the mechanisms involved in the interaction of the circuitries involved in depressive and anxiety responses.
The idea that depressive response may protect from excessive anxiety is also noteworthy because it may reconcile the biggest challenge for evolutionary theories of depression, namely, its recurrent nature. It has been observed that a depressive episode increases the probability of consecutive episodes (Solomon et al., 2000), which can hardly be considered adaptive and has been a major critique of regarding depression as an adaptation (Nettle, 2004). Yet, if depressive response can indeed protect from anxiety, once learned it is likely to be facilitated in the following encounters with adversity. In an environment with more repetitive and, therefore, highly predictable threats, such strategy can be adaptive because it would shorten or eliminate the initial counterproductive “protest” phase.
In our sample, SS and TS men had higher rates of depressive but not anxiety diagnoses compared with AS men (Figure 1). This finding has led to a post hoc extension of our hypothesis to suggest that SS and TS men adapt to their marginal status by engaging the depressive response and disengaging anxiety because marginalization by stature cannot be undone.
The psychology of SS has not yet been thoroughly studied. It is still an open question what personality traits and cognitive styles might mediate the effect of SS on vulnerability to depression. Our model may be a doorway to addressing this question, as it suggests that SS (and maybe TS) may bias male development toward more depressive than anxiety response to stress.
Pathological Depression Versus Adaptive Depressive Response
There is currently no unitary theoretical framework for depression, even though a variety of risk factors and mechanisms have been identified ranging from biological to psychological to social (Bogdan, Nikolova, & Pizzagalli, 2012). Rather than addressing the mechanisms of depression, evolutionary theory seeks an explanation of the origin and purpose of the depressive process as a systemic response to environmental pressure, thus going beyond the mechanistic question “how” to tackle the teleological “why.” A number of evolutionary theories of depression have been proposed and periodically reviewed (Keller & Nesse, 2006; Nettle, 2004; Watt & Panksepp, 2009). All evolutionary theories converge on the idea that depressive reaction has evolved as an adaptive response to insurmountable adversity, where behavioral and hedonic withdrawal is the main adaptive strategy achieved by downregulation of the motivation/reward system.
Evolutionary theory may provide useful guidance for psychotherapeutic intervention because it considers depressive response an adaptation and, accordingly, focuses on the strategies distressed organisms use to adapt to adversities and on those strategies’ effectiveness and weakness. This view is compatible with the main goals of therapeutic encounter, where better emotional, behavioral, and cognitive responses to the patient’s predicament are sought. Indeed, a recently developed therapy for depression is based on evolutionary theory and aims at facilitating adaptive depressive response (Krupnik, 2014).
From the epidemiological standpoint, evolutionary theory does not offer a clear prediction regarding the rates of depression in populations with chronically elevated stress, as marginalized groups are believed to be. On one hand, such groups are expected to manifest higher frequency of depressive symptoms, if we consider those symptoms adaptive reactions to stress. On the other hand, we might not expect a higher rate of debilitating depression than in the general population, as these individuals may develop greater resilience, and low intensity depressive response may provide sufficient protection. Indeed, it has been argued that although short people experience psychosocial pressure related to their SS, they are able to use their resilience mechanisms to compensate for this disadvantage (Sandberg & Colsman, 2005; Sandberg & Voss, 2002). Epidemiological studies comparing SS people with the general population commonly use health-related quality-of-life questionnaires that include questions about symptoms of anxiety and depression (Coste et al., 2012). Although these questionnaires quantify people’s perception of their general mental health as affected by “stress, depression, and problems with emotions,” they do not identify the presence of clinically significant syndromes such as depressive, anxiety, or stress-related disorders. It is assumed that all symptoms on the continuum of severity indicate psychological deficit or poor adjustment.
This raises two related questions. If symptoms of depression are a manifestation of an adaptive depressive response, is there a level of severity, where such response becomes maladaptive? If indeed there is a threshold, where adaptive depressive response turns maladaptive, does it correspond to the symptoms severity constituting a syndrome diagnosed as clinical (major) depression?
Regarding the first question, there are two main groups of evolutionary theories, whose opinions differ. Some argue that only depressive symptoms/traits are an adaptation, while depression as an illness is maladaptive—the “soft” theory (Gilbert & Allan, 1998; Nesse, 2000; Sloman, Gilbert, & Hasey, 2003), whereas others maintain that depression as an illness is adaptive too—the “hard” theory (Hagen, 1999; Price et al., 1994; Watson & Andrews, 2002). With respect to the second question, some psychiatrists believe that up to a certain threshold depressive symptoms do not constitute pathology and that the current classification of depressive disorders is too inclusive, which has led to overdiagnosing of depression (Parker, 2007; Wakefield & Schmitz, 2013). Indeed, in DSM-5, the diagnosis of major depression includes four levels of severity, and there are several additional diagnoses of depressive disorders.
The premise that up to a certain degree of severity depressive symptoms do not represent a deficit or pathology but are a manifestation of adaptive response to stress could reconcile the controversy about the effect of SS on mental health. Both sides may be correct in their assertions: SS people may experience higher stress and manifest more depressive symptoms but not necessarily suffer from higher rates of clinical/major depression. The available data lack the diagnostic specificity needed to make such conclusion.
End of the Controversy?
We believe that controversy about the effects of SS is partly due to (a) pathologizing the issue and (b) insufficient specificity in asking the questions about SS. As has been persuasively argued by the opponents of the use of growth hormone therapy for enhancement purposes, idiopathic SS is not an illness (Sandberg & Colsman, 2005). Whereas it is true that tall men have a significant and consistent advantage over short ones (Nettle, 2002), it appears no more of a health issue than the advantage attractive people have over less attractive ones. Then it becomes a personal choice whether and how to compensate for it.
It appears rather obvious that a general question whether size matters has been answered positively. However, it is also clear that it matters, where it matters. We believe that contradicting findings about the effects of SS resulted in part from the lack of agreed on specific target groups and that future research should address this possibility. According to our hypothesis, the effects of SS should be greatest in groups with intense intramale social competition, especially where physical prowess and appearance count. Our sample of young military men is but one example. Another prediction of our hypothesis was that men would be more affected by SS than women as height had presumably less importance for female social status. Indeed, mental health of men but not women was found to be affected by SS (Coste et al., 2012). In a recent large epidemiological study, the authors have shown that after controlling for a significant number of variables affecting life quality, such as health, socioeconomic status, and life circumstances, SS still has a significant negative effect on the sense of well-being in young men (Carrieri & De Paola, 2012). They have also shown that most important is the perceived stature, that is, body height relative to the reference group, which confirms the notion of stature as a marker of social status in young men. The importance of perceived stature has been recently demonstrated in an elegant experiment, where the perceived stature of the participants was manipulated with a virtual reality device (Freeman et al., 2013).
Should future research confirm our hypothesis that SS in men increases their vulnerability to depression, it will have a straightforward practical application. To our knowledge, there are no preventive programs specifically targeting shorter boys. We believe that such programs implemented in school could be beneficial for them in developing higher resilience to the pressure of low social status based on body height. It has been documented that parents sometimes opt for growth hormone therapy to increase their children’s height, a practice of questionable effectiveness, which has raised safety and ethical concerns (Sandberg & Colsman, 2005; Sandberg & Voss, 2002). Psychological intervention would obviate those concerns and may prove effective in long-term outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.