
Abstract
Self-criticism represents a central phenomenon among a variety of psychological distress and has been shown to relate to the motivational systems of competing and social ranking. The purpose of our study was to test the effect of online compassion-focused therapy (CFT)-based intervention (CFI) on Chinese international students in South Korea suffering from high self-criticism and related psychological distress. Thirty-two Chinese international students with a high level of self-criticism were randomized to either a four-session CFI group, a four-session rational emotive behavior therapy (REBT)—based online self-help approach group, or a wait-list (WL) control group. The results suggest that the CFI group demonstrated significant improvements in self-criticism, compassion, depression, anxiety, and shame, and these were greater than those in the REBT and WL groups. Our work provides evidence that CFI offers a possible approach for reducing self-criticism and related psychological distress and increasing compassion level for young Chinese populations.
Keywords
Introduction
In China, educational competition (referred to as the “enthusiasm for education”) is considered the only way to promote social ranking and has become an increasingly serious issue. This phenomenon has been suggested to relate to self-criticism and to have negative effects on psychological health (Gilbert, 2014). Evidence from a comparative study of high school students from China, Japan, Korea, and the United States (Zhao & Zhu, 2010) revealed that Chinese high school students reported greater levels of stress than those from other countries, with the biggest stressor being parents requiring them to enter the top 10 schools, reported by 24.5% of Chinese students. The second biggest stressor was high self-expectations, which refers to an individual’s inner expectation of achieving perfection and being competitive. Moreover, most Chinese students reported being depressed (76.7%), having anxiety (76%), and suffering from insomnia (47.4%). The researchers also suggested that the stress experienced by Chinese students is possibly becoming more and more internalized and repressed. According to Gilbert (2014), these findings supported that social ranking competition breeds self-criticism and could contribute to psychological distress.
Attention should also be paid to the mental health of Chinese international students in Korea. According to the data from the Korean Ministry of Education (2020), there are 67,030 Chinese international students in South Korea, which accounts for the largest portion (43.6%) of international students. However, Chinese international students have been reported to experience maladjustment and acculturative distress in their academic and daily lives (Gu et al., 2017; Gu & Hyun, 2021; Lim & Ham, 2009) and to be at a high risk of depression or depressive symptoms (H. J. Lee, 2011). Gu et al.’s (2017) research also revealed that shame has a significant relationship with maladjustment for Chinese international students. Moreover, self-criticism has been reported to be significantly associated with shame (Gilbert & Miles, 2000; Gilbert & Procter, 2006). Therefore, it seems necessary to consider Chinese international students’ psychological health as important and to recognize that they may suffer from self-criticism and related psychological distress (such as shame and/or depression).
Gilbert’s (2014) model of self-criticism is based on a cognitive–evolutionary perspective. A recent review on self-criticism summarized Gilbert’s model that self-criticism relates to the phenomenon within the motivational system for competing and social ranking (Werner et al., 2019). Other motivational systems suggested by Gilbert (2014) include those for cooperating and sharing, caring, and nurturing, and seeking and responding to care. Regarding the development of self-criticism, as the self-to-self relationship is built on interpersonal experiences (others-to-self relationships), self-criticism develops with experiences that take place within the motivational system for competing and social ranking. When self-criticism is developing, the system of self-reassurance develops out of the interpersonal experiences of caring for and nurturing others and the possibility of seeking and receiving care when in need. Therefore, individuals with higher levels of self-criticism tend to rely on dominant–submissive interpersonal schemas (Interpersonal Circumplex Model; Leary, 1957) with others and in their self-to-self relationship (Werner et al., 2019). This self-critical mode tends to be more automatic and the possibility of emergence for a compassionate and kind self-to-self mode decreased (Gilbert, 2014). These unbalanced motivational systems are supported by studies on neurophysiological correlations between self-criticism and self-reassurance (Longe et al., 2010). Self-criticism engenders a depressive vulnerability when the soothing/affiliative system is not working on self-reassurance (Gilbert et al., 2006). According to Werner et al. (2019)’s review, correlations of self-criticism with depressive symptoms have been found consistently in studies with clinical samples (e.g., Dinger et al., 2015; Ehret et al., 2015; Straccamore et al., 2017) as well as non-clinical samples (e.g., Liu et al., 2012; Sturman et al., 2015).
Self-criticism has also been reported to be significantly associated with shame proneness (Gilbert & Miles, 2000; Gilbert & Procter, 2006). Self-criticism and shame are both trans-diagnostic, cause many disorders, rise the possibility of vulnerability, affect the appearance of symptoms, and increase the risk of relapse (Gilbert & Irons, 2004; Tangney & Dearing, 2002; Zuroff et al., 2005). Vulnerability to shame-based self-criticism is commonly rooted in memories of the self being rejected, criticized, and shamed (Gilbert, 1989/2016, 1998, 2002; Gilbert & Irons, 2004; Kaufman, 1989) and/or abused (Andrews, 1998). In a longitudinal study (Stuewig & McCloskey, 2005) with children samples, over an 8-year period, shame as a self-conscious emotion was mediated by parental humiliation and rejection. Therefore, shame seems to push people into a ruminative self-critical mode, elevating their vulnerability to a range of difficulties.
A growing body of research has found that self-criticism could be both a vulnerability and maintenance factor in anxiety (Allen & Gilbert, 1997). Positive correlations between self-criticism and anxiety have been reported in clinical (Castilho et al., 2017; Iancu et al., 2015) and non-clinical samples (Campos et al., 2012; Shahar et al., 2015). Castilho et al.’s (2017) research revealed that the two types of self-criticism—seeing the self as inadequate and hating the self—were both significant mediators for anxiety and other psychopathological symptoms.
However, those with a high level of self-criticism have reported that it is difficult to feel relieved by cognitive therapy (D. A. Lee, 2005), and a diminishing mood can provoke self-criticism in recovered depressed individuals (Teasdale & Cox, 2001). Rector et al. (2000) reported that the treatment effect of individuals with high self-criticism in cognitive behavioral therapy (CBT) was less than that of individuals with relatively low self-criticism. Psychodynamic therapists also recognize that a high level of self-criticism and self-persecution may be difficult to treat (Scharffee & Tsignouis, 2003). A meta-analysis (Kirby, 2017) on the effects of compassion-focused interventions concluded that they could be helpful for a broad range of individuals in coping with clinical and nonclinical issues, especially self-criticism, depression, shame, and anxiety (Braehler et al., 2013; Gilbert & Procter, 2006; Kelly et al., 2010; Leaviss & Uttley, 2015; Neff & Germer, 2013). CFT (Gilbert, 2014, 2018) is based on evolutionary psychology integrated with attachment theory, applied psychological science research (neuroscience and social, emotional, and cognitive psychology), social mentality theory, and Buddhist psychology. Its clinical focus is on individual with complex and chronic mental health issues (often having abusive backgrounds), especially those with a high level of self-criticism and shame. Moreover, CFT provides a compassion-focused model of psychotherapy and has no specific time limitations or restrictions for individual (Kirby, 2017). According to Leaviss and Uttley (2015)’s review on CFT, evidence of the effectiveness of CFT includes randomized controlled trials (RCTs) (Arimitsu, 2016; Braehler et al., 2013; Kelly & Carter, 2015; Kelly et al., 2010), non-RCTs (Ashworth et al., 2014; Gale et al., 2014; Gilbert & Irons, 2004; Gilbert & Procter, 2006; Heriot-Maitland et al., 2014; Judge et al., 2012; Kelly et al., 2009; Lucre & Corten, 2013), and case studies (Ashworth et al., 2011; Beaumont & Martin, 2013; Boersma et al., 2014; Bowyer et al., 2014; Mayhew & Gilbert, 2008). Recently, Craig et al. (2020) reviewed CFT’s effectiveness and acceptability focusing on clinical population. According to their expert opinions, CFT shows promise for borderline personality disorder, eating disorders, depression, psychosis, opioid use disorder and mothers of children with ADHD who have depression, especially when delivered in a group format over at least 12 hours; and CFT is demonstrably well accepted by clients and clinicians. Therefore, CFT is mainly based on the science of psychology as well as CBT, focuses more on clinical populations who could understand the logic of CBT and generate alternative thoughts to self-criticism but rarely felt reassured by such efforts (D. A. Lee, 2005). Given the evidence from previous work, it is important to apply compassion-focused interventions with Chinese youth.
Given the rapid development of media technologies, counselors and practitioners have been exploring the therapeutic potential of online media since the late 1990s. Although compassion-focused interventions are traditionally delivered by professionals using a face-to-face format, a recent review on the online format of psychotherapy (Stoll et al., 2020) suggests this could offer more cost-effective and beneficial approach in situations in which face-to-face interventions are not available, such as the current COVID-19 pandemic. Moreover, most Chinese students are not familiar with psychological counseling or intervention and may feel uncomfortable or worried about not just the counseling process but also being at an unfamiliar place. An online format may be beneficial to them because they may feel safer and more comfortable at home (a usual place to engage in online counseling) than at a strange counseling center or institution.
As a typical example of the Chinese youth who are potential victims of education competition, Chinese international students might benefit from CFT-based intervention (CFI). As a review work on CFT suggested, more RCTs with active controls, follow-ups, consistent use and reporting of measures and diverse samples are needed (Wakelin et al., 2022). Present work is an important attempt to determine whether online CFI works for those Chinese students who have a high level of self-criticism. Therefore, the aim of the present study was to test the effect of online-based CFI on depression, anxiety, and shame through an RCT with Chinese international students who have a high level of self-criticism. The study addressed two hypotheses: (1) the level of self-criticism, depression, anxiety, and shame in the CFI group would reduce and the compassion level would increase; (2) the effect on the CFI group would be greater than that on the comparison (REBT) group and greater than that on the wait-list (WL) control group.
Method
Participants
Chinese international students in South Korea were recruited through online networks for international students. The final baseline sample consisted of 32 participants from the community enrolled in the RCT divided into three groups: CFI, n = 10; REBT, n = 10; WL, n = 12. The participants’ average age was 22.50 (SD = 2.41) years (range: 18–28). There were 4 males and 28 females in this sample. The participants were undergraduate (n = 20, 62.5%) and graduate students (n = 12, 37.5%). Their level of Korean proficiency (a National Korean Proficiency Test for foreigners; the higher of the sublevel, the greater of Korean proficiency) was distributed as follows: level 3: n = 2, 6.3%; level 4: n = 13, 40.6%; level 5: n = 9, 28.1%; level 6: n = 8, 25.0%. The characteristics of participants at baseline are presented in Table 1 and there was no significant differences between the three groups in gender, age, education level, and Korean proficiency.
Characteristics of Participants at Baseline.

Note. Dep = depression disorder; Anx = anxiety disorder; Bipolar = bipolar disorder; OCD = obsessive-compulsive disorder.
Measures
Self-criticism Scale of the Depressive Experiences Questionnaire (DEQ-SC)
The DEQ (Blatt et al., 1976; Chinese version: Ning et al., 2006) is a self-report questionnaire constructed to assess a wide range of experiences of depression. Three factors emerged from the DEQ: dependency, self-criticism, and efficacy, consisting of 66 items rated on a 7-point scale (1 = strongly disagree to 7 = strongly agree). This study applied 15 self-criticism related items as a screening tool. The DEQ-SC presented a Cronbach’s α = .57 (the Cronbach’s α’s reported for this study correspond to the first application of the instruments for the three groups combined).
Other as Shamer Scale (OAS)
The OAS (Goss et al., 1994; Chinses version: Yang et al., 2019) measures external shame, or the belief that others look down on and negatively judge the self (Goss et al., 1994). The original version is an 18-item scale and includes statements such as “I think that other people look down on me” and “Other people look for my faults” that are rated on a 5-point Likert scale (0 = never to 4 = almost always). In the original study, the scale showed good reliability with α = .92. The Cronbach’s α of the OAS used in this study was .93.
Chinese Compassion Scale (CCS)
The CCS (Gu, 2021) is a self-report scale with 25 items, each of which is scored using a 5-point Likert scale (1 = not at all true of me to 5 = very true of me). The scale focuses on four factors: sensitivity to others (STO), kindness to others (KTO), kindness to self (KTS), and tolerance of uncomfortable feelings (TUF). In the original study, the scale provided a good reliability with Cronbach’s α = .81, and in this study, the Cronbach’s α was .73.
Self-Compassion Scale (SCS)
The SCS (Neff, 2003) is a self-report scale, which consists of 26 items measuring six elements of self-compassion (self-kindness, self-judgment, common humanity, isolation, mindfulness, and over-identification) rated on a 5-point Likert scale (1 = almost never to 5 = almost always). The Chinese version of the SCS translated by Chen et al. (2011) was employed in this study. The Cronbach’s α in Chen et al.’s (2011) study was .84, and the test–retest reliability was .89. In this study, the Cronbach’s α was .92.
Depression
The Beck Depression Inventory (BDI-II; Beck et al., 1996; Z. Wang et al., 2011) is a 21-item scale that measures cognitive, behavioral, and affective symptoms of depression. Items are rated on a 4-point Likert scale where 0 = symptom is not present and 3 = severe symptom manifestation. The Chinese version of BDI-II in Z. Wang et al.’s (2011) study showed good validity and reliability (Cronbach’s α = .94). In this study, Cronbach’s α was .91.
Anxiety
This study employed the trait form of the Speilberger State–Trait Anxiety Inventory (STAI-T; Spielberger et al., 1983), a commonly used 20-item anxiety questionnaire that evaluates relatively stable aspects of “anxiety proneness,” including general states of calmness, confidence, and security. Responses were given on a 4-point scale (ranging from 1 = almost never to 4 = almost always). The Chinese version used in the present study was translated and validated by Li and Qian (1995, Cronbach’s α = .88). The Cronbach’s α was .87 in this study.
Research Design and Procedure
A screening test was conducted online to recruit potential participants. The Self-criticism Scale of the Depressive Experiences Questionnaire (DEQ-SC) (Blatt et al., 1976) was employed as the screening test tool. Before the screening test, all responders were informed about the general aspects of the study and the commitment involved in enrolling as a potential participant. Only responders in the screening test with a DEQ-SC score over 70 were enrolled as participants in the RCT. The cutoff score of the DEQ-SC was defined based on a pilot investigation (n = 209) to obtain the top 15% of the Chinese sample (M = 54.81, SD = 13.91). In total, 93 participants completed the screening test and 47 met the cutoff score, however, 14 declined to participate (ten could not be contacted and four refused). Those participants who had signed the online informed consent and completed the online pretest were randomly assigned to the CFI, REBT, or WL group by using a computerized random number generator. Only two participants in the REBT group dropped out (one lost contact after the first lecture and another did not finish the post-test questionnaires). The CFI program was offered to the WL and REBT groups (optional) at the end of the research. Figure 1 depicts the procedure.

Research design and procedure of this study.
Intervention Protocols
The CFI group participated in a 4-week CFI program consisting of attending weekly 2-hour online individual counseling sessions. The CFI program, based on CFT (Gilbert, 2018; Kolts, 2016, see Supplemental Material: CFI protocol), mainly included cognitive education regarding the three emotion regulation systems, finding and validating the inner critical voice, imagery practice, and meditation practice (mindfulness meditation and compassion meditation), which are from the Mindful Self-Compassion program (MSC, Neff & Germer, 2013). All participants were required to commit to 20 min of daily home practice (MP3 files with guided meditation were provided). Participants were also asked to continue doing home practice in the 2-week follow-up.
The professional counselor who engaged with the CFI group was the researcher (a qualified clinical psychologist in South Korea). Researcher allegiance bias may occur when the researcher is also the counselor (Leykin & DeRubeis, 2009). However, there are several ways to control this bias: (1) using reflectors (trained professionals); (2) using persons outside of the investigation to conduct the pre-, post-, and follow-up tests and prohibiting the researcher from participating in the data collection; and (3) analyzing the results of each case with independent coders of the pre-, post-, and follow-up test phases. The third approach was applied in this study.
The REBT group also participated in a 4-week REBT-based self-help approach, which consisted of attending a 2-hour online lecture each week. The REBT lecture protocol (Chinese version of Rational Emotive Behavior Therapy, Ellis & Ellis, 2015) was revised to focus on self-criticism and arranged into a 4-week structure to match the CFI program. In each lecture, one sample case and one case analysis were shared, and participants were asked to apply it to themselves as home practice. This work was conducted by a Chinese-speaking professional counselor, qualified in psychological counseling in South Korea. Participants in the REBT group were also required to engage in REBT home practice during the sessions and the 2-week follow-up.
Data Analysis
Participant characteristics were examined using descriptive statistics. The normality hypothesis was assessed by the Shapiro–Wilk test and homoscedasticity assumptions by Levene’s test for equality of variances. Sphericity was tested by Mauchly’s test, and the value of Greenhouse–Geisser was reported when the value of W was significant (p < .05). A one-way ANOVA was conducted to test the homogeneity of the three groups at baseline. A paired sample t-test was carried out for mean difference changes between the pre- and post-tests and between the pre- and follow-up tests within groups. A mixed repeated ANOVA was run to test the interaction effect between the two conditions (Time × Group) on all the dependent variables. All statistical analyses were performed using IBM SPSS version 23 for Windows.
Results
Preliminary Analyses
Shapiro–Wilk tests for normality were non-significant for all dependent variables at baseline, revealing normal distribution of data (except for DEQ-SC and BDI-II). Therefore, power transform was used to convert these data to normal distributions by taking the natural logarithm of the values. Levene’s test was non-significant for all variables, indicating equality of variances. Results of the one-way ANOVA (Table 2) suggested that there were no significant differences in any of the dependent variables between groups, indicating homogeneity of the three groups. The post hoc tests also suggested no significant differences between groups. This sample also demonstrated a high level of psychological symptoms. Given that a BDI-II total score of 0–13 is considered to reflect minimal depression, 14–19 is mild, 20–28 is moderate, and 29–63 is severe (Y. Wang & Gorenstein, 2013), the present sample (M = 27.28, SD = 11.49) reported a moderate level of depression. The level of anxiety for this sample (M = 59.65, SD = 9.71) was higher than the mean score (SD) of 36 (9) in STAI-T for working adults (Spielberger et al., 1983). The level of external shame (M = 35.68 and 14.39) was also higher than that of other samples (college student sample: M = 20.0, SD = 10.1, Goss et al., 1994; general population sample: M = 16.24, SD = 8.31, Balsamo et al., 2015).
Results of One-Way ANOVA for CFI, REBT, and WL at Baseline (Pretest).

Note. DEQ-SC = Self-criticism Scale of the Depressive Experiences Questionnaire; CCS = Chinese Compassion Scale; SCS = Self-Compassion Scale; BDI-II = Beck Depression Inventory II; STAI-T = Trait form of Speilberger State–Trait Anxiety Inventory; OAS = Other as Shamer Scale.
Mean Difference Changes in Groups
The results of the paired sample T-test for the CFI group are presented in Table 3. The results suggest that the mean difference changes between the pretest and post-test on all dependent variables were significant, and these changes remained at follow-up. That is, after the intervention, the CFI group showed improvement in self-criticism, compassion, depression, anxiety, and shame, and the positive changes remained at follow-up. Moreover, the mean difference changes in the four factors of the CCS were also tested. Interestingly, although the mean difference changes between the pre- and post-test on KTS and TUF were significant, those on STO and KTO were not. This result also remained at follow-up.
Results of Mean Difference Changes in Groups.
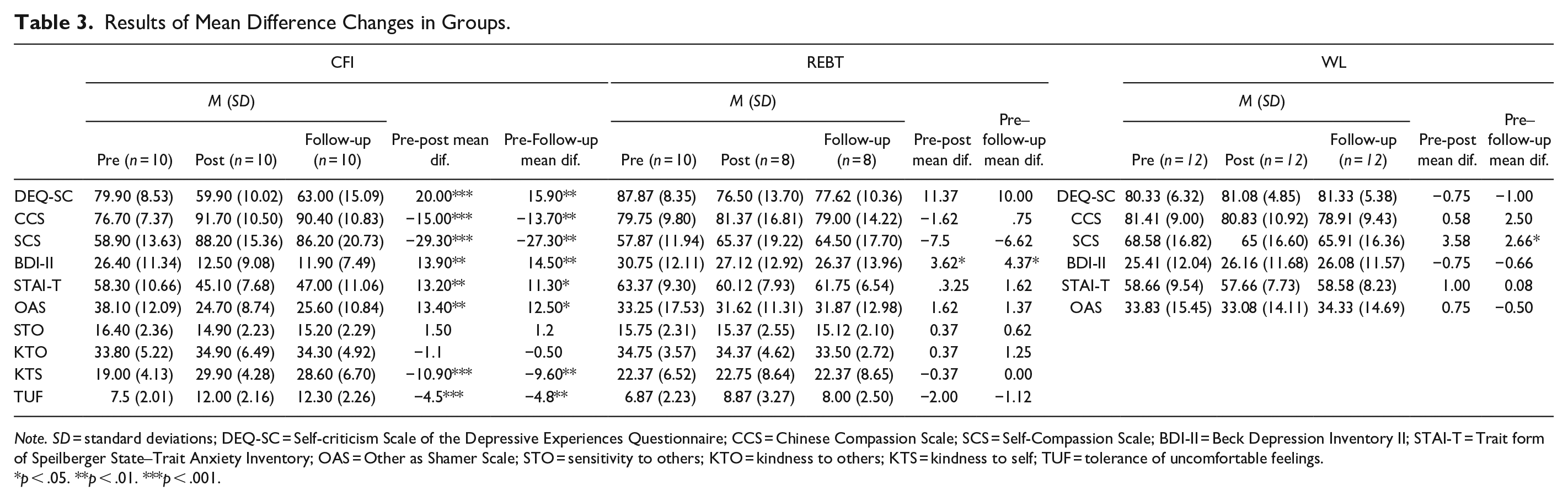
Note. SD = standard deviations; DEQ-SC = Self-criticism Scale of the Depressive Experiences Questionnaire; CCS = Chinese Compassion Scale; SCS = Self-Compassion Scale; BDI-II = Beck Depression Inventory II; STAI-T = Trait form of Speilberger State–Trait Anxiety Inventory; OAS = Other as Shamer Scale; STO = sensitivity to others; KTO = kindness to others; KTS = kindness to self; TUF = tolerance of uncomfortable feelings.
p < .05. **p < .01. ***p < .001.
The results (Table 3) suggest that the mean difference changes between the pre-, post-test, and follow-up for all dependent variables in the REBT group were not significant, except for BDI-II. That is, the REBT group did not show progress after the program for self-criticism, compassion, anxiety, or shame but did show progress for depression. The results for the WL group (Table 3) also show similar results that all the mean difference changes were not significant, except that the SCS level became worse. Moreover, the effect size of mean differences (pre-post-means) between CFI group and REBT group were as follows: dppc2 = 0.97 for DEQ-SC; dppc2 = 0.83 for BDI-II; dppc2 = 1.47 for CCS; dppc2 = 1.63 for SCS; dppc2 = 0.95 for STAI-T; dppc2 = 0.74 for OAS (Lenhard & Lenhard, 2016). The effect size of mean differences (pre-post-means) between CFI group and WL group were as follows: dppc2 = 0.2.69 for DEQ-SC; dppc2 = 1.20 for BDI-II; dppc2 = 1.84 for CCS; dppc2 = 2.04 for SCS; dppc2 = 1.16 for STAI-T; dppc2 = 0.86 for OAS.
Moreover, the result of CCS suggested that only the mean difference changes between the pre- and post-test of KTS (kindness to self) and TUF (tolerance of uncomfortable feelings) in the CFI group were significant and also remained at follow-up. In addition, all participants reported a lower level of KTS, TUF, and SCS at baseline (mean of total sample, n = 32: KTS = 20.90, SD = 6.33; TUF = 7.15, SD = 2.13; SCS = 62.00, SD = 14.64) than the original sample (Gu, 2021; n = 209; KTS = 31.83, SD = 4.09; TUF = 13.38, SD = 2.99; SCS = 95.29, SD = 12.90). However, the levels of KTO (kindness to others) and STO (sensitivity to others) (KTO: M = 35.31, SD = 4.09; STO: M = 16.19, SD = 2.14) at baseline were close to the original sample (KTO: M = 37.61, SD = 3.69; STO: M = 14.84, SD = 2.90).
Interaction Effect (Time × Group) between Groups
The mixed repeated ANOVA revealed significant interaction effects (Time × Group) on all dependent variables between the CFI group and the WL group (Table 4), where the CFI group presented greater improvements than the control group. The results also revealed significant interaction effects on all dependent variables between the CFI group and the REBT group except for DEQ-SC, where the CFI group showed greater improvements than the REBT group in compassion, depression, anxiety, and shame. Moreover, results of effect size were also presented in Table 4.
Results of Repeated ANOVA (Time × Group) Between Groups.

Note. ηp2 = partial Eta squared; DEQ-SC = Self-criticism Scale of the Depressive Experiences Questionnaire; CCS = Chinese Compassion Scale; SCS = Self-compassion Scale; BDI-II = Beck Depression Inventory II; STAI-T = Trait form of Speilberger State–Trait Anxiety Inventory; OAS = Other as Shamer Scale.
Discussion
The aim of our study was to test the effect of online CFI on depression, anxiety, and shame among Chinese international students with a high level of self-criticism. This work was conducted through an RCT comparing the CFI, REBT, and WL conditions.
The results support Hypothesis 1: participants who engaged in the CFI group decreased their levels of self-criticism, depression, anxiety, and shame and increased their levels of compassion, and the significant mean difference changes were maintained at follow-up. Moreover, post-mean of BDI-II score decreased below the cutoff value of clinical significance as well as follow-up mean. These results are consistent with previous research on CFT that CFT or CFT based programs enhance psychological well-being and improve psychological symptoms. For example, Gilbert’s compassionate mind training (CMT) had significant effects on self-reported anxiety and depression among people with high shame and self-criticism (Gilbert & Procter, 2006), which led to significant decreases in depression, shame, entrapment, and perceived social marginalization among patients with schizophrenia (Braehler et al., 2013). In addition, Arimitsu (2016) developed a new group program called the Enhancing Self-Compassion Program (ESP) based on CFT. Arimitsu (2016) found that ESP significantly improved self-compassion compared to the control group and the effect were maintained at follow-up. Matos et al. (2017) also found significant improvement in positive emotions, compassion level, and HRV; significant reductions in shame, self-criticism, fears of compassion, and stress in a 2-week CMT condition with a randomized control.
The REBT group did not demonstrate any significant mean difference changes except for depression. Although the mean difference changes of BDI-II were significant, the levels of depression at post-test and follow-up were still moderate (Wang & Gorenstein, 2013). As one of the first forms of cognitive-behavioral therapy, REBT has received significant empirical support (such as Dobson, 2000; Lazarus, 1991) and is widely accepted in the clinical field (Dryden et al., 2010). One possible explanation could be that since our sample was practically the same as a clinical population (see Tables 1 and 2), an online self-help approach may not have been enough. According to Haaga and Davidson (1993), for REBT treatment efficacy, clinicians need to pay more attention to methodological criteria, one of which is the adequacy of clinical protocols. Thus, our sample may have needed a more formal clinical protocol, and the REBT-based self-help approach may be adequate for nonclinical populations with the aim of preventative psychoeducation. Future studies should therefore focus on the adequacy of protocols.
The results also support Hypothesis 2: participants who engaged in the CFI group increased their levels of compassion and decreased their levels of self-criticism, depression, anxiety, and external shame more than the WL group. Although there were no significant interactions (Time × Group) in terms of self-criticism, the CFI group presented more significant improvements in levels of compassion, depression, anxiety, and external shame than the REBT group. To the best of our knowledge, this study is the first to test CFT-based intervention focusing on a Chinese sample using a RCT. The results indicate that this intervention did help those Chinese students suffering from self-criticism and related psychological symptoms. A recent RCT study on CFT also reported that CFT operated by cultivating self-reassurance, reducing self-criticism, and regulating positive and negative affect in a nonclinical sample. Further, the effects of CFT were significantly mediated by self-reassurance and self-criticism (Sommers-Spijkerman et al., 2018).
There were also several noteworthy findings. First, unsurprisingly, 50.5% of Chinese international students in the initial sample met the cutoff score of 70 (DEQ-SC) at the screening test, indicating that the mental health of Chinese international students might be at risk and thus it deserves more attention. Second, the result of CCS suggested that only the mean difference changes between the pre- and post-test of KTS and TUF in the CFI group were significant and also remained at follow-up. This finding indicates that the CFI did help participants raise the level of self-kindness and tolerance of distress but no other-kindness or sensitivity to others. Moreover, all participants reported a lower level of KTS, TUF, and SCS at baseline than the original sample. However, the levels of KTO and STO at baseline were close to the original sample (Gu, 2021). This finding indicates that those young Chinese students suffering from self-criticism and related psychological distress were low in KTS and TUF but might not have a low level in STO or KTO. It may suggest that those who are suffering from self-criticism and related distress might be sensitive to others’ pain and could be or want to be kind to them, but they can do nothing about their own suffering. A recent study (López et al., 2018) also found that compassion for others was not significantly related to self-compassion among a general population. Future studies are needed to explore the relationship between self- and other compassion across different samples.
Limitations and Future Directions
There are some limitations of this study that should be discussed. First, the comparison trial was weak. Although there were interactions between the professional counselor and participants through personal questions and feedback by email, the REBT-based self-help approach was a psychoeducation program rather than an intervention. Further research should compare CFI to standardized interventions. Second, the CFI program only consisted of four 2-hour sessions (total in 8 hours) and the follow-up was only 2 weeks. A recent review (Craig et al., 2020) reported a dose of at least 12 hours for more lasting effects in a group format. More studies should be conducted to test how long the positive changes last. Third, the sample in our study was small and the sex ratio is unbalanced. Future research should test the effect of CFI with larger and different samples, including clinical and nonclinical samples with a balanced sex ratio.
In conclusion, our study was the first attempt to apply CFI to Chinese students suffering from self-criticism and related psychological distress using an RCT. The results suggest that the CFI group showed greater improvements in self-criticism, compassion, depression, anxiety, and shame than the control and comparison groups. This work provides evidence that CFT-based intervention for reducing psychopathology and increasing well-being is effective for Chinese students, although more research is needed to replicate and explore the effects of CFT-interventions.
Footnotes
Acknowledgements
We would like to thank EssayReview (EssayReview.co.kr.) for English language editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The manuscript does not contain clinical studies or patient data. All study procedures were approved by the Institutional Review Board of the appropriate university (IRB; 1041078-201911-HRSB-349-01). Informed consent was obtained from all participants included in the study.