
Abstract
Prisons are considered high-risk environments for HIV transmission. This study aimed to measure HIV and syphilis prevalence and risk behaviors among inmates in Indonesia. An integrated HIV and syphilis biological and behavior survey was conducted on random samples of 900 male and 402 female inmates in 2010. Male inmates from 18 general prisons and detention centers were randomly selected using probability proportional to size. Female inmates were randomly selected from nine eligible institutions. HIV tests included two rapid tests and enzyme-linked immunosorbent assay (ELISA) for quality control. A rapid test was used for syphilis. Audio computer-assisted self-interview was used for collecting risk behavior information. HIV prevalence was 1.1% among male and 6.0% among female inmates. Syphilis prevalence was 5.1% for male and 8.5% for female inmates. A history of injecting drugs was the most important risk factor for HIV infection in male inmates; for females, it was co-infection with syphilis and being sentenced for illicit drug use. Inmates’ high-risk activities in prison included tattooing, piercing and inserting genital accessories without sterile equipment, and sex without condoms. The study found high-risk practices by male inmates and high HIV and syphilis prevalence in female inmates. Inmates need harm reduction initiatives.
Keywords
Introduction
Most men and women in Indonesia who have acquired HIV have a history of either injecting drug use, sex work, or of being a client of a sex worker (Indonesian National AIDS Commission, 2012). There have been numerous papers published about the association between HIV and syphilis and other sexually transmitted infections (STIs) among sex workers, transgender people, and men who have sex with men (MSM) in Indonesia (Magnani et al., 2010; Morineau et al., 2011; Pisani et al., 2004; Prabawanti et al., 2011; Sugihantono et al., 2003). Men who are considered high risk in Indonesia, based on their occupation and sexual risk taking, have been shown to have a low prevalence of HIV but a high rate of STIs, especially syphilis, with truck drivers being the most at risk (Mustikawati et al., 2009).
Given that some prisoners have a history of injecting drug use or sex work, some will already have HIV and/or syphilis before they enter prison. In one survey conducted in an Indonesian prison for drug-related offenses, prison entrants had an HIV prevalence of 7.2%, which was almost entirely related to injecting drug use (Nelwan et al., 2010). HIV may be of high risk for prisoners if they have limited access to sterile equipment for injecting drugs, tattooing, or piercing or inserting genital accessories.
Many studies have reported female inmates having a higher prevalence of HIV than male inmates (Butler & Papanastasiou, 2008; Strazza, Azevedo, & Massad, 2004; United Nations Office on Drugs and Crime, 2008). The most significant risks for HIV infection in women in prison have been reported to include HIV-infected sexual partners, casual sexual partners, injecting drugs, partners who inject drugs, sex work, and a history of STIs (Keinman, 2007; Miranda, Vargas, St Louis, & Viana, 2000). Studies have shown that women are at least twice as likely as men to contract HIV through sex, and STIs greatly increase the risk of contracting HIV (Butler & Papanastasiou, 2008). The proportion of women in prison with an STI has been reported as relatively high in several studies (Keinman, 2007; Miranda et al., 2000; World Health Organization [WHO], 2005). There have been no studies on the prevalence or association of HIV and syphilis conducted for women prisoners in Indonesia and little is known about their risk activities while in prison.
There have been several studies of individual prisons in Indonesia, although there have been limited studies of HIV and syphilis prevalence and associated risk behavior. The studies conducted have been in a few selected prisons where a significant proportion of their inmates may or may not have a history of illicit drug use. These studies do not represent the general prison population and may indicate pocketing of HIV epidemics in some prisons. International studies in prisons have shown a high prevalence of syphilis and HIV among prisoners (Adjei et al., 2008; Jurgens, Nowak, & Day, 2011; Stőver, Weilandt, Zurhold, Hartwig, & Thane, 2008). Few national studies have been conducted internationally to determine HIV and syphilis status and risk behavior in prisoners with studies from single prisons or regions unable to reflect national prevalence (Adjei et al., 2008; Jurgens et al., 2011; Weinbaum, Sabin, & Santibanez, 2005). Information about HIV prevalence and risk behaviors in prisons nationally among male and female prisoners is essential for developing an evidence-based HIV and syphilis control program for closed settings.
The objectives of the study were to determine the prevalence of HIV and syphilis in male and female inmates in general prisons and detention centers; prisoner characteristics; risk behaviors including injecting drugs, tattooing, piercing and inserting genital accessories, and sex; and access to services. The information is required to better understand the situation within prisons and detention centers to assist the Ministry of Justice and Human Rights to develop effective policies and to inform the design, implementation, and evaluation of HIV prevention and harm reduction programs in prisons and detention center in Indonesia.
Method
The study was voluntary and was approved by the Indonesian Ministry of Justice and Human Rights and Research Expert and Ethics Commission at the Faculty of Public Health, University of Indonesia.
A cross sectional design was used to sample male and female prisoners from prisons. There are an estimated 201 prisons and 201 detention centers in Indonesia, which held 74,927 male inmates in early 2010. Detention centers include both sentenced inmates and people on remand who are waiting to be sentenced. A two-stage-cluster random sampling was used to sample male prisoners. Prisons and detention centers were included in the sampling frame if they had at least 120 male prisoners above the age of 18 years and accessible within an hour driving radius from a routinely accessible airport. Smaller prisons were excluded due to the potential impact on prison officials. Overall, 125 prisons and 24 detention centers fulfilled these criteria. The prisons and detention centers excluded by the criteria held 27% of the male prisoners reported in Indonesia in early 2010.
A similar approach was used for sampling women, of whom there were 3,679 in 150 prisons and 127 detention centers; except that the lower limit per prison was 100 and the target sample size was 400. Four prisons and one detention center were eligible based on numbers but a further three detention centers with both male and female inmates were also chosen to represent women from mixed prisons. The second stage included randomly selecting 50 prisoners from each prison and a mixed number from detention centers, depending on the number of female inmates, using a list of inmates with the sample representing 7.9% of all women prisoners in prisons and detention centers.
Prisoners who were invited to participate in the survey were given an explanation about the aims, procedure, advantages and impact of being involved. Advantages included referral to voluntary counseling and testing (VCT) and treatment if infected, education on risk factors, and contributing to research to assist with designing prison programs to prevent HIV in the future. They could then choose whether or not to participate, and if they wanted to be involved, they had to consent verbally. A witness, the Audio Computer-Assisted Self Interview (ACASI) operator, signed the consent form to protect the participants’ identity. Consent was obtained for both the questionnaire and blood sample although they were allowed to stop participating at any stage. Inmates were excluded if they could not read or follow the ACASI instructions after consenting to participate; prison’s officers judged that they had profound intellectual disabilities, acute mental illness, or could not be safely moved to the interview area; were unavailable due to being transferred, in court or hospital.
Inmates who provided consent were interviewed using ACASI, with the Questionnaire Development System (QDS) version 2.6 used to program the ACASI questionnaire, in a room supervised by the ACASI operator. Respondents listened to the questions through headphones and responded by computer keystroke. Interviewers explained how to use the computer and provided assistance if needed. Data collected through interview included demographic characteristics; risk behaviors both in and out of prison such as sexual behavior, drug use, tattooing, piercing and inserting of genital accessories; knowledge about HIV; and use of programs related to HIV and drug use in and out of prison.
After completing the questionnaire, participants were asked to provide a capillary blood sample by finger prick for testing for HIV and syphilis. Each participant was provided with a referral card to access VCT and STI services in appointed health facilities as test results from the study were not available to participants. The number of referrals to services was recorded for each prison. A trained laboratory technician was responsible for organizing the collection of blood to test for HIV and syphilis. Two rapid HIV tests were conducted including Oncoprobe and Determine for HIV with enzyme-linked immunosorbent assay (ELISA) conducted for all cases positive on both rapid tests and 10% of a random selection of those negative on one or both, at the National Health Research and Development Laboratory for quality control. A rapid test, Determine, was used to test for syphilis.
Data were analyzed using Stata SA11. The prevalence of HIV and syphilis infections and 95% confidence intervals (CIs) were calculated separately for male and female participants. Prevalence odds ratios (ORs) were used as the measure of association between risk factors and infections. Logistic regression was used for multivariate analysis. Statistical significance was set at a 5% alpha level.
Results and Discussion
Response Rate
The overall refusal rate among those selected was 6% in males and 5% in females and ranged from 0% to 27% per facility. Reasons for not participating were not provided by inmates. A total of 1,302 inmates (900 men and 402 women) agreed to participate in the study. See Table 1 for information.
Number of Prisons, Detention Centers, and Prisoners in Study.

Note. DC = Detention Center.
At least 120 male prisoners.
At least 100 female prisoners.
At least 100 female prisoners.
Mixed sex DCs with female prisoners selected based on logistical access.
Background Characteristics
The average and median age of male participants was 32 years (SD = 10) and females 34 years (SD = 9). At least a secondary school level of education was started by 75% of females and 62% of males. Being divorced was reported by 8% of males and 25% of females. See Table 2 for the information.
Percentage Participants by Characteristics by Gender.

Prevalence of HIV and Syphilis
Overall, there were 10 male and 24 female participants found to have HIV in the prisons and detention centers, giving a prevalence of 1.1% and 6.0%, respectively. For those with a history of injecting drugs, the HIV prevalence was 8.0% in males and 12.0% in female prisoners compared with 0.5% and 5.6% who did not.
A higher proportion of male respondents in detention centers (1.6%) were HIV positive compared with those in prisons (0.9%). A slightly higher proportion of females in detention centers (6.4%) tested positive for HIV compared with those in prisons (5.5%).
Prevalence of syphilis in general prisons was 5.1% in male and 8.5% in female inmates.
Location of female detention centers and prisons was relevant to the HIV prevalence with 9.8% of female inmates in prisons and detention centers in the Jakarta region testing positive for HIV compared with 3.2% of female inmates in all other locations (OR = 3.3, 95% CI = [2.0, 5.5], p = .00). HIV cases were more evenly spread among male prisons and detention centers in all locations.
Risk Behavior
A history of illicit drug use was reported by 42% of female and 38% of male respondents with 8% of male and 6% of female respondents reporting having injected drugs. No female respondents and six (0.7%) male respondents reported having injected in the current prison. Only one male respondent and no female participants reported injecting drugs for the first time in prison.
Of the six male respondents who reported injecting in prison, none reported sharing used needles. Needle Syringe Programs (NSP) are included in the Indonesian guidelines for Comprehensive Services for HIV/AIDS, and STIs in Correctional Institutions, although there were no prisons that had officially sanctioned NSP at the time of this study, even though some prisoners did report receiving sterile needles and syringes in some prisons.
Ever having sex in prison was reported by 50 male (5.6%) and 15 female (3.7%) respondents with 25 (2.8%) male and 5 (1.2%) female respondents reported having had sex in the current prison. Of those who reported having had sex in prison, most had heterosexual sex. Most sex was with regular partners (68%), such as wife or girlfriend or boyfriend who visited, although 4 men reported having anal sex with another prisoner and 9 reported “other” people. No respondents reported having sex with a prison officer. The average frequency of having sex in prison in the last month was once with a range of 0 to 9 times. The use of condoms in prison was very low with only 3 (6%), 5% of males and 10% of females, reported using condoms at last sex and 2 reported always using condoms in the last year.
Having a tattoo was reported by 42% of male respondents and 14% of female respondents (14%), with 167 (19%) males and 6 (1%) females having tattoos done in prison.
Body piercing in prison was reported by 6% of male respondents and 3% of female respondents.
Only one female had a genital accessory although 16% of the male respondents had them inserted while in the current prison. Genital accessories are usually small plastic balls or ball bearings, which are inserted under the skin of the penis and are commonly referred to as beading or pearling.
A higher proportion of male and female prisoners reported risk behaviors associated with tattooing, piercing and inserting genital accessories than injecting drugs or having sex.
Risk Factors for HIV
HIV status was not related to receiving a narcotic or criminal sentence for male prisoners although it was related to a history of injecting drugs. Risk factors that were statistically significant (p ≤ .05) for testing positive for HIV for male prisoners were ever used drugs, ever injected drugs, body piercing in prison, and inserting a genital accessory in prison.
Risk factors that were statistically significant for female prisoners who tested positive for HIV included a drug-related sentence, ever used drugs, ever tattooed, and a positive test for syphilis. No women aged less than 25 years tested positive for HIV. See Table 3 for information.
Male and Female Prisoners’ HIV Prevalence and Significance of HIV Infection by Risk Factor.
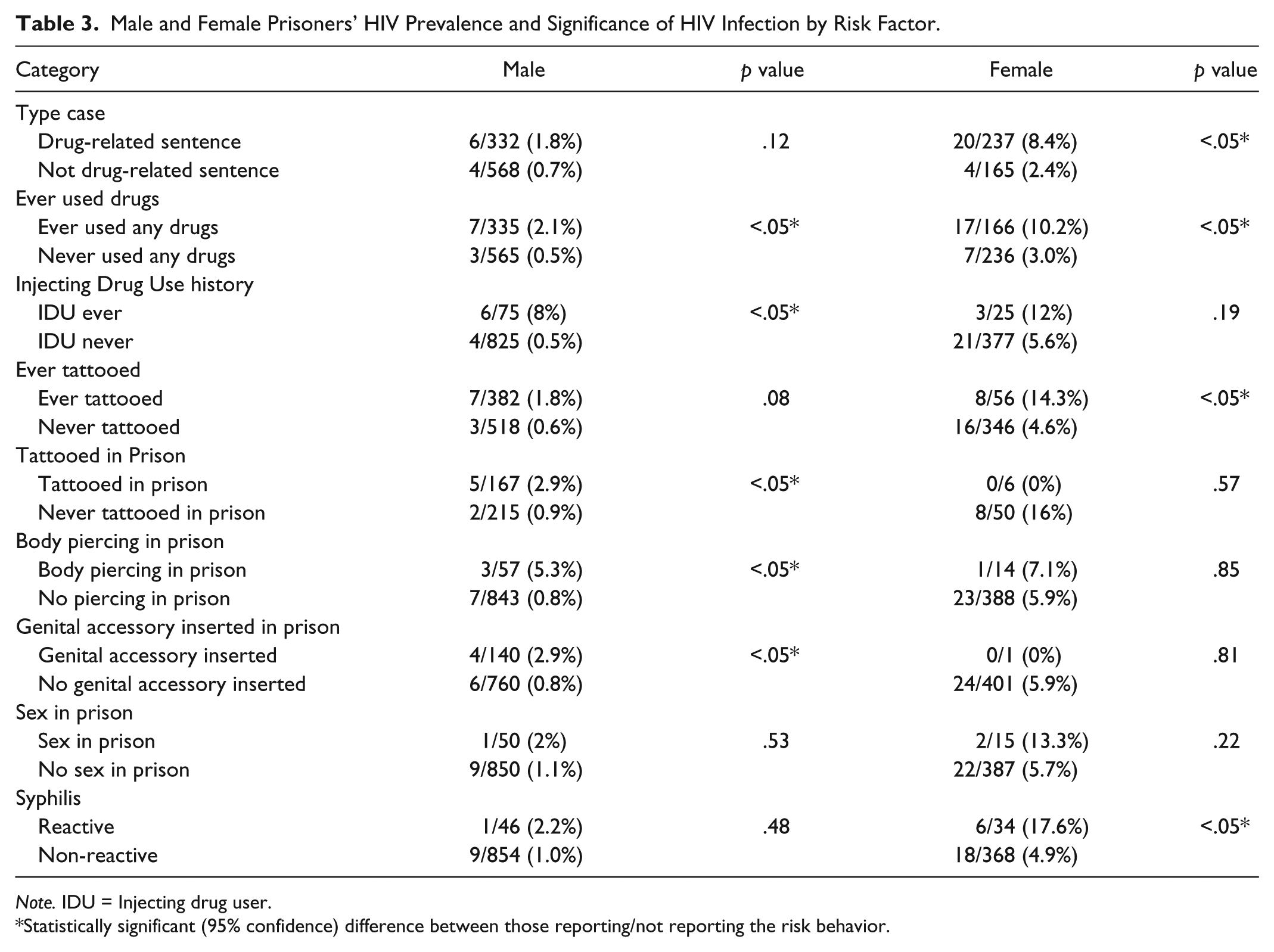
Note. IDU = Injecting drug user.
Statistically significant (95% confidence) difference between those reporting/not reporting the risk behavior.
After logistic regression of the risk factors that were statistically significant in univariate analysis for male prisoners with HIV, a history of injecting drugs has a statistically significant odds ratio with these inmates over 11 times more likely to be HIV positive than those with no history of injecting drugs (OR = 11.4, 95% CI = [2.2, 59.1], p < .00).
After logistic regression of the risk factors that were statistically significant in univariate analysis for female prisoners, those who had been sentenced for using illicit drugs were almost six times more likely to be infected with HIV than those who had not (OR = 5.8, 95% CI = [1.3, 26.8], p = .02) and those who tested positive for syphilis were over 4 times more likely to be infected with HIV than those who did not (OR = 4.2, 95% CI = [1.4, 12.3], p = .01). Female respondents aged 30 years or above were four times more likely to be infected with HIV than those aged under 30 years (OR = 4.39, 95% CI = [1.25, 15.46], p = .02). See Table 4 for information.
Odds Ratio of HIV Infection by Risk Factor for Male and Female Prisoners.
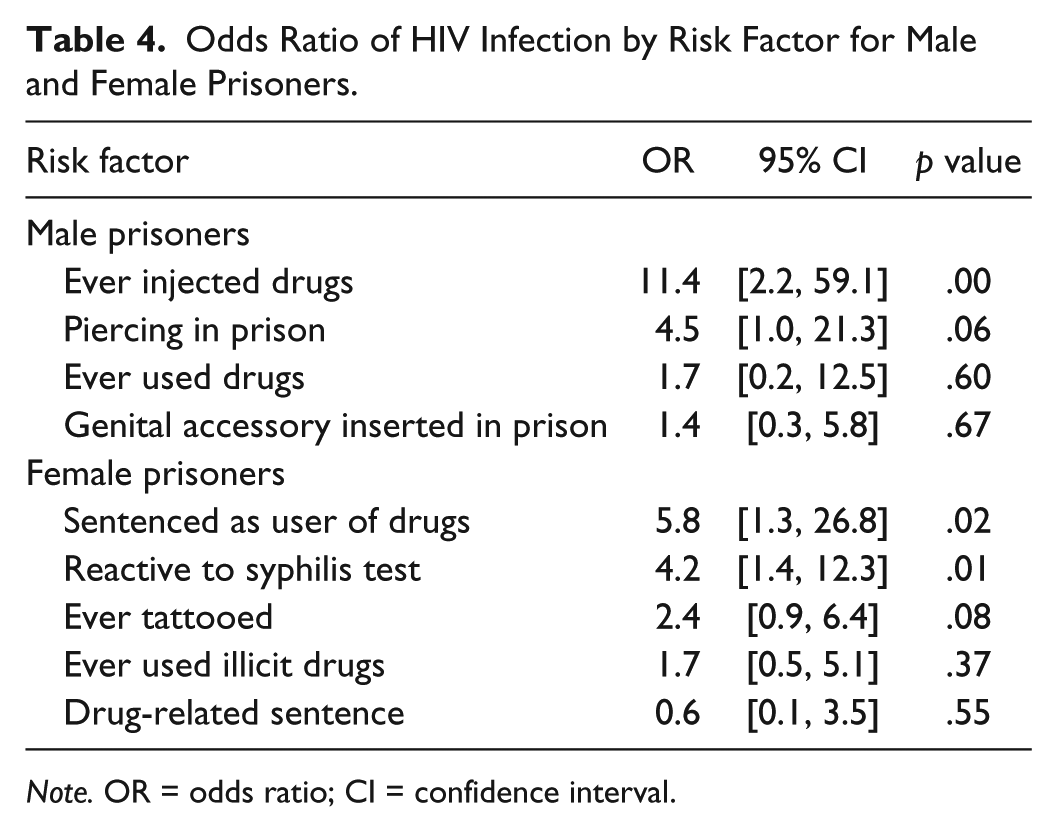
Note. OR = odds ratio; CI = confidence interval.
Key Findings
The key findings from the survey are as follows:
The main risk factor for male inmates with HIV is a history of injecting drug use. Some inmates have high-risk behaviors within prison, including injecting drugs, tattooing, piercing and inserting genital sex accessories, and sex. Given the high rate of HIV in male inmates with a history of injecting drugs, HIV and AIDS prevention and treatment policy and programs in the prison setting need to incorporate harm reduction strategies, such as the provision of methadone maintenance therapy, clean needles and syringes and bleach.
The high rate of exposure to syphilis in female inmates is associated with the high rate of HIV, suggesting sexual transmission of HIV prior to arriving in prison. Few female inmates have high-risk behavior within prison, but many will require treatment for HIV while incarcerated.
All the female inmates who tested positive for HIV were aged above 24 years which can be explained by sexual transmission of HIV given that heterosexual sex is relatively low risk compared with injecting drug use or anal sex and may also be due to the impact of safe sex programs in Indonesia, with greater use of condoms by younger women.
Few male or female inmates reported sexual activity, but those who had sex reported low condom use.
Conclusion
From this national study and other prison-based studies, it is evident that the prevalence of HIV varies between prisons based on the percentage of injecting drug users in the prison and by the HIV prevalence within injecting drug users in that geographical location, reflecting prevalence trends, as observed in other countries (Jurgens et al., 2011; Weinbaum et al., 2005).
The survey findings of a HIV prevalence of 1.1% in male prisoners is consistent with the monthly prison data reported by more than 120 prisons to the Directorate of Corrections, with HIV prevalence in male prisoners ranging from 0.8% to 1.2% per month from January to September in 2011. The random sampling process of selecting male prisons and detention centers and prisoners has provided Indonesia with a reliable national estimation of the HIV and syphilis prevalence in male inmates.
For female prisoners, the finding of a HIV prevalence of 6.0% corresponds with the high prevalence of syphilis at 8.5%. This demonstrates the additional risk of HIV from sexual transmission for female prisoners with 17.6% of those with HIV also testing positive for syphilis, whereas for HIV positive men, only 2.2% tested positive for syphilis. The monthly data reported by more than 120 prisons from January to September, 2011, reported a HIV prevalence ranging from 0.8% to 4.0% in women prisoners, and the VCT results from prisons found a HIV prevalence of 7.5% for those tested over the same time period, again ranging widely each month, from 2.8% to 15.0%. The number of female prisoners is low compared with male prisoners, giving a greater degree of variation each month. Most female prisoners are located in larger cities compared with male prisoners, and the selection of prisons for women in this study may have affected the representation of female prisoners from smaller cities to some degree. Female prisoners in prisons and detention centers in the Jakarta area were over 3 times more likely to test positive for HIV than those outside the area. The results may not be considered a national estimate for female inmates although this study does indicate that the female inmate HIV prevalence is high.
As found in a study in Brazil, the high prevalence of HIV and syphilis in female inmates provides an opportunity to prevent HIV transmission as many incarcerated women may contribute disproportionately to heterosexual and perinatal HIV and STI transmission and while incarcerated can receive treatment and counseling (Miranda et al., 2000).
This study relied on the honesty of participants about risk factors, such as injecting drugs in prison. The use of ACASI gave the prisoners as high a degree of confidentiality as was possible, with a large proportion, 80% of males and 85% of females, reporting that they had answered all the questions honestly. Those who reported not being honest about all questions may have injected drugs or had sex in prison and may have still been uncomfortable to answer these questions honestly.
Due to limited resources and logistical challenges, the low number of female inmates in many detention centers made it difficult to sample female inmates compared with male inmates in detention centers as there are many males in all detention centers, apart from the one female detention center in East Jakarta.
This study has provided baseline data for the Government of Indonesia to allow them to assess the impact of programs for HIV and AIDS prevention and treatment in the prisons and detention centers in Indonesia, as well as information for the further development of relevant policies and programs.
Harm reduction services, including condoms, bleach, and sterile injecting equipment, need to be provided to inmates to reduce the risk of HIV and syphilis transmission in closed settings, and VCT and health care for those with HIV and syphilis needs to be provided. As prisons in Indonesia, the United States, and elsewhere face financial and institutional constraints, substance abuse and harm reduction programs are often prevented from being widely implemented (Weinbaum et al., 2005). The Indonesian Ministry of Justice and Human Rights have produced guidelines for Comprehensive Services for HIV/AIDS and STIs in Correctional Institutions and are committed to addressing the challenges for inmates with limited funding. One of the good outcomes from this study is that 224 male and 258 female inmates received VCT, with prisons developing relationships with neighboring health care services if they did not have their own clinics.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Funding for the research was provided by UNODC and WHO through UNAIDS Program Acceleration Fund Mechansim, the Australian Government through the HIV Cooperation Program for Indonesia.