
Abstract
There is little evidence-based information available to guide adults in the general community on communicating effectively with adolescents about mental health problems or other sensitive topics. The Delphi methodology was used to develop guidelines to fill this evidence gap. An online questionnaire containing potential guideline statements was developed following a literature search and input from two focus groups. Two expert panels (Youth Mental Health First Aid instructors and young consumer advocates) rated the questionnaire over three rounds, according to whether or not they believed that the statements should be included in the guidelines. Results were analyzed by comparing endorsement rates between the panels. Of the 175 statements presented, 80 were rated as essential or important by ≥90% of both panels and were included in the guidelines. The Delphi process has offered an effective way to achieve consensus between expert panels on useful tips to help adults communicate with adolescents.
Although there is a range of advice available for communicating with adolescents about mental health problems, aimed at parents (Eisenberg, Sieving, Bearinger, Swain, & Resnick, 2006; Riesch, Jackson, & Chanchong, 2003; Vangelisti, 1992) and health professionals (Hardoff & Schonmann, 2001; Lerand, Ireland, & Boutelle, 2007), most of this advice is based on anecdote and individual opinion. There is little information to guide adults in the general community on these matters. In addition to mental health problems, adolescents may be struggling with other sensitive issues such as substance misuse (Bergen, Martin, Roeger, & Allison, 2005), same sex attraction (Beyondblue, 2012), bullying and abuse (Hemphill et al., 2011), body dissatisfaction (Hay, Mond, Buttner, & Darby, 2008), relationship problems, and physical development or illness. While some adults may be comfortable in communicating with adolescents on these topics, others may find it difficult. In particular, they may not feel confident in assisting a young person with a mental health problem (Kelly et al., 2011).
Adolescence and early adulthood is often the time when mental health problems first arise. Data from the 2007 Australian National Survey of Mental Health and Wellbeing (NSMHWB; Australian Bureau of Statistics, 2008) showed that 26% of young people aged 16 to 24 years met criteria for a mental illness. Yet, around three out of four of them did not access mental health services in the previous 12 months (Slade, Johnston, Oakley Browne, Andrews, & Whiteford, 2009).
When adolescents do seek help, it is more likely from informal sources such as friends and family (Rickwood, Deane et al., 2007) where a trusting relationship is already established. In contrast, formal help seeking implies conversing with a mental health professional, who is often a stranger. Some adolescents may find it difficult to trust someone they do not know and feel too shy, embarrassed, or afraid to disclose their most private experiences with them (Rickwood, 2001, 2002; Wilson, Bignell, & Clancy, 2003) or are concerned about possible breaches of confidentiality, for example, from a school counselor (Wilson & Deane 2001a, 2001b).
An unhelpful past experience with sources of help can significantly impact on future help-seeking intentions, as can beliefs such as “seeking help would not be useful,” or that “I should be able to sort out my own problems” (Rickwood, Deane, Wilson, & Ciarrochi, 2005; Rickwood, White, & Eckersley, 2007). Some adolescents do not seek help because of the stigma around mental illness and concern that they will be judged negatively by others (Hinshaw, 2005; Jorm & Wright, 2007; Walker, Coleman, Lee, Squire, & Friesen, 2008).
Adolescents with high levels of depressive symptoms (Sawyer et al., 2012) as well as those with suicidal ideation are less likely to seek help for their symptoms (Deane, Wilson, & Ciarrochi, 2001; Wilson, Deane, & Ciarrochi, 2005). Adolescent males have particularly low levels of help seeking (Rickwood et al., 2005). According to data from the 2007 NSMHWB, 22.8% of young men aged 16 to 24 met criteria for a mental disorder in the previous 12 months but only 13.2% of them accessed mental health services (Reavley, Cvetkovski, Jorm, & Lubman, 2010). This is of major concern as 27.8% of all male deaths aged 15 to 24 years in 2011 across Australia were due to suicide (Australian Bureau of Statistics, 2013).
Low emotional competence (or not having the language and skills to recognize, interpret, and share emotional experiences) is an inhibitor to help seeking. Boys and young men tend to have lower levels of emotional competence (Wilson & Deane, 2001a, 2001b) compared with girls and young women (Rickwood, 2001, 2002). Because adolescents often have low levels of mental health literacy, they lack the appropriate recognition of disorders, knowledge of help-seeking options, and effective treatments, which may lead to delays in seeking help and inappropriate help seeking (Jorm et al., 2006; Wang, 2007). Adults can play an important role in actively engaging with adolescents, rather than waiting for them to initiate help seeking (Sawyer et al., 2012) by recognizing that there is a mental health problem, providing information, encouraging professional help, and providing support (Highet, Thompson, & McNair, 2005; Jorm & Kitchener, 2011; Kelly, Kitchener, & Jorm, 2013). It is vital that adults have knowledge and skills about providing help for a mental illness and be able to communicate this to the adolescent. As there is no current benchmark to guide adults in the general community on this topic, guidelines are needed.
The aim of the current study was to develop guidelines for adults in the general community to communicate effectively with adolescents about mental health problems and other sensitive topics such as substance misuse, same sex attraction, bullying and abuse, body dissatisfaction, relationship problems, and physical development or illness. The guidelines are aimed at adults who are not necessarily the adolescent’s parent, for example, family members, teachers, sports coaches, employers, employees, chaplains, or other service personnel who have contact with adolescents.
Method
It would be unethical to undertake a randomized controlled trial to evaluate the best way for an adult to communicate with an adolescent who may be developing a mental illness, as it implies that only one group of adolescents would receive the intervention (i.e., communication tips), while the control group may receive substandard care (Miller & Brody, 2002) that could expose those adolescents to harms such as deterioration of mental health. Therefore, the accompanying guidelines were developed using a literature search and focus groups to develop questionnaire statements, and the Delphi consensus method to rate statements. The study was approved by the Mental Health Research and Ethics Committee of the Royal Melbourne Hospital (ID: 2009.658).
Literature Search
A literature search was used to find existing information on tips for adults to communicate with adolescents in general, as well as on mental health and other sensitive issues. This included journal articles, books, websites, and carers’ manuals. Searches were conducted on Google Scholar, PubMed, PsychInfo, and Academic Search Premier, using the terms “effective communication with” OR “guidelines to/for engag*,” “listening to” OR “communicat* with” OR “communicat* tips for adults” OR “talking with” OR “sensitive issues and” OR “mental health” AND “teen*/adolescent*/youth/young people/person.”
Information that was aimed purely at parents was excluded, as much of this was written in the context of a parent–adolescent relationship and could not be applied to adults in the broader community. Similarly, literature that focused on communication tips for health professionals was also excluded, as this was aimed at engagement in the “consulting room.” Any communication tips that were more appropriate for counseling or therapy were not included, as these were beyond the scope of providing initial assistance to an adolescent by adults in general. Statements that did not describe an action were excluded, as were statements aimed at specific scenarios.
Participants
Two focus groups—one of consumers, the other clinicians—were recruited from Orygen Youth Health (Orygen), a youth-specific mental health service in Melbourne, Australia. One group comprised current or past clients from Orygen who were part of a consumer advisory group. An overview of the project was presented during a meeting of the group, followed by an email invitation from the group coordinator to include those absent. Only those who considered themselves to be functioning well were encouraged to volunteer. In total, seven were recruited comprising two males and five females.
The other group, comprising clinicians and case managers from Orygen, was invited by email to participate. These clinicians were invited on the basis of having had experience of treating severely distressed adolescents and who could contribute to discussion on communication techniques that were effective in those instances. As with the literature search, any techniques used in counseling or therapy were omitted as it would be inappropriate for adults in the general community to assume the role of a clinician. In total, five clinicians were recruited, comprising a male and four females.
Each group met separately for 1.5 hr. The consumers received a small gratuity for participating. Each group was advised that an audio recording would be made during the meeting and all participants signed a consent form. The groups were facilitated by one of the authors (C.M.K.) while another author (J.A.F.) took notes. To guide focus group discussion, the following questions were posed:
Consumer group “Think about a time when you were a teenager when you were talking to an adult and you really felt that they were communicating effectively with you. Don’t think about a very distressing time, or tell us what the conversation was about. Think about what they said, how they said it and their body language. What was it that made you feel heard and understood?” In order to avoid possible distressing memories of a failed attempt at communicating with an adult (or its consequences), consumers were not asked to reflect on techniques that did not work for them.
Clinician and case manager group “Reflect upon what you find works and does not work when communicating with young people. Think about how an adult can make a young person feel comfortable, heard and understood when talking to them, e.g., body language, what the adult can say and how they should say it.”
Questionnaire Development
JAF transcribed the audio recordings from each focus group and extracted identified patterns of meaning to create potential themes (Braun & Clarke, 2006). Data around each potential theme were grouped into paragraphs. This process was replicated for text found in the literature search and combined with focus group data. Ideas within each paragraph were written as statements to create draft questionnaire items. This involved writing one idea per statement, with no ambiguity, written as an action, with minimal overlap with other items. A working party of the authors met to discuss and refine the draft items to ensure uniformity while trying to remain as faithful as possible to the original wording or source.
The questionnaire was divided into six sections: planning your approach (10 items), engaging with the adolescent (45 items), what to say and how (49 items), body language (22 items), discussing options (20 items), and handling difficulties in the conversation (8 items). Cultural items were included within these headings and were written in general terms so that they could be applied to a broad range of cultures, including that of Aboriginal and Torres Strait Islander peoples.
Expert Panelists
Two panels of experts were recruited to complete the online questionnaire: a professional panel with expertise in adolescent mental health (Youth Mental Health First Aid instructors) and a panel of youth mental health consumer advocates aged 18 to 25 years. This age range was chosen because it involved young people who were close to the adolescent age group but mature enough to reflect on what would be appropriate communication. The professional panel was recruited by emailing all accredited Youth Mental Health First Aid (MHFA) instructors currently practicing within Australia. Many hold additional roles such as teacher, registered nurse, school counselor, trainer, and CEO, or manager of a mental health or disability service. Out of 383 instructors approached, 68 agreed to participate (18%). Of these, 16 were male and 52 were female, aged between 23 and 64 years with a mean age of 43 years.
The young consumer advocates were recruited from two services from across Australia, via an email request sent from their internal networks on behalf of the authors. The first was ReachOut, which is an online community space for young people with an emphasis on mental health and well-being. ReachOut has a group of ambassadors from which six panel members were drawn; two ambassadors volunteered from each of the following states: Western Australia, New South Wales, and Queensland. The second service was beyondblue, Australia’s national depression initiative, which has a consumer advocacy group called “bluevoices.” An email was sent to 140 bluevoices members, of whom 20 agreed to participate. In total, the consumer advocates panel comprised 26 participants aged between 18 and 25 years with a mean age of 22 years, of whom 3 were male and 23 were female.
Delphi Method
The Delphi method (Jones & Hunter, 1995) provided a systematic basis to gauge expert consensus between the panel of young mental health consumer advocates and Youth MHFA instructors on items for guideline inclusion. This involved making private, independent ratings of agreement with a series of statements in a questionnaire.
The panelists’ task was to rate the statements according to how important they believed each item was for inclusion in guidelines on communicating effectively with an adolescent about mental illness or other sensitive issues. Items were rated on a 5-point scale, ranging from 1 = essential, 2 = important, 3 = do not know/depends, 4 = unimportant, 5 = should not be included. Panelists were advised that some of the items may seem contradictory or controversial, but were included because they reflected the wide range of people’s beliefs about communication.
Survey responses were analyzed by obtaining group percentages for consumer advocates and Youth MHFA instructors for each item. The following cutoff points were used:
Items rated as “Essential” or “Important” by at least 90% of both panels were accepted for inclusion in the guidelines.
Items rated as “Essential” or “Important” by at least 90% of one panel, or between 80% and 89.9% of both panels, were re-rated in the subsequent round.
All other items were rejected.
For each round of the study, panelists were sent an email with a link to an online questionnaire uploaded to SurveyMonkey (www.surveymonkey.com), which could be completed at a time that was convenient to each panel member. Those who partially completed the questionnaire could log back in at another time to finish it. Reminder emails were sent to partial and noncompleters, and they were granted another 2 weeks to complete it. Panelists were emailed a report 2 weeks after each round of the study had closed. This was to give participants enough time to read over the report and compare their personal rating (of items to be re-rated) with those of other panelists, before a link to the next round was sent.
Round 1
The questionnaire contained 154 items, divided into six sections. At the end of each section, panelists could make comments on any ambiguity or wording of the items presented and could suggest additional items. A blank field was provided for writing comments. It took approximately 45 min to complete the questionnaire. Consent was implied by responding to the survey.
Comments received from panel members in Round 1 were analyzed by JAF, who drafted new items from feedback. The working group reviewed the comments and refined the additional items. Only suggestions that represented a new idea, were considered unambiguous, and were actions were accepted as additional items. New items that were variations of items rejected in Round 1 were also not accepted. In total, 21 were accepted for Round 2 of the questionnaire.
The report fed back to each panel member at the end of Round 1 listed items that had been accepted, rejected, and required re-rating. It contained a statistical summary of individual and group ratings for items that needed re-rating. Panelists were offered the chance to maintain or change their rating in Round 2, in view of the group’s response.
Round 2
The Round 2 questionnaire contained 59 items, comprising items to be re-rated and any new items created from Round 1. It took approximately 30 min to complete. The Round 2 report listed items that had been accepted, rejected, and required re-rating. Items that fell into the re-rate category at the end of Round 2 (after already being re-rated at the end of Round 1) were excluded from the next round.
Round 3
The Round 3 questionnaire contained nine items, which were re-rates of new items generated from comments by the panelists during Round 1. It took approximately 10 min to complete. The report for Round 3 listed items that were endorsed or rejected.
Results
Table 1 shows the continuity of participation across the three rounds. There was a slightly higher percentage of males than females in the instructor expert panel (23%), compared with the consumer expert panel (12%).
The Number of Mental Health Consumers and Youth MHFA Instructors by Gender in Each Round of the Study.
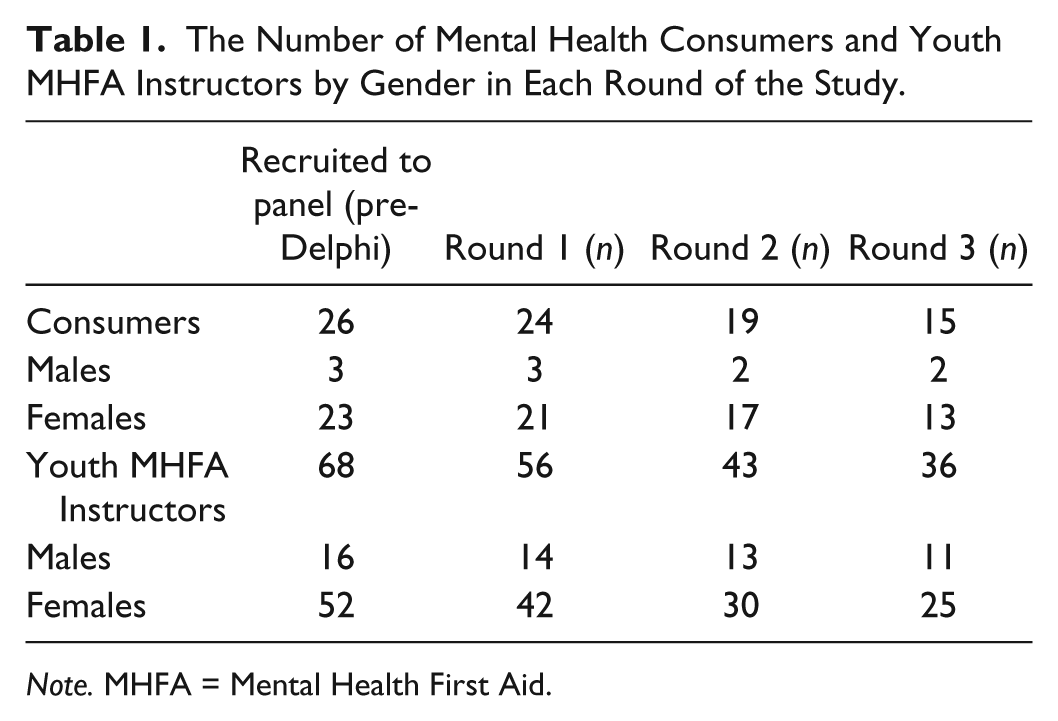
Note. MHFA = Mental Health First Aid.
Figure 1 shows the rates of inclusion, exclusion, and re-rating of the items in each round of the questionnaire. From a total of 175 items, 80 were endorsed and 95 were excluded. Endorsed items were written into prose by JAF to create the draft guidelines. These were emailed to the research-working group who refined them further, before being emailed to the expert panelists with a request for comments or minor changes. Along with the draft guidelines, panelists were sent a full list of items that had been endorsed or rejected throughout all survey rounds. The final version of the guidelines appears in Appendix A.

The number of communication questionnaire items that were included, excluded, and re-rated in three rounds of the study.
Discussion
Of the 80 items that were endorsed by both panels, there was 100% agreement between them on 10 items, depicted by an asterisk in Appendix B. Themes were around treating the adolescent with respect, using good listening skills, helping the adolescent find sources of help, and discouraging stigmatizing attitudes.
There was a high level of agreement between panels about the need for adults to be aware of differences in an adolescent’s culture regarding the way in which they use and interpret body language. Both panels also agreed that although some adolescents prefer confiding in adults of their own cultural background, it is best to ask adolescents individually if they prefer this.
Despite this consensus, there were some interesting differences between panels. Items that were not rated as “Essential” or “Important” by at least 90% of both panels were excluded from the guidelines, as per Appendix C. These items may reflect broad differences of opinion between panelists on issues regarding judgment, discretion, and the adolescent as an individual. Consumers were more likely to endorse self-disclosure by adults, including sharing their experience of a mental health problem with an adolescent. In contrast, most instructors disagreed with this idea citing professional boundaries and organizational policies.
Another difference was around asking the adolescent directly about their risk of harm. All instructor panelists believed that it is best for the adult to ask directly. However, it was not endorsed highly enough by consumers in order to be included in the guidelines. Other studies have reported that many adults and young people are reluctant to ask directly about suicide (Jorm et al., 2005; Jorm, Morgan, & Wright, 2008; Jorm & Wright, 2007), perhaps because of a concern that this might increase risk. This issue is addressed in the attached guidelines (Appendix A) by referring to Suicidal Thoughts and Behaviors: First Aid Guidelines (2008a) and Deliberate Non-Suicidal Self-Injury: First Aid Guidelines (2008b), which emphasize the importance of asking an adolescent directly if they are feeling suicidal.
Limitations
Because panelists who rated the items were all from Australia, it is not known if the guidelines are generalizable to other countries or to cultural minorities. The study may contain a female gender bias given there were so few males in all groups, that is, 20% of focus group clinicians, 29% of focus group consumers, 12% of expert panel consumers, and 23% of Youth MHFA instructors. The low response rate from currently practicing Youth MHFA instructors (18%) may mean responses are not representative of the wider instructor community. There were different sizes in group composition, for example, the consumer expert panel was around 2.5 times smaller than that of the Youth MHFA instructor panel. However, equal weighting was given to ratings by consumer panelists and instructor panelists to eliminate bias caused by unequal panel size. While a methodological weakness of the study is that focus groups were posed with slightly different questions to generate feedback, the researchers considered it important to focus on “what works” for consumers to avoid potential distress from reflecting on what has not worked for them.
Strengths
The items endorsed for inclusion in the guidelines go beyond individual opinion. By using the Delphi methodology, these guidelines have been informed by group consensus, which includes consumers who have had experience with mental illness, as well as instructors who deliver the Youth MHFA course to adults. The high level of consensus for items (90%) between these diverse groups is another strength.
A particular strength is the involvement of young consumers as experts. Future studies should encourage more consumer input in research, particularly from males, to capture viewpoints from these important groups.
The guidelines are written with enough flexibility to be applied by adults who are acquainted with the adolescent, to those who are not, and may also assist adults who do not have much contact with adolescents. They encourage the use of language that is free of stigma and assist the adult to explore the adolescent’s issues sensitively. They complement the existing suite of guidelines available from Mental Health First Aid Australia (www.mhfa.com.au) and will be incorporated in updates to the Youth MHFA manual (Kelly et al., 2013) and curriculum for future courses.
Conclusion
This process has shown that it is possible to develop communication guidelines that are acceptable to both professionals and mental health consumers. While the guidelines will be used within the context of Mental Health First Aid training, it will be important to monitor and evaluate their usefulness in the wider community. It is hoped that the guidelines will help facilitate effective communication with adolescents in general and, where required, assist conversations around mental health or other sensitive topics.
Footnotes
Appendix A
Appendix B
Items That Received ≥90% Consensus From Both Consumer and Youth MHFA Instructor Panels–Accepted in Guidelines.
| Round | |
|---|---|
| Planning your approach | |
| The adult should ask the adolescent where they feel more comfortable or safe to talk. | 1 |
| The adult should make sure that they approach the adolescent privately about their experiences at a time and place that is convenient and free of distractions. | 1 |
| The adult should be aware that the adolescent may feel more able to discuss their problems when no one else is listening. | 1 |
| The adult should be aware that the adolescent may not wish to open up until they feel that the adult cares enough, is trustworthy, and is willing to listen. | 2 |
| The adult should be aware that some adolescents (especially boys) may fear opening up about their problems in case their vulnerability is labeled as weak. | 2 |
| The adult should be aware that the adolescent may hide or play down their problem if they feel guilty about upsetting or disappointing the adult. | 2 |
| Although some adolescents prefer confiding in adults of their own cultural background, do not assume that this is always the case—ask if they would prefer this. | 3 |
| Engaging with the adolescent | |
| The adult should let the adolescent know that they are available to talk when the adolescent is ready and should not put pressure on the adolescent to talk right away. | 1 |
| The adult should set aside their own issues when communicating with the adolescent and try to focus on the adolescent’s own concerns. | 1 |
| The adult should give an adolescent their full attention. | 1 |
| The adult should be honest when interacting with the adolescent. | 1 |
| The adult should take the time to build rapport and trust with the adolescent. | 1 |
| a The adult should treat the adolescent with respect and fairness. | 1 |
| The adult should express interest in and curiosity about the adolescent. | 1 |
| a The adult should be genuine by “being themselves.” Adolescents are particularly tuned in to anyone who is “faking it.” | 1 |
| a The adult needs to recognize that each adolescent’s situation and needs are unique. | 1 |
| If the adolescent has disengaged from others, it is important for the adult to allow additional time to build trust with the adolescent. | 1 |
| The adult should be nonjudgmental when speaking with the adolescent. | 1 |
| The adult should convey a message of hope to the adolescent by assuring them that help is available and things can get better. | 1 |
| The adult should be caring and show warmth toward the adolescent. | 1 |
| The adult should be reliable and consistent in their behavior with the adolescent. | 1 |
| The adult should not make any promises to the adolescent that cannot be kept. | 1 |
| a The adult should be aware that the adolescent may hold a stigmatizing attitude toward their sensitive issue. | 2 |
| The adult should be careful not to communicate a stigmatizing attitude about the adolescent’s sensitive issue. | 1 |
| The adult should be careful in applying labels to the adolescent that the adolescent may find stigmatizing, for example, mentally ill, drug addict, and gay. | 1 |
| What to say and how | |
| a The adult should be a good listener. | 1 |
| The adult should not do all the talking. | 1 |
| As far as possible, the adult should let the adolescent set the pace and style of the interaction. | 1 |
| The adult should use a calm voice and steady tone when speaking with the adolescent. | 1 |
| The adult should stay calm when talking with the adolescent. | 1 |
| The adult should never raise their voice if they can help it. | 1 |
| The adult should ask the adolescent to explain their experience rather than make their own interpretation. | 1 |
| The adult should ask the adolescent about their experiences and how they feel about them. | 1 |
| After speaking, the adult should be patient and allow plenty of time for the adolescent to collect their thoughts, reflect on their feelings, and decide what to say next. | 1 |
| The adult should actively listen and use questions to check their understanding and acknowledge that they have heard what the adolescent has said. | 1 |
| The adult should talk “with,” not “at,” the adolescent. | 1 |
| The adult should avoid trivializing the adolescent’s feelings by using statements such as, “When you’re older . . .” or “Back in my day . . .” as this may appear dismissive of the adolescent’s perspective of their own experience. | 1 |
| The adult should not use scare tactics or threats when talking to the adolescent, for example, “If you keep thinking like this, you’ll end up in big trouble.” | 1 |
| The adult should avoid telling the adolescent to “snap out of it” or “stop thinking that way.” | 1 |
| If the adolescent is in a potentially harmful situation (e.g., experiencing abuse or bullying), the adult should reassure the adolescent that they want to keep them safe. | 1 |
| The adult should explain the limits of confidentiality, for example, anything that affects the safety of the adolescent or others (such as abuse or suicidal thoughts or behavior) may need to be discussed with someone who can act to keep them safe. | 1 |
| If the adult is having a private discussion with the adolescent and other people arrive, the adult should take a moment to ask the adolescent in private what they would like to do (e.g., continue the discussion in front of others, ask others to leave, or schedule another time to continue your discussion). | 1 |
| The adult should tell the adolescent that they want to help. | 2 |
| The adult should listen to the adolescent without interrupting them. | 2 |
| The adult should make a conscious effort to listen, to hear the feelings and meaning behind the adolescent’s words, and respond to this. For example, when the adolescent says, “Can’t use the car? Others are allowed!” It could mean, “I feel like you don’t trust me. I want you to treat me as a responsible person.” | 2 |
| The adult should reassure the adolescent that they are not required to talk about or reveal anything until they are ready to do so. | 2 |
| a The adult should tell the adolescent that when they want to talk, the adult will listen to them. | 2 |
| a The adult should allow the adolescent to talk about their experiences and beliefs if they want to. | 2 |
| If the adolescent appears distressed by what they are experiencing, the adult should reassure the adolescent that help is available. | 1 |
| The adult should avoid sounding condescending or patronizing. | 1 |
| The adult should avoid stereotyping adolescents, for example, “ . . . adolescents always like to be difficult and oppose adults.” | 1 |
| a If the adult finds that they have said something in error to the adolescent, they should be up front and address the error as soon as they can. | 1 |
| Although the adult should encourage the adolescent to lead the conversation, the adult should not be afraid to ask open, honest questions during the course of discussion. | 3 |
| Body language | |
| The adult should be aware of the adolescent’s body language as this can provide clues to how they are feeling or how comfortable they feel talking with the adult. | 1 |
| The adult should avoid negative body language such as crossing their arms, hands on hips, or looking uninterested. | 1 |
| The adult should avoid distracting gestures such as fidgeting with a pen, glancing at other things, or tapping their feet or fingers, as these could be interpreted as lack of interest. | 1 |
| The adult should be aware of their own body language and what this conveys when communicating with the adolescent (e.g., posture, facial expressions, and gestures). | 1 |
| The adult should use cues like nodding to keep a conversation going with the adolescent. | 1 |
| The adult should not only think about what they are saying but also how they are saying it (e.g., tone, volume of voice, and body language). | 1 |
| The adult should notice how much personal space the adolescent feels comfortable with and not intrude beyond that. | 1 |
| The adult should be careful not to disagree or minimize the adolescent’s thoughts and feelings. “ . . . you’re not depressed. You’re just bored.” | 1 |
| The adult should be aware that different cultures use and interpret body language in different ways. | 1 |
| Discussing options | |
| The adult needs to listen attentively and sensitively to the adolescent’s issue in full, before they suggest possible courses of action so as to avoid offering ill-considered or inappropriate advice based on only “‘half the picture.” | 1 |
| The adult should ensure that the adolescent has had a chance to fully express and explore their issue, before offering possible courses of action, so as not to appear to be minimizing or dismissing the problem. | 1 |
| The adult should try not to judge a situation on what they would do themselves but have a discussion with the adolescent about what could be done. | 1 |
| The adult should discuss with and help the adolescent to assess different courses of action and to understand the consequences of each. | 1 |
| If the adolescent resists seeing someone about their problem, offer phone numbers to Lifeline or Kids Help Line or websites, as these are anonymous and may be less confronting. | 1 |
| The adult should recommend that the adolescent talk to the relevant professional (e.g., teacher, doctor, or counselor) as early as possible, to talk about what they have been experiencing. | 1 |
| Handling difficulties | |
| The adult should be aware that some adolescents do not communicate well verbally, and it is important to adapt to their needs and abilities. | 1 |
| If the adolescent does not want to talk about their problems, the adult should not take it personally. | 1 |
| If the adolescent makes negative comments, the adult should not take these personally. | 1 |
| If the adolescent is being antagonistic or argumentative, the adult should not respond in a hostile, disciplinary, or challenging manner. | 1 |
| If the adult is left feeling bewildered or distressed following a discussion with the adolescent, they should confide their feelings to a trusted friend or health professional while maintaining the adolescent’s privacy. | 1 |
| If the adolescent does not feel comfortable talking to the adult, they should encourage the adolescent to discuss how they are feeling with someone else. | 2 |
| a If the adolescent asks the adult for help and the adult does not know much about the problem, the adult should still try to support the adolescent and assist them to get other help. | 2 |
| a If the adolescent does not feel comfortable talking to the adult, the adult should help the adolescent find a suitable person to talk to. | 3 |
| The adult should not presume that the adolescent does not want their help even if the adolescent has an initial negative reaction to them. | 1 |
| The adult should be aware of any barriers to the adolescent’s communication, for example, language difficulties, finding the right words, or an inability to express emotion. | 1 |
| The adult should try to be aware of when they are not being listened to and change the way they are saying or doing things. | 2 |
| a The adult should be aware that sometimes adolescents struggle to ask for assistance, or reject help when offered, even if they feel that a situation is out of control. | 1 |

Depicts items for which there was 100% agreement between panels.
Appendix C
Items Excluded From the Communication Guidelines.
| Round | |
|---|---|
| Planning your approach | |
| The adult should be aware that the adolescent is more likely to engage with them in a place that is within the adolescent’s comfort zone (e.g., in a café or at home). | 2 |
| When approaching the adolescent, it may be helpful for adults to be aware of the adolescent’s cultural background, local cultural norms, and hierarchy within their culture. | 3 |
| The adult should be aware that the adolescent may find it easier to talk during a time-limited activity that has a definite end point. | 1 |
| The adult should be aware that it may be easier for the adolescent to talk during activities that do not require a lot of eye contact. | 1 |
| The adult should be aware that the adolescent may feel more comfortable talking to people of similar age about their problems or experiences. | 1 |
| The adult should be aware that adolescents from diverse backgrounds may be more comfortable talking to an adult from their own culture. | 1 |
| The adult should be aware that the adolescent may feel more at ease about opening up to others who also have the same sensitive issue. | 1 |
| The adult should use a mutual activity as an opportunity to talk with the adolescent about a sensitive issue, for example, going shopping, going for a drive, or going for a walk. | 1 |
| Engaging with the adolescent | |
| The adult should use a friendly attitude when speaking with the adolescent (rather than treat the adolescent as they would an adult friend or peer). | 2 |
| The adult should treat the adolescent as responsible and capable of making decisions. | 2 |
| The adult should talk openly with the adolescent about the sensitive issue. | 2 |
| The adult should talk openly with the adolescent about the sensitive issue, taking into consideration the adolescent’s age. | 2 |
| The adult should talk openly with the adolescent about the sensitive issue, taking into consideration the adolescent’s maturity. | 3 |
| As a basis for discussion, it is sometimes useful for the adult to talk about how the adolescent’s sensitive issue is portrayed in the media (e.g., Does the media glamorize or spread myths about the particular issue?) | 2 |
| a The adult should not avoid speaking with or offering help to the adolescent out of fear that the adult may say or do the wrong thing. | 2 |
| a The adult should not use slang with which they are unfamiliar, as the adolescent will recognize that the adult is not being genuine. | 2 |
| a The adult should try to empathize with how the adolescent feels about their beliefs and experiences. | 2 |
| a The adult should offer the adolescent consistent emotional support and understanding. | 2 |
| a The adult should acknowledge the adolescent’s expertise about their own life. | 2 |
| a The adult should praise the adolescent when they’ve acted in a responsible way. | 2 |
| a The adult should be mindful of their own gender and that of the adolescent, and how this may relate to the adolescent’s current experience or previous trauma (e.g., an adolescent female who confides in a male adult about sexual abuse). | 2 |
| a The adult should ask the adolescent about the impact of their culture or background, rather than assume what this might be. | 2 |
| a The adult should be aware that the adolescent may hold a stigmatizing attitude toward their sensitive issue. | 2 |
| a The adult should talk openly with the adolescent about the sensitive issue. | 2 |
| a The adult should show a confident manner when interacting with the adolescent. | 3 |
| The adult should not compare the adolescent’s life to their own experiences at that age. | 1 |
| The adult should offer their first name to create a less formal atmosphere—using titles such as doctor or mister creates a hierarchy, which the adolescent may perceive as wanting power over them. | 1 |
| The adult should take the time to engage with the adolescent first (e.g., getting them to talk about their interests and social life) before discussing personal issues about any problems that the adolescent may be experiencing. | 1 |
| If the adult does not know about things the adolescent is interested in, they should ask and find out from them. | 1 |
| The adult should be aware that a laid-back or less formal dress sense helps to engage adolescents. | 1 |
| If the adolescent cannot or does not want to talk about what they are experiencing, the adult should respect this and not pry. | 1 |
| The adult should talk to the adolescent as they would to a friend. | 1 |
| The adult should lift the adolescent’s spirits and help them feel more positive about themselves. | 1 |
| The adult should avoid confronting the young person and should not criticize or blame them. | 1 |
| The adult should express positive attitudes about the adolescent’s culture. | 1 |
| The adult should familiarize himself or herself with technologies adolescents use as this may be a way of engaging adolescents more personally and in a way they understand, for example, with social networking tools such as Facebook, Twitter, and YouTube. | 1 |
| The adult should avoid using ideas about the sensitive issue from television, movies, and the media when speaking with the adolescent, as these are often both frightening and inaccurate. | 1 |
| What to say and how | |
| If the adult often uses long silent pauses, they should explain that they are just thinking about the adolescent’s options and talk to them through this, as the adolescent may otherwise misinterpret this negatively. | 2 |
| The adult should offer positive feedback to the adolescent as this may encourage them to communicate with the adult, for example, “I think it’s great that you are willing to talk to me about this—it shows a great deal of maturity.” | 2 |
| If the adult has personal experiences of the sensitive issue, they should gauge whether or not it may be helpful to share these with the adolescent on an individual basis. | 2 |
| If the adult chooses to share their own personal experience of a similar sensitive issue as the adolescent, they should ask the adolescent whether they want to hear it before going ahead. | 2 |
| a When sharing a personal experience of the same sensitive issue (e.g., depression), and there have been difficulties in the adult’s recovery, the adult should be careful not to convey a bleak attitude toward recovery to the adolescent. | 3 |
| a The adult should use open-ended questions in order to get the adolescent’s input into a conversation. Open-ended questions are questions that cannot be answered with a simple “yes” or “no,” for example, “How are you feeling about what happened?” instead of “Are you feeling OK about what happened?” | 2 |
| a The adult should take as much time as the adolescent needs to talk. | 2 |
| a If the adult has commenced talking with the adolescent about their issues but finds that they are running out of time, the adult should reschedule another time to talk with the adolescent. | 2 |
| a If the adult is from a different cultural background to the adolescent, they may need to make some adjustments to their usual style of communication, for example, the adolescent may be used to using physical terms (such as headache or stomach ache) to describe their emotional experiences, be used to a different level of eye contact or personal space, or it may not be appropriate in the adolescent’s culture to speak alone with an adult of the opposite sex. | 2 |
| a The adult should offer alternative actions that could help with the problem and allow for compromise to give the adolescent a sense of control. | 2 |
| a If a parent or guardian is present during a discussion with the adolescent, the adult should ensure that both the adolescent and the parent/guardian have a chance to talk and ask questions. | 2 |
| a If the adult is concerned about the adolescent’s safety or risk of harm, they should ask them directly about this. | 3 |
| If the adult has approached the adolescent, they should be straightforward and explain their concerns. | 1 |
| The adult should listen more than they talk to the adolescent. | 1 |
| The adult should not overuse the adolescent’s first name, as this may appear patronizing or over-familiar. | 1 |
| The adult should use “I messages” to communicate their thoughts and feelings to the adolescent. “I messages” are statements that tell the adolescent how the adult feels about their behavior and gives the adolescent an understanding of the effects of their behavior without blaming the adolescent, for example, “I feel very upset when you . . .” | 1 |
| The adult should use metaphor where appropriate. | 1 |
| The adult should use humor where appropriate. | 1 |
| The adult should not ask the adolescent to justify or explain their behavior as asking “why” can put the adolescent on the defensive. | 1 |
| The adult should pay attention to any topic the adolescent is finding distressing and avoid asking more about it. | 1 |
| The adult should avoid steering the conversation toward the answer they think will “solve” the adolescent’s problems. | 1 |
| The adult should avoid telling the adolescent what they should do to solve their problems. | 1 |
| If a parent or guardian is present during a discussion with the adolescent and the adult needs to ask the parent or guardian a question, they should then turn to the adolescent and ask the same question. | 1 |
| The adult should state that the topic may be sensitive, for example, “I want to talk to you about something, and it might be a sensitive topic . . .” | 1 |
| If the adult has personal experiences of the sensitive issue, they SHOULD share these with the adolescent, to normalize the experience for them. | 1 |
| If the adult has personal experiences of the sensitive issue, they should NOT share these with the adolescent. | 1 |
| The adult should ENCOURAGE the adolescent to talk to them about their experiences and beliefs. | 1 |
| Body language | |
| The adult should not make any comments about the adolescent’s body language, for example, avoiding eye contact or fidgeting. | 2 |
| If the adult feels startled or disturbed by what the adolescent says, the adult should remain neutral (e.g., phrasing, vocal tone, and body language). | 2 |
| a If the adolescent appears defensive, the adult should make their body language as open as possible by appearing relaxed, keeping their palms out, sitting alongside the adolescent but angled toward them and keeping their voice calm and low. | 2 |
| a The adult should maintain a comfortable level of eye contact when speaking with the adolescent. | 2 |
| a The adult and the adolescent should be positioned at the same level so that they do not have to look up or down at each other. | 2 |
| a The adult should be respectful of personal boundaries between themselves and the adolescent, but not to the point of being afraid to show comfort, if the adolescent asks for it (e.g., a brief hug or pat on the shoulder). | 3 |
| If the adolescent is relaxed and open, the adult should match their body language. | 1 |
| The adult should sit in a relaxed position. | 1 |
| The adult should sit face-to-face with the adolescent. | 1 |
| The adult should sit side by side with the adolescent. | 1 |
| When seated, the adult should lean forward to show interest when speaking with the adolescent. | 1 |
| When talking with the adolescent, the adult should not sit behind a desk. | 1 |
| The adult should maintain an appropriate distance with the adolescent in order to model clear personal boundaries. | 1 |
| If the adolescent is distressed, the adult should convey a sense of comfort by offering a brief hug or simple touch. | 1 |
| The adult should know the difference between “good” touching and “bad” touching when comforting the adolescent. Safe touching is extremely healthy, and it is important for adolescents to have models of this. | 1 |
| Discussing options | |
| a The adult should help the adolescent find solutions without trying to fix the problem for them. | 2 |
| The adult should ask permission to give opinions or offer advice so that it is not seen as criticism or taken defensively. | 1 |
| Handling difficulties in the conversation | |
| If the adolescent feels more comfortable talking to people with similar experiences or people their own age, the adult should recommend that the adolescent joins a support group. | 2 |
| If the adolescent asks the adult for help and the adult does not know much about the problem, the adult should learn more about that type of problem. | 2 |
| a If the adolescent is infringing the adult’s personal space, the adult should talk to them directly about it. | 2 |
| a If the adolescent is expressing excessive anger or behaving aggressively, the adult should clearly state that they cannot communicate with the adolescent if they are shouting or acting in a threatening way. | 2 |
| a If the adolescent is expressing anger, the adult should offer empathy and try to find out why they are feeling angry. | 2 |
| If the adolescent appears distressed by what they are experiencing, the adult should normalize it by saying it is common for adolescents to feel this way. | 1 |
| If the adolescent is finding it difficult to express their emotions, the adult should offer a few terms to pick from to help them find the language they are looking for. For example, “To me, you don't look very happy. Are you feeling sad, or angry, or frustrated?” | 1 |
| If the adolescent is distressed, the adult should convey a sense of comfort by using a few appropriate words, e.g. “It’s OK. I’m here.” | 1 |
| If the adult feels uncomfortable during their discussion with the adolescent, they should admit it. | 1 |
| If the adult feels uncomfortable during their discussion with the adolescent, they should ask the adolescent if they are uncomfortable also. | 1 |
| If the adult is having trouble interpreting the adolescent’s behavior, they should ask them directly to explain what they are doing. | 1 |
| If the adult is having trouble engaging or communicating with the adolescent, they should ask whether they would like some help to find someone else to talk to, for example, a person of a different age or gender. | 1 |
| If the adult feels uncomfortable with what the adolescent is saying, they should suggest that the adolescent find someone else to speak to and ask if they would like any assistance with this. | 1 |
| If the adolescent appears agitated, the adult should offer to take them outside for a walk while talking with them. | 1 |

Depicts items excluded on basis of falling into the “re-rate” category after two Rounds.
Acknowledgements
The authors gratefully acknowledge the time and effort of the panel members, without whom this project would not have been possible. They also thank Ms. Anna Ross for assistance in questionnaire development.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Funding was provided by the Australian National Health and Medical Research Council.
Author Biographies
![]() ) which aims to improve the mental health outcomes for teenagers.
) which aims to improve the mental health outcomes for teenagers.
![]() as one of the most cited researchers in Psychology/Psychiatry of the past 20 years.
as one of the most cited researchers in Psychology/Psychiatry of the past 20 years.