
Abstract
The objective of this study is to determine prevalence, risk factors, and prognostic impact of malnutrition. Nutritional state was assessed by Subjective Global Assessment (SGA) and body mass index (BMI). Risk factors for malnutrition and effect of malnutrition on morbidity, mortality, and length of hospital stay were analyzed. Prevalence of malnutrition on admission and on discharge was 73%. Risk factors significantly associated with malnutrition were severity of primary diagnosis (odds ratio [OR] = 3.42, 95% confidence interval [CI] = [2.26, 5.18], p < .0001), age (p < .001), and presence of comorbidities (OR = 1.67, 95% CI = [1.13, 2.46], p < .013). Malnourished patients had longer hospital stay (5.1 ± 4.9 days, p < .0001) and higher risk of dying (OR = 6.38, 95% CI = [1.14, 135.80], p < .030), and were more likely to be confined for more than 7 days (OR = 4.20, 95% CI = [1.89, 9.34], p < .001). The study concludes that malnutrition is prevalent on admission and discharge. Malnourished patients are older, suffer more serious disease, and have comorbidities. Complications risk is higher if malnourished.
Almost four decades have passed since hospital malnutrition was initially noted by Butterworth (1974). However, hospital malnutrition still remains to be a common, largely unrecognized and undertreated problem. Malnutrition is frequently ignored as it is considered a complication of the disease process, with little bearing on the prognosis and little possibility for therapeutic intervention.
Notwithstanding the latest advances in modern medicine, the local and worldwide prevalence of hospital-related malnutrition is high at 40% to 50% (Baccaro et al., 2007; Correia, Caiaffa, da Silva, & Waitzberg, 2001; Correia & Campos, 2003; Davis et al., 2004; Gupta et al., 2005; Kyle et al., 2005; Martineau, Bauer, Isenring, & Cohen, 2005; Planas et al., 2004; “Prevalence of malnutrition in the Philippines, n.d.”; Vila et al., 2010; Waitzberg, Caiaffa, & Correia, 2001). As to nutrition status, data show that more patients are well-nourished (Pablo, Izaga, & Alday, 2003; Sacks et al., 2000) and moderately malnourished (Baccaro et al., 2007; Ockenga et al., 2005; Pablo et al., 2003; Raslan et al., 2011; Sacks et al., 2000; Waitzberg et al., 2001). However, among patients with comorbidities, the prevalence of severe malnutrition rises to 45% (del Rosario, Inciong, Sinamban, & Llido, 2008; Fiaccadori et al., 1999; Ocampo, Camarse, Kadatuan, & Torillo, 2008).
Malnutrition has a profound impact on prognosis. The more severe the level of malnutrition, the risk of developing complications is greater (Beghetto, Luft, Mello, & Polanczyk, 2009; Fiaccadori et al., 1999; Middleton, Nazarenko, Nivison-Smith, & Smerdely, 2001; Ocampo et al., 2008; Ozkalkanli, Ozkalkanli, Katircioglu, & Savaci, 2009; Raslan et al., 2011), likelihood of mortality is higher (Fiaccadori et al., 1999, Gupta et al., 2005; Kyle et al., 2005; Middleton et al., 2001; Ocampo et al., 2008; Ozkalkanli et al., 2009; Sacks et al., 2000; Segall et al., 2009; Sungurtekin, Sungurtekin, Oner, & Okke, 2009), stay in the hospital is longer (Beghetto et al., 2009; Fiaccadori et al., 1999; Kyle et al., 2005; Ozkalkanli et al., 2009; Raslan et al., 2011), and rate of readmission within 30 days is increased (Ocampo et al., 2008). Severe malnutrition when identified early and managed accordingly would lead to a better outcome for the patient’s overall disease management (Alberda, 2009; del Rosario et al., 2008; Woodcock et al., 2001).
In the Philippines, data on prevalence and impact of hospital malnutrition are grossly lacking. It is therefore the intent of this study to answer the following questions: (a) What is the nutritional status of medical patients on admission and does it deteriorate over the course of their hospitalization? (b) What are the risk factors associated with malnutrition? and (c) Does malnutrition adversely affect the course of illness?
Method
Participants
This was a cross-sectional analytical study conducted from September 1, 2012, to November 30, 2012, on all patients aged 18 years old and above who were admitted to the Department of Medicine of St. Louis University Hospital of the Sacred Heart. This tertiary care hospital is a training institution located at Baguio City, Philippines. Each patient and/or relatives received a detailed oral explanation as to the nature and purpose of the study. Written informed consent was obtained from patients or their next of kin in case a patient could not communicate. The sample size was determined using Open Epi Version 2.3.1. At 95% confidence interval (CI), the minimum number of participants required was 384. The study was approved by the Research and Ethics Committee of the Institution.
Materials and Procedure
The nutrition status of patients was assessed on admission and discharge using Nutrition Risk Screening (NRS) 2002 questionnaire, Subjective Global Assessment (SGA) questionnaire, and body mass index (BMI). NRS 2002 screens patients for malnutrition based on four questions. Patients categorized as “nutritionally at risk” by NRS 2002 underwent formal nutritional assessment using the SGA questionnaire. SGA determines nutritional status on the basis of a clinical evaluation of patient history and a physical examination. The patient history is a structured questionnaire that details weight changes, dietary intake, gastrointestinal symptoms, functional capacity, and disease. The physical examination assesses subcutaneous fat, muscle wasting, edema, and ascites. The BMI was determined using weight and height. Two trained clinical examiners administered the questionnaires and did the required physical examination. Nutritional status was then rated as normal (no nutritional risk on NRS or SGA A and BMI of 18.5-25 kg/m2), moderate malnutrition (SGA A and BMI < 18.5 or > 30 kg/m2 or SGA B and BMI of 18.5-30 kg/m2) or severe malnutrition (SGA C regardless of BMI or SGA B and BMI of <18.5 or >30 kg/m2). Risk factors for malnutrition considered in this study were age, gender, admitting diagnosis (severe or benign), and presence or absence of comorbidities. Diseases that were considered “severe” in this study were malignancy, chronic kidney disease, congestive heart failure, cerebrovascular disease, chronic obstructive pulmonary disease, acute coronary syndrome, sepsis, and other conditions that required intensive management. All complications requiring therapeutic intervention, days of hospital confinement, as well as final outcome (death or discharge) were recorded. Outcomes evaluated were in-hospital mortality, in-hospital morbidity (infection, readmission, deterioration, cardiopulmonary arrest), and length of hospital stay.
Data were encoded using Microsoft Excel Starter 2010 and were statistically analyzed using Epi Info™ Version 7.1.0.6. Frequencies, ranges, and/or means (and standard deviations) were summarized to describe demographic characteristics and clinical profile of subjects. Frequencies were used to ascertain prevalence of malnutrition as well as nutrition status. To determine associations of malnutrition on risk factors and clinical outcomes, f-test for continuous variables, and either chi-square analysis or mid-P exact for categorical variables were used where applicable. Odds ratios (ORs) were then calculated using Open Epi™ to determine the strength of associations reported at 95% CI. A p value of <.05 was considered significant.
Results
In this study, 607 patients were included. The youngest participant was 18 years old and the oldest was 95 years old. Almost half of the patients were between 31 and 59 years old. The most common reason for admission was oncologic in nature. Almost 40% of the participants had comorbid conditions, predominantly cardiac in origin. The average length of stay was 3.9 ± 3.6 days (Table 1).
Demographic and Clinical Profile of the Study Population (N = 607).

Results are presented in n (%), mean, or range.
Of these, 96% (586 of 607) had a complete admission and discharge nutritional assessment. Twenty-one patients who were not reevaluated on discharge were assumed to be malnourished as they had some degree of malnutrition on admission. The prevalence of malnutrition on admission was 73%. The mean age for the severely malnourished group was 54.7 ± 20.6 years. More patients with severe disease and comorbidities had severe malnutrition. The mean duration of confinement for patients with severe malnutrition was 5.1 ± 4.9 days. Conversely, more severely malnourished patients died, developed complications, and stayed for more than 7 days in the hospital. (Table 2).
Patient Characteristics as to Nutritional Status (N = 607).

Note. Results are presented in n (%), M ± SD, or range.
The prevalence of malnutrition on discharge did not change, with more than half being moderately malnourished. There was no change in nutritional status from admission to discharge in 92% of the patients. The nutritional status declined in 2% of the subjects on discharge. Of patients admitted nutritionally compromised, 3% improved nutritionally while hospitalized (Table 3).
Nutritional Assessment on Admission and Discharge.

No data gathered on discharge because of any of the following reasons: Patients either died, transferred to hospital of choice, or went home against medical advice prior to reassessment.
Significantly more patients in the older age group were severely malnourished (p < .001). When kind of disease was considered, significantly more patients with malignancy or a more severe form of illness on admission were malnourished (OR = 3.42, 95% CI = [2.26, 5.18], p < .0001). The presence of comorbid disease is a risk factor for malnutrition (OR = 1.67, 95% CI = [1.13, 2.46], p < .013). Gender did not show significant association with nutritional status. Among the risk factors considered in this study, severity of disease seems to be the strongest risk factor associated with malnutrition (Table 4).
Risk Factors for Malnutrition on Admission.

Note. OR = crude odds ratio; CI = confidence interval (lower limit, upper limit). Statistically significant p values reported at p < .05 (two-tailed).
f-test.
Chi-square.
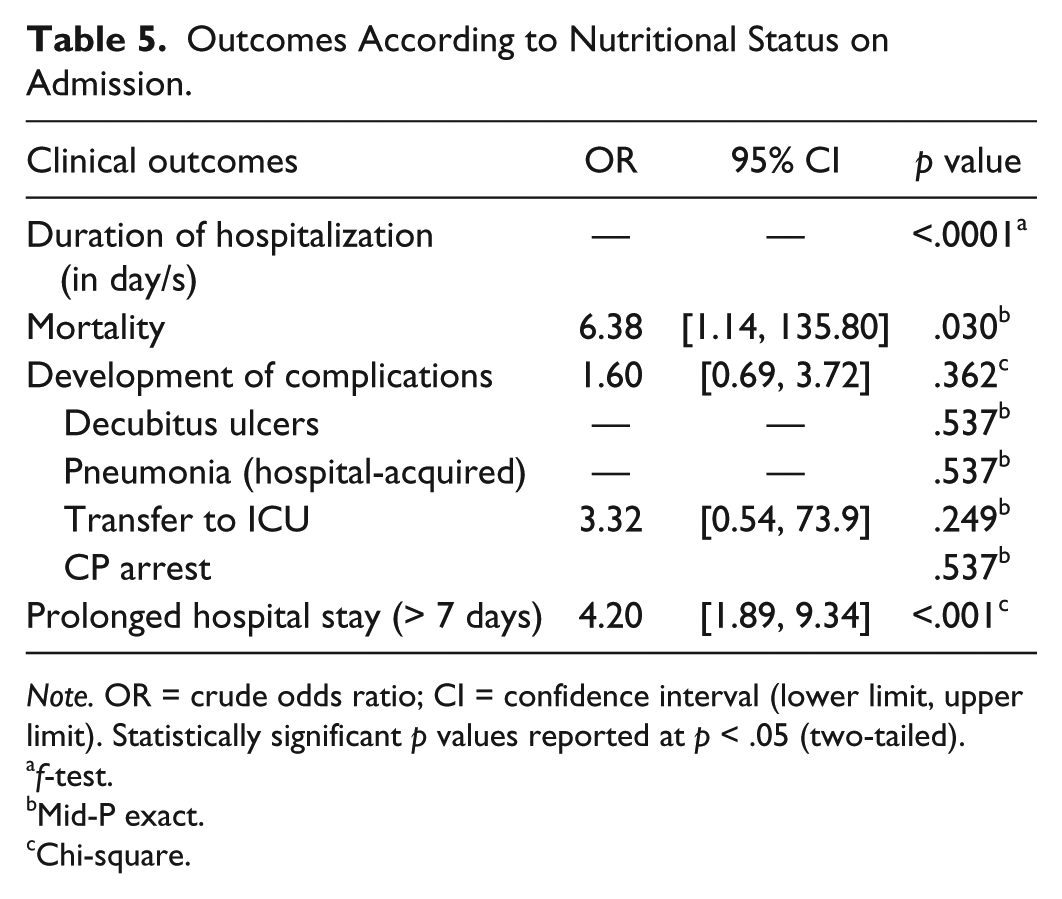
Severely malnourished patients significantly stayed longer in the hospital compared with those with normal and moderate nutrition status (p < .0001). There was a higher risk of dying in those who were severely malnourished (OR = 6.38, 95% CI = [1.14, 135.80], p < .03). Although the malnutrition rate was high, only 37 patients developed complications during their hospital confinement. The risk of developing complications in general was increased among malnourished patients, although the association was not statistically significant (OR = 1.60, 95% CI = [0.69, 3.72], p < .362). A tendency toward prolonged hospitalization for at least 1 week was observed among malnourished patients, regardless of primary admitting diagnosis (disease), and comorbidities (OR = 4.20, 95% CI = [1.89, 9.34], p < .001; Table 5).
Outcomes According to Nutritional Status on Admission.
Note. OR = crude odds ratio; CI = confidence interval (lower limit, upper limit). Statistically significant p values reported at p < .05 (two-tailed).
f-test.
Mid-P exact.
Chi-square.
Discussion
In this study, the malnutrition rate was alarmingly high, surpassing existing data from previous studies (Baccaro et al., 2007; Correia et al., 2001; Correia & Campos, 2003; Davis et al., 2004; Gupta et al., 2005; Kyle et al., 2005; Martineau et al., 2005; Planas et al., 2004; “Prevalence of malnutrition in the Philippines, n.d.”; Vila et al., 2010; Waitzberg et al., 2001). Malnutrition was especially prevalent among the older age group, those with severe disease and comorbidities. These findings are similar to the results of other studies showing that age, severity of disease, and presence of comorbidities are risk factors for malnutrition (American Society for Parenteral and Enteral Nutrition [A.S.P.E.N.] & Board of Directors and Standards Committee, 2005; Baccaro et al., 2007; Banks, Ash, Bauer, & Gaskill, 2007; Burgos et al., 2012; Correia & Campos, 2003; Correia et al., 2001; Pirlich et al., 2003; Pirlich et al., 2006; Vila et al., 2010; Waitzberg et al., 2001). This could be due to disease-related metabolic changes (Muscaritoli et al., 2010), markedly inadequate nutritional intake during hospitalization (Incalzi et al., 1996; Sullivan, Sun, & Walls, 1999), excess loss, and patient dissatisfaction with the food served (Incalzi, et al., 1996). In addition, older people have poor dentition, poor appetite, cognitive impairment, and multiple comorbidities that make them more vulnerable to malnutrition (Kayser-Jones, Schell, Porter, Barbaccia, & Shaw, 1999). Nutritional requirements are increased in the presence of disease. However, malnutrition does not only refer to undernutrition but to overnutrition as well. A considerable number of those with malnutrition in this study were classified as such primarily because their BMI was above normal. This could have exaggerated the malnutrition rate. There is limited data as to the prevalence and impact of overnutrition in the hospital setting.
The findings from this study show that the nutritional status of those with malnutrition did not improve during the course of their confinement. Studies show that a significant proportion of hospital patients do show evidence of undernutrition on admission to hospital and continue to deteriorate nutritionally during their hospital stay (Agradi, 1984; Braunschweig, Gomez, & Sheean, 2000; McWhirter & Pennington, 1994; Naber et al., 1997). Aside from the reasons for malnutrition mentioned earlier, medical unawareness might contribute to the worsening of nutrition status of hospitalized patients (Roubenoff, Roubenoff, Preto, & Balke, 1987). It seems that nutrition is not part of the patients’ routine care. In addition, the practice of nutritional therapy in the Philippines is still in its infancy stage. Inadequate detection and intervention can lead to the worsening of nutritional status during hospitalization (Kyle et al., 2005). However, the short hospital stay of majority of the patients in this study may have overestimated the prevalence of malnutrition on discharge. In a study done by Braunschweig et al. (2000), nutritional status deteriorated if confinement was ≥ 7 days. This was the case in this study. Weekly screening of nutritional status is therefore important for those not initially found to “at risk” (Watterson et al., 2009).
As anticipated, malnutrition is detrimental in terms of clinical outcomes. In this study, malnourished patients had prolonged hospital stay and increased risk of in-hospital mortality. These results are identical to that of previous studies (Beghetto et al., 2009; Burgos et al., 2012; Fiaccadori et al., 1999; Gout, Barker, & Crowe, 2009; Gupta et al., 2005; Kyle et al., 2005; Middleton et al., 2001; Ocampo et al., 2008; Ozkalkanli et al., 2009; Raslan et al., 2011; Sacks et al., 2000; Segall et al., 2009; Sorensen et al., 2008; Sungurtekin et al., 2009). Complications can occur when malnutrition adds to a preexisting illness. Malnutrition impairs the body’s ability to mount an effective immune response in the face of stress brought about by sickness (Scrimshaw & DanGiovanni, 1997). A state of malnutrition delays recovery, exacerbates anorexia, and increases convalescence time (Kubrack & Jensen, 2007). However, as malnutrition has complex interactions with illness severity, demonstrating that malnourished patients do poorly does not prove that malnutrition alone causes poor outcomes (Covinsky, 2002).
Recently, the Academy of Nutrition and Dietetics/ A.S.P.E.N. recommended taking into account disease etiology as well as six characteristics (energy intake, weight loss, muscle mass, subcutaneous fat, fluid accumulation, and functional status) to help clinicians recognize malnutrition (White et al., 2012). Once validated, this tool will standardize the approach to the diagnosis of malnutrition.
To my knowledge, this is the first study conducted in the Philippines that documents change in nutritional status. This study has shown that among hospitalized individuals in this tertiary care hospital, malnutrition is prevalent. The typical profile of the patient prone to develop malnutrition is age more than 60 years old, with malignancy and infectious disease, as well as comorbidities like diabetes, cardiovascular conditions, and stroke. These are the patients that would most likely benefit from closer assessment and monitoring of their nutritional status. Malnutrition causes additional burden in terms of prolonged hospital stay and greater risk of death. It is therefore imperative to identify the “nutritionally at risk” patient early in the management phase. Nutritional assessment before, during, and after hospitalization is mandatory to recognize malnutrition early and initiate timely nutritional therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, and/or authorship of this article: This research was supported by grants from St. Louis University.