
Abstract
In 2010-2011, the Vancouver Island Transgender Needs Assessment, a community-based, applied research project, sought to identify the health and social needs of trans people on Vancouver Island, British Columbia, Canada. An advisory board consisting of trans-identified community members and trans-service providers guided this descriptive analysis. A total of 54 individuals identifying as transgender participated in a survey modeled after the TransPULSE Ontario instrument. Of the participants, 43% identified on the transmasculine spectrum, 39% on the transfeminine spectrum, and 18% as transgender/genderqueer only. Participants were surveyed in regard to education, employment, and income; housing; health care needs and services; suicidality; violence; life satisfaction and attitudes toward self; posttransition experiences; and community belonging. They reported health care, social support, and public education/acceptance as top needs. The article concludes with a specific needs profile and a community-generated set of recommendations stressing the need for an island-based information and resourcing center.
In 2010-2011, the Vancouver Island Transgender Needs Assessment, a community-based, applied research project, sought to identify the health and social needs of trans people on Vancouver Island, Canada’s second most populous island. As Green, McGowan, Levi, Wallbank, and Whittle (2011) argued, societies need a broad understanding and acceptance of the range of gender expressions to “reduce the threat of gender essentialism that is needlessly abusive of the human and civil rights of gender-variant and indeed, all people” (p. 4). Needs assessments of transgender and transsexual individuals have found high levels of underemployment and lower levels of income (Clements-Nolle, Marx, & Katz, 2006; Fitzpatrick, Euton, Jones, & Schmidt, 2005; Lombardi, Wilchins, Priesing, & Malouf, 2001; Xavier & Simmons, 2000); high levels of depression (Clements-Nolle, Marx, Guzman, & Katz, 2001; Rotondi, 2011; Rotondi, Bauer, Kaay, Travers, & Travers, 2011; Rotondi, Bauer, Travers, et al., 2011); and high levels of suicidal ideation and attempts (Chamberland & Saewyc, 2011; Grant et al., 2011; Kenagy, 2005; Scanlon, Travers, Coleman, Bauer, & Boyce, 2010; Xavier & Simmons, 2000). Needs assessments have also consistently found needs for trans-related health care information, trans sensitivity awareness programs, and service provider training (Bauer et al., 2009; Sperber, Landers, & Lawrence, 2005; Xavier, Bobbin, Singer, & Budd, 2005). Furthermore, trans individuals have been found to be disproportionately affected by discrimination, unemployment, underemployment, HIV status, alcohol and substance abuse, violence and harassment (Chamberland & Saewyc, 2011; Currah, Juang, & Price Minter, 2006; Grant et al., 2011; Lombardi et al., 2001; Namaste, 2000; Nestle, Howell, & Wilchins, 2002).
In recent decades, estimates of the size of trans populations across the globe have increased (Spack et al., 2012; Winter & Conway, 2011), but population-based estimates of transgender percentages of a population remain rare (Gates, 2011). Estimates range from 0.3% (Gates, 2011) to 0.5% (Conron, Scott, Stowell, & Landers, 2012) to 3% (Winter & Conway, 2011). As Winter and Conway illustrate, if one applies Gates’s (2011) fairly conservative estimate of the U.S. transgender population to the world population, one would estimate about 15 million trans people in the world. Researchers worldwide detect the following trends: an equalizing of the transmasculine and transfeminine populations in terms of numbers, increases in the number of people identifying as transgender and/or presenting for care, and increases in the number of young children and young adults identifying as transgender (De Cuypere et al., 2007; Reed, Rhodes, Schofield, & Wylie, 2009).
Vancouver Island is the world’s 43rd largest island and Canada’s 11th largest island, with increasing population trends. Provincial estimates in 2008 set the island population at 740,000; almost half of the population (330,000) lives in Greater Victoria, the capital of British Columbia. The province has a population of 4.4 million; its largest city, Vancouver, is located on the mainland. The Vancouver metro area has 2.3 million residents. Based on the ranges prevalent in the literature to date, the trans population on Vancouver Island could range from 1,480 (at 0.2%) to 7,400 (at 1%).
In the province of British Columbia, services available to trans populations have changed significantly in the past two decades. The Gender Dysphoria Program (commonly referred to as the “Gender Clinic”), offered by the Centre for Sexual Medicine of the Vancouver Hospital and Health Sciences Centre since the 1980s, closed in 2002. The Gender Clinic provided specialized psychological, psychiatric, endocrinological, urological, gynecological and social services to trans people and their families in a model that centralized services for the province. It was also the only provider recognized by the Medical Services Plan of British Columbia (MSP) to assess patients for surgery. The closure of the clinic created an urgent demand for access to trans services. Two months after the closure was announced, staff of Vancouver Coastal Health (VCH) met with trans organizations. VCH is one of six publicly funded, regional, health care authorities providing medical services to approximately 25% (1 million people) of British Columbia’s population. Participants reached consensus that there was “a need to create an alternative model for health service delivery to transgendered people across the province” (Goldberg, Matte, MacMillan, & Hudspith, 2003, p. 2). A community survey on transition and crossdressing services in British Columbia resulted from the meeting and yielded 179 responses, including 37 from Vancouver Island. The community survey identified immediate needs: access to endocrinological information for providers and patients, a crisis plan for trans people affected by the closure of the Gender Clinic, and a resource list of health and social service professionals for the province. Participants further identified ongoing needs: an ongoing partnership between service users and VCH staff, service delivery planning based on the Harry Benjamin International Gender Dysphoria Association’s (now World Professional Association for Transgender Health) Standards of Care, and a blended model of service delivery including centralized and decentralized structures to reach the greatest number of service users (Greater Vancouver Region) but also allowing access for those in other parts of the province, and physician training. Overall, the survey pointed “to the need for a comprehensive model of service delivery, one that addresses the social determinants of health” (Goldberg et al., 2003, p. 26). Kopala (2003), a clinical professor with the Center for Complex Disorders in the Department of Psychiatry at the University of British Columbia, also analyzed the survey results and conducted further focus groups and interviews. Kopala offered a list of 19 specific recommendations, including the creation of a new community-based transgender health center in Vancouver; partnerships between medical providers, clients, and advocacy organizations; and creation of educational and information materials including a web site and workshop curricula. These efforts led to the creation of the VCH Transgender Health Program in 2003. A 1-year report on the program reported the top three barriers for health and social service access as cost, lack of availability, and waitlists (Goldberg, 2004). The Transgender Health Program partnered with Transcend Transgender Support & Education Society to develop the Trans Care Project. The Canadian Rainbow Health Coalition funded this project, which ran from 2004 to 2006, to develop a series of clinical care guidelines.
Members of trans communities and allies in British Columbia have continued to engage in community-based research to better understand the issues facing trans communities and to use this information to bring about change. In 2008, a survey of the Department of Family Practice in the Faculty of Medicine at the University of British Columbia asked respondents about transgender health issues. The results were not published but presented at conferences and used informally within VCH programs to improve care delivery and to inform advocacy efforts with other organizations. The Transgender Health Program remains in place today (transhealth.vch.ca); its mission continues to be “to bring together transgender people and loved ones, health care providers, health planners, and researchers to work on improving transgender health services in BC” (transhealth.vch.ca). The Transgender Health Program is an information program, not a clinical program. It has a mandate to serve the entire province, yet the annual budget is only about CAD$130,000, and since the program’s foundation, support groups run by the program have only met in Vancouver. Transportation to and from Victoria, the capital of British Columbia, to Vancouver is by plane or ferry only and expensive, with a vehicle round-trip by ferry costing about CAD$130 for one person as of June 2013.
There are no Transgender Health Program resources dedicated specifically to Vancouver Island. Many island residents rely on the program’s website as it is the only government-supported centralized resource. However, it contains little information pertaining to Vancouver Island, and some of the island-specific information is dated. Applied research conducted by providers and community members, island students, and faculty in recent years has focused substantially on Vancouver-area populations although some included participants from Vancouver Island (Goldberg et al., 2003; Townsend, 2009). It appears that there has never been a Vancouver Island-specific needs assessment despite the documented presence of trans individuals and/or communities in all geographic areas of Vancouver Island. The Gay/Lesbian/Bisexual/Transgender student organizations of the University of Victoria and Camosun College are the primary sponsors of events open to the Greater Victoria public; a community activist group (TransAction Victoria) is intermittently active and maintains a Facebook presence.
An advisory board consisting of trans-identified community members and trans-service providers guided the design of the study, which was led by a researcher who had transitioned on the island. Complementary to the applied rationale of establishing empirical information about the needs of the island trans population, the advisory board also envisioned the Vancouver Island Needs Assessment to add to the growing global database of community needs assessments (e.g., Kenagy, 2005; O’Brien, 2006; Xavier et al., 2005; Xavier & Simmons, 2000). As Bauer, Travers, Scanlon, and Coleman (2012) noted, little is known about sociodemographic factors in Canadian trans communities; much of the data are based on U.S. communities. There is a lack of reliable Canadian national probability samples for transgender populations. As the project goals were to generate a descriptive analysis of island needs and to create knowledge as a tool for social change, local trans people were involved in every stage of the research. The research process began with a compilation of island resources and led from the administration of the survey to community debriefings and a community workshop, knowledge dissemination, and generation of recommendations.
Method
The research question guiding the project asked: What are the needs of trans individuals and communities on Vancouver Island?
Survey Instrument
The research team received permission from the TransPULSE Ontario (http://www.transpulseproject.ca/aboutTransPulse.html) project to replicate portions of its survey instrument, which had been developed over a period of several years via extensive community collaboration and consultation and was vetted by the University of Western Ontario as well as the Canadian Professional Association for Transgender Health (CPATH). Funding by the Canadian Institutes of Health Research, Canada’s federal agency for funding health research, reflects the scholarly endorsement of the survey instrument created in this process. The Trans PULSE study is the largest Canadian study to date. This constituted an efficient use of resources, allowed the adoption of a high-quality instrument, and created the potential for data comparisons. The original TransPULSE survey was extensive (87 pages); the research team distilled the Vancouver Island survey to 22 pages and adapted a number of questions to be specific to the island. Questions selected for the Vancouver Island instrument focused on access to health services, employment, housing, information access, public acceptance, violence, social support, and community. The Vancouver Island survey was administered as a multimode survey, meaning that respondents could receive a copy in the mail and return it via stamped, pre-addressed envelopes; fill out the survey during a meeting with the researcher; complete the survey over the phone if requested; or complete, scan, and email the survey back to the researcher.
Data Collection
In contrast to the TransPULSE Ontario survey, which placed significant emphasis on its respondent-driven sampling process, the researchers administered the Vancouver Island survey via snowball and network sampling with the simple aim of attracting as many respondents as possible. It was important to the island research team to establish an empirical, inclusive data set with much time spent on personally connecting with the participants. Data analysis consisted of descriptive statistics such as frequencies, means, and percentages. Surveys were administered from 2010 to 2011. Research Ethics Board approval was granted by the Royal Roads University Research Ethics Board. Participants were recruited via flyers, emails, online groups, social media posts, trans-service providers, GLBTQ community and student groups, researchers, and activists, ensuring that each formally organized GLBTQ presence on the island was aware of the study and disseminated the recruitment flyer. Participants had to be 18 or older and live on Vancouver Island or on one of the small surrounding islands. Participants had to self-identify as “trans” following the Vancouver Coastal Transgender Health Program definition as, a person with a gender identity that is different from their birth sex or who expresses their gender in ways that contravene societal expectations of the range of possibilities for men and women. This umbrella term may include crossdressers, drag kings/queens, transsexuals, people who are androgynous, Two-Spirit people, and people who are bi-gendered or multi-gendered, as well as people who do not identify with any labels. (transhealth.vch.ca)
The consent form provided the definition cited above; participants also were explicitly asked to affirm that they considered themselves to be “trans” on the survey.
Prospective participants received a consent form and engaged in electronic or face-to-face conversations about the purpose of the project with the lead researcher. The majority (43) of the 54 survey respondents met with the researcher at a place of their choice to obtain the survey and to discuss the project; sometimes participants chose to complete the survey in the presence of the researcher. Participants received a CAD$15 grocery card after submitting a completed survey; they also received a CAD$10 grocery card for successfully referring other prospective participants. About a third of participants were recruited via this snowball sampling technique.
Data Analysis
A research assistant tabulated the survey results, and the lead researcher cross-checked them. The survey also asked respondents to identify their top need in an open-ended response. The researchers coded and thematically grouped the responses following a “general inductive approach for qualitative data analysis” commonly used in health and social science research (Thomas, 2003). This approach consisted of two independent readings of the open-ended responses by two research assistants and comparison of the categories, which emerged from the data. Not all respondents answered all questions; this is reflected in the numerical responses via adjusted totals of responses. The four surveys that lacked more than 10% of responses to questions were excluded from the data analysis. The data analysis provides a breakdown of transfeminine, transmasculine, and transgender/genderqueer individuals to ensure that those who do not identify along gender binaries are not rendered invisible (Harrison, Grant, & Herman, 2012). The categories of transmasculine and transfeminine were operationalized to refer to transgender people assigned to the female sex at birth and identifying as male or masculine now (transmasculine) and to refer to transgender people assigned to the male sex at birth and identifying as female or feminine now (transfeminine).
The preliminary results of the study were presented at a public presentation on November 9, 2011, in Victoria; a group of 20 individuals stayed for an open community workshop that allowed participants to discuss the findings and generate recommendations for health educators, governmental agencies, service providers, and the community itself.
Results
Participant Demographics
All participants identified as “trans” and ranged in age from 18 to 68 (M = 40); 52% had been assigned to the female sex at birth, and 48% had been assigned to the male sex at birth. Of all participants, 43% identified on the transmasculine spectrum, meaning they selected boy/man and/or trans boy/trans man and/or FTM to describe their gender identity; 39% identified on the transfeminine spectrum, meaning they selected girl/woman and/or trans girl/trans woman and/or MTF to describe their gender identity. The remaining 18% described their gender identity as transgender, bigender, mixed gender, or genderqueer only and did not select a gender-specific referent. Two thirds (67%) of the respondents identified (not exclusively) with the gender/sex opposite from the gender/sex assigned at birth (boy/man or girl/woman); a third (33%) of the respondents identified with a trans-identifying label (e.g., transgender, trans boy, trans girl, genderqueer) only. The majority (60%) selected more than one label to describe their sexual orientation. Overall, the most frequently chosen label was queer (41%); participants assigned to the male sex at birth most frequently chose the label lesbian (18%), followed by bisexual (15%); participants assigned to the female sex at birth most frequently selected the label queer (28%), followed by straight (17%). Half of the participants (50%) fell into the age category 31 to 50 years of age; the second most frequent age group was 18- to 30-year-olds (28%), then those aged 51 and above (22%). Transmasculine participants had a mean age of 35, transfeminine participants a mean age of 43, and transgender/genderqueer participants a mean age of 46. The majority of participants (83%) had transitioned socially and/or physically or was living in their felt gender. At least 18%, however, did not publicly identify as transgender or transsexual, did not participate in trans community events and only participated in the survey after having assured themselves that strict confidentiality would be maintained. Most (63%) lived in the Greater Victoria area; the remainder came from Central Vancouver Island (11%), Nanaimo (7%), Southern Vancouver Island (7%), Northern Vancouver Island (2%), remote rural locations (4%), and neighboring islands (6%). In terms of ethnicity, 67% were of British descent, 47% of other European descent, 13% of Aboriginal descent, and 9% of East or South Asian descent. Table 1 provides an overview of the participants’ gender identity, sexual orientation, and ethnicity.
Sexual Orientation, Gender Identity, and Ethnicity Vancouver Island Survey Respondents, 2010-2011 (n = 54).

Participants were also given the opportunity to provide a label of their own. No label provided by the participants yielded more than four mentions.
Participants were able to select more than one identifier.
Top Needs
In response to the open-ended question asking participants to identify their personal top need, health care (24%), social support (24%), and public education/acceptance (19%) emerged as top needs. Fewer prioritized mental health care access (12%), legal assistance (7%), or employment (7%) as priority needs. The remaining answers yielded other individualized concerns. Specifically, participants identified health care needs as quick, affordable access to surgeries within the province (12%); local, speedy access to trans-specific medical expertise (10%); and access to information about long-term use of hormones (2%). The participants identified social support needs as support for the community (17%) and support from the community (7%). Specifically, they identified such needs as a physical community space; access to current, local information, and resources; an opportunity to provide support as much as to receive it; peer and professionally guided support groups; hotlines; recreational and nonactivist social events; and an island-specific web site with current information. In regard to public education/acceptance, participants noted a need to educate the public on trans-related issues. In regard to mental health care access, respondents noted that it’s difficult to obtain affordable individual therapy in a timely manner in general and that free or affordable access to therapists with trans expertise is scarce.
Health Care
Conditions
About half (54%) of the participants declared health issues other than gender identity issues. Of these, 20% reported more than one condition. The most commonly reported conditions were mental health (24%), chronic illness (22%), and mobility conditions (18%). The survey differentiated between mental health care needed for reasons related to gender identity and mental health care needed for other reasons. Most (68%) had accessed mental health care due to being trans; five respondents noted in handwritten notes that they only accessed mental health for gender-identity-related reasons because this was a requirement for access to surgery and/or hormones.
Access to care
The majority had British Columbia health care coverage (96%) and a family doctor (85%). The majority (72%) had had to travel away from their hometown to obtain trans-related medical care at some point. Travel required to obtain services included 9% traveling to another town on the island, 43% traveling to the mainland, 13% traveling to another province (Alberta, Ontario, Quebec, Saskatchewan), and 11% traveling to another country (United States, Thailand, Belgium). Travel was mostly necessary to obtain surgical care. Of the 68% who had accessed mental health care for trans issues, 19% declared having mental health issues. Thirty percent of all participants said they continue to need access to trans-related mental health care and cannot obtain such care. Mental health care services requested most frequently for reasons related to gender identity were support groups, psychologists, and social worker/counselors. A total of 54% said they need access to mental health services for issues other than for their gender identity, and of those, 24% said they cannot obtain access to such care. Mental health care services requested most frequently for reasons other than gender identity were social workers/counselors and support groups.
Hormones
Of all, 61% were currently taking hormones. Of the remainder, 20% were still deciding whether hormones are right for them, 9% had taken hormones in the past but stopped, 9% could not find a doctor to prescribe hormones, 6% were not interested in taking hormones, 4% had been denied hormones, and 4% were waiting for the beginning of hormone therapy. Of the respondents currently taking hormones, 79% reported that the effect of hormones on their body was consistently monitored by a physician. The majority (65%) considered the Internet to be their primary source of information about hormones. Other sources of information about hormones were physicians (39%), trans community (24%), friends (20%), medical journals, (17%) and print media (6%). Most (61%) said they had sufficient information about hormones for gender transition or confirmation; 31% said they weren’t sure if they had sufficient information.
Quality of care
Half (52%) did not report any negative behavior from family physicians. Negative behaviors were identified as the following: refusal to provide care; ending care; using hurtful or insulting language; refusing to address trans-related issues; stating that one is not really trans; discouraging gender exploration; refusal to examine body parts; belittling or ridiculing; or stating that lack of knowledge meant they could not provide care. The most commonly reported (30%) type of negative behavior was the lack of knowledge to provide care. A majority (68%) of those who sought mental health care reported no negative behaviors from mental health providers; the most commonly reported types of negative behavior were lack of knowledge to provide care tied with negation of one’s trans identity. The majority (76%) said they trust physicians mostly or completely in regard to confidentiality. Of the participants with a regular family doctor, most (86%) were comfortable or very comfortable discussing their trans status and trans-specific health care needs. Most respondents (59%) said they would feel uncomfortable or very uncomfortable discussing trans issues with a doctor they did not know. The survey also inquired about respondents’ assessments of provider knowledge. Of those who had a regular doctor, 37% reported not having had to provide education about trans issues; 63% reported having had to provide education. Of those who had a regular doctor, 11% said their doctor was not at all knowledgeable, 43% said somewhat knowledgeable, 26% knowledgeable, 13% very knowledgeable, and 7% said they did not know how knowledgeable their doctor was. Of those who had accessed mental health care due to being trans, 51% said they never had to educate a mental health care provider, and 49% said they had to provide education.
Suicidality
The majority (63%) reported having either considered (35%) or considered and attempted (28%) suicide. Of those who considered committing suicide, 71% attributed this to being trans, which means that of all participants in the study, 44% considered committing suicide due to trans-related factors. Participants assigned to the female sex at birth reported a higher rate (68%) of considering or attempting suicide than participants assigned to the male sex at birth (58%). Of those who had considered and attempted suicide, 15% declared a mental health condition as did 12% of the participants who had considered but not attempted suicide. The age group reporting the highest number of considerations or attempts (50%) was 31 to 50 years.
Table 2 provides an overview of participants’ self-reported health care needs.
Self-Reported Health Care Needs, Vancouver Island Survey Respondents, 2010-2011 (n = 54).

Percentages based on N seeking care.
Social Support
Community belonging
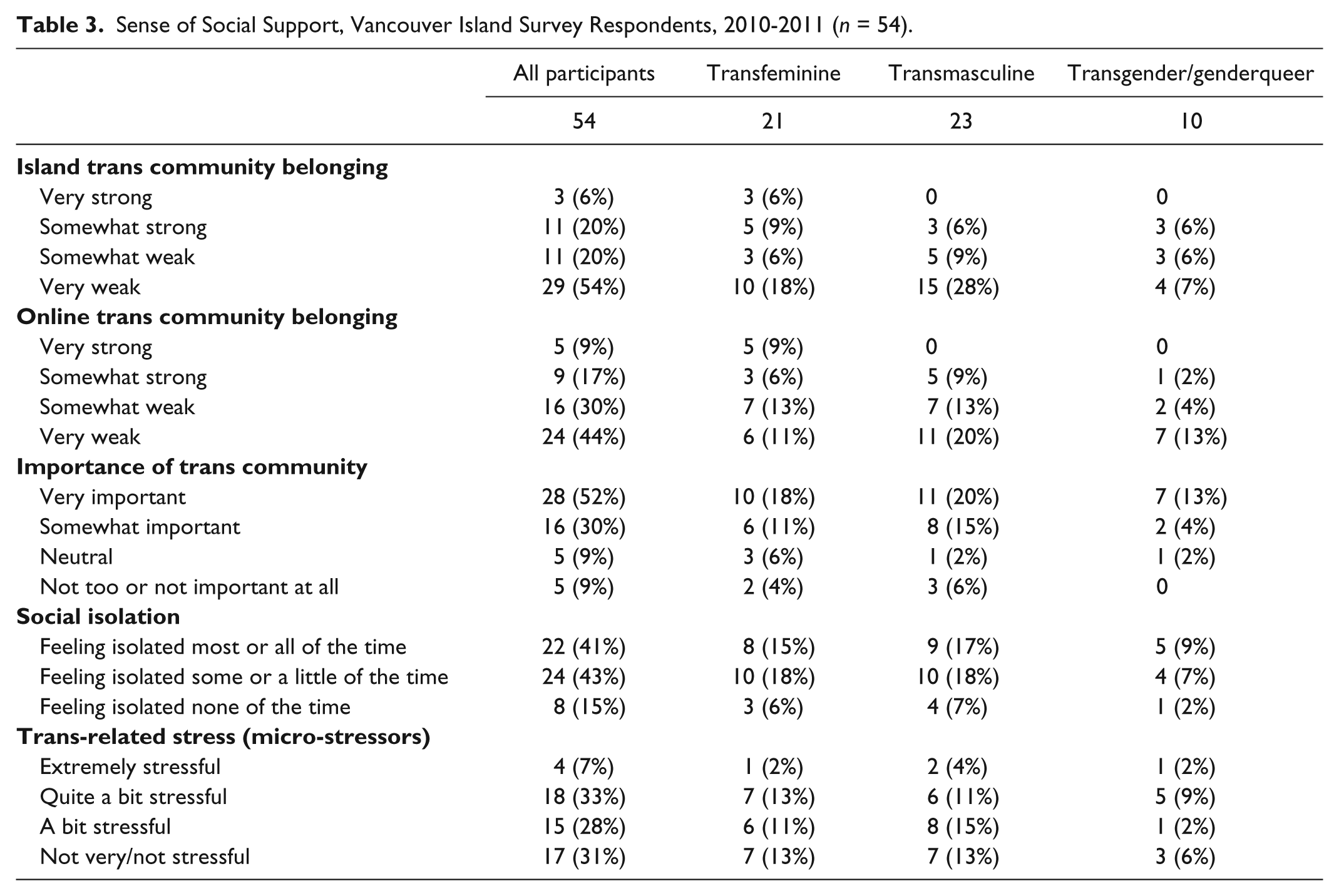
The survey explored individuals’ sense of belonging to a “trans community” to better analyze social isolation and communication needs. The majority (74%) described their sense of belonging to the island “trans community” as somewhat weak (20%) or very weak (54%). Most (92%) also described their sense of belonging to the mainland “trans community” as somewhat weak (22%) or very weak (70%). Most (85%) described their sense of belonging to the international “trans community” as somewhat weak (17%) or very weak (68%). Participants identified the strongest sense of belonging with an online trans community but even in this setting, the majority (74%) described their sense of belonging as somewhat weak (30%) or very weak (44%). At the same time, most (82%) reported that being connected to a strong trans community was very important (52%) or somewhat important (30%) to them.
Social isolation
Measures of social isolation were consistent with a weak sense of community belonging. Of the total sample, 41% reported feeling most or all of the time socially isolated. Of the pretransition participants, 67% reported feeling most or all of the time socially isolated. Participants reported having between 1 and 30 close friends and relatives—defined as people whom they felt at ease with and could speak to freely. The mean number of close friends was 2.6, with 26% of participants reporting more than five close friends and 13% reporting having one close friend. Participants reported that someone would be available to help them with daily chores if they were sick all of the time (22%), most of the time (24%), some of the time (13%), a little of the time (24%), or none of the time (17%). Participants also reported that someone would be available to listen when they need someone to talk to all of the time (19%), most of the time (24%), some of the time (28%), a little of the time (28%), or none of the time (2%). Twenty-one participants (39%) said they have worried many times about growing old alone; 33% sometimes, 15% once or twice, and 11% never. Micro-stressors related to being trans were also identified; 68% reported the amount of trans-related stress in their lives as a bit, quite a bit, or extremely stressful. Table 3 provides an overview of measures of social support.
Sense of Social Support, Vancouver Island Survey Respondents, 2010-2011 (n = 54).
Public Education/Acceptance
Life satisfaction
The majority (68%) reported being either somewhat or very satisfied with their life in general and consistently reported positive attitudes toward self. This trend was also reflected in unsolicited personal communication from participants. A majority of respondents indicated that they were satisfied with themselves, had a number of good qualities, were able to do things as well as others, were a person of worth equal to others, and took a positive attitude toward themselves. The only item on which participants reported negative attitudes toward self was self-respect, with 67% stating that they wished they could respect themselves more. The majority of participants who had transitioned socially and/or physically or were living in their felt gender and reported that their quality of life had improved somewhat (38%) or a lot (29%) since transitioning. The majority of those who had either not transitioned or were not living in their felt gender (17% of all participants) expected that their quality of life would stay the same (44%) or get worse (33%) after transition.
Acceptance
Of all, 24% experienced being made fun of or called names for being trans many times, 17% sometimes, 43% once or twice, and 15% never. Many (57%) had heard many times that trans people are not normal; 19% had heard it sometimes; 17% once or twice, and 6% never. Respondents had felt that being trans hurt and embarrassed their family many times (43%), sometimes (26%), once or twice (11%), or never (15%). Respondents had felt that being trans hurt and embarrassed their friends many times (21%), sometimes (35%), once or twice (19%), or never (25%). Respondents had felt that being trans hurt and embarrassed their employer/colleagues many times (6%), sometimes (22%), once or twice (15%), or never (39%). Since identifying as trans, respondents reported many times (21%), sometimes (35%), once or twice (19%), or never (22%) trying to pass as non-trans to be accepted. Most (87%) reported that they had not experienced physical violence or sexual assault; 13% did experience physical violence and/or sexual assault. A majority (79%) reported never having experienced any form of police harassment for being trans. More than half of the participants who had transitioned or were living in their felt gender rated parents, siblings, and significant others as somewhat or very supportive of their transition.
Participants who had transitioned reported avoiding a number of situations due to the fear of being harassed, being read as trans, or being outed. Of these participants, 56% had experienced verbal harassment; a majority of 82% had experienced silent harassment, defined in the survey as “e.g., being stared at, being whispered about.” Sixteen percent had experienced sexual harassment (“e.g., cat calling, being propositioned”), 11% physical intimidation and threats, and 13% physical violence (“e.g., being hit, kicked or punched”) and/or sexual assaults (“e.g., unwanted sexual touching or sexual activity”). The majority reported avoiding gyms or pools, followed by public washrooms and clubs or social groups, because of a fear of being harassed or outed. More than half (56%) of those who had not transitioned expected that they would experience physical intimidation and threats during or after transition. A majority (89%) expected they would experience silent harassment and verbal harassment. The majority (78%) expected that they would avoid gyms or pools, not travel abroad (67%) and avoid public washrooms (44%) because of a fear of being harassed or outed posttransition. Pretransition expectations were more negative than actual experiences reported by those who had transitioned.
Table 4 provides an overview of measures related to public education and acceptance.
Public Education/Acceptance, Vancouver Island Survey Respondents, 2010-2011 (n = 54).

Discussion
The largest survey of transgender people ever in the United States (Grant et al., 2011) concluded that
Transgender and gender non-conforming people face injustice at every turn: in childhood homes, in school systems that promise to shelter and educate, in hard and exclusionary workplaces, at the grocery store, the hotel front desk, in doctors’ offices and emergency rooms, before judges and at the hands of landlords, police officers, health care workers and other service providers. (p. 2)
The findings presented here reflect a differentiated picture for the Canadian island participants in this study, a picture that contains some of the elements of structural and personal discrimination identified by other surveys but one that also reflects positive experiences of support by institutions and individuals.
Health Care
Given the differences between the U.S. and the Canadian health care systems, it is not surprising that the majority of participants (85%) had a family doctor, which is on par with the provincial average of 86.1% reported in the 2011 Census of the Population. Participants voiced strong trust and levels of comfort in regard to regular family physician interactions but not for interactions with providers they did not know. They expressed concerns about the extent of general physicians’ level of knowledge. Participants expressed a need for trans-related health care information, trans sensitivity awareness programs, and training for service providers. Even those providing social and medical transgender case advocacy are likely to need additional support and access to information (Holman & Goldberg, 2006; Lawrence, 2007). Since the inception of the study, several training sessions for providers on the island have taken place. The Women’s Sexual Assault Centre of Victoria offered a series of trainings in early 2012 to help center staff improve the capacity to support trans and gender-variant people; the first session was a primer workshop (Trans 101) offered by the medical director of the Transgender Health Program. In a similar vein, a program in Fall 2011 trained outreach health workers at a youth clinic in Victoria.
Consistent with prior research, this study reflected high rates of suicidal ideation and attempts. Seven participants noted (by providing comments in margins or specifically raising this in verbal communication or interviews) that suicidal ideation or attempts were a temporary phenomenon and had stopped being a part of their lives post transition. This aligns with Bauer’s (2012) findings that trans people’s risk for suicidal ideation and attempts dropped to almost none for participants who had completed transitioning, based on their own assessment.
Social Support
According to Statistics Canada research (Shields, 2008), a strong sense of community belonging is linked to good physical and mental health. This study supports previous studies’ findings about the social isolation experience of trans people. Clearly, the community and social belonging needs of trans people on Vancouver Island are not met. Apart from university and college student support groups, no institutionally backed support groups exist in the area. Currently, information appears mostly to be sought and obtained via online groups (e.g., Yahoo groups, Facebook) of alias identities, which puts the burden of assessing the safety and credibility of that information on the individual. Queries posted to the island resource website created in conjunction with this project often consist of requests for endorsed physicians and counselors, safe and confidential contacts with other local trans people, and ways of socially transitioning on the island. Although participants consistently reported that they relied on the Internet to access information about transgender issues and to connect with trans people, a trend that has been widely documented (Kailey, 2005; Shelley, 2008), it is clear from the measures of belonging that electronic communication is not perceived as a sufficient substitute for face-to-face contact. The assessment suggests that information and communication needs are not being consistently met, and that lack of an island-specific, centralized, public information center makes it difficult to identify resources even if they are available.
The findings lead to the following recommendations:
Easier and faster access to knowledgeable providers who are experienced in transgender physical and mental health care;
Availability of an online, current, public, credible resource list of professionals and agencies on the island;
Staffing of a province-wide toll-free 24-hr phone line for emergency counseling; referral to providers, agencies, and trans community support; and information for health care providers;
Institutional maintenance (e.g., public health program) of an interactive online presence for a Vancouver Island transgender health and information program that integrates social media (Twitter, Facebook, discussion groups);
Community-led peer support groups and speakers’ bureaus for public presentations in schools, chambers of commerce, government agencies, and so on;
Availability of public education resources (pamphlets, guides) that describe the various steps involved in transitioning (e.g., name change, gender marker change) with specific, current, local information and contacts;
Financial support for a Vancouver Island transgender information and resource center that allows for a physical drop-in space, community meeting space and resource library, support group meetings, social events and funding for a part-time or full-time coordinator.
Several of these recommendations are identical to those of Kopala’s (2003) recommendations for a transgender health program in British Columbia. While the Transgender Health Program of Vancouver Health Authority includes some of these recommended features, it is apparent that the degree of geographical distance from the Vancouver metro contributes to a specific subset of needs on Vancouver Island. For Vancouver Island trans people, identification of and access to local (island) resources is crucial.
Since the study was conducted, a group of Victoria-based individuals has revived an online directory of gay/lesbian/bisexual/and trans-friendly providers and services. Another group of local trans people has begun holding a social night once a month, and outreach to trans youth in particular has increased by several gay/lesbian/bisexual/trans organizations. However, these efforts are driven by individual volunteer efforts and ebb and flow as individuals’ time and interests or access to resources change. For example, a local queer thrift store (Out of the Closet) started up in July 2010. It offered a trans-friendly community bulletin board and was supported by volunteers from the trans community, but these opportunities ended when the store closed in October 2012. One question that, in retrospect, would have been an informative question to include was that of individuals’ perception of the size of the trans population on the island. It was often the first question that participants asked of the lead researcher—How many of us do you think there are? This was often followed by a disclosure that the individual either knew only of a handful of other trans people on the island and, later on, surprise at the number of participants who had taken part in the study. Perception of the size of the community likely has an effect on the experience of social isolation, although this is a potential relationship that would need to be examined.
Public Education/Acceptance
The findings point to the need to examine and identify more complex patterns within trans populations. The participants reported, overall, high levels of support and positive attitudes toward self, yet still reported high rates of suicidal ideation and attempts. The expectations of those considering transition appeared more negative than the actual experiences of those who had completed their transitions. The World Professional Association for Transgender Health (Coleman et al., 2012) urges, in its 2012 Standards of Care, “the de-psychopathologization of gender nonconformity worldwide” (p. 168) and notes that the stigma that societies often attach to gender nonconformity causes significant minority stress. Minority stress “may make transsexual, transgender, and gender-noncomforming individuals more vulnerable to developing mental health problems” (p. 168). Measures of stress are important as the prevalence of mental health issues has been theoretically linked to stress resulting from stigma and marginalization (Chamberland & Saewyc, 2011; Hatzenbuehler, 2009; Meyer, 2003).
Many participants were quite vocal, during the recruitment and survey administration process, that they did not feel represented by victimizing portrayals and that they live productive lives. Of those individuals who considered themselves not out, most volunteered that they were participating out of a desire to give back and to provide support, rather than receive support. They also spoke of the need to build community with others who feel positively about being trans and do not vocalize negative attitudes toward self. This is consistent with cultural trends. Alegria (2011) points to more positive media coverage of transgender people in recent years as well as a higher level of education and social activism by transgender people. Greatheart (2010) conducted a narrative study involving eight people on the female-to-male spectrum in Vancouver. These participants discussed, in focus groups and in-depth interviews, their dissatisfaction with the “dominant negative transition story” and pathologizing discourse perpetuated by peers and providers, and they described positive transition experiences, including navigation of the health care system (p. ii).
These findings further suggest a need to be sensitive to the particular cultural, geographical, and political locale of trans populations. While there is some overlap with U.S.-generated recommendations to improve services for trans people, other areas diverge in a direct reflection of different legal and sociopolitical realities across nations, provinces, and states. The intersectionalities of discrimination (ethnicity, class, ability status, income) may play out differently in larger urban centers than in other locations and have been shown to affect one’s trans identity process and understanding and lead to different levels of social support (Eliason & Schope, 2007; Koken, Bimbi, & Parsons, 2009). It is worth considering the transformative potential within the community itself. Indicators such as life satisfaction, support from social networks, and positive transition experiences underscore the possibility that trans communities can be proactive in helping those struggling with issues of gender identity. The findings demonstrate that trans individuals and communities need some assistance in doing so.
Limitations
This needs assessment presents a descriptive analysis of a particular point in time. Since the inception of the project, volunteer organizations have come and gone, and individual involvement of community leaders has changed significantly. The study would have benefitted from a larger sample, a probability sample, comparison groups, or within-group statistical testing. The participant demographics reflect, broadly speaking, Vancouver Island ethnic distributions; participant identifications in regard to gender identity are consistent with research reflecting increasing adaptation of “transgender” or “genderqueer” identification among trans people (Ekins & King, 2006; Gay, Bisexual and MSM . . . , 2012; Yerke & Mitchell, 2011). The participants in this study reported few experiences of violence and crime; however, this survey reported on a convenience sample. Despite outreach attempts by members of the community, particularly marginalized demographic groups, such as sex trade workers, immigrants, refugees, migrants, homeless people, racialized people, youth, the elderly, or prison inmates (Holman & Goldberg, 2006) were not widely represented. The needs assessment did not specifically assess HIV status, and while participants did not raise HIV status as a top need, it is possible that some of the 12 participants who declared chronic illness may be HIV positive. Given the sampling, the results should not be construed to argue that these issues are not of concern to all of the trans population on the island. However, the survey does reflect that for the majority of 54 trans people on the island, characterizations of pathology and victimization do not reflect their everyday experiences. The results point to the overall need of an island-based central information and resourcing agency, center, or unit that can provide the institutional stability and credibility required to consistently frame volunteer efforts; serve as a resource to trans people, their families and friends, and health care providers; and help implement the community-generated recommendations.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the Advisory Board of the Vancouver Island Transgender Needs Assessment: Aaron H. Devor, Gail Knudson, Lenore Newman, Bernard Schissel, Liam (Captain) Snowdon, Lucretia van den Berg, and Julian Young and to the Research Assistants Theo Jakob Naven and Jordan Duffy. This study could not have taken place without the generous support, advice and participation of members of the transgender communities and supporters on Vancouver Island and members of the TransPULSE Ontario Project. The feedback provided by Marria Townsend and Todd Sakakibara, physicians at Three Bridges Community Health Centre in Vancouver who provide care to transgender clients, was invaluable. The authors also gratefully acknowledge the feedback provided by peer reviewers and the article editor.
Authors’ Note
This article presents the final results and supersedes earlier releases of preliminary results.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Funding for the needs assessment was provided by internal research grant support of Royal Roads University.