
Abstract
It is argued that to improve health, health systems are required to meet people’s needs and therefore health systems should identify these needs and find a way to prioritize these. For those with chronic diseases, these needs are necessary to manage their condition and go beyond purely the health system. A literature search found that studies published on identifying the needs of people with chronic diseases fall into the following categories: standardized tools, comparison of needs between individuals and health professionals, tools for evaluation, and description of needs. This review highlights the gap between tools used to assess health care needs versus needs for health. It found that a considerable portion of articles focused solely on health care needs. Many tools focused specifically on psychological or psychosocial needs and only one tool identified included a broad range of needs for health. The literature fails to address the wider needs of people with chronic conditions and is still focused on medical interventions. Given the disease burden and the impact of needs outside of the formal health system, needs assessments should be able to capture the full range and scope of the needs of an individual.
Introduction
As argued by Asadi-Lari, Packham, and Gray (2003b), to improve health, health systems are required to be designed to meet people’s needs. However, what do we mean by the word “need” especially with regard to meeting the individual’s need or needs in terms of health and health care?
Needs are what is necessary for humans to develop and function normally (Brewster Smith, 1977; Lederer, 1980). A need is created by something that is lacking and creates a state of “disequilibrium” (Doyal & Gough, 1991). Alderfer (1972) states that needs are required to be met for the “maintenance of homeostasis.” Needs are something necessary to achieve a given state of being, for example, being healthy, a member of a family, a worker, and so on (McLean & McMillan, 2009). Most authors agree that meeting basic needs prevents “serious harm” and death (Doyal & Gough, 1991; Kamenetzky, 1992; Lederer, 1980; Mallmann, 1980; Marshall, 1998; McLean & McMillan, 2009; Reader, 2005; Soper, 1981; Thomson, 1987; Wiggins, 2005). Others add to this definition, specifically referring to the avoidance of illness and improvement of quality of life (Loewy, 1990; C. B. Macpherson, 1977). Gough (2004) and Alkire (2005) state that needs and the way they are met are often determined by experts and not people who they are supposed to benefit. Needs as defined by experts are referred to as normative needs. In looking at normative needs, these are defined through guidelines. As experts may disagree and also evidence may change over time, differences may exist in these normatively defined needs. It is also debatable if these needs are applicable to the population as a whole.
Need in health care is caused by some form of “disturbance in health and well-being” (Donabedian, 1973). Cohen (1996) states that health care is a basic need as if the person does not receive this care he or she will greatly suffer from it. Also health and therefore health care are necessary for participation in society, which makes it an essential need (Loewy, 1990). In addition, needs in health care are “teleological” in that they serve a purpose rather than being needed themselves (Asadi-Lari, Packham, & Gray, 2003a; Baldwin, 1998). For example, the need for insulin itself is linked to it being necessary for survival. McKee (1996) discusses the requirement to differentiate between the need for health care and the need for health. The need for health care is based on interventions and can be viewed as a medical approach, whereas health incorporates wider social issues. The Medical Subject Heading (MeSH) “Needs assessment” is defined as “Systematic identification of a population’s needs or the assessment of individuals to determine the proper level of services needed” (National Library of Medicine, 2012). This term captures the difference discussed by McKee between health care needs and needs for health. This review will assess whether for chronic diseases and diabetes needs assessments focus on the delivery of health care services or address wider social issues to assess the gap in the literature.
Method
Entering the term “needs assessment” into PubMed, with a limit on the term only appearing in the title and abstract, no limits on language and articles published in the past 20 years yields 2,418 results. Adding the search term of “chronic disease” yields 18 results. From these, 9 were excluded as it was felt that they did not fit in with this precise definition of the MeSH term. For example, 3 of these articles focused on the needs of professionals for specific training. This process is detailed in Figure 1.
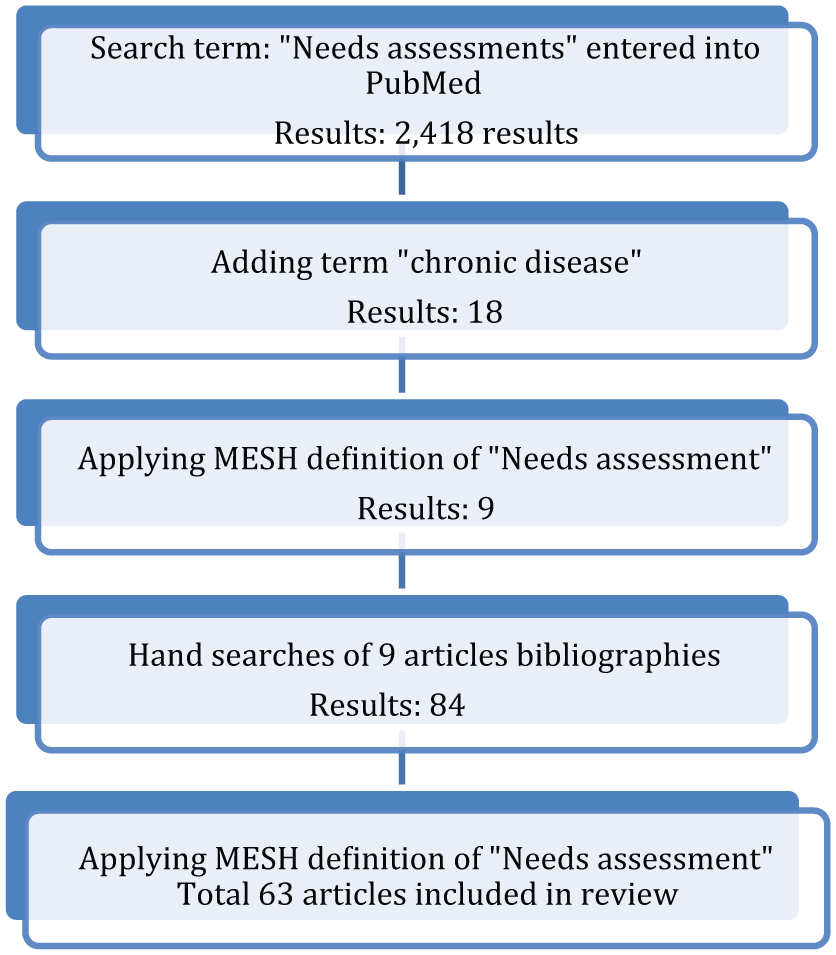
Literature review process.
Further hand searches of articles referenced in these publications by the author enabled another 75 articles to be identified. Again, the MeSH definition of needs assessment was applied focusing only on publications dealing with chronic conditions or diabetes, but no limit was placed on time of publication. A specific focus on diabetes was also used to identify some of these further publications. Diabetes was chosen as it has been argued that it is a good condition to be used as a tracer for health systems and their management of chronic diseases (Beran, 2012; Kessner, Carolyn, & Singer, 1973; Nolte, Bain, & McKee, 2006). Each article was assessed based on the definition and then classified into different categories as well as assessed if it addressed health care needs and/or needs for health.
Results
A total of 63 articles were reviewed to assess whether they assessed health care needs or needs for health. Fifty-eight articles focusing on chronic diseases or diabetes were classified into the following categories:
Standardized tools;
Comparison of needs between individuals and health professionals;
Tools for evaluation;
Description of needs.
Each of these types of tools plays a role in assessing the range and scope of needs an individual may have taking different approaches. Five were specifically for diabetes and proposed frameworks for assessing need in diabetes. Of the 58 articles, 23 of these (40%) did not address needs for health and focused solely on health care needs (see Tables 1-4). The following sections detail the main tools as well as including a summary table highlighting if both health care needs and needs for health are assessed and which specific needs for health are included.
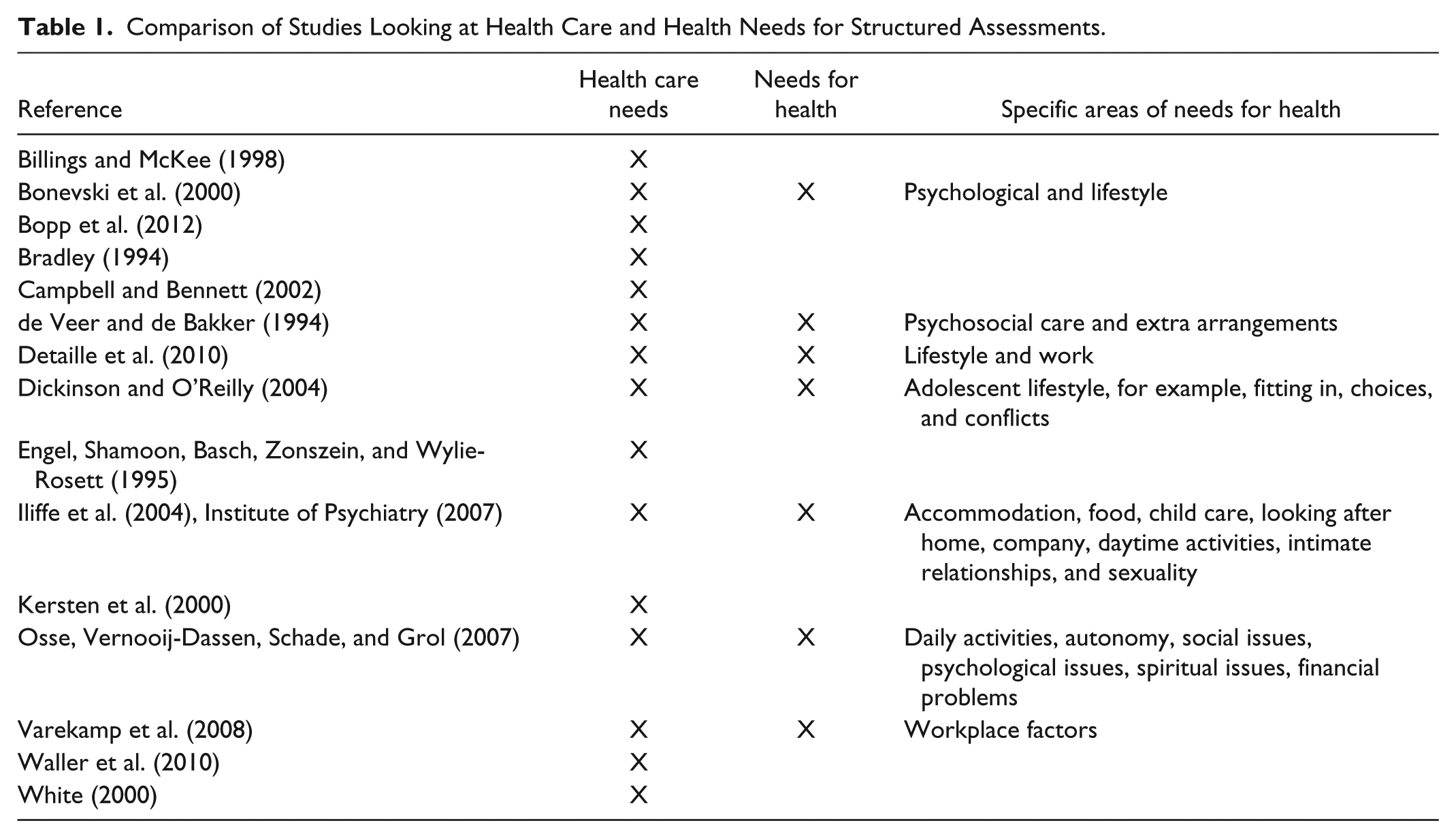
Comparison of Studies Looking at Health Care and Health Needs for Structured Assessments.
Comparison of Studies Looking at Health Care and Health Needs for Studies Comparing Needs Identified by Patients and Those by Health Care Workers.
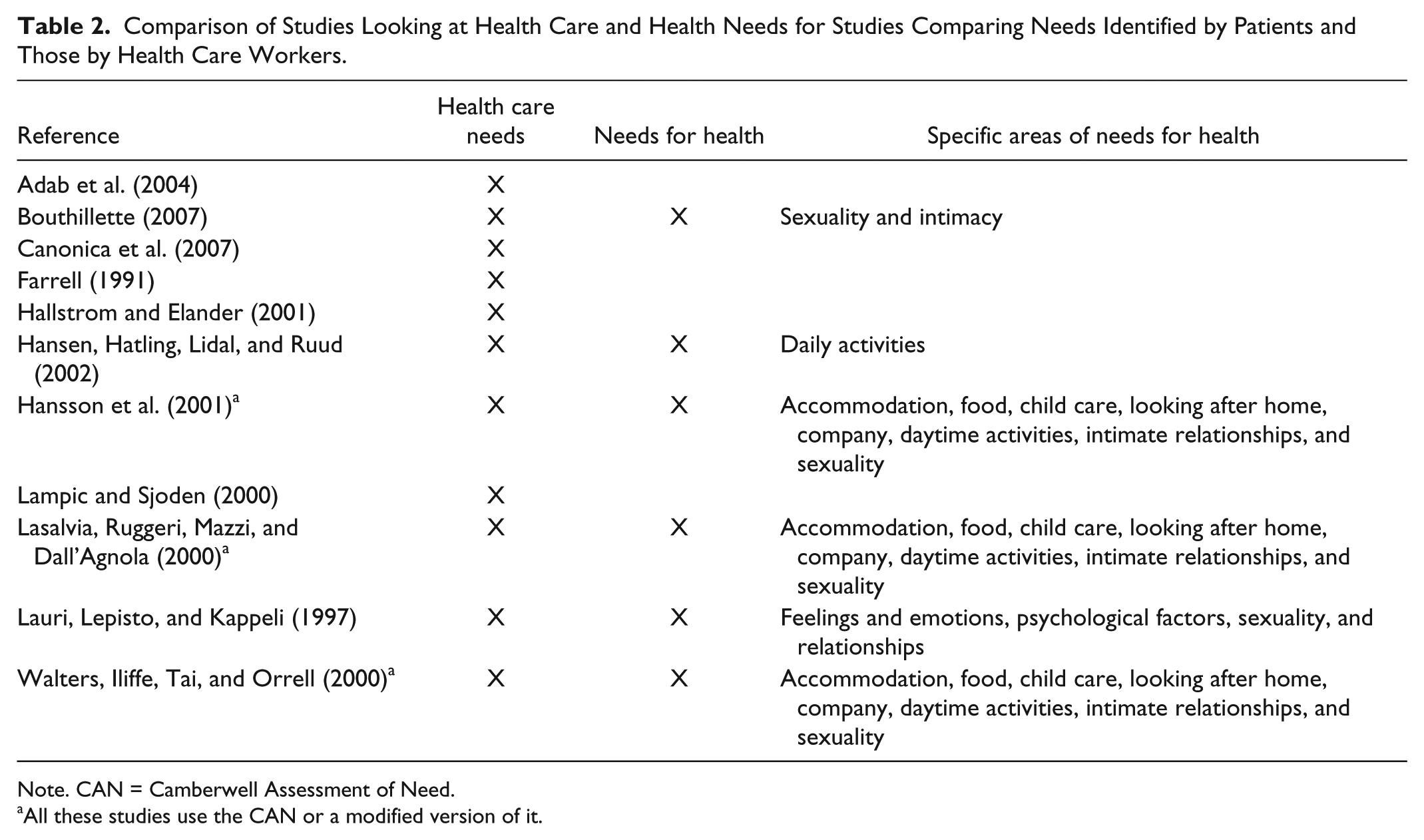
Note. CAN = Camberwell Assessment of Need.
All these studies use the CAN or a modified version of it.
Comparison of Studies Looking at Health Care and Health Needs for Studies Using Needs Assessments as a Tool for Evaluation.

Comparison of Studies Looking at Health Care and Health Needs for Studies Taking a Descriptive Approach to Needs.
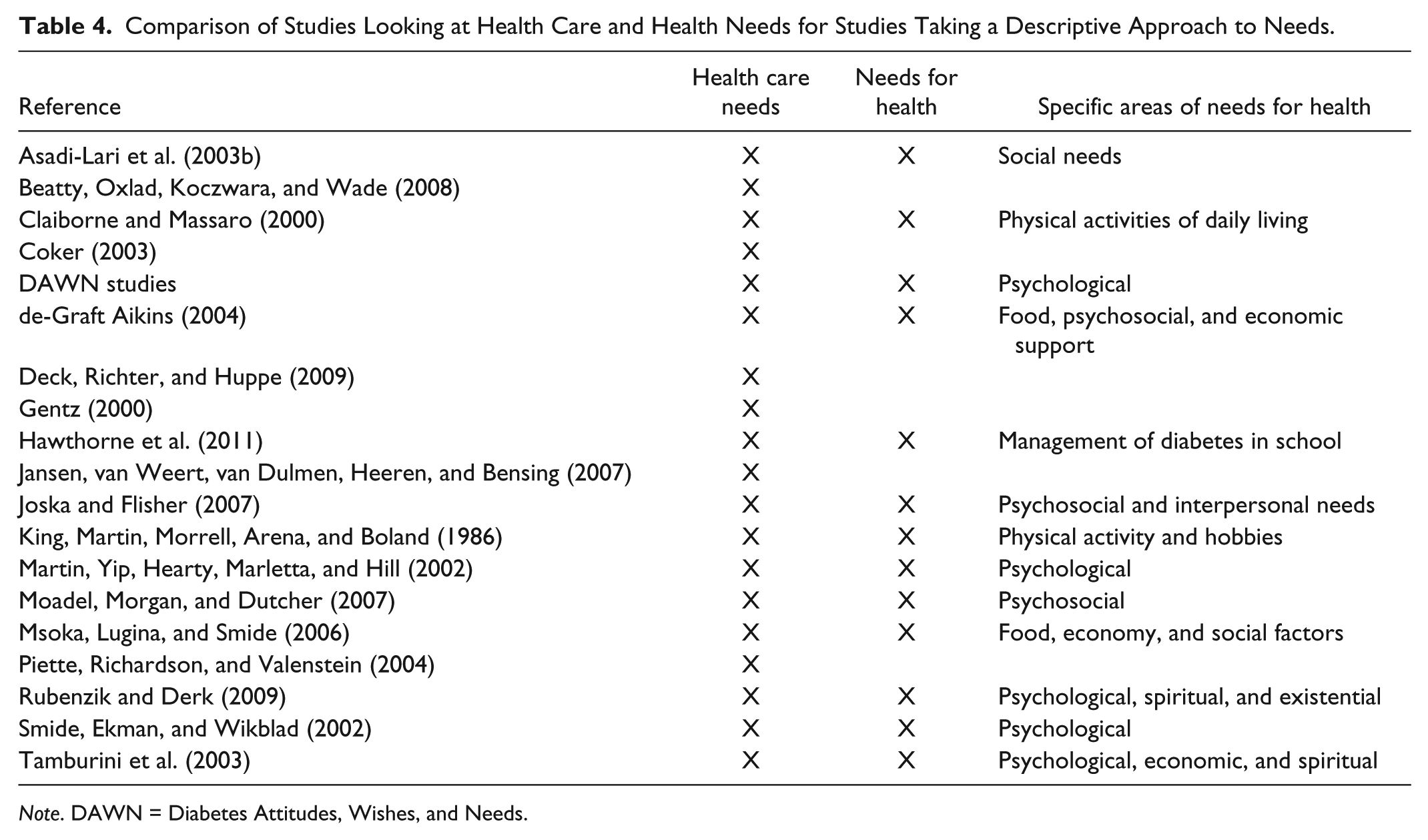
Note. DAWN = Diabetes Attitudes, Wishes, and Needs.
Standardized Tools
Specific tools such as the Camberwell Assessment of Need (CAN) have been developed to measure the health and social needs of people with mental health problems and have been used in various settings (Iliffe et al., 2004; Institute of Psychiatry, 2007). Specifically, for palliative care, the “Problems and Needs in Palliative Care” questionnaire assesses the needs of people and is used as a self-reporting questionnaire (Osse, Vernooij-Dassen, Schade, & Grol, 2007). It employs a checklist to help people identify their own needs and how and who should respond to these. This focuses on different areas of need such as daily activities, physical symptoms, autonomy, social issues, psychological issues, spiritual issues, financial problems, and other issues the individual may have. Another tool is the “Supportive Care Needs Survey” (Bonevski et al., 2000). This tool has as its aim to assess the needs of people with cancer. It looks at different types of needs psychological, health system, treatment, information, and impacts on lifestyle of cancer.
Standardized tools were also used to assess the needs of people with diabetes. These focused on specific subpopulations, for example, adolescent females who live with Type 1 diabetes (Dickinson & O’Reilly, 2004) or Hispanic patients in inner city New York (Engel, Shamoon, Basch, Zonszein, & Wylie-Rosett, 1995). Other tools identified were used in specific contexts such as assessing needs in clinical trials (Bradley, 1994) or identifying needs for a given patient during a given consultation (White, 2000). Another structured tool in diabetes, the Diabetes Patient Assessment Questionnaire (DPAQ) focuses on improving the care process by collecting subjective and objective data from the patients as well as carrying out an assessment of their needs (Campbell & Bennett, 2002). Table 1 summarizes the different tools included in this section as well as describing which needs they address.
Comparison Between Needs Defined by Individuals and Health Professionals
Different tools and studies were used to compare the needs of individuals, carers, and health professionals (Hallstrom & Elander, 2001; Hansson et al., 2001; Walters, Iliffe, Tai, & Orrell, 2000). Five out of 11 of these studies focus only on health care needs (Table 2). Many of these studies note that there are significant differences in the needs identified by professionals versus those seen as important by patients (Adab et al., 2004; Bouthillette, 2007; Canonica et al., 2007; Farrell, 1991; Hallstrom & Elander, 2001; Hansen, Hatling, Lidal, & Ruud, 2002; Lampic & Sjoden, 2000; Lasalvia, Ruggeri, Mazzi, & Dall’Agnola, 2000; Lauri, Lepisto, & Kappeli, 1997).
Tools for Evaluation
Poland, English, Thornton, and Owens (1970) define basic clinical needs of a hospital-based pediatric population as “dietary,” “vital signs,” “cleanliness,” “suction,” “oxygen therapy,” “toileting” and “turning.” Poland et al. (1970) argue that these needs should be used as a measure of hospital-based care rather than beds as each bed is occupied by a patient with very different needs depending on the reason for his or her admission.
Three studies use the CAN as tool for evaluation, one for psychiatric reform in Sweden (Arvidsson, 2003), another with regard to outreach programs in the United Kingdom (R. MacPherson, Gregory, Slade, & Foy, 2007), and a third looking at the link between meeting needs and Quality of Life (QoL) showing that unmet needs may not be a direct link to poor QoL, but rather act as an influence on this (Slade et al., 2004). Other approaches looked more at satisfaction of needs, looking to see if specific symptoms that children had were responded to appropriately by the health system (Liberatos, Elinson, Schaffzin, Packer, & Jessop, 2000), people’s expectations and satisfaction with health care workers (Bendtsen & Bjurulf, 1993), or if the consultation met people’s needs (Benett, 1994; J. Miller, 1982). Needs assessments for chronic diseases were also used by Chan and Griffiths (2009) and Rodriguez et al. (2006) to look at the needs of populations following natural disasters. It is interesting to note that the majority of these studies do not evaluate needs for health, but rather health care needs (Table 3).
Description of Needs
Other studies identified take a descriptive approach to the needs of people with different chronic diseases and diabetes. A study of ethnic minority needs in cancer care by Moadel, Morgan, and Dutcher (2007) looked at unmet needs, unmet psychosocial needs, and “unwanted needs.” “Unwanted needs” were those that did not fit with what individuals wanted and may have a negative impact. Needs for people with cancer have been identified such as emotional, physical, daily life, support, financial issues, information, and spiritual, but Moadel et al. state that it is unclear if they are applicable to the specific subpopulation they studied. This s of needs for health that these studies highlight range from economic support, food, and psychological as described in Table 4. In looking at health care needs, many studies focus on information needs, information on medicines, and their side effects (Beatty, Oxlad, Koczwara, & Wade, 2008; Coker, 2003; Jansen, van Weert, van Dulmen, Heeren, & Bensing, 2007; Tamburini et al., 2003). Gentz (2000), in a review, also describes those informational needs that include aspects such as understanding the actual procedure, anatomy and physiology, management of risk factors, changes in lifestyle, and use of medicines.
One of the key problems identified in tailoring the response to the needs of the individual was that health care workers are focused on treating the specific disease and do not address the patient as a whole (Asadi-Lari et al., 2003b; Brown, 1963). This issue was highlighted in a variety of studies where the specific needs of the elderly were not taken into account (Deck, Richter, & Huppe, 2009; King, Martin, Morrell, Arena, & Boland, 1986). Other research shows that psychosocial/psychological needs are often not addressed with a few studies specifically looking at diabetes and depression (Claiborne & Massaro, 2000; Joska & Flisher, 2007; Martin, Yip, Hearty, Marletta, & Hill, 2002; Piette, Richardson, & Valenstein, 2004; Rubenzik & Derk, 2009).
Five studies looking at diabetes take different approaches to identify needs. Hawthorne et al. (2011) looked at children and their parents’ experience and how this should be used to inform practice. A cross-cultural assessment of need was conducted by Smide, Ekman, and Wikblad (2002) in Sweden and Tanzania with regard to different levels of satisfaction around different aspects of treatment in these two countries. Two studies looked at needs of people with diabetes in sub-Saharan Africa, Msoka, Lugina, and Smide (2006) identifying needs by looking at the quality of life of people with diabetes and those without diabetes in Tanzania and de-Graft Aikins (2004) in Ghana by taking a critical social-psychological approach. One of the largest needs assessments with regard to diabetes was the Diabetes Attitudes, Wishes, and Needs (DAWN) Study conceived and initiated by Novo Nordisk 1 (Alberti, 2002). The aim of the DAWN study was to increase the “understanding of the role psychosocial factors play with regards to diabetes outcomes” and to find ways to “improve the psychosocial management related to diabetes care” (Rubin, Peyrot, & Siminerio, 2006, p. 1257). It also had as its objectives to increase the understanding of patient perceptions surrounding diabetes and to identify the main psychosocial barriers and solutions to improve management of diabetes (Novo Nordisk, 2001). This study included 5,426 people with diabetes, 2,194 primary care provides, 556 specialists, and 1,122 nurses (specialist and general) from Australia, Poland, Denmark, France, Germany, India, Japan, Norway, Spain, Sweden, The Netherlands, United Kingdom, and United States (Novo Nordisk, 2001; Peyrot, 2008; Peyrot et al., 2006)
Frameworks for Assessing Need in Diabetes
In addition, for diabetes, specific frameworks with regard to need were developed. For example, in exploring the experiences of children with Type 1 diabetes, Miller (1999) finds that children’s descriptions could fall into the following themes and subthemes:
“Finding out”
“Daily discipline”
“Being normal”
“Good things”
“Bad things”
“Support”
Dickinson and O’Reilly (2004), in a study to gain insight into the lives of adolescent females with Type 1 diabetes, used Van Manen’s phenomenological framework, which aims to describe and interpret lived experiences. They analyzed five themes:
“Blending in with the adolescent culture”
“Standing out and being watched”
“Weighing the options and making choices”
“Being tethered to the system and to diabetes”
“Struggling with conflicts”
The Zuluaga–Raysmith model defines 10 basic needs for elderly people focusing on not only health issues but also living conditions (Zuluaga, 2000). This model defines 10 basic needs:
Physical health;
Mental, emotional, social, and spiritual health;
Income;
Accommodation;
Protection and security;
Knowledge;
Mobility;
Communication;
Self-development;
Need to make a contribution.
The model states that a deficit in any one of these may have a negative impact on well-being.
Coles (1996) describes three models of adjustment to diabetes in that the physiological needs concern the management of symptoms and everyday life, emotional needs relate to the distress level of the person with diabetes, social needs are linked to the person with diabetes’ relationships and interactions with others, and finally self-actualization with the ability to function effectively with diabetes. Using this model, Coles states that lower needs need to be met first before moving to higher needs.
In a study looking at what children with Type 1 diabetes know and want to know about their condition, Olsen Roper et al. (2009) found that six themes emerged from this study: “Care,” “Physiology,” “Consequences,” “Impact on the family,” “Experience at time of diagnosis,” and “Cure.” The care theme was divided into three subthemes with Physical, Emotional, and Ambiguous care. Physical care was the practical aspects of managing diabetes, such as insulin administration, diet, and on. Emotional care was linked to dealing with the emotional and psychological aspects of diabetes. The authors created the theme “Ambiguous care” for elements that could not be placed in the other two care subthemes. Physiology knowledge related to how the body worked, the impact of diabetes, and the science behind the disease. Consequences related to the short- and long-term complications of diabetes. Impact on the family related to how family members assisted children in the management of diabetes.
Conclusion
This review of the literature was by no means systematic but had as its aim to highlight the gap between tools used to assess health care needs versus needs for health. It found that a considerable portion of articles focused solely on health care needs. Many tools focused specifically on psychological or psychosocial needs. Different studies presented a variety of needs assessed from sexuality and intimacy to food, but only the CAN addressed a wide range of needs. A medical view of needs is taken and, in some instances, these studies were more “satisfaction surveys” or looking at the failings of guidelines or consultations than true assessments of needs. These tools developed for chronic diseases or diabetes are standardized and very specific and do not allow for a wide view or variation of needs for people at different disease stages and also in different contexts to be studied. The DAWN study focuses too much on psychological issues as well as not presenting its methodology in detail. Msoka et al. (2006) fail to combine both the wider issues and clinical aspects, whereas de-Graft Aikins (2004) and Zuluaga (2000) do the opposite with too much of a medical focus.
Osse, Vernooij-Dassen, de Vree, Schade, and Grol (2000), in a review of tools used to assess the needs of people with cancer and their families during palliative care, find that most tools developed failed to address all aspects palliative care and that these tools were often for research purposes and not adapted to the clinical setting. Wen and Gustafson (2004), in a review, find that the tools developed did not always look at the needs at the different stages of the person’s disease.
The focus of the MeSH term is on the population’s needs or the individuals’ to determine the proper level of services needed. The focus of the literature is still very much on medical interventions and not needs outside of the health system. For people with chronic conditions, these needs may be more important than what is provided by the health system. It is important in addressing the burden of chronic diseases to look beyond specific health system needs as most of the time the individual manages his or her condition falls outside of the realm of the health system (Beran, 2014). In parallel, nonmedical needs may affect clinical management and therefore the health system needs to be aware of these and be able to include this in the management of the individual to ensure good overall health.
The development of tools to assess the needs of patients often do not include the beneficiaries themselves and assess the needs that health care workers feel are important (Richardson, Sitzia, Brown, Medina, & Richardson, 2005). These assessments also fail to clearly define what they mean by need as all needs cannot be met by the health system, but in some cases it is important that the health care worker knows that this need is or is not met. Richardson et al. (2005) argue that needs assessments should be used
As a communication tool for the interaction between health care workers and their patients;
As an integral part care;
To identify patient needs;
To identify areas where patients want health care workers to focus on;
To reassess the given situation of a patient;
With a view that the outcomes should assist with clinical care;
For monitoring and evaluation.
To provide adequate care for chronic conditions, governments need to assess the health needs of their populations and this should include the social, financial, or cultural factors that can be potential barriers (Bobadilla, 1996; Kay, Bengoa, & Assal, 2006; World Health Organization [WHO], 2007). Needs are infinite, whereas resources for the health system are finite (Bobadilla, 1996), and therefore with increasing need and limited resources, there is a widening gap between what people need and what can be provided. With the increase in chronic diseases, these needs are also becoming more complex and also should be adapted to each individual (Beran, 2012, 2014). Therefore, as argued by McKee (1996), people managing health systems should identify the needs of users of the health system and find a way to prioritize these. Therefore, a wider approach to care is needed with an assessment of the individual’s needs as an integral part of the care process (Slade et al., 2004). Interventions would then take into account not only the clinical aspect of the illness but also all unmet needs the individual faces.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.