
Abstract
The present study aims to investigate the relationship between severity of late effects and subjective quality of life of childhood cancer survivors in different age brackets. The sample consisted of 147 cancer survivors (70 boys and 77 girls) aged 8 to 18 who were in remission 2 to 5 years. The analyses were carried out separately for younger (8-12 years) and older (13-19 years) age groups. Cancer survivors were asked to complete Minnesota–Minneapolis Quality of Life Instrument (MMQL) as well as other methods of measuring involvement in everyday life activities and parent–child interactions Social And Health Assessment (SAHA) were used. Severity of late effects was assessed on a 4-point scale in accordance with Common Terminology Criteria for Adverse Events v3.0. While severity of late effects correlated positively only with parental warmth in younger age bracket, there were many relationships between severity of late effects and quality of life in older age bracket. The difference between the two age brackets is explained by the fact that adolescents are able to assess the impact of the disease.
Introduction
Due to the remarkable advances in the research and treatment of cancer in children and adolescents, about 80% patients reach long-term remissions today (Koutecký, Kabíčková, & Starý, 2002; Ries et al., 2007), as compared with less than 30% of childhood cancer survivors in 1960s. Therefore, late effects of anticancer therapy and related quality of life of survivors came into focus of clinicians (Oeffinger & Robinson, 2007). Two thirds of childhood cancer survivors suffer from at least one chronic health problem, approximately half of which are serious or even life-threatening (Geenen et al., 2007; Hudson et al., 2009; Mladosievičová, Kaiserová, & Foltinová, 2007; Oeffinger et al., 2006). Only one third of survivors have no health problems.
Specific types of late effects on somatic health include physical damage (limb amputation, permanent alopecia), restriction of physical functions due to conservational surgeries (resection of affected bones and homograft replacements), chronic organ dysfunctions (heart, intestines, liver, kidneys, and urinary bladder), diseases occurring in adult age (cardiovascular problems and diabetes), impaired growth and other disorders of endocrine functions (particularly after radiotherapy [RT] of neurocranium or bone marrow transplantation), neurological disorders (pareses, plegias, polyneuropathies), dysfunctions of sensory organs (hearing loss, partial or complete loss of sight), and infertility. Extremely unfavorable effects of oncological treatment include secondary malignities. According to certain authors, the overall risk of incidence of these tumors in survivors is 2%, but in some specific types of malignities, it can be much higher (25%-30%; Mahajan & Jenney, 2004; Vlčková, 2011).
The most severe psychosocial effects of therapy include disorders of neurocognitive functions. Most often, the following areas are studied in association with anticancer therapy (radiotherapy and chemotherapy): verbal competences, verbal learning and memory, information processing speed, visual memory, spatial and psychomotor coordination, attention span and concentration, executive functions (Kepák et al., 2007). Learning difficulties and problems with memory and concentration can be also a consequence of absence from the school (Eiser et al., 2007). Cognitive difficulties tend to intensify with the lapse of time after treatment. Other serious consequences include social difficulties and problems forming close/intimate relations. The impaired social functioning may cause more distress than physical effects of the illness (Zebrack et al., 2004). About 12% of cancer survivors develop posttraumatic stress disorder (PTSD; Langeveld, Grootenhuis, Voute, & de Haan, 2004). In the long term, childhood cancer survivors may also have problems finding employment. The contributing factors include cognitive impairments and poor school performance, physical limitations, suboptimal social skills, and preconceptions on the part of some employers. Cancer survivors live with uncertainty over their future health, and worry about possible relapse of the disease and secondary tumors and about the limitations presented by late effects. They have to come to terms with a compromise in their physical and social functioning.
Quality of lives of cancer survivors is influenced not only by the presence and number of late effects of therapy but also by their severity. Studies on the relationship between severity of late effects and perceived quality of life are rather scarce and, what is more, they provide ambiguous results. For instance, Benesch et al. (2009) observed in survivors of medulloblastoma/ependymoma (median of time after therapy 56 months, range = 1-174) significant negative correlation only between neurological late effects and scores of Children Quality of Life Questionnaire KINDL. Meeske, Patel, Palmer, Nelson, and Parow (2007) studied 86 survivors aged 8 to 18 years (average time after therapy 7.8 years) and found out that fatigue and severe effects of therapy were associated with impaired physical functioning. On the contrary, Löf, Winiarski, Giesecke, Ljungman, and Forinder (2009) observed in 53 adult survivors of childhood SCT (stem cell transplantation) that adverse effects had none or limited impact on their health-related quality of life (HRQoL).
The relationship between severity of late effects of anticancer therapy and perceived quality of life are however affected also by other factors such as type of diagnosis, tumor localization, type of therapy, age at the time of therapy, time of therapy termination, and age of respondents at the time of completion of questionnaires (Skinner, Wallace, & Levitt, 2007). For instance, infertility significantly decreases perceived quality of life in adolescence and young adulthood, but not in childhood, as children usually cannot understand the consequences. Similarly, infertility does not have to influence quality of life of older adults who had already come to terms with it. Age of respondents can explain weak or no correlation between severity of effects and perceived quality of life reported by Löf et al. (2009), who performed a study with adult survivors.
The present study analyzes the relationships between severity of late effects of anticancer therapy and perceived quality of life in two brackets: children aged 8 to 12 years and adolescents aged 13 to 19 years. It was assumed that severity of late effects in children would be compensated by good physical functioning—as physical activities are extremely important for them (Langmeier, Langmeier, & Krejčířová, 1998)—and overall outlook on life. The assumption in adolescents was that, in addition to previously demonstrated relationship between severity of late effects and decreased physical functioning (Meeske et al., 2007) and cognitive functioning (Kepák et al., 2007), there would be negative correlation between severity of late effects and involvement in social relations and leisure time activities, forming intimate relations and body image, as these aspects of life are very important in adolescence (Brown & Larson, 2009; Connolly & McIsaac, 2009). The influence of severity of late effects on overall outlook on life was expected also in adolescents.
Method
Sample
The study sample consisted of 52 anticancer therapy survivors aged 8 to 12 years (M = 10.17, SD = 1.23; 29 girls, 23 boys) and 95 anticancer therapy survivors aged 13 to 19 let (M = 15.95, SD = 1.88; 48 girls, 47 boys). At the time of inquiry, younger respondents were in remission for 20 to 118 months (median = 37 months), having been diagnosed to have central nervous system (CNS) tumor (12 persons), leukemia (22 persons), and solid extracranial tumors (18 persons). Older respondents were in remission for 8 to 140 months (median = 40 months), having been diagnosed to suffer from CNS tumor (20 persons), leukemia (10 persons), and solid extracranial tumors (65 persons).
Instruments
Involvement in leisure time activities was measured by the Conventional Involvement scale taken from SAHA (Social and Health Assessment) questionnaire (Schwab-Stone et al., 1999; Weissberg et al., 1991). Children indicate frequency of individual activities on a 5-point scale (“How often in the week . . .? 0x, 1x, 2x-3x, 4x-5x, 6x-7x; scale range = 0-4). Total involvement in afterschool and leisure activities is expressed as the mean score.
Interactions between parents and children (parenting aspects) were measured using the Parent–Child Interactions Scale, again from SAHA questionnaire, that determines four aspects of parenting—parental involvement (Cronbach’s α = .598), parental warmth (Cronbach’s α = .649), parental control (Cronbach’s α = .705) and inconsistency of parenting (Cronbach’s α = .560. Children assess parents’ behavior on a 4-point scale (never, rarely, sometimes, often; 1-4). Level of individual parenting aspects is again expressed as the mean score.
Other domains of QoL were assessed using the Minneapolis–Manchester Quality of Life Instrument (Bhatia et al., 2002; Bhatia et al., 2004) that was designed specially for children who underwent anticancer treatment. The questionnaire has two forms, the youth form (8-12 years) and the adolescent form (13-20 years).
The youth form includes the following domains of QoL: physical symptoms (e.g., headaches, Cronbach’s α = .667, range of scale = 1-4), physical functioning (e.g., have a lot of energy, Cronbach’s α = .761, range of scale = 1-4), psychological functioning (e.g., feeling sad, Cronbach’s α = .620, range of scale = 1-5) and outlook on life (e.g., happy with the way things are, Cronbach’s α = .782, range of scale = 1-4). The adolescent form evaluates the following domains of QoL (range of scales = 1-5): physical functioning (Cronbach’s α = .802), cognitive functioning (Cronbach’s α = .812), psychological functioning (Cronbach’s α = .665), social functioning (Cronbach’s α = .856), intimate relations (Cronbach’s α = .736), body image (Cronbach’s α = .831) and outlook on life (life satisfaction, Cronbach’s α = .843).
Severity of effects was measured using a 4-point scale (0 = none, 1 = less severe, 2 = moderately severe, 3 = highly severe). Late effects were assessed by a physician on the date of investigation using appropriate medical records. Individual late effects and their combinations were evaluated in accordance with Common Terminology Criteria for Adverse Events v3.0 1 (CTCAE). The resulting degree of severity was established according to the most severe late effect recorded.
Methods of Analysis
The relationship between late effects of anticancer therapy and perceived quality of life was assessed by correlation analysis: Spearman’s rank correlation coefficient was used due to ordinal nature of variable reflecting the severity of effects.
Results
Descriptive data about severity of late effects of therapy in dependence on patient’s age and type of diagnosis are stated in Table 1.
Frequency of Severity of Late Effects of Therapy According to Age and Type of Diagnosis.

Note. Table 1 states numbers of respondents and row percentages.
Table 1 demonstrates that overall severity of effects was slightly lower in children aged 8 to 12 years than in adolescents aged 13 to 19 years. This may be influenced by higher incidence of extracranial solid tumors and lower incidence of leukemia in adolescents as compared with younger respondents (Tables 2 and 3).
Relationships Between Psychosocial Characteristics and Severity of Effects of Anticancer Therapy—Children.

Note. MMQL = Minnesota–Minneapolis Quality of Life Instrument.
5% level of significance.
Relationships Between Psychosocial Characteristics and Severity of Effects of Anticancer Therapy—Adolescents.
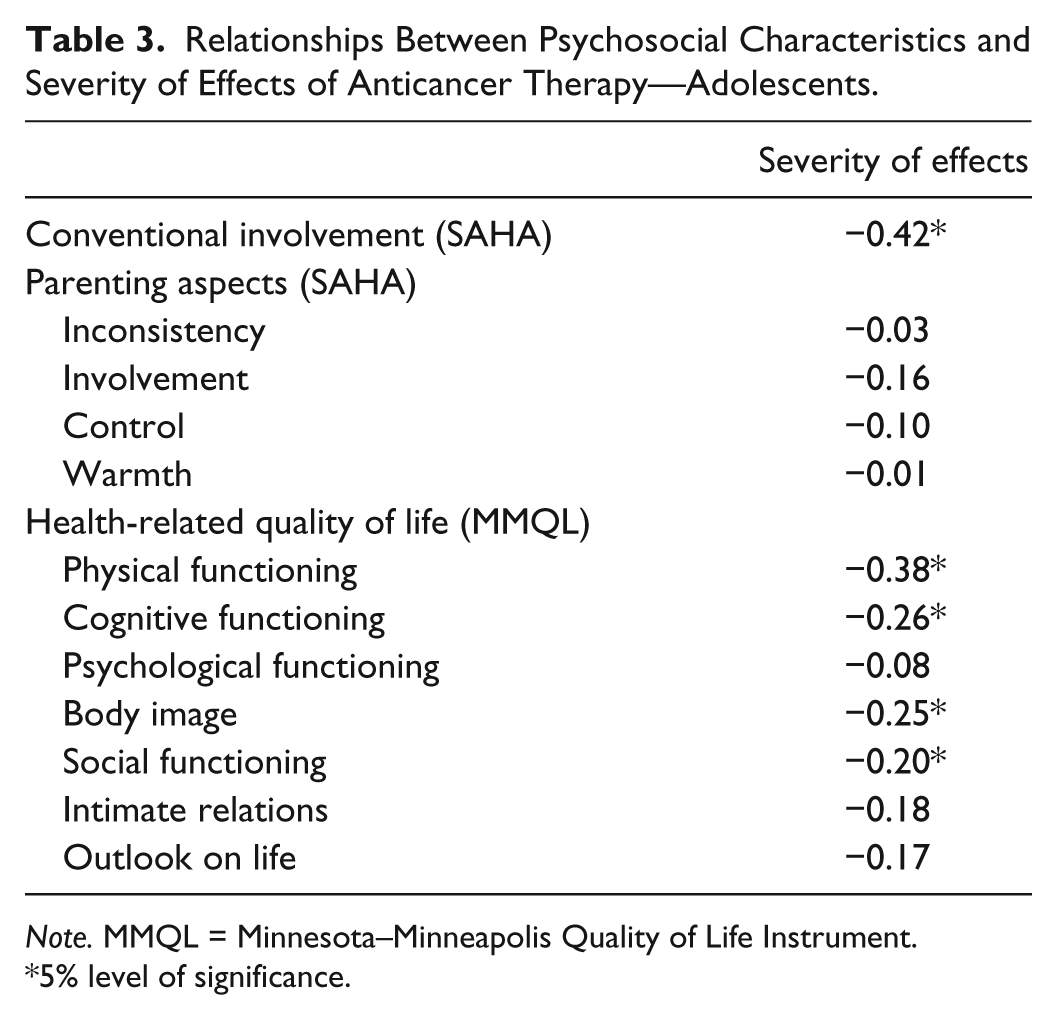
Note. MMQL = Minnesota–Minneapolis Quality of Life Instrument.
5% level of significance.
In children, severity of late effects of therapy is correlated only with perceived parental warmth. Physical functioning, psychological (emotional) functioning, and overall outlook on life decrease with higher severity of late effects; this relationship however is not statistically significant. In adolescents, severity of late effects of therapy is associated with many aspects of perceived quality of life. Severity of late effects correlates negatively with cognitive functioning, physical and social functioning, and body image. Overall outlook on life and satisfaction with intimate relations decreases in adolescents with higher severity of late effect of therapy. Nevertheless, these relationships were not statistically significant.
Discussion
The incidence of late effects of anticancer therapy observed in the present study sample corresponds with many studies that identified certain late effect in up to 70% survivors (e.g., Blaauwbroek et al., 2007; Lackner et al., 2000). It was also proved that the most severe late effects are found in survivors of CNS tumors, whereas the least severe effects are seen in patients with history of leukemia.
It was assumed that severity of late effects of therapy in various age categories would correlate with different aspects of perceived quality of life. However, only a part of this hypothesis was confirmed. As expected, more relationships between severity of late effects and perceived quality of life were observed in adolescents. Although the anticipated relationships were found in younger bracket as well, they were not statistically significant—this was namely the relationship between severity of late effects and decreased physical and psychological functioning and pessimistic outlook on life.
The only statistically significant relationship between severity of late effects of therapy and perceived quality of life in children was the correlation between severity of late effects and parental warmth: The severer the effects, the more the parental warmth. This relationship could explain the absence of other statistically significant correlations between perceived quality of life and severity of late effects of therapy: Parental warmth can compensate for children’s handicaps resulting from the consequences of therapy.
In fact, more relationships between late effects severity and perceived quality of life were found in adolescents. This might be due to the fact, that they took an adult attitude about their disease, were fully aware of its effects, and could anticipate future consequences. In accordance with other authors, the present study indicated that severity of late effects reduced perceived quality of life in the area of physical and cognitive functioning (Meeske et al., 2007; Mulhern et al., 2004). The results of this study suggest that severity of effects negatively influences also involvement in leisure time activities, social functioning, and body image. This is perhaps because adolescents (aged 13-19 years; 15.95 years on average) consider physical appearance and conventional involvement as key domains of their lives (Lerner & Steinberg, 2009). Moreover, adolescents showed negative relationships between severity of late effects and outlook on life and satisfaction with intimate relations. These relationships were however statistically insignificant.
The results of the present study confirm the hypothesis that severity of late effects of anticancer therapy should be studied in relation to not only specific diagnosis, tumor localization, type of therapy, and age of patients at the time of therapy but also age of respondents at the time of inquiry. Actually, criteria of perceived quality life as well as domains that are most affected by the consequences of anticancer therapy can change with time.
Limitations
This study has typical limitations of inquiries based on self-report data. However, as it studies quality of life, it has to work with such data. This study is also limited by uneven distribution of diagnoses in the sample, as adolescent survivors of CNS tumors and leukemia are not represented sufficiently. Hence, possible interaction between severity of therapy effects and the type of diagnosis and their overall impact on perceived quality of life could not be analyzed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the Czech Science Foundation (Grant No. P407/11/2421) and Czech Republic’s support for long-term strategic development of research organization (RVO: 68081740).