
Abstract
With the accelerating aging of the population, the accessibility of healthcare services has become a critical factor affecting the quality of life of older adults. Based on data from the 2018 Chinese Longitudinal Healthy Longevity Survey, this study analyzes 12,115 older adults (Mean = 84.27 years old, Standard Deviation = 11.38), using coefficient clustering method to quantify the impact effects and their magnitudes. This study explores the effect strength of opportunities for older adults to access, obtain, and utilize healthcare services on their quality of life, as well as the age differences in these effects. The empirical results show that: (1) Both subjective and objective healthcare accessibility significantly improve older adults’ quality of life, with subjective accessibility consistently showing stronger effects across age groups (60–69, 70–79, 80–89, and ≥90 years old). (2) Among different age groups, The effect strength of subjective healthcare accessibility shows a first Increase and then decrease trend, while the effect strength of objective healthcare accessibility gradually decrease. (3) The disparity in effect size between the two types of healthcare accessibility further widens among the oldest age groups, increasing from 1.1 to 4.1 times, this suggests that for the oldest-old, there is a greater emphasis on shifting healthcare service resources from “passive accessibility” to “proactive service.” The findings provide empirical evidence for the development of age-stratified healthcare service policies, they contribute to more precisely addressing the diverse healthcare needs of older adults in China and other developing countries, thereby effectively enhancing their quality of life.
Plain Language Summary
As older adults age, their ability to conveniently access healthcare directly affects their quality of life. Based on data from a large-scale survey, this study analyzes how subjective healthcare accessibility (how convenient older adults feel it is to get medical care) and objective healthcare accessibility (the actual availability of medical resources) impact the quality of life of older adults across different age groups. The results show that older adults’ perceived convenience has a greater effect on their quality of life, with this effect first Increase and then decrease as age advances. Meanwhile, the impact of actual medical resource availability gradually decrease with age. For the oldest-old, the gap between perceived and actual accessibility widens, indicating a greater need for proactive healthcare services rather than passive waiting. The findings highlight the importance of understanding both subjective and objective healthcare accessibility in influencing older adults’ quality of life, and suggest that healthcare policies should be tailored to the needs of different age groups to provide more appropriate services and improve their well-being.
Keywords
Introduction
As China enters a stage of deep and even severe aging, the demand for healthcare services among older adults continues to grow. The National Health Commission predicts that by 2035, the population aged 60 and above will exceed 400 million, accounting for more than 30% of the total population (Wei et al., 2019). By around 2050, the aging population is expected to reach its peak, with approximately 75% of older adults suffering from at least one chronic disease (Zeng et al., 2024), indicating a high disease burden among the elderly. Against the backdrop of chronic diseases becoming the main health threat to the elderly, it is necessary to establish an efficient integrated healthcare service system to improve healthcare accessibility. Healthcare accessibility not only affects whether older adults can obtain timely health services but also relates to accurately reducing disease burden and lowering the severity of chronic illnesses, thereby enhancing quality of life globally and promoting healthy aging.
Measuring the quality of life of older adults has become an increasingly urgent task. With the acceleration of population aging and the extension of life expectancy, older adults face more severe physical and psychological functional decline (Maresova et al., 2019; Saavedra et al., 2023). The prevalence and incidence of diseases among the elderly continue to rise, leading to significantly heightened demands for medical and health services within this population. Particularly in low- and middle-income countries, healthcare accessibility remains a major challenge (Alijanzadeh et al., 2024). Healthcare accessibility generally encompasses dimensions such as service quality, geographic accessibility, economic affordability, and acceptability of services (Peters et al., 2008). Previous studies have demonstrated a close relationship among healthcare expenditure, demographic aging, and disease burden (Howdon & Rice, 2018). Inadequate healthcare provision has been associated with increased risk of depression among older adults (Stein et al., 2019) and even elevated mortality risk (Lindström et al., 2020). Furthermore, older adults with functional impairments exhibit more pronounced needs for long-term care, and systematic care plans have been shown to effectively improve their well-being and emotional states (Chang et al., 2024; Rahman et al., 2022). Therefore, the accessibility and quality of healthcare services directly influence the quality of life of older adults. The quality of life in this population is considered a multidimensional, subjective, and value-driven construct, serving as a critical criterion for evaluating the effectiveness of long-term care services (Soosova, 2016). To safeguard the health and well-being of older adults, it is essential to provide high-quality, comprehensive, and person-centered healthcare services (Makai et al., 2014). Simultaneously, optimizing the allocation of healthcare resources to ensure equitable access to medical services for the older adults of different age groups is imperative.
However, in the context of limited resources, which types of healthcare services are most critical for improving the quality of life of older adults? How can healthcare resource supply be scientifically assessed and matched to demand? These questions remain prominent challenges in policy-making and practical interventions. Therefore, this study further distinguishes between the subjective and objective dimensions of healthcare accessibility to explore their relative impacts on the quality of life of older adults across different age groups. The innovations of this research are threefold: (1) It reveals the differential effects of various healthcare accessibility dimensions on older adults’ quality of life from a dual subjective-objective perspective. (2) It provides evidence-based policy recommendations and targeted service models based on empirical data from China that are applicable to China and other developing countries. (3) It responds to the core issue of “improving healthcare accessibility” within the global healthy aging strategy.
Theoretical Framework
Quality of Life of Older Adults
The quality of life is an increasingly important concept in aging research. The World Health Organization’s Quality of Life Group adopts a multidimensional and holistic approach, emphasizing subjective perceptions and cultural contexts, defining Quality of Life as “an individual’s perception of their position in life within the context of the culture and value systems in which they live, and in relation to their goals, expectations, standards, and concerns” (Haraldstad et al., 2019; Makai et al., 2014). However, the different dimensions defining the quality of life of older adults not only overlap but also interact with each other, reflecting its complexity and multidimensionality. According to existing studies, the quality of life of older adults can be summarized by three key attributes.
An individual’s subjective evaluation of their own living conditions. This includes self-assessments of satisfaction and well-being across various aspects of life, based on personal perceptions, emotions, and values.
An individual’s perception of others’ evaluations of their life satisfaction. This refers to how individuals assess their physiological, psychological, and social well-being based on feedback and behaviors from others, involving content related to these three domains.
An individual’s objective evaluation of their quality of life and related factors. This includes objective assessments of physical health (such as bodily functions and health status), mental health (including emotions, sense of achievement, and fulfillment), and social relationships (such as social support, friendships, and sense of belonging). It also encompasses important external factors affecting quality of life, such as housing conditions and economic status.
The quality of life of older adults is influenced by many age-related normative conditions and other factors—ranging from changes in health status to coping with new life limitations, as well as redefining new roles, opportunities, and available social support (Soosova, 2016). Previous studies have identified demographic variables (age, gender, and ethnicity; Campos et al., 2014), socioeconomic status (education level, income, social support; Henriques et al., 2020), health factors (disease conditions, functional status, healthcare services; Crocker et al., 2019), and personal characteristics (stress coping and self-efficacy; Bagheri et al., 2022; Shaabani et al., 2017) as key determinants of quality of life. For older adults residing in long-term care facilities or nursing homes, the provision of care needs and psychological intervention programs, as well as reliance on others to improve health status, have systematic effects on quality of life (Shin & Park, 2017; Van Malderen et al., 2013). It has been found that most studies measure the quality of life of older adults through fragmented factors, with relatively few focusing on healthcare accessibility as a core factor influencing their quality of life.
Healthcare Accessibility and the Quality of Life of Older Adults
Insufficient utilization of healthcare services has long been a significant global public health and policy issue. In response, academia has conducted in-depth explorations of healthcare accessibility from multiple dimensions. According to existing research, the understanding of healthcare accessibility is mainly explained from different perspectives such as spatial factors, agency, opportunities, and both supply and demand sides.
From the spatial perspective, X. Wang et al. (2018) proposed measuring the accessibility of primary healthcare based on indicators such as higher spatial accessibility, shorter travel time for medical visits, lower inequality, and more abundant primary healthcare resources (such as the number of beds, doctors, and health professionals).
From the perspective of agency and opportunity, Levesque et al. (2013) introduced a patient-centered concept of healthcare accessibility, emphasizing patients’ opportunities and abilities in seeking, obtaining, and utilizing healthcare services.
From the combined supply and demand perspective, Santana et al. (2023) defined supply-side accessibility as factors including the distance to healthcare facilities, waiting time, service content, and physician attitude; demand-side accessibility includes factors such as individual economic status, illness conditions, and self-rated health status.
Research on healthcare accessibility has shown significant associations with the health, well-being, life satisfaction, life expectancy, and quality of life of older adults. Community care services can substantially improve both the objective and subjective health and well-being of the elderly. Specifically, daily living care positively impacts physical health, healthcare services significantly enhance well-being, and recreational and spiritual services markedly increase both objective and subjective health scores, meeting basic material as well as higher-level spiritual needs (King et al., 2012; Mah et al., 2021; W. Ma & Shen, 2023). Healthcare services help prevent physical health decline and alleviate feelings of loneliness among older adults. The provision of medical services at home by trained healthcare professionals allows older adults to enjoy better overall health, further improving their quality of life (Papachristou et al., 2023; X. Zhao et al., 2020). Access to healthcare services—including online healthcare, virtual care, and consultations with medical specialists—also influences older adults’ self-reported mental health and behavioral changes (von Humboldt et al., 2022). Regarding the equity of healthcare services for older adults, significant differences exist in healthcare accessibility between younger and older populations across 11 high-income countries. Continuity of family care and personalized care plans have positive effects on the well-being, health, and life satisfaction of older adults. Compared to older adults aged 60 to 79, those aged 80 and above exhibit lower dependency in instrumental activities of daily living (Hargreaves et al., 2015; Predebon et al., 2021). The adequacy of healthcare services received by older adults partially influences their life expectancy. Women aged 65 to 85 who receive sufficient healthcare experience a net increase in life expectancy of 6% to 8%, while the corresponding net increase for men is 10% to 14% (Hao et al., 2020). Healthcare accessibility significantly influences older adults’ health status, well-being, and quality of life across multiple dimensions, playing a prominent role in extending lifespan, enhancing life satisfaction, and meeting physical and psychological needs. Given the broad and profound impact of healthcare accessibility, it is essential to further consider it from both subjective and objective dimensions. Subjective accessibility emphasizes individuals’ perceptions and cognition regarding access to healthcare services, reflecting psychological and cognitive acceptance. Objective accessibility focuses on quantifiable real-world conditions such as distance, cost, and allocation of medical resources. The interaction and complementarity of these two dimensions hold important practical value for achieving healthcare equity and optimizing policy resource allocation.
The Present Study
In summary, a review of existing research on healthcare accessibility shows that most scholars define healthcare accessibility from the perspective of residents’ ease of obtaining medical services, considering factors such as economic, spatial, and temporal dimensions (Satinsky et al., 2019; X. Wang et al., 2018), the aspects of agency and opportunity (Levesque et al., 2013), and the supply and demand sides (Santana et al., 2023). Relevant studies have indicated that healthcare accessibility exerts varying degrees of influence on the health or well-being of older adults across different genders and ages (Mah et al., 2021), life satisfaction (Predebon et al., 2021), life expectancy (Hao et al., 2020), and quality of life (Papachristou et al., 2023). However, no studies have yet differentiated healthcare accessibility into subjective and objective dimensions to further explore how these two aspects impact the quality of life of older adults, and whether these effects vary across different age groups. Therefore, this study constructs a systematic analytical framework, as shown in Figure 1, aiming to provide a more comprehensive understanding of the quality of life among older adults. The following research hypotheses are proposed.

Research framework.
Research Design
Data Sources and Samples
This study uses data from the Chinese Longitudinal Healthy Longevity Survey, organized by the Center for Healthy Aging and Development Studies at Peking University. The survey employed a stratified sampling method and covered 23 provinces/municipalities/autonomous regions across China. The questionnaire included topics such as the elderly’s mental health, cognitive function, social participation, lifestyle habits, and family economic status. The survey results were adjusted with complex sampling weights to ensure good representativeness. This study’s data have undergone rigorous review and approval by the Peking University Ethics Committee. All participants were informed of the survey content and provided their consent. Additionally, the research process was conducted anonymously, with strict confidentiality maintained for participants’ personal information. This study selected the latest released 2018 Chinese Longitudinal Healthy Longevity Survey data for a cross-sectional analysis. A total of 15,874 older adults were surveyed through questionnaires. After removing outliers and missing values of core variables and performing data cleaning, older adults (≥60 years old) were selected as the study population, resulting in a final sample of 12,115 older adults for analysis.
Variable Measurement
Dependent Variable
The quality of life (QOL) of older adults serves as the dependent variable. It is an important concept in the fields of medicine, sociology, and psychology. Referring to the World Health Organization defines quality of life as: “Individual’s perception of his or her position in life in the context of the culture and value system where they live, and in relation to their goals, expectations, standards and concerns” (Haraldstad et al., 2019; Makai et al., 2014). This study measured the quality of life of older adults using the question “How do you rate your life at present?.” For research purposes, reverse coding was applied, with a continuous variable range from 1 to 5, where higher values indicate better quality of life for older adults.
Independent Variable
Referring to the research on healthcare accessibility by relevant scholars (Levesque et al., 2013), healthcare accessibility can be measured from the aspects of seeking healthcare services, obtaining healthcare resources, utilizing healthcare services, and the likelihood of actually receiving services that meet healthcare needs. The academic community mainly measures healthcare accessibility from two perspectives: “service utilization” and “degree of fit.” First, accessibility measurement based on the concept of “service utilization.”Andersen (1968) was the first to explicitly propose the concept of healthcare accessibility. From the perspective of service utilization, he divided accessibility into potential accessibility and realized accessibility, equal accessibility, and unequal accessibility, as well as high-efficiency and low-efficiency accessibility. Second, accessibility measurement constructed from the perspective of “degree of fit.” Building on Andersen’s work, Penchansky and Thomas (1981) further refined the concept by developing measurement dimensions based on the fit between services and customers, including service availability, accommodation, accessibility, affordability, and acceptability. In the context of mental healthcare utilization and access, these were further detailed into service availability, financial accessibility, service acceptability, and geographic accessibility (Satinsky et al., 2019). Therefore, this study distinguishes between two core independent variables for analysis: subjective healthcare accessibility and objective healthcare accessibility.
(2) Subjective healthcare accessibility. Referring to Cylus and Papanicolas (2015), subjective healthcare accessibility emphasizes an individual’s perception of whether healthcare services are available. It relates to real-world barriers in accessing medical services, quality of care, waiting times, and unmet needs. Subjective healthcare accessibility is measured through questionnaire items covering three aspects: timely treatment, preventive health checkups, and medical insurance coverage. First, the question “If you become seriously ill, can you get timely hospital treatment?” is coded as 0 for “No” and 1 for “Yes.” Second, the question “Do you undergo a routine physical examination once a year?” is coded as 0 for “No” and 1 for “Yes.” Third, for the question “Which social security and commercial insurance do you currently have?” those who do not participate in any of the following—public medical care, urban employee or resident medical insurance, new rural cooperative medical insurance, or commercial medical insurance—are coded as 0, participation in at least one is coded as 1. Exploratory factor analysis resulted in a cumulative variance contribution rate of 0.70, suggesting that the scale has a relatively stable structure and good representativeness. Accordingly, a continuous variable was generated by summing the item scores, with higher scores indicating a higher level of subjective accessibility to medical services among older adults.
(3) Objective healthcare accessibility. Referring to F. Wang (2012), who emphasizes the supply-side perspective of healthcare service provision, objective accessibility encompasses factors such as maximizing the coverage of healthcare facilities and minimizing the distance to medical institutions. In this study, objective healthcare accessibility is measured using three survey items: the distance from the respondent’s home to the nearest medical facility, and whether the community provides healthcare-related services. Specifically, the question “How far is the nearest medical facility from your home?” is coded as 1 for responses indicating a distance within 3 km, and 0 for distances exceeding 3 km. The question “Does your community provide door-to-door medical visits or medication delivery services for older adults?” is coded as 1 for “yes” and 0 for “no.” Similarly, the question “Does your community offer health education services for older adults?” is coded as 1 for “yes” and 0 for “no.” Exploratory factor analysis resulted in a cumulative variance contribution rate of 0.77, indicating that the scale has a stable structure and good representativeness. A continuous variable was created by summing the item scores, with higher scores reflecting a higher level of objective accessibility to medical services among older adults.
Control Variables
Referring to relevant factors influencing the quality of life among older adults (Soosova, 2016), this study includes the following control variables: First, demographic characteristics of older adults, including gender, place of residence, marital status, educational level, household economic status (with household annual income below the average indicating poorer economic conditions), and living arrangements. Second, Health-related behavior variables of older adults, including whether they exercise, smoke, drink alcohol, and whether they are enrolled in a retirement or pension system. Finally, the mean age of the older adults is 84.27 with a Standard Deviation of 11.38, and the age range is from 60 to 117 years. The age of the elderly was categorized into four groups of 60 to 69, 70 to 79, 80 to 89, and ≥90 years old according to the purpose of the study. The variable assignment and descriptive statistics, as shown in Table 1.
Variable Assignment and Descriptive Statistics.

Note. Continuous variables describe means and ranges of values.
Analytical Strategy
This study uses Stata 17.0 software for data processing and analysis. First, the overall goodness of fit of the statistical model is assessed, and Pearson correlation analysis is performed on the core variables (subjective and objective healthcare accessibility, quality of life) by different age groups. Second, the effect of subjective and objective healthcare accessibility on the quality of life of older adults across different age groups is tested. Third, a further analysis is conducted to compare the intensity of the impact of subjective and objective healthcare accessibility on the quality of life of older adults and to examine the age differences in this effect. Finally, age was included as a moderating variable, and no multicollinearity issues were detected. Robustness analysis was conducted with reference to relevant studies on moderating variables (L. Zhao, 2024). If the interaction terms between the independent variables (subjective and objective healthcare accessibility) and the moderating variable (age) have a significant effect on the dependent variable (quality of life of older adults) (p < .05), it indicates that the impact of subjective and objective healthcare accessibility on the quality of life of older adults shows age differences and has good robustness.
Using the coefficient clustering method (Li et al., 2017), this approach not only estimates the effect sizes but also allows for direct comparison of their magnitudes. In this study, it is applied to compare the strength and differences of the effects of subjective and objective healthcare accessibility on the quality of life of older adults. Specifically, the method obtains a set of bundled coefficients for a group of observed variables measuring latent variables through an iterative process. The principle of coefficient clustering is as follows:

In expression (1),


Expressions (2) and (3) are substituted into (1):

In expression (4), the bundled variables have been standardized during the iterative process, maintaining the equivalence between the latent variable equation and the observed variable equation. Coefficient bundling is performed on the two sets of explanatory variables—subjective and objective healthcare accessibility—resulting in a bundled coefficient estimated for each set. This allows for a direct comparison of the effect sizes of the two sets of independent variables on the dependent variable.
Empirical Results
Correlation Analysis
In the research model examining the impact of subjective and objective healthcare accessibility on the quality of life of older adults, structural relationships were tested using the maximum likelihood estimation method. The results indicate a good model fit: χ2 = 123.51, df = 9, χ2/df = 13.72, CFI = 0.93, TLI = 0.88, SRMR = 0.02, and RMSEA = 0.03. These model fit indices suggest that the proposed structural model fits the empirical data well. Additionally, Pearson correlation coefficients between older adults’ quality of life, subjective healthcare accessibility, and objective healthcare accessibility were calculated across different age groups (as detailed in Appendix 1, see Table A1), the results show that both subjective and objective healthcare accessibility are significantly and positively correlated with the quality of life of older adults (p < .05).
Effect Strength
As shown in Table 2, both subjective and objective healthcare accessibility were included in the analysis for older adults across different age groups, with control variables incorporated into all models (as detailed in Appendix 2, see Table B1). The results show that in Models 1, 3, 5, and 7, subjective healthcare accessibility has a significantly positive effect on the quality of life of older adults (p < .05). The strength of this effect increases progressively from the 60 to 69 age group to the 70 to 79 and 80 to 89 age groups, but diminishes in the ≥90 age group, hypothesis 1 is supported. In Models 2, 4, 6, and 8, objective healthcare accessibility also demonstrates a significant positive impact on the quality of life of older adults (p < .05). However, the magnitude of this effect gradually decrease from the 60 to 69 age group to the ≥90 age group, hypothesis 2 is supported.
Effect Strength of Subjective and Objective Healthcare Accessibility on the Quality of Life of Older Adults.
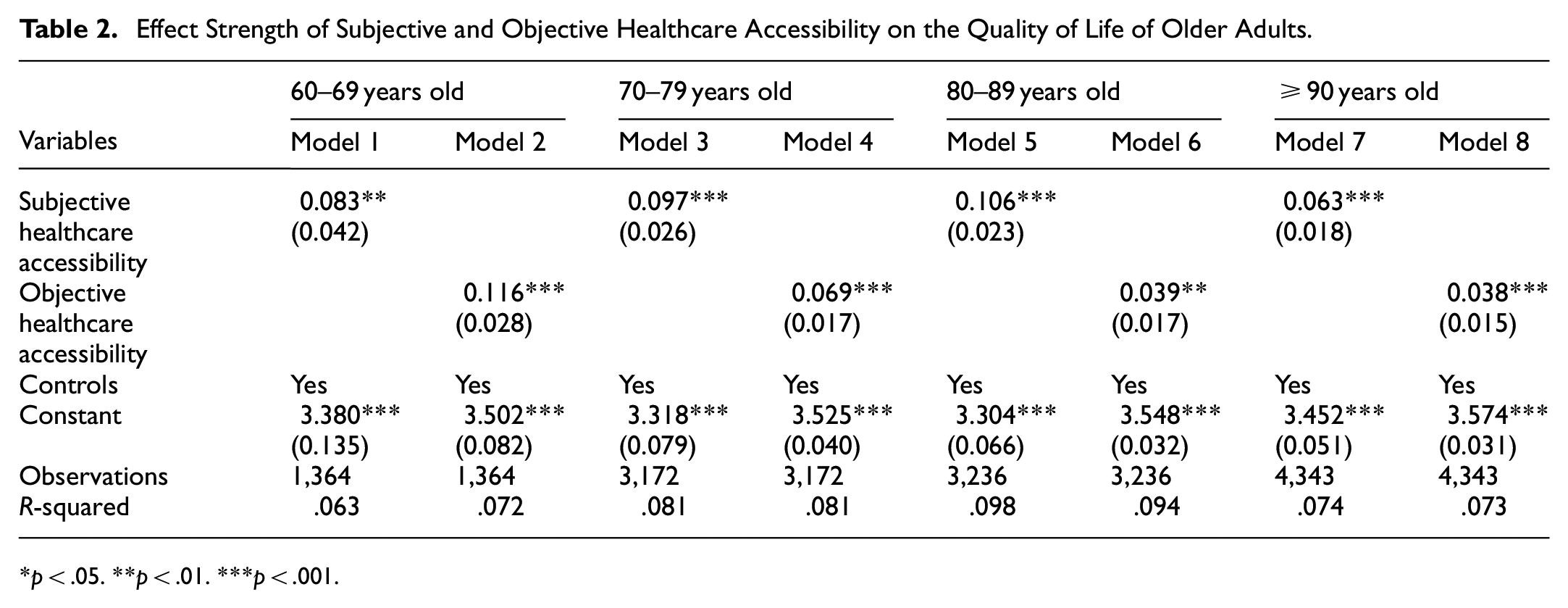
p < .05. **p < .01. ***p < .001.
As shown in Figure 2, the effect of subjective healthcare accessibility on the quality of life of older adults exhibits a first increase and then decrease, with a noticeable drop among the oldest-old (≥90 years old). This highlights a warning sign regarding the weakening effect of subjective perceptions in this age group, which may stem from issues such as cognitive decline, reduced mobility, and barriers to receiving information. Policy efforts should therefore focus on providing alternative services such as home visits, telemedicine, and community health outreach programs.

Effect strength of subjective and objective healthcare accessibility on quality of life.
In contrast, the effect of objective healthcare accessibility on quality of life gradually decrease with age, having the greatest impact on the younger elderly group (60–69 years old). This may be due to physical and mobility limitations in the oldest-old, which prevent them from fully utilizing available healthcare resources despite their objective presence. As a result, it is particularly important to develop proactive services for this age group, such as in-home medical visits and family doctor contracting, thereby shifting from “resource accessibility” to “proactive service delivery.”
Effect Size Comparison and Age Differences
Using the coefficient clustering method, this study estimates and compares the effect size of each sub-dimension of subjective and objective healthcare accessibility, aiming to assess the relative importance of these two types of accessibility in influencing the quality of life among older adults. As shown in Table 3, across all age groups, the effect size of subjective healthcare accessibility on quality of life is consistently stronger than that of objective healthcare accessibility (0.095 > 0.086, 0.110 > 0.045, 0.115 > 0.038, and 0.102 > 0.025), with all 95% Confidence Intervals excluding 0. This may suggest that as age increases, older adults place greater importance on emotional security and psychological support in healthcare services. As a result, perceptions such as “feeling convenient”“feeling respected” and “trusting the doctor” may have a greater influence on their healthcare behaviors and overall life experiences than physical distance or medical expenses.
Effect Strength Comparison of Subjective and Objective Healthcare Accessibility on Quality of Life.

p < .05. **p < .01. ***p < .001.
As shown in Figure 3, further visualizes the comparison of effect sizes of subjective and objective healthcare accessibility on the quality of life among older adults. The results indicate that the effect of subjective healthcare accessibility on older adults’ quality of life remains relatively stable at around 10% (ranging from 0.095 to 0.115), while the effect of objective healthcare accessibility on their quality of life gradually decrease (decreasing from 0.086 to 0.025). Comparing different age groups of older adults, from 60 to 69 years old to ≥90 years old, the difference in the effects of subjective and objective healthcare accessibility on quality of life progressively widens, with the ratios being 1.1, 2.4, 3.0 to 4.1 times, respectively, thus supporting Hypothesis 3. These findings suggest that healthcare resource planning should comprehensively consider both subjective and objective healthcare accessibility, and be tailored precisely to the actual needs of older adults across different age groups.

Effect size comparison of subjective and objective healthcare accessibility on quality of life.
Robustness Analysis
Grouping older adults by age may introduce potential bias. To address this, age was further included in the model as a continuous moderator variable instead of a grouped variable to conduct a robustness check. As shown in Table 4, in Models 9 and 11, both subjective and objective healthcare accessibility have significant positive effects on the quality of life of older adults, with the effect of subjective healthcare accessibility being stronger than that of objective healthcare accessibility (0.074 > 0.055). The 95% Confidence Intervals do not include 0, consistent with previous results. In Models 10 and 12, interactions between subjective and objective healthcare accessibility and age were tested. The coefficients of the interaction terms are both negative (β = −.003 and −.002), with 95% Confidence Intervals excluding 0, confirming the robustness of the age-related differences in the effects of subjective and objective healthcare accessibility on the quality of life of older adults.
Robustness Analysis.

p < .05. **p < .01. ***p < .001.
Discussion
Comparison with Previous Research Findings
With the increase in life expectancy, the demand among older adults for health and high-quality living is growing increasingly urgent. Meeting their subjective healthcare accessibility needs is closely linked to maintaining their physical health and improving their quality of life. This aligns with existing research that emphasizes the importance of improving treatment quality, reducing healthcare costs, and bringing healthcare services to people’s homes to enhance overall health and quality of life for older adults (W. Ma & Shen, 2023; Papachristou et al., 2023; X. Zhao et al., 2020). It can be inferred that ensuring both subjective and objective healthcare accessibility, as well as improving accessibility in terms of economy, time, and geographic factors, are key pathways to enhancing the quality of life for older adults and achieving healthy aging. Previous research has primarily focused on objective healthcare accessibility, such as the number of medical facilities, distribution of healthcare institutions, and the level of medical technology (Satinsky et al., 2019; X. Wang et al., 2018). This study is the first to incorporate subjective healthcare accessibility into the analysis framework and finds that its impact on the quality of life of older adults is generally stronger than that of objective healthcare accessibility across different age groups. This finding provides a new perspective for further exploring how different types of healthcare accessibility influence the quality of life of older adults.
Most studies treat the healthcare needs of different age groups equally, relatively overlooking that older adults typically have higher demand for medical services compared to younger adults. L. Ma et al. (2018) pointed out that there is a significant difference in healthcare needs between older and younger adults, showing that older adults require medical care 3 to 5 times more than younger people. Therefore, the impact of age differences on healthcare demand should be taken into account. This emphasizes the need to consider the impact of age on healthcare demand and to allocate medical resources and healthcare services based on age-specific needs. This study conducts an in-depth analysis of the comparative intensity of subjective and objective healthcare accessibility on the quality of life of older adults, revealing that, for different age groups, the impact of subjective healthcare accessibility remains relatively stable, while the impact of objective healthcare accessibility shows a declining trend. This finding highlights the differential effects of healthcare accessibility on older adults of different ages, providing a scientific basis for governments or relevant authorities to allocate healthcare resources and develop differentiated healthcare policies. The conclusions of this study are largely consistent with existing research, which has demonstrated that improving accessibility to healthcare services, providing continuous home care, and offering personalized care have positive effects on the healthy lifespan, well-being, and life satisfaction of older adults (≥65 years old; Hao et al., 2020; Predebon et al., 2021; Rodriguez-Blazquez et al., 2012). However, current studies have not further explored the differential effects among older adults of different age groups from a comparative perspective.
The study on the impact of healthcare accessibility on the quality of life of older adults expands academic understanding in this field and provides new empirical evidence. First, in terms of comparing the strength of the effects of subjective and objective healthcare accessibility on quality of life, subjective healthcare accessibility has a more stable impact. Older adults’ subjective perceptions of healthcare experiences and interactions (such as convenience of medical services and comfort of the healthcare environment) are likely to form stable healthcare habits and psychological expectations. Second, regarding the differences in the effects of subjective and objective healthcare accessibility on the quality of life of older adults across different age groups, as age increases, older adults’ physical functions gradually decline, and their reliance on the spatial distribution and utilization of healthcare resources grows. For younger elderly adults, convenience and comfort of medical services are more important, while for the older elderly population, they may be more focused on transitioning healthcare resources from “resource accessibility” to “active service.” Third, based on empirical research on China’s aging issue, for low- and middle-income countries, a tiered healthcare system can achieve a stepwise allocation of medical resources, bringing basic healthcare services to communities and rural areas to meet older adults’ demand for convenient medical services at a lower cost. For developed countries with a higher degree of aging, this approach provides new ideas for solving the challenge of transitioning older adults from “passive healthcare seeking” to “active health intervention.” These findings suggest that dynamically adjusting healthcare service supply strategies based on the characteristics of different age groups is an effective path to improving overall healthcare accessibility and the quality of life for older adults, which is worth considering and applying according to each country’s specific conditions.
Policy Implications
Firstly, healthcare accessibility has a significant positive effect on the quality of life of older adults. The government should attach great importance to the impact of healthcare accessibility on the quality of life of older adults, with particular attention to the fact that the effect size of subjective healthcare accessibility is generally stronger than that of objective healthcare accessibility. Relevant studies support strengthening the provision of community healthcare services and recreational mental health services, as well as offering adequate medical resources and personalized home care. These measures have a positive impact on the health, well-being, and life satisfaction of older adults (W. Ma & Shen, 2023; Predebon et al., 2021). Given the role of healthcare accessibility in improving older adults’ quality of life, efforts should be made to reinforce it at both institutional and service levels.
At the institutional level, strengthen the planning and enhancement of healthcare resources and optimize the structure of the primary healthcare system. Through policy guidance and financial subsidies, build a comprehensive healthcare system that integrates prevention, treatment, rehabilitation, and nursing care to improve institutional support capacity.
At the service level, emphasize the humanistic care in medical services and actively promote family doctor contract services and diversified health service models, such as developing smart healthcare services like “Internet + Healthcare,” to improve the convenience and experience of older adults in accessing medical care. Encourage medical institutions and healthcare workers to provide older adults with more equitable, high-quality, and efficient medical services, thereby comprehensively enhancing their physical and mental health.
Secondly, while improving the overall accessibility of healthcare services, differentiated healthcare policies should be developed to address the specific needs of older adults in different age groups. Relevant studies have focused on the complex processes and pathways between physical function, cognitive function, emotional function, and the quality of life of the oldest-old. It is important to increase healthcare institutions and facilities, encourage and maintain the functional activity capacity of older adults, and sustain their physical activity to enhance their quality of life (Munawar et al., 2024). To achieve a more effective support system, efforts should be advanced on both short term and long term levels.
In the short term, priority should be given to improving the medical emergency response system by establishing temporary community medical stations and deploying mobile medical service vehicles to quickly fill the gap of medical resources in remote areas, as well as establishing a dynamic health record updating system for older adults.
In the long term, systematic reforms of the healthcare service system are needed, with sustained increases in financial investment for the intelligent upgrading of primary healthcare facilities and the training of specialized geriatric care professionals. Promoting continuous innovation in medical insurance, developing a nationwide health perception monitoring system for older adults to achieve effective integration of medical insurance and long term care, thereby enhancing the health of older adults in a systematic and sustainable manner.
Finally, the government and relevant organizations should fully recognize that both subjective and objective healthcare accessibility have significant impacts on the quality of life of older adults, with notable differences across age groups and between urban and rural areas. Based on these differences, the health system should optimize resource allocation by improving community healthcare services in urban areas, prioritizing medical resources for rural regions, and narrowing the urban-rural gap through telemedicine and other approaches. At the same time, health administrators should establish a dynamic monitoring system for healthcare accessibility, regularly analyzing service utilization and perception among different groups to provide data support for policy-making. Ultimately, scientific and precise healthcare policies should be formulated to meet the objective needs of older adults, enhance their subjective satisfaction, and effectively ensure their quality of life. On this basis, further classification and targeted supply should be implemented according to the age characteristics of the older adult population.
For younger older adults, the focus should be on improving the convenience and accessibility of medical services by providing services centered around home care units and adult day care centers. These services can effectively delay functional decline, enhance their ability to live independently, and increase social participation, such as day care centers, rehabilitation centers, and social and recreational activity centers.
For the oldest older adults, more attention should be given to their psychological needs and emotional support. The emphasis should be on building services centered on continuous care, home visits, and health monitoring systems, with a focus on developing residential care and assistance service institutions for older adults, such as nursing homes, crisis intervention centers, and sheltered housing.
Strengths and Limitations
This study is based on a nationally representative dataset and analyzes the relationship between healthcare accessibility and the quality of life of older adults. Its main strength lies in a clever research design that quantitatively measures and distinguishes between subjective and objective healthcare accessibility. The study presents the effects of both subjective and objective healthcare accessibility on the quality of life of older adults, for the first time, innovatively compares the strength of these effects, and analyzes age differences. From the perspectives of subjective and objective healthcare accessibility, it provides a comprehensive assessment of older adults’ quality of life, offering empirical support for promoting healthy aging globally.
This study also has several limitations that need to be addressed in future research. First, it explores the impact of healthcare accessibility on the quality of life of older adults using cross-sectional data, which may lead to potential reverse causality—where lower quality of life affects access to healthcare. Future studies will adopt longitudinal or experimental designs to track and evaluate the quality of life of older adults, aiming to obtain more reliable conclusions. Second, the quality of life of older adults was primarily measured through self-reports, which may involve self-reporting bias and result in relatively low correlations between subjective/objective healthcare accessibility and quality of life. Future research will expand the use of proxy reports or weighted accessibility scores to build a more comprehensive index system for assessing the quality of life of older adults. Lastly, future studies should explore the underlying mechanisms through which healthcare accessibility affects health outcomes and quality of life among older adults. This should involve assessments at the macro-institutional, community support, and family microsystem levels to develop policy recommendations with a global perspective.
Conclusions
Both subjective and objective healthcare accessibility have significant positive effects on the quality of life of older adults. The study finds that the impact of subjective healthcare accessibility on the quality of life is consistently stronger than that of objective healthcare accessibility across different age groups, revealing the relatively greater importance of meeting older adults’ subjective healthcare accessibility needs.
For older adults of different age groups, the effect of subjective healthcare accessibility on quality of life first increases and then decrease, while the effect of objective healthcare accessibility gradually decrease. Furthermore, significant differences are found in the impacts of subjective and objective healthcare accessibility on the quality of life across different age groups.
For older adults aged 60 to 69, 70 to 79, 80 to 89, and ≥90 years old, the effect of subjective healthcare accessibility on quality of life remains relatively stable, while the effect of objective healthcare accessibility shows greater fluctuations. The ratio of the effects of subjective to objective healthcare accessibility gradually increases from 1.1, 2.4, 3.0 to 4.1 times across these age groups. This suggests that future longitudinal studies are needed to further confirm the causal pathways through which subjective and objective healthcare accessibility impact the quality of life of older adults, deepening the understanding of health support mechanisms for different age groups.
Footnotes
Appendix 1
The Correlation Coefficients Between Quality of Life and Subjective and Objective Healthcare Accessibility.

| Variables | 60–69 years old | 70–79 years old | ||||
|---|---|---|---|---|---|---|
| Subjective healthcare accessibility | Objective healthcare accessibility | Quality of life | Subjective healthcare accessibility | Objective healthcare accessibility | Quality of life | |
| Subjective healthcare accessibility | 1.000 | 1.000 | ||||
| Objective healthcare accessibility | 0.110** | 1.000 | 0.142** | 1.000 | ||
| Quality of life | 0.064*** | 0.110*** | 1.000 | 0.067*** | 0.069*** | 1.000 |
| 80–89 years old | ≥90 years old | |||||
| Subjective healthcare accessibility | 1.000 | 1.000 | ||||
| Objective healthcare accessibility | 0.120** | 1.000 | 0.103*** | 1.000 | ||
| Quality of life | 0.087*** | 0.046*** | 1.000 | 0.044*** | 0.035*** | 1.000 |
p < .05. **p < .01. ***p < .001.
Appendix 2
Effect Strength of Subjective and Objective Healthcare Accessibility on the Quality of Life of Older Adults.

| Variables | 60–69 years old | 70–79 years old | 80–89 years old | ≥90 years old | ||||
|---|---|---|---|---|---|---|---|---|
| Subjective healthcare accessibility | 0.083** (0.042) | 0.097*** (0.026) | 0.106*** (0.023) | 0.063*** (0.018) | ||||
| Objective healthcare accessibility | 0.116*** (0.028) | 0.069*** (0.017) | 0.039** (0.017) | 0.038*** (0.015) | ||||
| Gender | −0.033(0.061) | −0.032(0.060) | −0.085**(0.037) | −0.085**(0.037) | −0.012(0.034) | −0.006(0.034) | −0.070**(0.030) | −0.067**(0.030) |
| Residence | −0.085(0.068) | −0.093(0.068) | 0.008(0.044) | −0.004(0.044) | 0.118***(0.040) | 0.102**(0.040) | 0.150***(0.034) | 0.138***(0.034) |
| Marital status | 0.167**(0.068) | 0.176***(0.067) | 0.031(0.037) | 0.027(0.037) | −0.031(0.031) | −0.026(0.031) | −0.094***(0.036) | −0.086**(0.036) |
| Educational level | −0.004(0.007) | −0.005(0.007) | 0.006(0.004) | 0.006(0.004) | −0.008*(0.004) | −0.008*(0.004) | 0.001(0.004) | 0.001(0.004) |
| Household economy | 0.384***(0.058) | 0.382***(0.057) | 0.416***(0.035) | 0.420***(0.035) | 0.440***(0.034) | 0.448***(0.034) | 0.306***(0.029) | 0.310***(0.029) |
| Residence arrangements | −0.032(0.084) | −0.026(0.084) | 0.144***(0.044) | 0.151***(0.044) | 0.166***(0.033) | 0.164***(0.033) | 0.196***(0.029) | 0.193***(0.029) |
| Exercise | 0.147***(0.046) | 0.157***(0.046) | 0.152***(0.029) | 0.154***(0.029) | 0.179***(0.029) | 0.185***(0.029) | 0.184***(0.030) | 0.191***(0.030) |
| Alcohol | 0.095*(0.057) | 0.100*(0.057) | 0.007(0.035) | 0.010(0.035) | 0.019(0.035) | 0.018(0.035) | 0.040(0.031) | 0.040(0.031) |
| Cigarette smoking | −0.032(0.062) | −0.036(0.062) | 0.036(0.038) | 0.031(0.038) | 0.041(0.035) | 0.037(0.035) | 0.056*(0.031) | 0.054*(0.032) |
| Have departure or retirement system | 0.190***(0.067) | 0.190***(0.067) | 0.068(0.044) | 0.070(0.044) | 0.030(0.042) | 0.027(0.042) | 0.072*(0.038) | 0.068*(0.038) |
| Constant | 3.380***(0.135) | 3.502***(0.082) | 3.318***(0.079) | 3.525***(0.040) | 3.304***(0.066) | 3.548***(0.032) | 3.452***(0.051) | 3.574***(0.031) |
| Observations | 1,364 | 1,364 | 3,172 | 3,172 | 3,236 | 3,236 | 4,343 | 4,343 |
| R-squared | .063 | .072 | .081 | .081 | .098 | .094 | .074 | .073 |
p < .05. **p < .01. ***p < .001.
Acknowledgements
We thank the Center for Healthy Aging and Development Studies at Peking University for providing the data from Chinese Longitudinal Healthy Longevity Survey. We would also like to add our thanks to the blind peer reviewers for their helpful comments and advice on previous versions of this article. Finally, to editors of SAGE Open for their meticulous editing efforts and supports.
Data Sharing Statement
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Ethics Approval
The study protocol was reviewed and approved by the Institutional Accreditation Committee of the Peking University (CLHLS 1998-2018), and participants provided written informed consent to participate in this study.
Funding
This study was funded by Research on the influence mechanism and intervention of digital life interaction on the physical and mental health of older adults in Yunnan Province “” (QN 202553).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.