
Abstract
The purpose of this study is to investigate the Ferrans and Powers Quality of Life Index (QLI) and its domains in Brazilian athletes. The sample comprised 219 athletes from six sports, and included 127 men and 92 women, with mean age of 23.1 years (±5.2). All participants were associated with a sports organization and participated in official competitions at the professional, semiprofessional, and amateur levels, and completed a self-report demographics survey and the QLI during one testing session. Kruskal–Wallis and Mann–Whitney U tests were utilized to compare differences between competitive levels and gender, respectively. Significant differences were reported between professional and amateur athletes for the socioeconomic (p = .016; professional: 17.2, amateur: 15.1) and psychological/spiritual (p = .011; professional: 24.3, amateur: 21.9) domains and between genders on the family domain (p = .027; male: 21.8, female: 20.2). These findings suggest that professional athletes are more satisfied from a socioeconomic and psychological/spiritual perspective when compared with the amateur group. In addition, the results suggest that family issues are more satisfying and/or have less importance for males than for females. This study provides further insights into the quality of life of athletes and suggests differences based on competition levels and gender. Future studies are needed to further our understanding of the quality of life in athletes.
The quality of life is an important issue in contemporary society and is central to the development of social policy dedicated to individuals, small groups or society in general (Phillips, 2006). In a way, people have some intuitive idea of the quality of life meaning, but it can represent distinctive aspects and components to different people.
The concept of quality of life is eminently human, which has been approximated to the satisfaction in diverse aspects of life. It implies the ability to make a synthesis of all cultural elements that particular society considers their standard of comfort and well-being (Minayo, Hartz, & Buss, 2000). The term encompasses many meanings, which reflect knowledge, experience, and values of individuals and collectivities related to it in different times, diverse places and stories, thus being a social construct with the brand of civilizing relativity (Minayo et al., 2000).
Despite variations in the formal definition of quality of life (Cummins, 2005; Snyder et al., 2010; Walters, 2009), the general evaluation of quality of life involves the physical, material, social, and emotional well-being of a person as well as the activities and development of an individual (Pino, 2003). The aim of quality of life research is to analyze factors that are relevant in the daily lives of individuals, and to allow individuals to express their satisfaction or dissatisfaction with these important aspects of life (Ferrans & Powers, 2012). According to Bakas et al. (2012) there are considerable diverse models in the quality of life literature that have not been sufficiently tested or refined such as specific disease’s models that were not compared with global models like World Health Organization model, for example. Among the global models used to investigate quality of life, there is the method developed by Ferrans and Powers, who adopted the notion that “individuals are the only proper judge of their quality of life, because people differ in what they value,” which is known as an individualistic ideology (Ferrans, 1996, p. 293). For this reason, the individualistic approach presented in the concept of quality of life intends to investigate the individual and subjective aspect of quality of life, respecting the references of athletes in their given context. (Minayo et al., 2000).
There are very few studies that investigate quality of life in athletes, but these studies have appeared more frequently in recent years. Findings from the available literature suggest that athletes report better quality of life than nonathletes in some aspects of life such as physical functioning, general health perceptions, social functioning, and mental health (Snyder et al., 2010). In addition, it appears that the level of competition (competitive vs. amateur [Modolo, Mello, Gimenez, Tufik, & Antunes, 2009] and elite vs. nonelite [McAllister, Motamedi, Hame, Shapiro, & Dorey, 2001]) can also positively impact the quality of life of athletes. These findings suggest that frequency and volume of the sports practice and level of competition can impact the quality of life of an individual. Furthermore, findings also suggest that male athletes experience better quality of life than female athletes, particularly in emotional functioning (Tanabe, Snyder, Bay, & Mcleod, 2010).
Although these studies provide insight into the quality of life of athletes, there are several limitations in the current literature. First, it is unclear as to the most appropriate outcome measures for athletes and also for specified age groups. In the case of adolescents, for example, the authors of the Short Form-36 (SF-36) state that their instrument may not be the most appropriate for this age group (Medical Outcomes Trust, 2013). Due to differences between athletes and the general population (McAllister et al., 2001; Snyder et al., 2010), it is important to understand how different patient-rated outcome measures, such as Ferrans and Powers Quality of Life Index (QLI), perform in the athletic population. In addition, it is necessary to mention that in general, studies about the quality of life in athletes have focused on clinical practice implications, especially related to sports injuries (McAllister et al., 2001; Valovich Mcleod, Bay, Parsons, Sauers, & Snyder, 2009). The approach in these studies is very relevant for the advancement of science in this area. However, it is important that further studies contemplate other factors that also influence the quality of life including distinctive performance levels, in different sports, from diverse nationalities, with varied training conditions, from a distinct social and economic background. Consequently, there is a great difficulty in obtaining data allowing comparison between studies and deeper analysis of the results. Above all, it is necessary to recognize the perspective of the athletes, thus contributing to a broader understanding on the topic “quality of life in sports.” In this sense, there is much to be explored. Thus, the objective of this study is to investigate the QLI in Brazilian athletes. Specifically, we were interested in describing potential differences in quality of life based on competition level and gender. We hypothesized that different categories of athletes such as professionals, semiprofessionals, and amateurs have distinct levels of quality of life. Furthermore, we hypothesized that the differences will be reported when comparing male and female athletes based on QLI scores.
Materials and Method
This descriptive and exploratory study was conducted between February and November of 2011 in the cities of Barueri, Itapevi, Santo André, São Bernardo do Campo, São Caetano do Sul, and São Paulo, São Paulo State, Brazil. The study was approved by the institutional review board and received the permission of the management and technical staff in the institutions in which data were collected to adhere to research ethics procedures. The athletes who participated in the study received necessary explanations and stated in writing that they understood the objectives and procedures of the study and that they consented to participate in the study.
Sample
Athletes over the age of 18 were eligible to be part of the research if they were associated with a sports federation during the study period, and participated in any official competition in 2011. The sample consisted of 127 males aged between 18 and 51 years, with a mean age 22.9 (±5.3) years, and 92 females aged between 18 and 37 years, with a mean age of 23.4 (±4.9) years. In all, 219 individuals aged between 18 and 51 years, with a mean age 23.1 (±5.2) participated in the study. The sports that the participants in this study practice included athletics/track and field (e.g., vertical jumps, horizontal jumps, throws, sprints), basketball, handball, indoor soccer, judo, and karate. All athletes who had been invited to participate in the study responded to the questionnaires. However, two questionnaires were excluded from final analysis because they were incomplete.
Instruments
Self-report survey
A self-report survey was developed from an adaptation of the Pelé Law, Chapter III, Article 3 of the Federal Law No. 9615 of March 24, 1998 (Brazil, 1998). For this instrument, the athlete recorded their sport, age, gender, and his or her status as a professional, semiprofessional or amateur athlete according to the above legislation. The instrument used a simplified language using a dictionary of Portuguese synonyms and antonyms to ensure easy comprehension (Villar, 2008). It is noteworthy that the instrument does not assess whether the athletes are actually professional, semiprofessional or amateur athletes; it measures whether the athletes self-identified as professional, semiprofessional or amateur athletes. The instrument assessed each athlete’s situation at the time the data collection was performed. Athletes considered the below categories when describing their sports participation:
Professional: There is a written contract between the athlete and the institution where he or she practices, and the athlete receives a regular salary as an athlete who represent the institution.
Semiprofessional: There is a contract between the athlete and the institution where he or she practices, and the athlete receives incentives to represent the institution, however, does not consider these incentives to be a wage.
Amateur: The athlete is free to participate or not participate in competitions, and the athlete does not receive material incentives to represent the institution.
Ferrans and Powers QLI
The Portuguese version of QLI, which was validated by Kimura and Silva (2009), was utilized to measure quality of life. This instrument has been translated into various languages and is ready for used in a phrase structure syntax file via homepage (http://www.uic.edu/orgs/qli). Its psychometric properties have been measured in several studies (Bakas et al., 2012; Ferrans & Powers, 1985; Ferrans & Powers, 1992; Halabi, 2006; Oliveira & Santos, 2011; Rustoen, Wiklund, Hanestad, & Burckhardt, 1999).
The instrument was chosen for consistency between the theoretical concept of quality of life and the construction of the instrument itself, which was developed to evaluate quality of life depending on the levels of satisfaction and importance concerning diverse aspects of life (Kimura & Silva, 2009). Furthermore, according to Dantas, Sawada, and Malerbo (2003) QLI is one of the most commonly utilized generic quality of life instruments in Brazilian research. For example, the QLI has been used in healthy college students (Kawakame & Miyadahira, 2005) and in groups with specific health problems such as patients with wounds (Yamada & Gouveia, 2009) and chronic renal failure (Rudnicki, 2007).
The QLI comprised two parts. The first part concerns the satisfaction that the individual has with aspects of life. For example, in Part 1 there is the question “How satisfied are you with your health care?” and each item has six response options on a scale ranging from 6 (very satisfied) to 1 (very dissatisfied). In Part 2 there is the question “How important to you is your health care?” and this scale ranges from 6 (very important) to 1 (no importance). The score calculation weighs each satisfaction item with its corresponding item of importance, thus combining the values. Values are calculated by recording the scores given to satisfaction item and then subtracting the value of 3.5 from the response for each satisfaction item (Ferrans & Powers, 2012). Consequently, the values are −2.5, −1.5, −0.5, +0.5, +1.5, +2.5. Then, these values are multiplied by the raw answer regarding the importance (Part 2 of the survey), equaling 1, 2, 3, 4, 5, and 6, according to each corresponding item. The weighted values of all items are then summed, and divided by entire number of items answered to calculate the total score. This calculation yields values ranging from −15 to +15. Finally, the value 15 is added to these scores, so the lowest value that could be, that is −15 changes into 0 and all values become positive, which ensure a final variation from 0 (worse quality of life) to 30 (better quality of life) for the QLI.
The formula for calculating the QLI is the following:

Qi: Question i;
P1: Part 1 of the questionnaire;
P2: Part 2 of the questionnaire.
The QLI instrument groups the items in four domains, which can be calculated using the same process:
Health/functioning domain (QLIHEA), which includes factors like health, health care, pain, energy (fatigue), ability to take care of yourself without help, control over life, chances for living as long as you would like, sex life, ability to take care of family responsibilities, usefulness to others, worries, things for fun, chances for a happy future;
Socioeconomic domain (QLISOC), which includes factors like friends, emotional support from people other than your family, neighborhood, home, job/not having a job, education, financial needs;
Psychological/spiritual domain (QLIPSY) that includes factors like peace of mind, faith in god, achievement of personal goals, happiness in general, life satisfaction in general, personal appearance, self;
Family domain (QLIFAM) that includes factors like family health; children, family happiness, spouse, lover, or partner, emotional support from family;
Data Collection
Using the Internet, we searched for sports federations and institutions that participate in federation organized competitions. We then contacted the sport manager and coaches of each institution to facilitate athlete access. Coaches selected dates and times for data collection that did not interfere with training routines. We presented and explained the study to the athletes, and they were asked to complete the questionnaires during one testing session. We reiterated that all answers were confidential, and we encouraged the athletes to honestly complete the instruments. The athletes had unlimited time to complete the instruments, which usually took about 25 min. The athletes then deposited their completed instruments in a sealed box, designed to prevent identification.
Data Analysis
All data were recorded in a Microsoft® Office Excel 2007 (Microsoft Corp., Redmond, Washington), spreadsheet that coded individuals, sport, gender, age, category (professional, semiprofessional and amateur), and the QLI values. Data analysis was performed using the Statistical Package for Social Sciences for Windows released version 17.0 (SPSS Inc., Chicago) and BioStat 5.0 software (Microsoft Corp., Redmond, Washington), and the graphs were created in Excel 2010. Descriptive statistics were calculated to evaluate the frequency, mean, standard deviation, median, minimum, and maximum of the variables of interest. Quantitative data were presented as the mean and standard deviation. The information related to sports, gender, and category was presented as the frequency and percentage of occurrence in each class. The means of the quantitative variables were compared using the Kruskal–Wallis or Mann–Whitney test, because some variables lack normality. In cases with significant difference, the Student–Newman–Keuls test was used to identify where these differences occurred. We used the Bonferroni correction to reduce the risk of a Type I error. Values were considered significant only for p values below .017 for the variable category (α / [no. of comparisons] = 0.05 / 3).
Results
No differences were reported for subject demographics that are shown in Tables 1 and 2. QLI values are reported in Table 3 with socioeconomic domain reporting the lowest value and the psychological/spiritual domain reporting the highest values.
Summary Measures for the Age Variable by Gender.

Distribution of Participants by Category.

Descriptive Measures of the Variables of Quality of Life Index (QLI) and Its Domains.

Significant differences were reported for the socioeconomic and psychological/spiritual domains between competitive groups (Table 4). Specifically, amateur individuals had significantly lower socioeconomic values when compared with professional athletes (p = .004). No differences were reported for this domain when considering the group. Similarly, amateur athletes reported lower values on the psychological/spiritual domain when compared with professional athletes (p = .006) but these differences were not statistically significant. No other differences were reported for competition levels.
Descriptive Measures of the Quality of Life Index (QLI) Variables by Category.

Statistically significant.
For between-gender comparisons, only a statistically significant difference was reported for the QLI family domain with the male group reporting higher values compared with females (Table 5). The male group had higher absolute value compared with the female group in the health/functioning and psychological/spiritual domains, but in these two domains, the differences were not significant. Similarly, for the socioeconomic domain, the male group had a lower absolute value compared with the female group, but this difference was also not significant.
Descriptive Measures of the Quality of Life Index Variables by Gender.
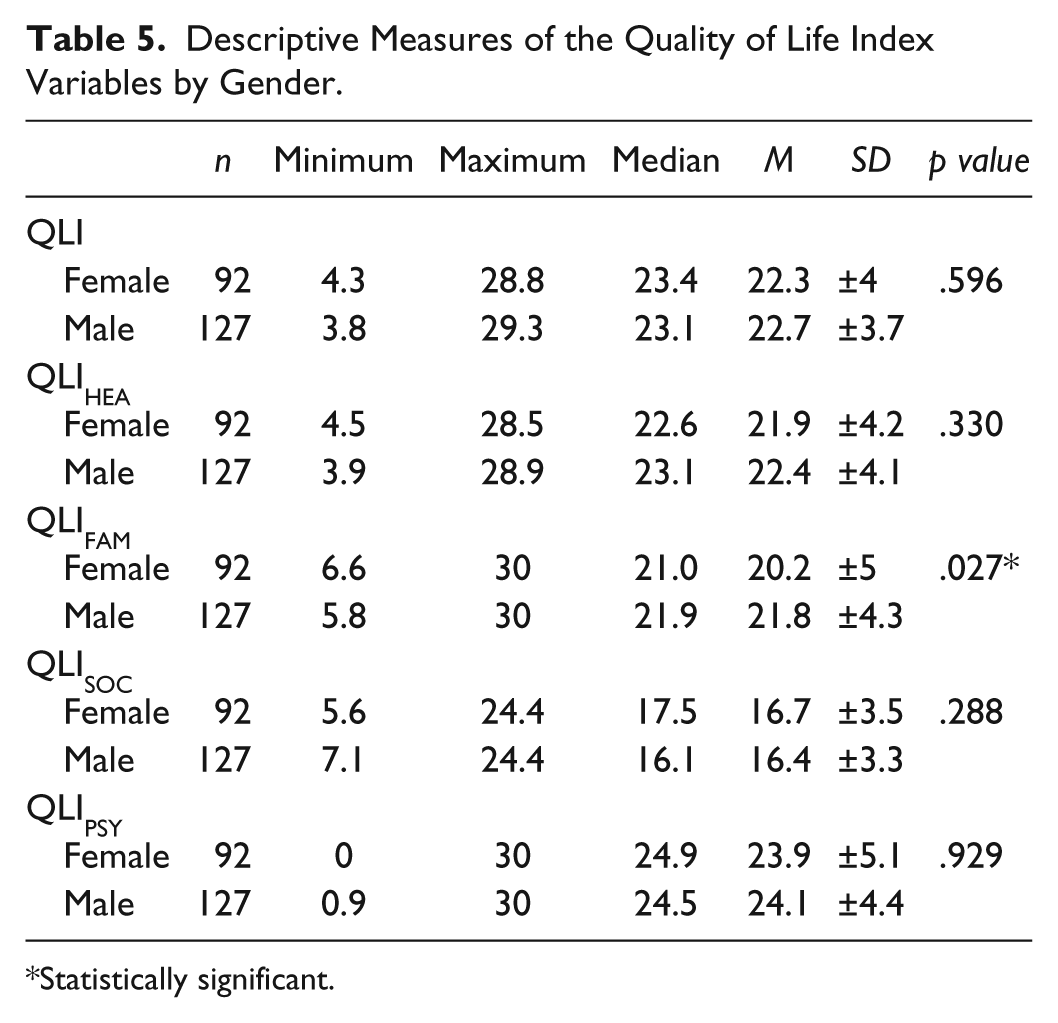
Statistically significant.
Discussion
The purpose of this study was to investigate the quality of life in Brazilian athletes as measured by the QLI. There were significant differences between competitive levels for the socioeconomic and psychological/spiritual subscales that suggest that professional athletes are more satisfied with the factors related to these areas and/or assign less importance to these factors than the amateur group. Moreover, there were significant group differences between males and females regarding the family domain, which indicate that factors related to family issues are more satisfying and/or have less importance for men than for women, as conceptual assumption of the instrument used in the research.
When considering comparisons between competitive levels, it is necessary to remember that the athletes classified themselves as amateur, semiprofessionals or professionals despite the different criteria as received a salary, received some type of aid or getting nothing, it is possible to imagine that the real difference in monetary values can be small, which may influence the results of the current study. A common consideration in research involving the athletic population is the criteria by which to define athletes. Aspects such as enrollment in federations, participation in official competitions and receiving salaries or benefits as a result of sports participation can help reproducible principles in future studies. Although most of the athletes in our sample considered themselves to be professionals, the lowest scores were reported for the socioeconomic domain that captures things like employment and financial independence. According to the survey answers in this study, even when the athletes describe themselves as professionals, they either do not consider this occupation to be a job, or they were not satisfied with this employment. It cannot be ignored that many athletes believe that sport is a way to escape poverty and expect to enhance economic and social status through sports. The reality is that few athletes can turn this dream into reality (Woods, 2011). Perhaps the unrealized expectations of the athletes cause dissatisfaction with the opportunities that the sport can offer. It theoretically seems a plausible explanation for the low scores found in the socioeconomic domain.
One cannot ignore the difficulty of delineating a precise definition of the concept of professional and amateur athletes to appropriately compare the groups. Depending on the athlete’s social group, the understanding of who is a professional athlete may involve a compensation officer, the amount of sponsorships or incentives, individual performance and results, membership in a federation, guidance on current legislation in a given region, the intensity of the athlete’s training or a combination of these factors. Despite the possibility of important differences during competitions, international athletes are especially subjected to the same conditions. In this sense, it is important to understand the living conditions, lifestyles, and the quality of life of athletes and provide proper support (International Olympic Committee [IOC], 2009). Increased knowledge about this topic can help coaches and sport managers improve individual experiences in the sporting systems.
In our study, we reported differences between professional and amateur athletes for the socioeconomic domain. In the case of professional athletes, the survey instrument requires a contract between the athlete and the institution. Somehow, in this case, the athletes can make future predictions about the continuity of their activities and their remuneration. In the case of the amateur athletes, the situation is opposite, there is no guarantee the continuity of work. It is plausible to imagine that institutions that have signed contracts with their athletes have clarity about what it is offered to the athlete and what should be required from the athlete. The definition of the roles of the institution and the athlete, and the stability of their relationship, defined by a contract may be an important factor to explain the difference between the groups of amateur and professional athletes, in relation to the quality of life socioeconomic domain.
The psychology/spiritual domain had the highest mean values across all domains. However, we found a significant difference between the amateur group and professional group, with the largest differences found for items related to “peace of mind” and “self-satisfaction.” To our knowledge, there is no previous study that has compared the quality of life among professional categories of athletes, which could help to explain these differences. However, this is an extremely important aspect for individuals who are exposed to competitive tension in daily lives. Furthermore, this finding draws attention to the fact that among all the factors of quality of life, the major value was found in the item that refers to “faith in God.” Woods (2011) claimed that athletes use religion to manage with pressure, uncertainty, and anxiety; to give life and sport a proper perspective; to provide meaning to sport participation; and to strengthen their bonds with teammates. Possibly, the results of this study express this relationship of the athletes with religiosity, which must be respected.
The comparison between genders revealed a significant difference in the family domain in which males reported higher scores than females. This result suggests that the structure of sport might differently influence men’s and women’s family relationships. According to Smith (2010), feminist theory indicates that the sport is a social construct essentially male. Even today the sport is more compatible with the family role of man (Smith, 2010). The roles of women in the family as a wife, homemaker, and mother probably produce conflicts with sports daily activities. For example, becoming a parent has a different impact on the sports career of men and women. The results regarding the quality-of-life family domain may reflect that fact. Additional research is required to more fully comprehend gender differences in athletes.
A comparison of the results with other studies was difficult because the differences in the studied population and instruments, like the Medical Outcomes Short Form SF-36 as a survey. Previous studies have indicated that the level of competition may impact quality of life. (McAllister et al., 2001; Modolo et al., 2009) For example, it has been reported that individuals who participate on competitive (Modolo et al., 2009) and elite levels (McAllister et al., 2001) tend to report better quality of life than those who participate on amateur and nonelite levels, respectively. These findings are in line with the results of the current study. Furthermore, a previous study (Tanabe et al., 2010) comparing quality of life of adolescent athletes found that males tended to report better quality of life than females, particularly for psychological well-being. Although we did not find gender differences for psychological well-being, we did report gender differences for family quality of life, further suggesting that the male and female athletes differ on certain aspects of quality of life.
However, the comparison between the QLI and SF-36 should be cautious, as the SF-36 has 36 questions divided into 8 subscales. (Ware & Sherbourne, 1992) Another aspect that needs to be taken into consideration is that the Medical Outcomes Short Form SF-36 has questions that may not be the most appropriate for athletes, for example: “Does your health now limit you in bathing or dressing yourself? Does your health now limit you in walking one block? Does your health now limit you in climbing one flight of stairs? Does your health now limit you in lifting or carrying groceries?” (Ware & Sherbourne, 1992). Anyway, the survey Medical Outcomes Study Short Form SF-36 is an instrument widely used in studies of quality of life, including sports field.
Another possibility of analyses is to examine some research using the QLI in other populations, even when the groups have a specific condition or health problem. Gullberg, Hollman-Frisman, and Ek (2010) conducted a study using the QLI in Sweden. The female group showed better results than the male group with regard to the family domain, which is different from the results found within the group of athletes in this study, and that might be explained by feminist theory mentioned above. Rossen and Knafl (2007) conducted a study of women between 61 and 91 years and also found the absolute highest value in the psychological/spiritual domain, but the lowest value was found in the health/functioning domain. Rannestad and Skjeldestad (2011) used the QLI in a study of female survivors of cancer and also found the highest absolute value in the psychological/spiritual domain and smallest absolute value in the health/functioning domain. In the studies cited above (Gullberg, Hollman-Frisman, & Ek, 2010; Rannestad & Skjeldestad, 2011; Rossen & Knafl, 2007) the absolute value of the quality of life in health/functioning domain was greater than the absolute value obtained with athletes in this research. In relevance to this analysis, it is important to note the data collection was done on time and location of training, before or after the practice sessions, so it was assumed that the athletes were in adequate health to sports. The absence of control of sports-related injuries can be a limiting factor in this analysis.
Previous studies indicate that athletes should report a significantly better quality of life related to health/functioning than nonathlete groups (McAllister et al., 2001; Snyder et al., 2010). Note that the health/functioning domain includes factors such as health, pain, and physical independence. Wrisberg (1996) may have an explanation for this fact when he said that “pain is venerated as the ‘manly sacrifice’ of competitive athletics, and playing with pain or even injury is an implicit expectation of many coaches and teams” (p. 400). Moreover, he claimed that “pressure to compete in the face of physical adversity—and to win—also comes from spectators and the media.” It should be noted that the concept of health and quality of life frequently is not well differentiated. This lack of conceptual precision might result in misleading conclusions, especially in sports. Athletes likely meet the recommendations of international organizations regarding the minimum level of physical activity for a healthy life (World Health Organization [WHO], 2010), assuming that athletes have healthy, and consequently, high quality of life. Yet, there are few studies in this area, and how factors related to athletes’ daily lives affect their quality of life remains unclear.
Study limitations include the unequal number of participants in each professional category. In addition to this, there are differences in living conditions that should be taken into consideration in limiting generalizations the results, as regards the sport and geographical differences; however, the results are available for comparison of new studies that enrich the future discussion on this subject.
Conclusion
The results revealed significant differences in the QLI socioeconomic and psychological/spiritual domains between amateur and professional athletes in Brazil. Additional differences on the family domain were found between male and female athletes. Future research that examines a wide range of aspects of athletes’ quality of life would increase the understanding of sports environment, and professional and amateur quality of life.
Footnotes
Acknowledgements
The author acknowledges the thoughtful comments of the Editor and two anonymous reviewers. The author is also grateful to Jackline Gense for statistical assistance in data analysis and all the institutions and athletes who participated in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The study was conducted with financial support from FAPESP (Research Support Foundation of São Paulo).