
Abstract
Obesity rates are high among employed adults and have shown a consistent increase over the past few decades. Musculoskeletal disorders related to work are a major cause of disability in working individuals. The objective of this study was to verify the associations between weight status and musculoskeletal pain and related symptoms in different body regions among workers. The sample comprised 203 factory workers. Anthropometric measures were assessed with standardized protocols and body mass index (BMI) was calculated. Participants were classified as nonoverweight (BMI ≤ 24.9 kg/m2) or overweight/obese (BMI ≥ 25 kg/m2). Musculoskeletal pain and related symptoms was assessed with the Nordic Questionnaire of Osteoarticular Symptoms. The association of BMI and musculoskeletal pain and related symptoms was analyzed with logistic regression. Overweight/obese participants were more likely to have musculoskeletal pain and related symptoms in the shoulders (odds ratio [OR] = 2.129, p = .023). Our results emphasize the need of worksite interventions to promote healthy weight as a way to prevent musculoskeletal pain and related symptoms.
Introduction
Overweight and obesity are one of the world’s most challenging public health problems (World Health Organization [WHO], 2003).The prevalence of overweight has reached epidemic proportions in most Western countries, including Portugal (Carreira, Pereira, Azevedo, & Lunet, 2012).
Overweight and obesity rates are high among employed adults and have shown a consistent increase over the past few decades (Snijder, Visser, Dekker, & Seidell, 2004; van Dam, Willet, Manson, & Hu, 2006). Overweight and obesity are well documented to be associated with major chronic illnesses, including hypertension, diabetes, arthritis, heart diseases, cancer, and all cause mortality (Christensen et al., 2011; Linde et al., 2012; van Dam et al., 2006). Excessive body weight has also been shown to increase the risk for musculoskeletal pain (Han, Schouten, Lean, & Seidell, 1997), sick leave, and early retirement from the workforce, causing high socioeconomic costs (Christensen et al., 2011; Tunceli & Williams, 2006; Verweij, Coffeng, van Mechelen, & Proper, 2011;). Obesity is associated with negative consequences in working populations, including more frequent absenteeism, workplace injury and disability pension claims, and higher health care costs (Linde et al., 2012).
It is also known that musculoskeletal disorders related to work are a major cause of disability in working-age individuals (Christensen et al., 2011; Verweij, Proper, Weel, Hulshof, & van Mechelen, 2009). Several studies have linked obesity with musculoskeletal disorders and the repetitive work (Christensen et al., 2011; Miranda, Viikari-Juntura, Martikainen, Takala, & Riihimäki, 2001; Tunceli & Williams, 2006).
As employed adults spend approximately half their waking time at work, worksites provide a logical setting in which the environment might be reshaped to promote healthier behaviors and improve weight control. Employers may be motivated to make changes due to concerns about quality or cost of employee health care (Osilla, 2012), and worksites may be in a unique position to develop resources and promote social support among coworkers for obesity preventive behaviors (Samuel, Raleigh, Hower, & Schwartz, 2003). Environmental changes that make conceptual sense for obesity prevention include targeting food service (i.e., availability of energy-dense foods, portion sizes, cost), the physical environment (e.g., opportunities for exercise), and information distributed to increase knowledge of behaviors related to obesity risk (French, Story, & Jeffery, 2001; Hill, Wyatt, Reed, & Peters, 2003).
According to public health perspective, effective well-documented initiatives for reducing weight, improving physical capacity, and reducing musculoskeletal pain among health care workers are therefore needed. Moreover, there is lack of evidence about the association between weight status and musculoskeletal injury in different body regions.
The aim of this study was to verify the associations between weight status and musculoskeletal pain and related symptoms in different body regions among workers.
Method
Study Design and Sampling
The present study derives from a larger research project on Physical Activity at Worksite, which is aimed to decrease physical disability, indicated by musculoskeletal disorders and related symptoms; increase work ability; and decrease sickness absence among workers with high physical work demands.
This study was conducted from November 2010 to September 2011, in a multinational manufacturing appliances company with office in Portugal. These 11 months included preliminary evaluation, selection of experimental group (EG) and control group (CG), the intervention program that lasts 6 months along with tests performed at baseline and at the end of the intervention.
For the purpose of this study, we only use the baseline data and limited the analysis to the variables under the scope of this study.
This study began by carrying out several introductory meetings about the project: the administration board, the medical department, production department, human resources department, as well as, the workers.
At the beginning of this intervention, 221 employees were invited (93 men; 128 women) to participate, from those, 212 agreed to participate (88 men; 124 women) in baseline tests and measures. The employees who did not participate did not significantly differ from those who agreed to participate, with regard to age, gender, and body mass index (BMI; p > .05, for all). Some participants were not included in our analysis (n = 9) because their weight and height information was missing. Therefore, the final sample comprised 203 participants (82 men; 121 women).
All the participants were full-time workers (40 hr/week) and employed in the company for at least 6 months.
All participants in this study were informed of its goals and provided written informed consent to participate. The study was approved by the Faculty of Sport, University of Porto Ethics Committee; it was conducted in accordance with the World Medical Association’s Helsinki Declaration for Human Studies.
Anthropometry Measures
Body height was measured to the nearest millimeter in bare or stocking feet with the participant standing upright against a stadiometer (Holtain Ltd., Crymmych, Pembrokeshire, United Kingdom). Weight was measured to the nearest 0.10 kg, lightly dressed using a portable electronic weight scale (Tanita Inner Scan BC 532, Tokyo, Japan). BMI was calculated from the ratio between body weight (kg) and body height (m2). Participants were categorized as nonoverweight, overweight, and obese, applying the cutoff points suggested by the WHO (2000).
Percentage of body fat (% BF) was estimated using a bio impedance scale (Tanita Inner Scan BC 532, Tokyo, Japan), which was set to “standard” for body frame, and the participant’s age, height, and gender were entered.
Waist circumference was measured twice, with a nonelastic metal anthropometric tape, midway between the lower rib margin and the iliac crest at the end of normal expiration (Lohman, Roche, & Martorell, 1988). The average of the two measures was used for analysis. If the two measurements differed by more than 1 cm, a third measurement was taken and the two closest measurements were averaged.
Sociodemographic Variables
Participants answered a questionnaire that assessed several sociodemographic variables (age, marital status, etc.). Participants were divided according to their job position in factory, that is, “white-collars” (skilled occupations) and “blue-collars” (unskilled and manual jobs).
Musculoskeletal Disorders and Related Symptoms
Musculoskeletal pain and related symptoms were assessed by Nordic Questionnaire of Musculoskeletal Disorders (NMQ; Kuorinka et al., 1987), supplemented with questions about localized pain intensity. This questionnaire has been validated to the Portuguese population (Mesquita, Ribeiro, & Moreira, 2010). The NMQ consists of 27 binary choice questions (yes or no). The questionnaire has three questions correlating to nine anatomic regions (neck, shoulders, writs/hands, lumbar region, dorsal region, hips/thighs, knees, ankles/feet)—“had some troubles or pain in the last 12 months,” “in the last 12 months felt some limitation caused by work in the daily activities,” and “had some troubles or pain in the last 7 days.” In the sense of facilitating the identification of the corporal areas, the questionnaire also includes a corporal diagram detaching all of the involved corporal areas (Kuorinka et al., 1987). The pain intensity in the “last 7 days” was included in the numeric pain scale (range = 0-10).
Statistical Analysis
Descriptive characteristics of the participants were presented as means ± standard deviation and percentages. The Kolmogorov–Smirnov test was used to assess the assumption of normality. Two-tailed t test was performed to compare groups for continuous variables and χ2 test for categorical variables. The association between weight status and musculoskeletal pain and related symptoms was analyzed with logistic regression adjusted for age, gender, and jobs position. Only the significant results of logistic regression models are presented. The data were analyzed for statistical significance by using the statistical package of social science (SPSS 20.0) software for Mac OXS. A p value below .05 was denoted as significant.
Results
In the total sample (n = 203), 38.4% was classified as overweight and 22.2% as obese (Table 1). Overweight/obese participants had higher proportion of “blue-collars” jobs compared with nonoverweight participants (76.4% vs. 23.6%, respectively, p = .013). No significant differences for age and proportion of gender were seen between weight status.
Descriptive Characteristics of the Participants, by Weight Status.

Note: BMI = body mass index; WC = waist circumference; % BF = % body fat. Data are mean (± standard deviation).
Analysis by t test for continuous variables.
Analysis by χ2 for categorical variables.
As depicted in Table 2, the overweight/obese participants reported more frequently musculoskeletal pain and related symptoms in the shoulders (p = .007) and wrist/hand in the last 12 months (p = .04) compared with their normal weight counterparts.
Musculoskeletal pain in different body regions of the target population.

Note: n (%);1 Data are mean (standard deviation); a analysis by t-test for continuous variables; b analysis by X2 for categorical variables.
12m – concerned the question of NMQ about “had some troubles or pain in the last 12 months” in body regions.
Avoid - concerned the question of NMQ about “in the last 12 months felt some limitation caused by work in the daily activities”
7days - concerned the question of NMQ about “had some troubles or pain in the last 7 days”
Logistic regression analysis showed that overweight/obese participants were more likely to have musculoskeletal pain and related symptoms in the last 12 months in the shoulders (odds ratio [OR] = 2.129, p = .041; Table 3).
Odds Ratios for Pain in the Last 12 Months in Shoulder and Wrist/Hand by Weight Status.
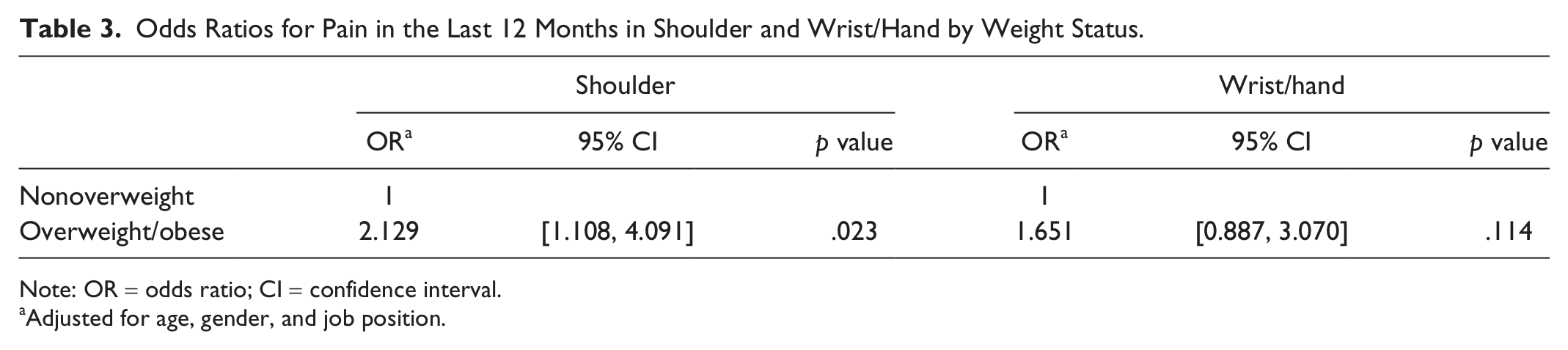
Note: OR = odds ratio; CI = confidence interval.
Adjusted for age, gender, and job position.
Discussion
In this study, we found that overweight/obese participants reported higher pain intensity only in shoulders and wrist/hand compared with their lean counterparts. The results suggested that overweight/obese participants were more likely to have musculoskeletal pain and related symptoms in the last 12 months in the shoulders. This association was not confounded by age, gender, and jobs position as it remained significant after adjustments.
In this study, a higher proportion (60.6%) of overweight/obesity was seen among workers. Likewise, a cross-sectional study has found overweight/obesity prevalence above 60% among Kuwait Oil Company workers (Al-Asi, 2003). Choi et al, (2010) in a longitudinal study also showed that the prevalence of overweight/obesity increased significantly from 1995-2002 among factory workers. Moreover, overweight and obesity are more prevalent among blue-collar and shift workers than among white-collar and office workers (Karlsson, Knutsson, & Lindahl, 2001; Nakamura, Nakamura, & Tanaka, 2000; Nakamura et al., 1997). In our study, we also found a higher proportion of overweight/obesity in blue-collar workers. Furthermore, obesity may represent an additional risk factor for diseases that result from workplace exposures (Schulte et al., 2007). These findings emphasize that efficient weight loss programs are highly relevant as health promotion for this sector. Indeed, we find an example in a Danish workplace health promotion study with workers. The study consisted in promoting correct ergonomic setup, frequent rest, stretching and strengthening exercises and showed a reductionin a few degrees of the physiological and psychological load in the body. In another study, a randomized controlled trial, included 16 school worksites (8 interventions and 8 controls), the intervention schools formed committees to develop and implement health promotion activities for employees. Anthropometric and self-report data were collected at baseline and at the end of the intervention (2 years later). The primary outcome measures were BMI, waist–hip ratio, physical activity, and fruit and vegetable consumption. This participatory intervention resulted in a modest improvement in health status and possible unmeasured secondary gains, such as improved morale and increased productivity (Siegel, Prelip, Erausquin, & Kim, 2010). Thus, some studies highlight the importance of the reduction of body weight in sedentary works, to decrease the risk to related musculoskeletal disorders and occupational-psychosocial stress, and improve life quality (Christensen et al., 2011; Schulte et al., 2007).
In our study, we found a positive association between BMI and musculoskeletal pain and related symptoms in last 12 months in the shoulder and in the wrist/hand. Several studies observed a positive association between overweight/obesity and increased risk of musculoskeletal disorders, sickness absence, work disability, cardiovascular disease, and mortality (Schmier, Jones, & Halpern, 2006). It has also been described that obesity appears to have a significant positive association with absenteeism (measured as work loss days; Bungum, Satterwhite, Jackson, & Morrow, 2003; Schulte et al., 2007). Sethi, Sandhu, and Imbanathan (2011), in 301 workers with different jobs and shifts in an engineering plant, found a significant association (p < .001) between high BMI and increased scores of musculoskeletal discomfort and occupational stress. The authors of the latter study also reported a higher incidence of overweight and obesity in these workers compared with the national average for similar age classes; therefore meetings were organized at the plant on awareness and information on correct lifestyle and diet targeted for shift workers. Bihari, Kesavachandran, Pangtey, Srivastava, and Mathur (2011) also found in cross-sectional study that the risk of musculoskeletal pain among overweight/obese individuals was 1.7-times more as compared with nonoverweight participants.
Some limitations of the present study should be acknowledged. As in every cross-sectional study, conclusions related to cause and effect cannot be drawn. With the use of self-reported musculoskeletal pain and related symptoms, one cannot rule out some reporting bias; however, the questionnaire has been previously tested (Mesquita et al., 2010). BMI may not be a sensitive measure of body fatness when there are some sophisticated methods to accurately measure body fat, such as magnetic resonance imagining or dual-energy X-ray. However, such techniques are not feasible to apply in work environment, because they are complex and time-consuming. Thus, BMI has been widely used as an index of relative adiposity among adults and in studies of the impact of work on obesity.
Conclusion
In our study, we found that overweight/obesity is positively associated with musculoskeletal pain and related symptoms in shoulders among workers. This study provides the insight to the health professionals about the relationship between BMI and musculoskeletal pain and related symptoms, to formulate well-designed training program to avoid overweight.
Footnotes
Acknowledgements
We thank all the participants and the Bosch Company.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by FCT- MCTES Grant PEst-OE/SAU/UI0617/2011.
Author Biographies