
Abstract
Sexual behavior change is a complex issue influenced by complex variables, intrinsic and extrinsic. This study aimed to assess factors influencing actual use of a male condom among secondary school students in southern Tanzania. In all, 227 sexually experienced participants aged 14 to 18 completed a pretested questionnaire. Out of 227 sexually active participants, 120 (53%) reported consistent condom use and (62.5%) had multiple sexual partnerships. Of 120 who reported condom use, 42 (35%) had tested for HIV. Among males, age was positively correlated with actual condom use, while being a Catholic and having multiple concurrent sexual partners were negatively correlated with actual condom use. Among females, being a Protestant was positively related with actual condom use, while being a Catholic, reporting multiple sexual partnerships, and perceived barriers to condom were negatively correlated with actual condom use. In conclusion, sexually active youth in this population practice risky sexual behaviors, with a low proportion of condom use. Efforts are warranted to motivate sexually active youth to engage in HIV prevention, including condom use and HIV testing.
Background
Human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) remain a worldwide public health problem with an estimated 36 million people living with HIV globally (UNAIDS, 2010). Sub-Saharan Africa (SSA) is most heavily affected by HIV/AIDS, with an estimated 22.9 million people living with HIV, two thirds of the global HIV burden (UNAIDS, 2010). Tanzania ranks among seven countries with the highest HIV prevalence among adults. By the end of 2010, an estimated 1.7 million Tanzanian were living with HIV, with an overall prevalence of 15% among 15- to 24-year-olds (Tanzania Commission for AIDS, Zanzibar AIDS Commission, National Bureau of Statistics, & ORC Marco, 2008; World Health Organization [WHO], 2010). Indicators of sexual activity among youths in Tanzania revealed that a substantial proportion of unmarried females as well as males are sexually experienced (Holm-Hansen, Nyombi, & Nyindo, 2007; Kazaura and Masatu, 2009; Masatu, Kazaura, Ndeki, & Mwampambe, 2009; Njau et al., 2006; Tanzania Demographic and Health Survey [TDHS], 2010). Previous studies conducted in SSA on early sexual debut and high-risk sexual behaviors have identified a host of environmental, economic, gender inequalities, and social norms that influence adolescent sexuality (UNAIDS, 2010). Although the above-mentioned factors may be outside the individual’s control, it has been observed that psychosocial ideational factors, defined as proximate determinants (e.g., perceived risks, self-efficacy, and social approval) have an indirect influence on the choice of protective behaviors such as condom use (Babalola, 2005; Fisher & Fisher, 2000; Underwood, Sachonda, Serlemitsos, & Bharath-Kumar, 2006).
The cost-effectiveness of condom use interventions to prevent HIV infection has been well documented (Creese, Floyd, Alban, & Guinness, 2002; Walker, 2003). There are several factors that motivate youths to use condoms. For example, a study by Njau et al. (2006) among Tanzanian youth revealed that personal knowledge about HIV prevention, influence of significant others or peers, perceived vulnerability, and self-efficacy regarding condoms were the important motivators to condom use. However, previous investigators have identified some barriers to condom use among youth including myths, misconceptions, and suspicion of condom accuracy in the protection of HIV infection (Kennedy, Nolen, Applewhite, Waiters, & Vanderhoff, 2007; Ochieng, Kakai, & Abok, 2011; Toroitich-Ruto, 2004). Therefore, to motivate youths to engage in condom use, health planners and program managers need to have a broad understanding regarding correlates of condom use among this high-risk group.
This study uses the Health Belief Model (HBM) to understand the correlates of condom use among secondary school students. According to the HBM, several factors, such as perceived severity or vulnerability, perceived severity of an outcome or condition, perceived efficacy or benefits of a preventive measure, cues of action (i.e., external influences promoting the desired behavior, may include information provided or sought, reminders by significant others, persuasive communications, and personal experiences), and the perceived barriers are important factors in decision making (Champion & Skinner, 2008; Muela & Ribera, 2003).
The HBM was adopted in this study because it is based on the idea that value and expectancy beliefs guide behavior. Another key reason is that HBM is among few health behavior theories, which explicitly includes perceived symptoms of illness, such as AIDS. This often underappreciated the dimension of HBM, theorizing that medical symptoms are cues to action that prompt behavior, such as condom use. Last, constructs in the HBM have received substantial empirical support for their ability to predict correlates of health behavior, such as condom use (Champion & Skinner, 2008).
There is dearth of empirical evidence that theoretical constructs mediate condom use in Tanzania. Previous studies conducted on condom use among secondary school students in Tanzania were mainly concentrated on knowledge, attitude, and practices (KAP), and were not grounded on theoretical models, such as the Health Belief Model (HBM).
This study therefore aims to identify factors that motivate or hinder condom use among secondary school youths in a rural setting. Findings from this study will add knowledge to the literature by exploring how HBM factors might explain actual use of a male condom and provide a basis for designing an effective HIV prevention program for secondary school youths aged 15 to 18 years in rural communities of Tanzania.
Method
Recruitment
The study was conducted in Rungwe district in Mbeya region of the Southern highlands of Tanzania. The district is a mixed Christian and Muslim community with a total population of approximately 3 million people, the majority of whom are tea farmers and traders (National Bureau of Statistics, 2002). Administratively, the town is divided into two divisions and 30 wards. The overall prevalence of HIV in this area is 9.2%. The district has a total of 46 secondary schools, with an estimated 24,198 students aged between 15 and 24 years (TDHS, 2010). The secondary Education system in Tanzania is categorized as public (government or community owned) or private (nongovernment or religious owned) and consists of two tiers. The first tier is ordinary level (O-level) of 4 years postprimary education (Years 1-4). The second tier is advance level (A-level), which is 2 years post O-level (Ministry of Education and Vocational Training, 2011). In addition, secondary schools in Tanzania can be single sex (boys or girls) or mixed sex (coeducation).
The following assumptions were used to arrive at the required minimum sample size. We used Epi-Info version 6.0 statistical software to calculate an appropriate sample size. Condom use was estimated based on the prevalence of a male condom use (34.2%) among youth in Tanzania (TDHS, 2010). To detect a 10% difference in the rate of condom use with 80% power, a sample of 350 was needed. An additional 10% of the estimated size was added to adjust for dropout (nonresponse rate), giving the final sample size of 385.
A multistage random sampling method was used. All secondary schools in Rungwe district formed the primary sampling frame and were clustered according to school category (i.e., public/private), which formed the sampling units in the study. Clustering of schools ensured that all the different segments in the sampling frame were represented.
Based on geographical location, the schools were randomly selected using the lottery method to ensure that each school had an equal chance of being selected, thus avoiding selection bias. Out of 46 secondary schools in Rungwe district, stratified into public (40) and private (6) schools, a total of 11 (9 public, 2 private) schools were sampled (7 coeducation schools, 2 boys only, and 2 girls only). Of the students, 10% per selected schools were interviewed. In the coeducation schools, a ratio of 1:1 was used for male and female students.
Within the schools, study participants were selected using systematic random sampling. Every year level in a school formed a secondary sampling frame. To obtain a truly random sample a list of all students in a secondary sampling frame were randomized, prior to determine the sampling interval. To decide on the sampling interval the researcher first calculated 10% of the total population in a school. The result was then divided by the number of the year levels in the school to determine the sample size per class. The sampling interval (nth) was then calculated by dividing the number of students in a class (N) by the class sample size (n).
The students were organized alphabetically and the first student was selected blindly using a table of random numbers after which the remaining students were selected at regular intervals (nth) from the secondary sampling frame. This process was repeated until the required school sample size was achieved.
Primary data were collected using a pretested self-administered questionnaire adopted from Benin (Hounton, Carabin, & Henderson, 2005), and adapted to elicit response on demographic variables, sexual risk behaviors, and key HBM constructs.
Study Measures
The outcome variable was condom use in the last 3 months, which was assessed with a single question with a yes or no response. Demographic variables include sex, age, religion, grade level, and type of school. Independent variables were based on the key HBM constructs, namely (a) perceived susceptibility, (b) cues to action for condom use, (c) perceived barriers to condoms, (d) social approval for condom use, and (e) perceived self-efficacy for condom use. The primary variables of interest were assessed as follows. Unless indicated otherwise, the response was a 5-point Likert-type scale to index the psychosocial variables.
Sexual Risk Behaviors
Participants were asked about unprotected sex and actual condom use in the last 3 months. Responses were dichotomized and coded: “no condom” (reported noncondom use) or “condom use” (reported condom use) depending on whether participants had sex with or without condom. Women participants were asked whether their male partner used a condom when they had sex in the past 3 months (e.g., “In the last 3 months, did your male partner use a condom during sexual intercourse?”).The expected response was 1 = yes; 2 = no.
Perceived Susceptibility
Perceived susceptibility regarding HIV infection was assessed by one question (e.g., “Do you think you are susceptible of getting HIV infection?”). Expected answering categories was 1 = yes; 2 = no.
Cues to Action for Condom Use
Cues to action were assessed by four items on communication skills that may motivate youths to use condom. Respondents were asked whether they communicate about actual condom use: (a) it is important to discuss condom use prior to having sex; (b) it is important to negotiate condom use prior to having sex; (c) it is important to ask for condom use prior to having sex; and (d) it is important to have a condom prior to having sex. The expected response was 1 = yes; 2 = no.
Perceived Barriers to Condom Use
A belief-based index was assessed by six items addressing perceived barriers to condoms: (a) condoms reduce pleasure; (b) use of condoms encourages promiscuity; (c) I don’t like condoms; (d) my religion prohibits condom use; (e) condoms offer no protection; and (f) I feel shy to buy condoms. The reliability scale was α = .92. Responses in each domain were coded 0 to 5 and added to create barrier score, with higher scores indicating difficulties to access a male condom. The mean perceived barrier to condoms score was categorized into low barrier score (0-2) and high barrier score (3-5).
Social Approval for Condom Use
Perceived social approval for condom use was assessed by a four-item index that asked the respondents whether they believe that specific significant others would approve of condom use if allowed to have sex. The significant others inquired about included peers, parents, religious leaders, and health workers (e.g., “Do your parents approve you using condoms, if you are allowed to have sex?”). The response choices were 1 = yes; 2 = no. This scale was reliable at α = .73.
Perceived Self-Efficacy for Condom Use
Five self-efficacy items were used to ask the respondents about level of confidence to be (a) able to buy a male condom; (b) able to use a male condom correctly; (c) able to carry a male condom when planning to have sex; (d) able to use a condom with a partner with whom they have a long trusting relationship; and (e) able to refuse to have sex if a partner will not use a condom. The expected response categories ranging from 1 = strongly disagree to 5 = strongly agree. The reliability scale was α = .59. Responses in each domain were coded 0 to 5 and added to create self-efficacy score, with higher scores indicating difficulties to access a male condom. The mean self-efficacy score was categorized into low self-efficacy (0-2) and high self-efficacy (3-5).
The survey questionnaire consisted of precoded questions and developed in English with back-and-forth translated in Kiswahili. The instrument was then piloted with a convenient sample of n = 15 (6 males vs. 7 females). Four trained research assistants (2 males and 2 females) who had the same age (range = 15-18 years old) were at hand to assist participants that need help completing the questionnaire. To ensure confidentiality, the completed questionnaires were put in sealed envelopes, and no names were recorded. Research and ethical clearance were obtained from Kilimanjaro Christian Medical University College Ethics Committee and from local administrative officers for implementation of the study. Consent was obtained after the potential participants and their parents/guardians (for those below 18 years) were informed of the study’s objectives. All parents/guardians were given the opportunity to withhold their child from the study. Only students aged between 14 and 18 years who gave informed consent as described above to participate were included in the study.
Data Analysis
The questionnaires were checked for accuracy, completeness, and uniformity, and then entered. Data were analyzed using Statistical Package of Social Sciences (SPSS) for Windows Version 20.0. Descriptive statistics were estimated as proportions. A subset of the sample size that was sexually active was used to assess actual condom use. The chi-square test was used to compare proportions between categorical variables; the logistic regression model was used to estimate the association between the categorical dependent variable (any condom use in the last 3 months) and a number of explanatory factors. A p value of .05 or less (two-tailed) was considered to be significant.
Factors that were significantly related to condom use in bivariate analysis were included in a multivariate logistic regression model. Considering that the correlates of condom use would differ by gender, we constructed separate models for the male and female respondents and estimated the effect of these predictors on actual condom use. For each gender, we estimated two models. The first model only included sociodemographic variables, while the second model combined sociodemographic variables, HBM constructs, and sexual activities.
In the multivariate analysis, all variables for measuring HBM constructs were dichotomized. The cutoff for dichotomization was a mean score of less than or equal to 2. The parameter estimates, p values, adjusted odds ratios (AOR), and 95% confidence intervals (CI) are shown in Tables 4 and 5.
Results
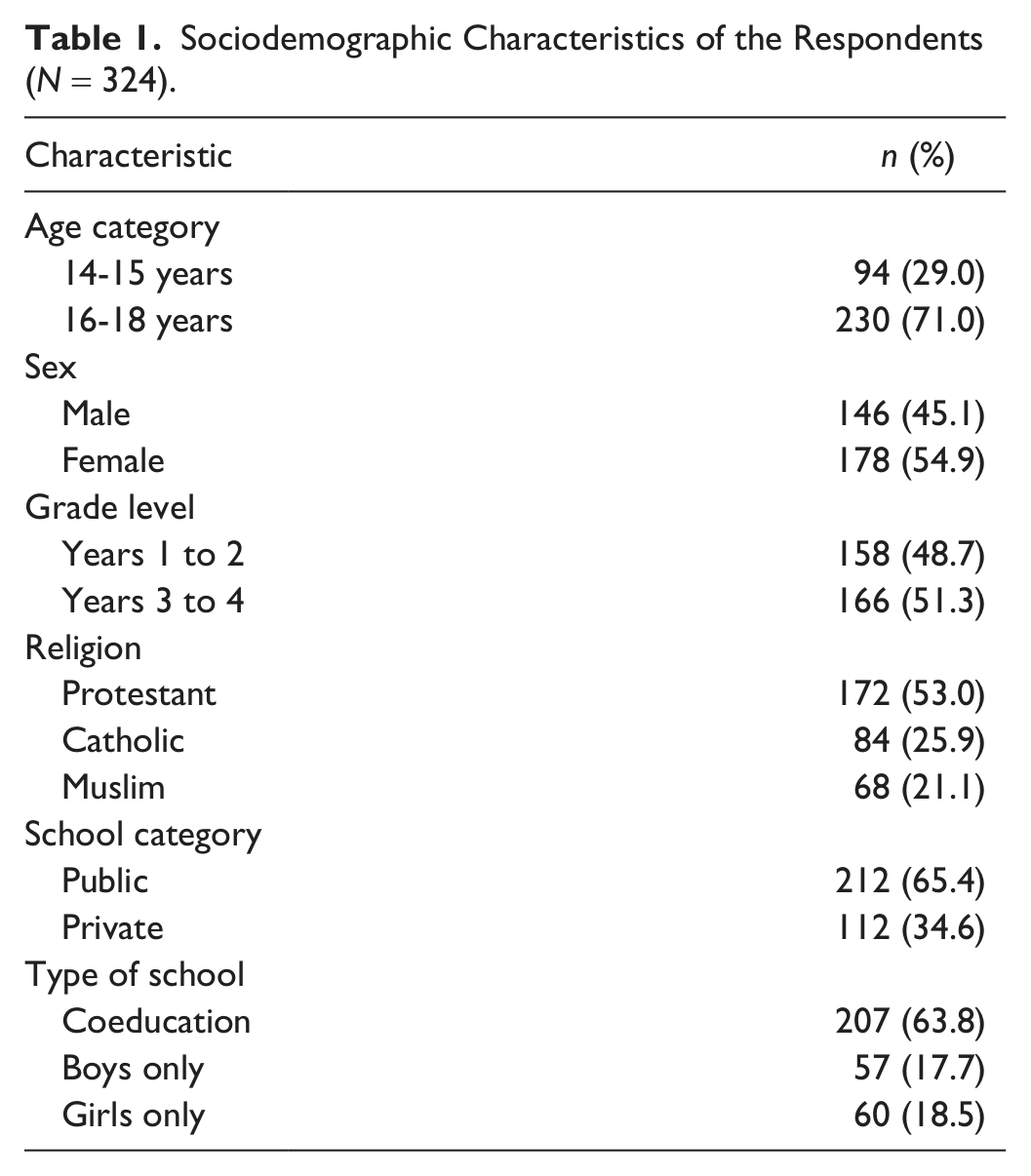
A total of 324 students participated in the study, a participation rate of 84.2%. Table 1 summarizes sociodemographic characteristics of the study participants. More than half (55%) were females, 71% were aged 16 to 18 years, 51.2% were in Years 3 to 4, and 78.9% were Christians.
Sociodemographic Characteristics of the Respondents (N = 324).
Demographics Characteristics and Actual Condom Use
In this study, 227 participants reported being sexually experienced; of these, 120 (52.8%) reported actual condom use in the last 3 months. Age and religion were demographic characteristics associated with actual condom use in the last 3 months. Younger participants (14-15 years) were significantly less likely to use condoms compared with their older counterparts (13.7% vs. 98.1%; p ≤ .001). In addition, Christians were less likely to use condoms as compared with their Muslim counterparts (p ≤ .001). There was no association between actual condom use and gender, grade level, or type of school (Table 2).
Sociodemographic and Condom Use (n = 227).

Note. REF = reference category.
p < .001.
Condom Use Among Sexually Active Participants
More than two thirds, 142/227 (62.5%), of sexually active participants reported multiple (>1) concurrent sexual partners. However, those who practiced multiple sexual partnerships had slightly higher proportion of condom use as compared with those who have had a single partner (64.2% vs. 35.8%). Cues to action, perceived barriers to condoms, social approval, and self-efficacy were HBM constructs that were associated with actual condom use. Participants who were unable to discuss condom use prior to having sex were 56% less likely to report actual condom use (OR = 0.44; 95% CI = [0.24, 0.82]; p < .005). Participants who had low perceived barrier to condom score had a 24-fold (95% CI = [10.46, 58.2]; p < .001) odds of reporting actual condom use as compared with those who had a high score. Perceived social approval was associated with reported condom use. Participants who disagree the importance of significant others (peers, parents) approval of condom use were more likely to report condom use as compared with those who agreed (OR = 2.32 [1.23, 4.40]; p < .005). Last, self-efficacy to condom use was strongly associated with reported condom use. Participants who had a low mean self-efficacy score had a 4-fold (95% CI = [2.05, 8.62]) odds of reporting actual condom use, compared with those with a high mean score. Half, 115/227 (50.7%) of sexually active participants reported to have had HIV testing; of these, 45/115 (37.5%) reported condom use. The difference between testers and nontesters with actual condom use was statistically significant (Table 3).
Factors Associated With Condom Use in Bivariate Analysis (n = 227).

Note. REF = reference category.
p < .005; ***p< .001.
Correlates of Condom Use by Gender
Multivariate analysis revealed some significant gender differences in use of condoms in the last 3 months: 58.2% for sexually experienced unmarried males compared with 47.3% of unmarried females. We therefore conducted stepwise models separately for males and females as shown in Tables 4 and 5.
Adjusted Odds Ratios (AOR) and 95% Confidence Intervals [CI] From Logistic Regression Analysis Examining Associations Between Selected Variables and Condom Use, by Gender.

Note. Models 1a and 2a include social-demographic variables only; Models 1b and 2b include sociodemographic and HBM variables. REF = reference category.
p < .02. **p < .005. *** p < .001.
Adjusted Odds Ratios (AOR) and 95% Confidence Intervals [CI] From Logistic Regression Analysis Examining Associations Between Selected Variables and Condom use, by Gender.

Note. Models 1a and 2a include social-demographic variables only; Models 1b and 2b include sociodemographic and HBM variables. REF = reference category.
p < .02. **p < .005. *** p < .001.
In Model 1a for males, some sociodemographic variables such as age and religion were associated with actual condom use. Participants aged 16 to 18 years were more likely to report condom use as compared with younger youth. An increase of 1 year in age was associated with ninefold (OR = 9.73 [3.12, 28.54]; p < .001) increase in actual condom use. When sexual activities and perceived barrier to condom scores were included in Model 1b, age maintained its relationship with reported condom use (OR = 14.88 [3.25, 68.10]; p < .001).
Religion was another factor that was associated with reported condom use. Catholic participants were 75% less likely (OR = 0.25 [0.09, 0.68]; p < .001) to report condom use as compared with Muslims and Protestants. The effect of religion on condom use remained (OR = 0.32 [0.13, 0.81]; p < .001) when the HBM constructs were added in Model 1b.
Multiple sexual partnerships, however, were negatively associated with reported condom use. Males who reported having two or more concurrent sexual partners were 64% (OR = 0.36 [0.15, 0.85]; p < .005) less likely to report condom use as compared with those who had single partner. However, perceived barriers to condom use in Model 1b did not predict reported condom use.
The results from Model 2a for females show that older females (aged 16-18 years) had a fourfold (95% CI = [1.64, 8.91]; p < .02) increase of reported condom use, compared with their younger counterparts. However, when a sexual activity variable was introduced in Model 2b, age did not appear to have an influence on condom use.
Religion appeared to be an important predictor for reported condom use among females. Protestants were 5 times (95% CI = [1.65, 16.40]; p < .005) more likely to report condom use as compared with Catholics and Muslims. The predictive effect of religion on condom use remained in Model 2b (OR = 4.97 [1.44, 17.21]; p < .02).
Multiple sexual partnerships were negatively associated with reported condom use. Female respondents who reported having two or more sexual partners were less likely to report condom use (OR = 0.04 [0.01, 0.20]; p < .001).
Perceived barriers to condom use was the only HBM variable associated with reported condom use among female respondents. Females who had a high perceived barrier score on condoms were less likely to report actual condom use (OR = 0.09 [0.03, 0.31]; p < .001), compared with those with lower perceived barriers to condom score (Table 5).
Discussion
This study has shown that use of male condoms among secondary school respondents is associated with different factors for males and females. In this study, male respondents were more likely to report condom use in their last sexual intercourse (last 3 months) than their female counterparts. This observation is probably linked to the fact that male respondents are generally more mobile and have more access to information on condoms and the ability to buy condoms (Ochieng et al., 2011). However, our finding is in contrast with previous investigators in Tanzania, who found that condom use was higher among females than males (Exavery et al., 2011). The most important explanatory factor to this observation may be gender power differences in condom use among male and female participants (Prata, Vahidnia, & Fraser, 2005). In addition, gender disparities in condom negotiation skills may explain the discrepancy of frequency of reported condom use between males and females (Babalola, 2005; Njau et al., 2006).
The likelihood of actual condom use was higher among older respondents (16- to 18-year-olds) than their younger counterparts (14- to 15-year-olds), and this observation can possibly be due to the knowledge differences regarding transmission and prevention of sexually transmitted infections (STIs), including HIV, because of longer exposure to sensitization messages on condom use (Exavery et al., 2011; Njau et al., 2006; TDHS, 2010). This observation underscores the importance of sexual health education in secondary schools. However, the lack of association observed in the estimated model for females between age and reported condom use may imply that age does not solely influence reported condoms among females. Religious beliefs significantly shape individual’s practices of condom use (Ragnarsson, Onya, & Aaro, 2009; Zou et al., 2009). In this study, being a Christian was associated with reduced condom use as compared with Muslims. This observation is in agreement with findings from other studies (Gray, 2004; Lagarde et al., 2000; Zou et al., 2009). Interestingly, female Protestants were more likely than their Catholic counterparts to report condom use in the logistic regression analysis. This observation of reported condom use among female Protestants can partly be explained by the fact that the Lutheran church generally has a more flexible stand on condom use than Catholics (Agha, Hutchinson, & Kusantahn, 2006). However, this observation should be taken with caution because the study’s main objective was not to determine the role of religion on reported condom use.
In this study, nearly half of sexually experienced respondents never used a condom in their last sexual intercourse (last 3 months). Furthermore, two thirds reported having had sex with multiple concurrent sexual partners in the last 3 months. This observation raises concern that respondents in the study area remain at risk of contracting STIs, including HIV and unintended pregnancies (Kazaura & Masatu, 2009; UNAIDS, 2010). Overall, low rates of condom use coupled with high rates of multiple concurrent sexual partners among males may increase the spread of HIV in Tanzania (TDHS, 2010). This alarming observation calls for Adolescent Sexual and Reproductive Health (ASRH) interventions (e.g., peer-assisted ASRH lessons, distribution of free condoms and social marketing of family planning, etc.) in secondary schools in Tanzania (Renju et al., 2010).
This study used the HBM to determine how HBM constructs might explain condom use. Out of five HBM constructs, only perceived barriers to condom use were associated with reported condom use, particularly among female respondents in the logistic regression model. Female respondents who had a higher perceived barrier score were less likely to report condom use. This observation may be partly attributable to the fact that perceived barriers to condoms often correlate with lower levels of condom use (Lawonyin & Kanthula, 2010). It may also be linked to variations in social cultural gender norms (Exavery et al., 2011) or lack of skills in condom use (Adebiyi & Asuzu, 2009). This finding is consistent with the HBM (Champion & Skinner, 2008; Fishers & Fisher, 2000) and suggests that an intervention designed to increase motivation for condom use, while addressing perceived and actual barriers to condom use, may be an effective approach, particularly among females (Lauby, Bond, Eroglu, & Batson, 2006; Noar, 2008; Outlaw, Naar-King, Janisse,& Parsons, 2010).
Despite the fact that most sexually active respondents practiced risky sexual behaviors, a significant proportion had never tested for HIV. It is well documented that HIV testing is an entry point to changes in HIV risk behavior practices, HIV reduction strategies, and improved knowledge of sexual focus of HIV prevention (Fiorillo et al., 2012; Holm-Hansen et al., 2007). The low proportion of HIV testers in this study is disturbing and calls for increased efforts for HIV testing and counseling strategies among adolescents in secondary schools in Tanzania (Renju et al., 2010).
Strengths and Limitations of the Study
This study must be interpreted in light of its limitations. First, as a cross-sectional study design, it is not able to draw conclusions about causality of any of the identified associations. Second, given that this study was conducted in one location, it may not be applicable to other settings. Third, the study used the HBM, a cognitive based model, which is limited in accessing the emotional components of behavior (Champion & Skinner, 2008). Last, some item-level analyses were limited due to moderate internal reliability of the scales (e.g., perceived self-efficacy for condom use), and may therefore affect the validity of the study findings.
Conclusion
Importantly, the study findings indicate that sexually experienced youths in the study area practice risky sexual behaviors, such as unprotected sex and multiple sexual partnerships, with low proportions of HIV testing. Efforts are warranted to motivate sexually experienced youths to engage in HIV prevention strategies, including condom use, HIV testing, counseling, and sexual health education in secondary schools in rural Tanzania.
Footnotes
Acknowledgements
We gratefully acknowledge all secondary school students who participated in this study. We also thank local educational authorities who provide permission to conduct this study. Last, we thank Drs Melissa Watt and Elizabeth Reddy of Duke University, USA, for critical review and editing of the manuscript.
Declaration of Conflicting Interest
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Author Biographies