
Abstract
Yearly influenza vaccination continues to be underutilized by those who would most benefit from it. The Health Belief Model was used to explain differences in beliefs about influenza vaccination among at-risk individuals resistant to influenza vaccination. Survey data were collected from 74 members of at-risk groups who were not vaccinated for influenza during the previous flu season. Accepting individuals were more likely to perceive flu as a threat to health and perceive access barriers, and cues to action were the most important influence on whether they plan to get vaccinated. In comparison, resistant individuals did not feel threatened by the flu, access barriers were not a problem, and they did not respond favorably to cues to action. Perceived threat, perceived access barriers, and cues to action were significantly associated with plans to be vaccinated for influenza in the next flu season. Participants who saw influenza as a threat to their health had 5.4 times the odds of planning to be vaccinated than those who did not. Participants reporting barriers to accessing influenza vaccination had 7.5 times the odds of reporting plans to be vaccinated. Those responding positively to cues to action had 12.2 times the odds of planning to be vaccinated in the next flu season than those who did not. Accepting and resistant individuals have significant differences in their beliefs, which require different intervention strategies to increase vaccination rates. These findings provide important information to researchers and practitioners working to increase influenza vaccination rates.
Influenza vaccination rates have varied slightly in recent years in response to H1N1 and changing recommendations but are still far below national goals (Centers for Disease Control and Prevention, 2010). Health beliefs strongly influence whether someone engages in a simple, voluntary health behavior like obtaining an annual influenza vaccination. Unfortunately, unvaccinated individuals who would benefit from the vaccine’s protection hold health beliefs that undermine efforts to achieve targeted vaccination rates.
It has been estimated that approximately 80% of the U.S. population are members of a special at-risk group that the Advisory Committee on Immunization Practices (ACIP) recommends for priority vaccination (Centers for Disease Control and Prevention, 2010). Because the proportion of the population considered at risk is so large, since 2010, the ACIP has recommended universal vaccination of everyone 6 months of age and older. However, only 39% of the U.S. adult population was vaccinated for influenza during 2011-2012 (Centers for Disease Control and Prevention, 2012).
Public health has had some success in reaching people who are most receptive to vaccination. Public health’s primary focus has been on people 65 years of age and older, which is the group most likely to receive a vaccination. This age group had a vaccination rate of 66% during 2008-2009. Influenza vaccination rates for other priority groups were much lower. Among those with a high-risk condition, such as asthma, only 33% of 18- to 49-year-olds and 51% of 50- to 64-year-olds were vaccinated in 2008-2009. Also of concern is that, in 2007-2008, less than half (49%) of health care workers, who can transmit the virus within the health care system, were vaccinated (Centers for Disease Control and Prevention, 2010).
Although vaccination rates have varied within a narrow range in the United States over the last few years, rates have not improved dramatically among any group for more than a decade. Rather than simply increasing intervention efforts that have proven to work in the past with receptive individuals (Briss et al., 2000), public health must now develop and adopt new strategies to interest those who are indifferent or resistant to vaccination efforts. It should not be assumed that increasing the intensity or reach of recognized best practices that have worked among the most receptive will be effective in reaching the less willing and the least receptive.
To increase rates of influenza vaccination, public health will need to respond with new approaches targeted at beliefs and perceptions about influenza vaccination. The Health Belief Model (HBM) can be used to understand beliefs and perceptions about influenza vaccination and guide the choice of interventions for people indifferent or resistant to influenza vaccination. According to the HBM, individuals are more likely to get vaccinated for influenza if they think they are susceptible to influenza, think influenza is a serious condition, believe influenza vaccination would reduce their susceptibility to influenza or make influenza symptoms less severe, do not think the flu shot has excessive personal costs and the benefits of vaccination outweigh those costs, and are confident in their ability to obtain a vaccination (Rosenstock, 1966; Rosenstock, Strecher, & Becker, 1988).
Perceived susceptibility is the belief in personal vulnerability to influenza. Previous studies have established that people who had been vaccinated for influenza were more likely to see themselves at higher risk for influenza than the unvaccinated, whereas those who were not vaccinated for influenza saw themselves as unlikely to contract influenza (Brewer & Hallman, 2006; Chapman & Coups, 1999; Mayo & Cobler, 2004; Nowalk, Zimmerman, Shen, Jewell, & Raymund, 2004; Santibanez et al., 2002; Tabbarah et al., 2005; Telford & Rogers, 2003; Willis & Wortley, 2007; Zimmerman, Santibanez, et al., 2003). However, two studies have shown that individuals resistant to influenza vaccination are concerned about the susceptibility of vulnerable family members, and were willing to get vaccinated to protect the health of someone they cared about (Bardenheier et al., 2006; John & Cheney, 2008).
Perceived severity refers to an individual’s belief about the seriousness of influenza and its consequences. This includes physical health and social consequences such as ability to work and maintain family and social relationships. According to the HBM, perceived severity is particularly important when susceptibility beliefs are high. However, research has shown that perceived severity alone was not a significant predictor of influenza vaccination (Armstrong, Berlin, Schwartz, Propert, & Ubel, 2001; Blue & Valley, 2002; Brewer & Hallman, 2006) probably because most people, whether vaccinated or unvaccinated, saw it as a serious illness, particularly for someone their age (Chi & Neuzil, 2004; Lindley, Wortley, Winston, & Bardenheier, 2006).
Perceived threat refers to an individual’s joint perceptions of susceptibility and severity. Beliefs in susceptibility and severity must be high before influenza is seen as a serious threat to personal health (Brewer & Rimer, 2008).
Perceived benefit refers to an individual’s belief in a range of potential benefits of obtaining a flu vaccination. One of the most important benefits is the effectiveness of the vaccination in a given year to reduce the risk or seriousness of influenza. Several studies have found that perceived effectiveness of the vaccine is one of the most consistent predictors of influenza vaccination (Brewer & Hallman, 2006; Chapman & Coups, 1999; Prislin, Dyer, Blakely, & Johnson, 1998; Tabbarah et al., 2005).
Perceived barriers are an individual’s belief about the physical and psychological costs of getting vaccinated for influenza. Those who are resistant to vaccination are more likely to report experiencing vaccination side effects or getting sick from the influenza vaccination (Armstrong et al., 2001; Brewer & Hallman, 2006; Chapman & Coups, 1999; Chi & Neuzil, 2004; Gosney, 2000; John & Cheney, 2008; Lindley et al., 2006; Mayo & Cobler, 2004; Santibanez et al., 2002; Tabbarah et al., 2005; Winston, Wortley, & Lees, 2006; Zimmerman, Santibanez, et al., 2003). Previous research has also documented knowledge barriers (Gosney, 2000; Lindley et al., 2006; Ritvo et al., 2003) and a general concern about the safety of the influenza vaccination (Allison et al., 2010; Chen et al., 2011; John & Cheney, 2008; Lindley et al., 2006; Telford & Rogers, 2003; Willis & Wortley, 2007; Wray et al., 2007). Despite these misgivings, about half (48%) of older adults who doubted the effectiveness of the vaccine and a third (37%) of those who thought the vaccine causes illness would still agree to get a vaccination to protect others (Bardenheier et al., 2006).
Costs and benefits: Research has shown that, regardless of vaccination status, people see vaccination as entailing costs and benefits. Those who were not vaccinated commonly acknowledged some benefits to vaccination, but, on balance, saw more costs than benefits (Bardenheier et al., 2006; Blue & Valley, 2002; Chi & Neuzil, 2004; Nowalk et al., 2004; Zimmerman, Santibanez, et al., 2003).
Self-efficacy refers to an individual’s confidence in his or her ability to successfully get vaccinated. Few studies related to influenza vaccination have looked directly at the role of self-efficacy, perhaps because vaccination is a simple, time-limited behavior that does not require lifestyle adjustments or changes to complex health behaviors such as adhering to an exercise program or eating a healthier diet (Brewer & Rimer, 2008; Champion & Skinner, 2008). In the case of influenza vaccination, self-efficacy does not appear to be an important determinant of influenza vaccination among adults (Chapman & Coups, 1999).
Cues to action are environmental prompts to activate an individual’s readiness to seek a vaccination. Considered a trigger to take action within the HBM, it is the link between belief and behavior. Health care provider recommendation has been associated with higher rates of influenza vaccination (Allison et al., 2010; Armstrong et al., 2001; Chen et al., 2011; Mayo & Cobler, 2004; Winston et al., 2006) primarily for those who are more accepting (Bardenheier et al., 2006; Chi & Neuzil, 2004; Nowalk et al., 2004; Winston et al., 2006). Even for those who were resistant to influenza vaccination, a provider recommendation made vaccination more likely (Bardenheier et al., 2006; Chi & Neuzil, 2004; Lindley et al., 2006; Wray et al., 2007).
Family members are considered another source of an effective cue to action (Nowalk et al., 2004; Zimmerman, Nowalk, et al., 2003; Zimmerman, Santibanez, et al., 2003) although not all studies found them to be influential (Mayo & Cobler, 2004). A belief that influenza vaccination is the social norm (Allison et al., 2010; Chapman & Coups, 1999) was also found to be an effective cue to action.
Existing research provides relevant information about vaccine acceptance. However, it does not help as much if we wish to understand what influences the behavior of the unvaccinated. There is little information available about individuals resistant to influenza vaccination. The objectives for this study were to utilize the HBM as a framework for understanding beliefs surrounding indifference or resistance to influenza vaccination and to identify intervention points and messaging strategies to increase future vaccination rates among the unvaccinated.
Method
This formative research was based on survey data collected during eight focus group discussions with 74 individuals from Oklahoma County, Oklahoma, that were conducted between March and June 2007. The purpose of the focus group discussions was to understand individual attitudes, behaviors, and concerns about influenza vaccination and how practitioners can improve influenza vaccination rates among resistant individuals. Results of the focus group discussions are reported elsewhere (John & Cheney, 2008). The focus of the present study is on the questionnaires that were administered to the focus group participants.
Participants were eligible to participate in the study if they were a member of a population group whose influenza vaccination rates were lower than the general population and/or were members of identifiable high-risk groups (Centers for Disease Control and Prevention, 2010), including ethnic minority, low socioeconomic status, and chronically ill adults. Additional inclusion criteria were age above 30 and to not have received an influenza vaccination during the 2006-2007 flu season.
A purposive sampling strategy was used to recruit individuals in high-risk groups who had not received an influenza vaccination in the past year. Participant recruitment information was distributed through a wide variety of community sources to increase representativeness of the sample, including local businesses, community centers, local clinics, distribution lists from local community coalitions and service organizations, libraries, and grocery stores. A signed informed consent was obtained from each person before participation in the study and each participant received a US$30 store gift card at the end of the session.
Every participant filled out two questionnaires, one at the beginning of the focus group discussion and the second following the discussion. Each questionnaire took approximately 10 min to complete. The first questionnaire contained questions about basic demographic information and social characteristics, past and anticipated flu vaccination behavior, health status and conditions, and work or caregiving responsibilities that would place them in contact with vulnerable groups (chronically ill, children, or elderly).
The second questionnaire collected health belief information about influenza vaccination that is important in understanding what influences and issues may be important in getting reluctant individuals to get a flu shot. The 45 questions in this questionnaire were based on previous research of influenza vaccination assessed in adult populations (Bardenheier et al., 2006; Chi & Neuzil, 2004; Hebert, Frick, Kane, & McBean, 2005; Nowalk et al., 2004; Prislin et al., 1998; Zimmerman, Santibanez, et al., 2003). Each of the surveys except Prislin et al. (1998) was developed for adults 65 years of age or older. The Prislin et al. questionnaire was developed for adults who had a child aged 2 to 24 months living at their home.
To test the HBM, the analysis incorporated variables that specified the main constructs of the model: perceived susceptibility (1 variable), perceived severity (3 variables), perceived benefits (9 variables), perceived barriers (23 variables), and cues to action (4 variables). Although self-efficacy is now routinely added to the HBM, it is not needed to understand simple health behaviors like obtaining an influenza vaccination (Brewer & Rimer, 2008; Champion & Skinner, 2008).
Because of the large number of independent variables used to specify the HBM constructs, factor and/or reliability analyses were conducted on the perceived benefits, perceived barriers, and cues to action variables. For each of the constructs with a large number of variables (perceived benefits and perceived barriers), a principal axis factor procedure with varimax rotation was run to identify latent variables and reduce the number of independent variables that would be used in the multivariate logistic regression analysis. Because the number of cases with missing values was small, missing values were replaced with the mean. After the factors were identified, a reliability analysis was conducted on the perceived benefits and barriers subscales. All data analysis was conducted using SPSS 19 (IBM, 2010).
Perceived Benefits Scale
A principal axis factor procedure with varimax rotation was run using the nine perceived benefits. The final solution resulted in a factor that contained the following five variables: “I am willing to get a flu shot if I were sure it prevented the flu,” “I would get the flu shot to stay healthy,” “Getting a flu shot is a wise thing to do,” “I would get a flu shot to prevent spreading the disease to people close to me,” and “I would rather have a flu shot than get the flu.” Analysis established that the measure of sampling adequacy was very good (Kaiser-Meyer-Olkin [KMO] = .86) and the model fit the data well. Reponses were summed across the five variables to create a perceived benefits scale. The scale was additive and highly reliable (Cronbach’s α = .90).
Perceived Barriers Scales
A principal axis factor procedure with varimax rotation was run using the 23 perceived barriers. The final solution resulted in four factors and analysis established that the measure of sampling adequacy was adequate (KMO = .79) and the model fit the data well. The first factor, which we labeled Access Barriers was composed of “Doctors or clinics that give the flu shot are hard to reach,” “Doctors/clinics that give the flu shot are not open when I can get there,” and “It is difficult for me to find the time to get a flu shot.” This three-item scale had very good reliability (Cronbach’s α = .84). The second barriers scale, Perceived Harm, was composed of “The flu shot causes a person to get the flu,” “Serious side effects from the flu shot are common,” and “I worry about side effects from the flu shot.” This three-item scale had adequate reliability (Cronbach’s α = .74). The third perceived barriers scale was composed of three variables: “I wonder about the safety of the flu vaccine,” “Flu shots are unnecessary,” and “Healthy people do not need to get a flu shot.” We labeled this scale Belief Barriers. This three-item scale had marginally adequate reliability (Cronbach’s α = .69). The final perceived barriers scale was composed of “I do not trust a doctor’s advice to get a flu shot,” “Getting a flu shot is more trouble than it is worth,” and “I do not like the way doctors and clinic staff that give the flu shot treat me.” This three-item scale, which we labeled Mistrust, also had marginally adequate reliability (Cronbach’s α = .66).
Cues to Action
Four variables were use to construct a cues to action scale: “I would get a flu shot if my doctor or nurse recommended it,” “I would get a flu shot if my family wanted me to,” “News of a bad flu season would influence me to get the flu shot,” and “I am willing to get both pneumonia and flu vaccines at the same time if my doctor recommends it.” None of these variables contained missing values. This four item scale had excellent reliability (Cronbach’s α = .88).
To identify significant independent variables that were not included in one of the benefits or barriers subscales, bivariate correlations were calculated to determine whether any of the variables that were not included in one of the scales was associated with the two dependent variables (whether the respondent plans to get a flu shot next year and whether they never ask their doctor or nurse for the flu shot). This resulted in the identification of an additional benefit variable and two barrier variables that were included in the logistic regression analysis. The relatively small sample size placed constraints on the logistic regression analysis. Therefore, all the independent variables used in the analysis were dichotomized at the median.
Results
Characteristics of Focus Group Participants
As seen in Table 1, participants ranged in age from 30 to 75 years, with a mean age of 49.3 years. Two thirds of the participants (66.2%) were women. More than two thirds of the participants were non-Hispanic White (36.5%) or African American (35.1%).
Demographic Characteristics of Participants.
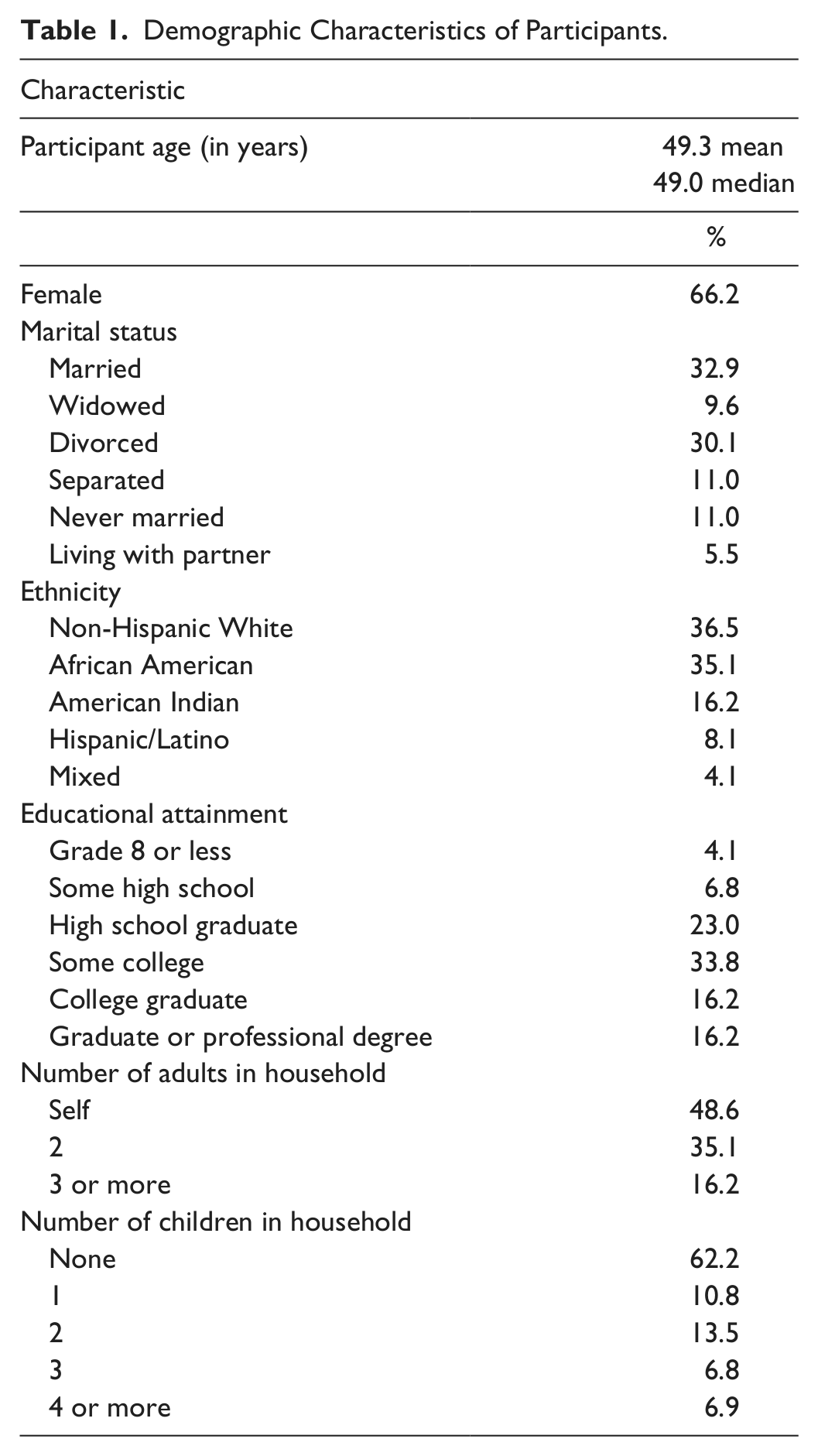
Participants tended to be highly educated with approximately one third having obtained a college degree (16.2%), a graduate or professional degree (16.2%), or some college (33.8%).
Table 2 documents the self-reported health status, behaviors, and resources of the participants. The vast majority of participants were in good or excellent self-rated health, 63.5% and 16.2%, respectively. Participants tended to appraise their health as about the same (41.9%) or better (44.6%) and only 13.5% as worse than others their age. Among the participants, 73% said they have a usual place of health care.
Health Status, Behaviors, and Resources of Participants.

None of the participants got an influenza vaccination during 2006-2007. However, 30.6% said they planned to get an influenza vaccination next year. This information was collected before the focus group discussion began, so the response was not influenced by the information or opinions expressed by the group.
HBM
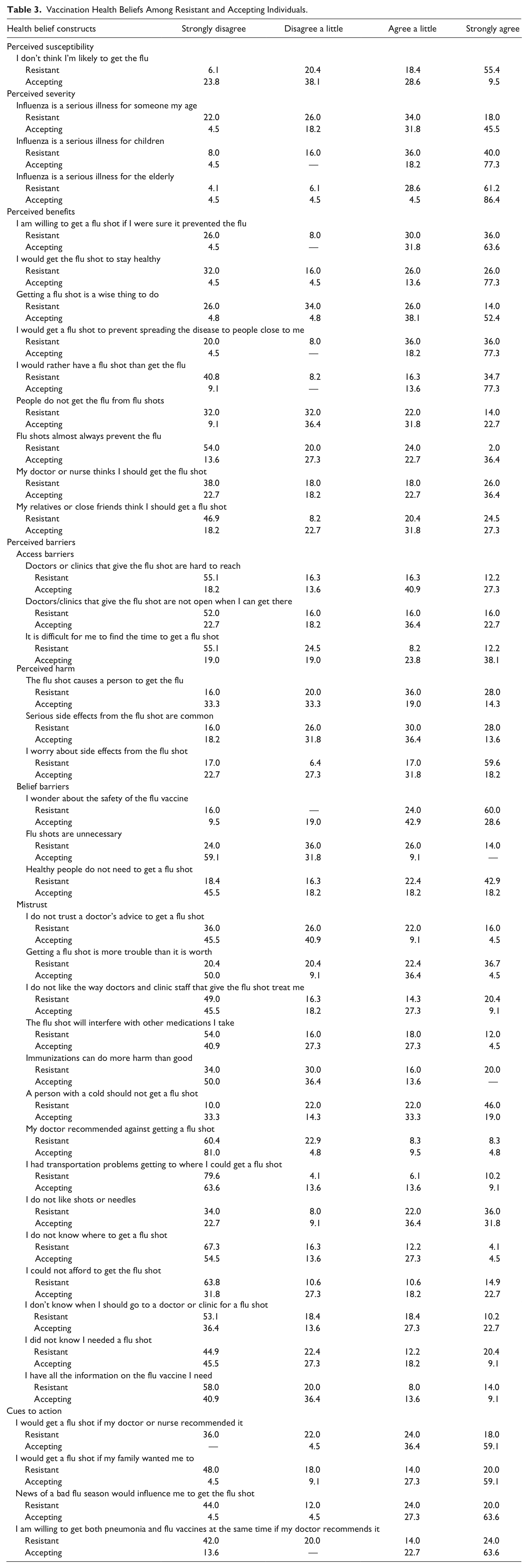
Table 3 shows the level of agreement of participants who were accepting and resistant to influenza vaccination for each of the major constructs of the HBM.
Vaccination Health Beliefs Among Resistant and Accepting Individuals.
Perceived susceptibility
Table 3 documents that resistant individuals did not believe they were susceptible to the flu. Whereas 74% of resistant individuals agreed with “I don’t think I’m likely to get the flu,” only 38% of accepting individuals agreed.
Perceived severity
Three items assessed beliefs in the severity of influenza for self and vulnerable others. Many resistant individuals did not perceive influenza as a serious illness for someone their age. Participants were somewhat more likely to perceive influenza as a serious illness for children, and there was general agreement that influenza is a serious illness for the elderly. However, the intensity of these beliefs differed between resistant and accepting individuals. Responses to “I don’t think I am likely to get the flu” (perceived susceptibility) were reverse coded and multiplied by “Flu is a serious illness for someone my age” (perceived severity) to create a perceived threat variable (Champion & Skinner, 2008).
Perceived benefit
Nine items measured beliefs about the benefits of influenza vaccination. Accepting individuals were far more likely than resistant individuals to strongly endorse each of the five items in the perceived benefits scale. Differences between groups in the other four items were less pronounced, but resistant individuals were less likely to favorably perceive the endorsement of vaccination by health care personnel or relatives and friends, were less sure that the vaccine does not cause the flu, and did not believe that flu shots prevent the flu.
Perceived barriers
The 23 perceived barriers comprised the largest number of independent variables. Table 3 reveals that accepting individuals were more likely to perceive access barriers to vaccination than resistant individuals. In contrast, resistant individuals were more likely to endorse the issues that comprise the Perceived Harm, Belief, and Mistrust barriers.
Cues to action
As seen in Table 3, accepting individuals were more likely to respond favorably to each of the cues to action. What is clear from these results is that family members were not a significant influence on resistant individual’s vaccination behavior and apparently were less influential than recommendation by a physician, especially among the most intensely resistant.
Logistic regression analysis
Tables 4 and 5 document the results of the logistic regression analysis using the HBM constructs to predict whether an individual plans to get a flu shot next year and whether they would ask a doctor or nurse for a flu shot. In the unadjusted model for plans to get a flu shot next year (Table 4), all the main HBM constructs were significant. This is what would be predicted by the HBM and confirms a general finding in the literature. Three barriers, access to vaccination, belief that the vaccination will cause harm, and negative beliefs about flu vaccination were significantly associated with plans to be vaccinated for influenza in the next flu season. Perceived barriers associated with mistrust of medical providers and the vaccine were not significantly associated with plans to be vaccinated next year.
Predictors of Plans to Get Influenza Vaccination Next Year.

Note: HBM = Health Belief Model.
Predictors of Asks Doctor or Nurse for Flu Shot.

Note: HBM = Health Belief Model.
All variables in the first panel were tested for inclusion in the final multivariate model using the forward stepwise method based on the likelihood ratio, which is recommended as the best method for this purpose (IBM, 2010). In the adjusted model, only perceived threat, perceived access barriers, and cues to action were significantly associated with plans to be vaccinated for influenza in the next flu season. People who saw influenza as a threat to their health had 5.4 times the odds of planning to be vaccinated than those who did not see influenza as a threat to health. Those who reported barriers to accessing influenza vaccination had 7.5 times the odds of reporting plans to be vaccinated, documenting that accepting individuals perceive barriers to obtaining vaccination while resistant individuals do not. Finally, those who responded positively to cues to action had 12.2 times the odds of planning to be vaccinated in the next flu season than those who did not respond positively to the cues.
Based on the final model, accepting individuals were more likely to perceive flu as a threat to health (perceive they were susceptible and that flu is a serious illness), access barriers were a problem that negatively influences their vaccination behavior, and cues to action were the most important influence on whether they plan to get vaccinated. In comparison, resistant individuals did not feel threatened by the flu, access barriers were not a problem because they were not trying to get vaccinated, and they did not respond favorably to cues to action from any source.
A discriminant analysis was run to determine how well the final model predicted group membership. The discriminant analysis confirmed that these three variables discriminated well between the two groups. The canonical correlation was .64 and 83.3% of cases were correctly classified using the cross-validation procedure in SPSS. In contrast to a previous study (Blue & Valley, 2002), this model was better at predicting group membership especially among resistant individuals (84%) compared with accepting individuals (82%).
In the first panel of Table 5, the unadjusted model reveals that each of the main HBM constructs was significantly related to asks doctor or nurse for a flu shot. Only Access and Mistrust barriers were not significant. However, once all the influences of the HBM constructs were taken into consideration using the same procedure as the previous analysis, only cues to action were independently related to asking for a flu shot.
Discussion
This study reveals that accepting and resistant individuals have significant, determinant differences in their health beliefs about influenza vaccination. These differences begin with diametrically opposed views of their susceptibility to the illness and the severity of influenza as a personal health problem. Furthermore, these divergent health beliefs extend to opposing views of the benefits of obtaining a flu vaccination, with accepting individuals subscribing to much more favorable opinions of the vaccine. More differences are evident when barriers are considered. Access is only a problem for those who intend to obtain a flu shot, so improving access will not matter for resistant individuals. Accepting individuals perceive access barriers while resistant individuals do not. In comparison, resistant individuals perceive harm, have negative health beliefs about the vaccine, and are somewhat more mistrustful of medical care. Finally, cues to action positively influence accepting individuals while resistant individuals ignore or actively dismiss these messages.
These results have profound implications for the prospect of improving influenza vaccination rates in the United States. Our results show that more of the recommended interventions or more intense or improved techniques that support these interventions will only succeed in marginal improvements in the influenza vaccination rates and will continue to fall well short of targeted vaccination goals advanced in Healthy People 2020.
Although more research is needed to gain an in-depth understanding of the population that is unresponsive or avoids annual vaccination, this research has established that it is a distinctly different population than the one that has been reached successfully so far. This research suggests that the pivotal issues that need to be addressed are within the Perceived Benefits and Perceived Barriers parts of the HBM. Cues to action will not have any influence unless basic perceptions are modified to shift neutral or negative beliefs in a more positive direction. Our research has shown that it is only among receptive individuals that these social influences are successful. Moreover, we do not believe that a direct fear appeal will be effective in changing perceived threat which the HBM considers essential because resistant individuals do not believe influenza is a threat to their personal health. Resistant individuals will not obtain a seasonal influenza vaccination to protect their health and any attempt to appeal to their sense of personal vulnerability will not succeed. Other evidence suggests that resistant individuals are concerned about the health of elderly relatives and children and an appeal to their altruism is more likely to succeed (John & Cheney, 2008). In this case, health provider recommendation may be more effective if the cue to action is to reduce the threat to significant others rather than themselves.
Additional Strategies to Increase Influenza Vaccination
The HBM focuses on the individual and their self-regarding behaviors, but individual behavior change is difficult to initiate and sustain without acknowledging and changing the surrounding social environment. Future studies could examine the effectiveness of interventions structured around the Ecological Model (McLeroy, Bibeau, Steckler, & Glanz, 1988), targeting family and social networks, organizations, community, and policy, to increase vaccination rates in this population. Asking resistant individuals to accompany family members to be vaccinated to ensure they received their vaccination, then being vaccinated themselves to increase the protection for vulnerable family members is one strategy to increase vaccination rates. Asking businesses and community organizations to vaccinate their employees during work hours would help accepting individuals overcome access barriers. In addition, working with health insurance companies to waive the co-pay for influenza vaccination or to expand coverage to more providers during vaccination season to allow accepting individuals more flexibility in time and place to be vaccinated may also help to increase rates. These ideas address access issues and are unlikely to alter the behavior of indifferent or resistant individuals. Resistant individuals need better knowledge about the vaccine that dispels misperceptions and fears, and messaging touting the benefits of being vaccinated to protect the health of significant others (especially the elderly and children).
HBM Limitations
These results document that the HBM is a useful framework for understanding differences between those individuals who are accepting and resistant to influenza vaccination, but it has limitations. Research has shown that past vaccination behavior is one of the strongest predictors of future influenza vaccination (Armstrong et al., 2001; Brewer & Hallman, 2006; Chapman & Coups, 1999; Chi & Neuzil, 2004; Mayo & Cobler, 2004; Xakellis, 2005), but past behavior is not explicitly incorporated into the HBM. Chapman and Coups (1999) suggested the influence of past behavior is partly accounted for by perceived effectiveness of the vaccine, along with the likelihood of side effects, so that individuals would be more likely to be vaccinated if their previous experience suggested that the vaccine was effective in preventing influenza and caused no or few side effects. In the absence of a positive personal experience with the flu shot, beliefs regarding the flu shot (whether well-founded or nonrational) will be the primary determinant of behavior.
To determine the influence of past experience on intent to obtain a flu shot, the sample was divided into three groups: those who never had a flu shot and did not intend to get one next year (the Never/Nots), individuals who ever received a flu shot and did not intend to get a flu shot the next year (the Ever/Nots), and individuals who had received a flu shot before and intended to get one next year (Accepting). A series of cross-tabulations of group by HBM variable revealed that the biggest differences are between the Never/Nots and the Accepting group. This analysis revealed that individuals in the Accepting group are true believers in the flu shot. They have few doubts about the merits of being vaccinated. The Never/Not group is the mirror image of the true believers, exhibiting a substantial negative consensus about the problems with flu vaccination. In general, the Ever/Not group is intermediate with mixed perceptions of the flu shot, but more like the Never/Nots than Accepting individuals. From the standpoint of the HBM, the individuals who are most resistant to influenza vaccination have no personal experience on which they base their perceptions.
Another deficiency of the HBM is that it assumes that health behaviors are the result of concern for one’s own health. However, this research provides additional evidence that this is a weak motivation for indifferent or resistant individuals who appear to be more willing to be vaccinated in response to the health threat to vulnerable others (John & Cheney, 2008). Engaging in a health behavior based on altruistic beliefs of a health threat to others is not adequately accounted for in the model. For this particular health behavior, an altruistic appeal to protect the health of significant others may be the only appeal that will make a difference to resistant individuals.
The HBM represents health beliefs as static and research using the HBM is overwhelmingly cross-sectional, looking at health beliefs at one point in time. Our research is consistent with this approach. However, we do not have an indication of how stable these beliefs are over time, taking into account vaccine effectiveness from year to year, the increasing age of the individual, and increasing media coverage of influenza outbreaks such as H1N1. On the other hand, for many individuals, strongly held beliefs are difficult to change. No research has established the extent to which beliefs about influenza vaccination can be modified for resistant individuals. If they are difficult to change, the HBM loses some of its utility and is not as useful as an alternate model such as Social Marketing, which has a primary focus on changing behaviors based on precisely targeted appeals to specific audience segments that have different beliefs and attitudes toward the health behavior. In a sense, this research confirms the existence of distinct audience segments with different psychographics toward the behavior.
Study Limitations
As an exploratory research project based on a purposive sampling strategy, the primary limitation of this study is the small sample size. Every precaution was taken to minimize this problem, including data reduction, analysis of measures of sampling adequacy, using binary variables, and limiting the number of independent variables in the multivariate logistic regression models. However, a larger sample size would have improved the data reduction process and strengthened the formation of the HBM scales and the multivariate logistic regression results.
A potential secondary limitation is that the sample was not a random sample and the results may not be generalizable to the population of individuals who are indifferent or resistant to seasonal influenza vaccination. This limitation was intentional and unavoidable because few studies have sought to understand the health beliefs of the majority of Americans who fail to get a seasonal influenza vaccination on a regular basis. The indifferent or resistant population is the population that needs to be the subject of influenza vaccination research.
Another potential limitation raised by one reviewer is the questionnaire’s placement after the focus group discussion. Although it is possible that the focus group discussion influenced questionnaire responses, the influence should have been minimal or beneficial for our purpose. Focus group discussions are meant to allow participants to fully consider their views and compare them with the views of others on a particular topic and then be able to offer an informed opinion in contrast to the instantaneous, top-of-the-mind initial reaction required by most survey research. If anything, the focus group discussion helped participants develop a refined opinion about their beliefs and attitudes toward influenza vaccination.
Conclusion
Accepting and resistant individuals have significantly different beliefs toward influenza vaccination that require different intervention strategies to increase vaccination rates. This research provides important information to researchers and practitioners by focusing interventions on different constructs of the HBM to increase influenza vaccination. Accepting individuals need better access, fewer barriers, more effective cues to action, and messages that heighten their sense of personal susceptibility. Although necessary, these features of an influenza vaccination intervention will only result in marginal improvements in vaccination rates because these features are not seen as important by indifferent and resistant individuals. Resistant individuals need to be convinced that there is a reason for them to practice a behavior that they do not view favorably or for which they do not see a need because they do not view influenza as a threat to their health. To increase vaccination among resistant individuals, this research suggests the need to address a number of health beliefs such as worry about side effects and healthy people do not need a flu shot, and to expand the HBM to include health behaviors done for altruistic motives to protect the health of vulnerable loved ones. In this case, the latter concern would not require resistant individuals to change their beliefs about the vaccine, but still practice the behavior.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Partial funding for this project was provided by the Oklahoma State Department of Health.
Author Biographies